
Therapeutic Efficacy of Transcutaneous Electrical Nerve Stimulation Acupoints on Motor and Neural Recovery of the Affected Upper Extremity in Chronic Stroke: A Sham-Controlled Randomized Clinical Trial

 , , ,
, , ,  and
and
Abstract
:1. Introduction:
2. Subjects and Methods
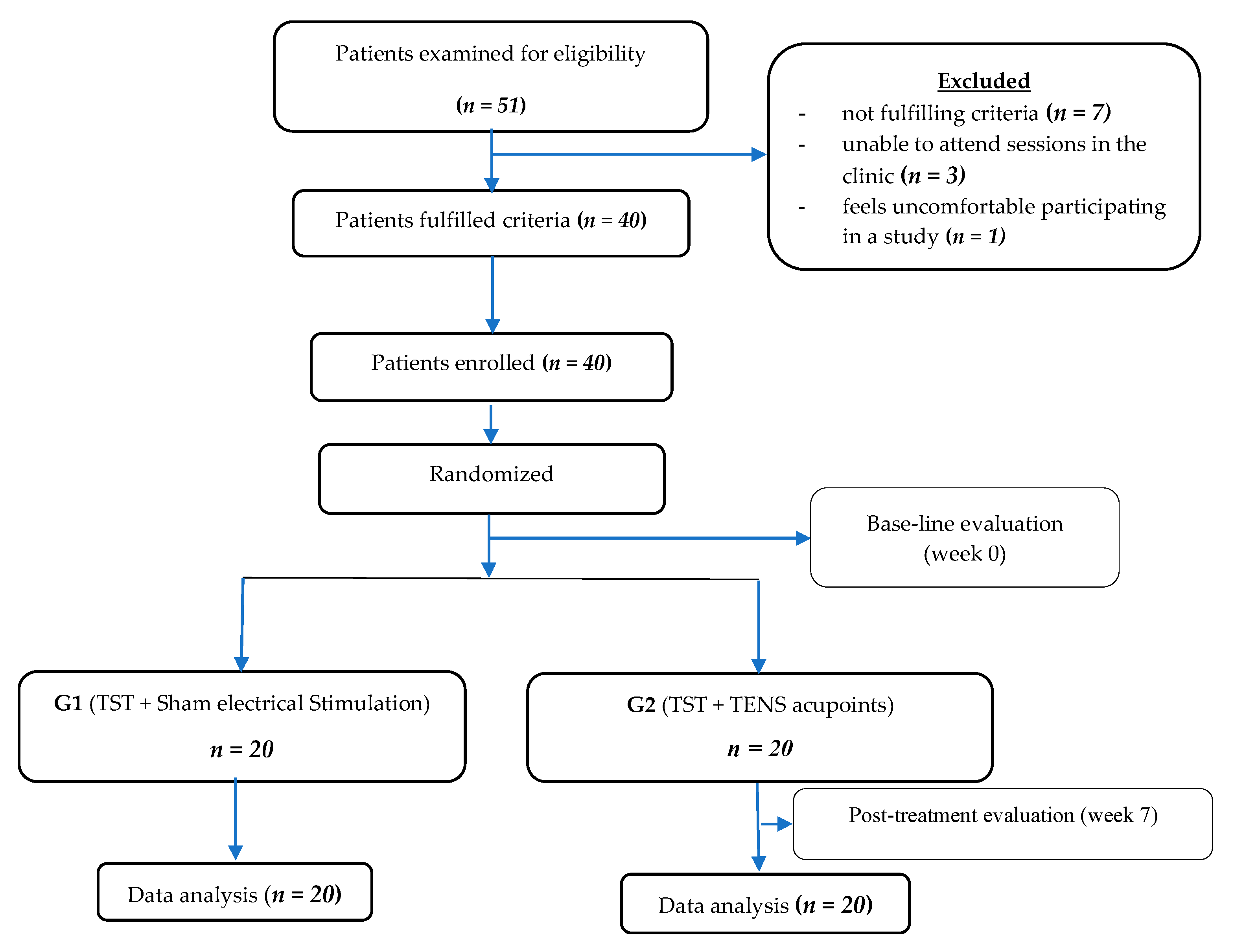
2.1. Study Design
2.2. Randomization
2.3. Sample Size
2.4. Clinical Examination
2.4.1. Fugl-Meyer Assessment of the Upper Extremity (FMA-UE)
2.4.2. Box and Block Test (BBT)
2.4.3. Quantitative Electroencephalogram (QEEG)
2.5. Therapeutic Interventions and Procedures
2.5.1. Task-Specific Training (TST)
- mimicking drinking water from a glass;
- holding a cup of water and raising it to a level of 90° shoulder flexion while maintaining the elbow joint extended;
- picking up five tennis balls and moving them from a table to a box;
- polishing a table with a towel, in various directions, while keeping the elbow joint extended;
- holding a cone and moving it from a table to a shelf;
- brushing the hair using a comb.
2.5.2. Transcutaneous Electrical Nerve Stimulation (TENS) Acupoints
2.6. Statistical Analysis
3. Results
3.1. Demographic Data and Baseline Clinical Characteristics
3.2. Clinical Scales
3.3. Quantitative Electroencephalogram (QEEG)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyer, S.; De Bruyn, N.; Krumlinde-Sundholm, L.; Peeters, A.; Feys, H.; Thijs, V.; Verheyden, G. Associations between Sensorimotor Impairments in the Upper Limb at 1 Week and 6 Months After Stroke. J. Neurol. Phys. Ther. 2016, 40, 186–195. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J.; et al. Heart Disease and Stroke Statistics—2015 Update. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaheen, H.A.; Wahed, W.Y.A.; Hasaneen, S.T. Prevalence of Stroke in Fayoum Governorate, Egypt: A Community-Based Study. J. Stroke Cerebrovasc. Dis. 2019, 28, 2414–2420. [Google Scholar] [CrossRef]
- Trujillo, P.; Mastropietro, A.; Scano, A.; Chiavenna, A.; Mrakic-Sposta, S.; Caimmi, M.; Molteni, F.; Rizzo, G. Quantitative EEG for Predicting Upper Limb Motor Recovery in Chronic Stroke Robot-Assisted Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Sahin, N.; Ugurlu, H.; Albayrak, I. The efficacy of electrical stimulation in reducing the post-stroke spasticity: A randomized controlled study. Disabil. Rehabil. 2011, 34, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Persson, H.C.; Danielsson, A.; Broeren, J.; Lundgren-Nilsson, Å.; Sunnerhagen, K.S. SALGOT—Stroke Arm Longitudinal study at the University of Gothenburg, prospective cohort study protocol. BMC Neurol. 2011, 11, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noma, T.; Matsumoto, S.; Shimodozono, M.; Iwase, Y.; Kawahira, K. Novel Neuromuscular Electrical Stimulation System for the Upper Limbs in Chronic Stroke Patients. Am. J. Phys. Med. Rehabil. 2014, 93, 503–510. [Google Scholar] [CrossRef] [Green Version]
- Au-Yeung, S.S.Y.; Hui-Chan, C.W.Y. Electrical acupoint stimulation of the affected arm in acute stroke: A placebo-controlled randomized clinical trial. Clin. Rehabil. 2013, 28, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Swethankh, K.S.; Vasu, D.T.; Jimshad, T.U. Effect of Acupuncture-Like Tens on Hand Function in Sub-Acute Stroke—A Comparative Study. Int. J. Phys. Educ. Sports Health 2016, 3, 261–264. [Google Scholar]
- Yan, T.; Hui-Chan, C. Transcutaneous electrical stimulation on acupuncture points improves muscle function in subjects after acute stroke: A randomized controlled trial. J. Rehabil. Med. 2009, 41, 312–316. [Google Scholar] [CrossRef] [Green Version]
- Johansson, B.B.; Haker, E.; Von Arbin, M.; Britton, M.; Långström, G.; Terént, A.; Ursing, D.; Asplund, K. Acupuncture and Transcutaneous Nerve Stimulation in Stroke Rehabilitation. Stroke 2001, 32, 707–713. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.-G.; Cao, C.-H.; Liu, C.-Z.; Han, B.-J.; Zhang, J.; Li, Z.-G.; Yu, T.; Wang, X.-H.; Zhao, H.; Xu, Z.-H. Effect of acupuncture treatment on spastic states of stroke patients. J. Neurol. Sci. 2009, 276, 143–147. [Google Scholar] [CrossRef]
- Wang, B.H.; Lin, C.L.; Li, T.M.; Lin, S.D.; Lin, J.G.; Chou, L.W. Selection of acupoints for managing upper-extremity spasticity in chronic stroke patients. Clin. Interv. Aging 2014, 9, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.L.; Cui, S.; Fook-Chong, S. The effect of acupuncture on motor cortex excitability and plasticity. Neurosci. Lett. 2005, 384, 145–149. [Google Scholar] [CrossRef]
- Yan, T.; Hui-Chan, C.W.Y.; Li, L.S.W. Functional Electrical Stimulation Improves Motor Recovery of the Lower Extremity and Walking Ability of Subjects with First Acute Stroke. Stroke 2005, 36, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chipchase, L.; Schabrun, S.; Hodges, P. Peripheral electrical stimulation to induce cortical plasticity: A systematic review of stimulus parameters. Clin. Neurophysiol. 2011, 122, 456–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, L.-L.H.; Yang, W.-W.; Kao, C.-L.; Tsai, M.-W.; Wei, S.-H.; Fregni, F.; Chen, V.C.-F.; Chou, L.-W. Effects of 8-week sensory electrical stimulation combined with motor training on EEG-EMG coherence and motor function in individuals with stroke. Sci. Rep. 2018, 8, 9217. [Google Scholar] [CrossRef] [PubMed]
- Volz, M.S.; Suarez-Contreras, V.; Mendonca, M.E.; Pinheiro, F.S.; Merabet, L.B.; Fregni, F. Effects of Sensory Behavioral Tasks on Pain Threshold and Cortical Excitability. PLoS ONE 2013, 8, e52968. [Google Scholar] [CrossRef] [Green Version]
- Carr, J.H.; Shepherd, R.B. Neurological Rehabilitation: Optimizing Motor Performance; Churchill Livingstone: London, UK, 2010. [Google Scholar]
- McCombe, W.S.; Whitall, J. Bilateral arm training: Why and who benefits? Neuro. Rehabil. 2008, 23, 29–41. [Google Scholar]
- Hubbard, I.J.; Parsons, M.W.; Neilson, C.; Carey, L.M. Task-specific training: Evidence for and translation to clinical practice. Occup. Ther. Int. 2009, 16, 175–189. [Google Scholar] [CrossRef]
- Agni, P.N.; Kulkarni, V. Effect of Strength Training, Functional Task Related Training and Combined Strength and Functional Task Related Training on Upper Extremity in Post Stroke Patients. Int. J. Physiother. 2017, 4, 184–190. [Google Scholar] [CrossRef]
- Khallaf, M.E. Effect of Gravity and Task Specific Training of Elbow Extensors on Upper Extremity Function after Stroke. Neurol. Res. Int. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Thant, A.A.; Wanpen, S.; Nualnetr, N.; Puntumetakul, R.; Chatchawan, U.; Hla, K.M.; Khin, M.T. Effects of task-oriented training on upper extremity functional performance in patients with sub-acute stroke: A randomized controlled trial. J. Phys. Ther. Sci. 2019, 31, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Bashir, S.; Mizrahi, I.; Weaver, K.; Fregni, F.; Pascual-Leone, A. Assessment and Modulation of Neural Plasticity in Rehabilitation with Transcranial Magnetic Stimulation. PM&R 2010, 2, S253–S268. [Google Scholar] [CrossRef] [Green Version]
- Finnigan, S.; van Putten, M.J. EEG in ischaemic stroke: Quantitative EEG can uniquely inform (sub-)acute prognoses and clinical management. Clin. Neurophysiol. 2013, 124, 10–19. [Google Scholar] [CrossRef]
- Schleiger, E.; Sheikh, N.; Rowland, T.; Wong, A.; Read, S.; Finnigan, S. Frontal EEG delta/alpha ratio and screening for post-stroke cognitive deficits: The power of four electrodes. Int. J. Psychophysiol. 2014, 94, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Cauraugh, J.H.; Lodha, N.; Naik, S.K.; Summers, J.J. Bilateral movement training and stroke motor recovery progress: A structured review and meta-analysis. Hum. Mov. Sci. 2010, 29, 853–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- See, J.; Dodakian, L.; Chou, C.; Chan, V.; McKenzie, A.; Reinkensmeyer, D.J.; Cramer, S.C. A Standardized Approach to the Fugl-Meyer Assessment and Its Implications for Clinical Trials. Neurorehabilit. Neural Repair 2013, 27, 732–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, S.C.; Dodakian, L.; Le, V.; McKenzie, A.; See, J.; Augsburger, R.; Zhou, R.J.; Raefsky, S.M.; Nguyen, T.; Vanderschelden, B.; et al. A Feasibility Study of Expanded Home-Based Telerehabilitation After Stroke. Front. Neurol. 2021, 11. [Google Scholar] [CrossRef]
- Hsieh, Y.-W.; Wu, C.-Y.; Lin, K.-C.; Chang, Y.-F.; Chen, C.-L.; Liu, J.-S. Responsiveness and Validity of Three Outcome Measures of Motor Function After Stroke Rehabilitation. Stroke 2009, 40, 1386–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontson, K.; Marcus, I.; Myklebust, B.; Civillico, E. Targeted box and blocks test: Normative data and comparison to standard tests. PLoS ONE 2017, 12, e0177965. [Google Scholar] [CrossRef]
- Chen, H.-M.; Chen, C.C.; Hsueh, I.-P.; Huang, S.-L.; Hsieh, C.-L. Test-Retest Reproducibility and Smallest Real Difference of 5 Hand Function Tests in Patients with Stroke. Neurorehabilit. Neural Repair 2009, 23, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Santisteban, L.; Térémetz, M.; Bleton, J.-P.; Baron, J.-C.; Maier, M.A.; Lindberg, P.G. Upper Limb Outcome Measures Used in Stroke Rehabilitation Studies: A Systematic Literature Review. PLoS ONE 2016, 11, e0154792. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult Norms for the Box and Block Test of Manual Dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Niedermeyer, E.; Lopes, S.F.H. Electroencephalography: Basic Principles, Clinical Applications, and Related Fields; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Kleim, J.A.; Jones, T.A. Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation After Brain Damage. J. Speech Lang. Hear. Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef]
- Arya, K.N.; Verma, R.; Garg, R.; Sharma, V.; Agarwal, M.; Aggarwal, G. Meaningful Task-Specific Training (MTST) for Stroke Rehabilitation: A Randomized Controlled Trial. Top. Stroke Rehabil. 2012, 19, 193–211. [Google Scholar] [CrossRef]
- Deadman, P.; Baker, K.; Al-Khafaji, M. A Manual of Acupuncture, 2nd ed.; Journal of Chinese Medicine Publications: East Sussex, UK, 2007. [Google Scholar]
- Li, W.; Ahn, A. Effect of Acupuncture Manipulations at LI4 or LI11 on Blood Flow and Skin Temperature. J. Acupunct. Meridian Stud. 2016, 9, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.; Yang, L.-J.; Zhang, W.-B.; Jia, S.-Y.; Tian, Y.-Y.; Wang, G.-J.; Mu, X.; Wang, L.; Litscher, G. Observation of Microvascular Perfusion in the Hegu (LI4) Acupoint Area after Deqi Acupuncture at Quchi (LI11) Acupoint Using Speckle Laser Blood Flow Scanning Technology. Evid. Based Complement. Altern. Med. 2012, 2012, 1–4. [Google Scholar] [CrossRef]
- Large Intestine LI 11. Available online: http://www.acupuncture.com/education/points/largeintestine/li11.htm (accessed on 14 August 2020).
- Umemoto, K.; Naito, M.; Tano, K.; Terayama, H.; Koike, T.; Ohmichi, M.; Ohmichi, Y.; Sakabe, K.; Nakano, T. Acupuncture Point “Hegu” (LI4) Is Close to the Vascular Branch from the Superficial Branch of the Radial Nerve. Evid. Based Complement. Altern. Med. 2019, 2019, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Large Intestine LI 4. Available online: http://www.acupuncture.com/education/points/largeintestine/li4.htm (accessed on 14 August 2020).
- Adhikari, S.P.; Tretriluxana, J.; Chaiyawat, P.; Jalayondeja, C. Enhanced Upper Extremity Functions with a Single Session of Action-Observation-Execution and Accelerated Skill Acquisition Program in Subacute Stroke. Stroke Res. Treat. 2018, 2018, 1490692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edemekong, P.F.; Bomgaars, D.L.; Sukumaran, S.; Levy, S.B. Activities of Daily Living. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK470404/ (accessed on 1 January 2021).
- Jacqueline, F.; White, A. Medical Acupuncture: A Western Scientific Approach; Churchill Livingstone: Edinburgh, UK, 1998. [Google Scholar]
- Rand, D. Proprioception deficits in chronic stroke—Upper extremity function and daily living. PLoS ONE 2018, 13, e0195043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshmukh, M.; Kumar, C.; Goyal, M. Application of Transcutaneous Electrical Stimulation on Lower Limb Acupoints as an Important Adjunctive Tool in Stroke Rehabilitation Program & Its Effects on Spasticity and Functional Ability. Int. J. Physiother. Res. 2013, 3, 63–69. [Google Scholar]
- Kwong, P.W.; Ng, G.Y.; Chung, R.C.; Ng, S.S. Transcutaneous electrical nerve stimulation improves walking capacity and reduces spasticity in stroke survivors: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1203–1219. [Google Scholar] [CrossRef]
- Lim, S.M.; Yoo, J.; Lee, E.; Kim, H.J.; Shin, S.; Han, G.; Ahn, H.S. Acupuncture for Spasticity after Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2015, 2015, 870398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, L.; Mattison, P.; Paul, L.; Wood, L. The effects of transcutaneous electrical nerve stimulation (TENS) on spasticity in multiple sclerosis. Mult. Scler. J. 2007, 13, 527–533. [Google Scholar] [CrossRef]
- Shaygannejad, V.; Janghorbani, M.; Vaezi, A.; Haghighi, S.; Golabchi, K.; Heshmatipour, M. Comparison of the effect of baclofen and transcutaneous electrical nerve stimulation for the treatment of spasticity in multiple sclerosis. Neurol. Res. 2013, 35, 636–641. [Google Scholar] [CrossRef]
- Zhao, W.; Wang, C.; Li, Z.; Chen, L.; Li, J.; Cui, W.; Ding, S.; Xi, Q.; Wang, F.; Jia, F.; et al. Efficacy and Safety of Transcutaneous Electrical Acupoint Stimulation to Treat Muscle Spasticity following Brain Injury: A Double-Blinded, Multicenter, Randomized Controlled Trial. PLoS ONE 2015, 10, e0116976. [Google Scholar] [CrossRef]
- Zhang, C.; Zou, Y.; Li, K.; Li, C.; Jiang, Y.; Sun, J.; Sun, R.; Wen, H. Different effects of running wheel exercise and skilled reaching training on corticofugal tract plasticity in hypertensive rats with cortical infarctions. Behav. Brain Res. 2018, 336, 166–172. [Google Scholar] [CrossRef]
- Chung, S.H.; Kim, J.H.; Yong, S.Y.; Lee, Y.H.; Park, J.M.; Kim, S.H.; Lee, H.C. Effect of Task-Specific Lower Extremity Training on Cognitive and Gait Function in Stroke Patients: A Prospective Randomized Controlled Trial. Ann. Rehabil. Med. 2019, 43, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Richards, L.G.; Stewart, K.C.; Woodbury, M.L.; Senesac, C.; Cauraugh, J.H. Movement-dependent stroke recovery: A systematic review and meta-analysis of TMS and fMRI evidence. Neuropsychologia 2008, 46, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Z.; Sui, M.; Zhuang, Z.; Liu, H.; Zheng, X.; Cai, C.; Jin, D. Effectiveness of Neuromuscular Electrical Stimulation on Lower Limbs of Patients with Hemiplegia After Chronic Stroke: A Systematic Review. Arch. Phys. Med. Rehabil. 2018, 99, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Sharififar, S.; Shuster, J.J.; Bishop, M.D. Adding electrical stimulation during standard rehabilitation after stroke to improve motor function. A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2018, 61, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.S.; Hui-Chan, C.W. Transcutaneous Electrical Nerve Stimulation Combined with Task-Related Training Improves Lower Limb Functions in Subjects with Chronic Stroke. Stroke 2007, 38, 2953–2959. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Demographic Data | G1 (n = 20) | G2 (n = 20) | p Value | Cohen’s d | Effect Size (r) |
|---|---|---|---|---|---|
| Age (years) | 51.8 ± 5.7 | 52.5 ± 4.9 | 0.584 a | −0.132 | −0.066 |
| Gender (male/female) Type (infarction/hemorrhage) | 11/9 12/8 | 8/12 13/7 | 0.457 b 0.652 b | - - | - - |
| Height (cm) | 166.1 ± 7.21 | 164.7 ± 8.34 | 0.784 a | 0.180 | 0.089 |
| Weight (kg) | 65.2 ± 9.42 | 67.3 ± 11.31 | 0.651 a | −0.201 | −0.100 |
| Duration of stroke (month) | 21.22 ± 2.09 | 22.21 ± 3.07 | 0.949 a | −0.377 | −0.185 |
| FMA-UE | G1 | G2 | p Value | Cohen’s d | Effect Size (r) |
|---|---|---|---|---|---|
| Pre-test | 24.8 ± 3.05 | 24.8 ± 2.65 | 0.999 b | 0 | 0 |
| Post-test | 27.2 ± 3.14 | 28 ± 1.99 | 0.4116b b | −0.304 | −0.150 |
| p Value | 0.0001 a,* | 0.0001 a,* | - | - | - |
| BBT | G1 | G2 | p Value | Cohen’s d | Effect Size (r) |
|---|---|---|---|---|---|
| Pre-test | 23 ± 21.9 | 14 ± 15.5 | 0.517 b | 0.474 | 0.231 |
| Post-test | 38 ± 22.1 | 20 ± 12.3 | 0.790 b | 1.006 | 0.449 |
| p Value | 0.005 a,* | 0.002 a,* | - | - | - |
| QEEG (C3) | G1 | G2 | p Value | Cohen’s d | Effect Size (r) |
|---|---|---|---|---|---|
| Pre-test | 8.326 ± 0.13 | 8.501 ± 0.1 | 0.394 b | 1.363 | 0.563 |
| Post-test | 8.298 ± 0.03 | 9.443 ± 0.4 | 0.001 *,b | −4.037 | −0.896 |
| p Value | 0.886 a | 0.0005 *,a | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
M. Alwhaibi, R.; Mahmoud, N.F.; M. Zakaria, H.; M. Ragab, W.; Al Awaji, N.N.; Y. Elzanaty, M.; R. Elserougy, H. Therapeutic Efficacy of Transcutaneous Electrical Nerve Stimulation Acupoints on Motor and Neural Recovery of the Affected Upper Extremity in Chronic Stroke: A Sham-Controlled Randomized Clinical Trial. Healthcare 2021, 9, 614. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050614
M. Alwhaibi R, Mahmoud NF, M. Zakaria H, M. Ragab W, Al Awaji NN, Y. Elzanaty M, R. Elserougy H. Therapeutic Efficacy of Transcutaneous Electrical Nerve Stimulation Acupoints on Motor and Neural Recovery of the Affected Upper Extremity in Chronic Stroke: A Sham-Controlled Randomized Clinical Trial. Healthcare. 2021; 9(5):614. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050614
Chicago/Turabian StyleM. Alwhaibi, Reem, Noha F. Mahmoud, Hoda M. Zakaria, Walaa M. Ragab, Nisreen N. Al Awaji, Mahmoud Y. Elzanaty, and Hager R. Elserougy. 2021. "Therapeutic Efficacy of Transcutaneous Electrical Nerve Stimulation Acupoints on Motor and Neural Recovery of the Affected Upper Extremity in Chronic Stroke: A Sham-Controlled Randomized Clinical Trial" Healthcare 9, no. 5: 614. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050614