
Mechanical Changes of the Lumbar Intervertebral Space and Lordotic Angle Caused by Posterior-to-Anterior Traction Using a Spinal Thermal Massage Device in Healthy People

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
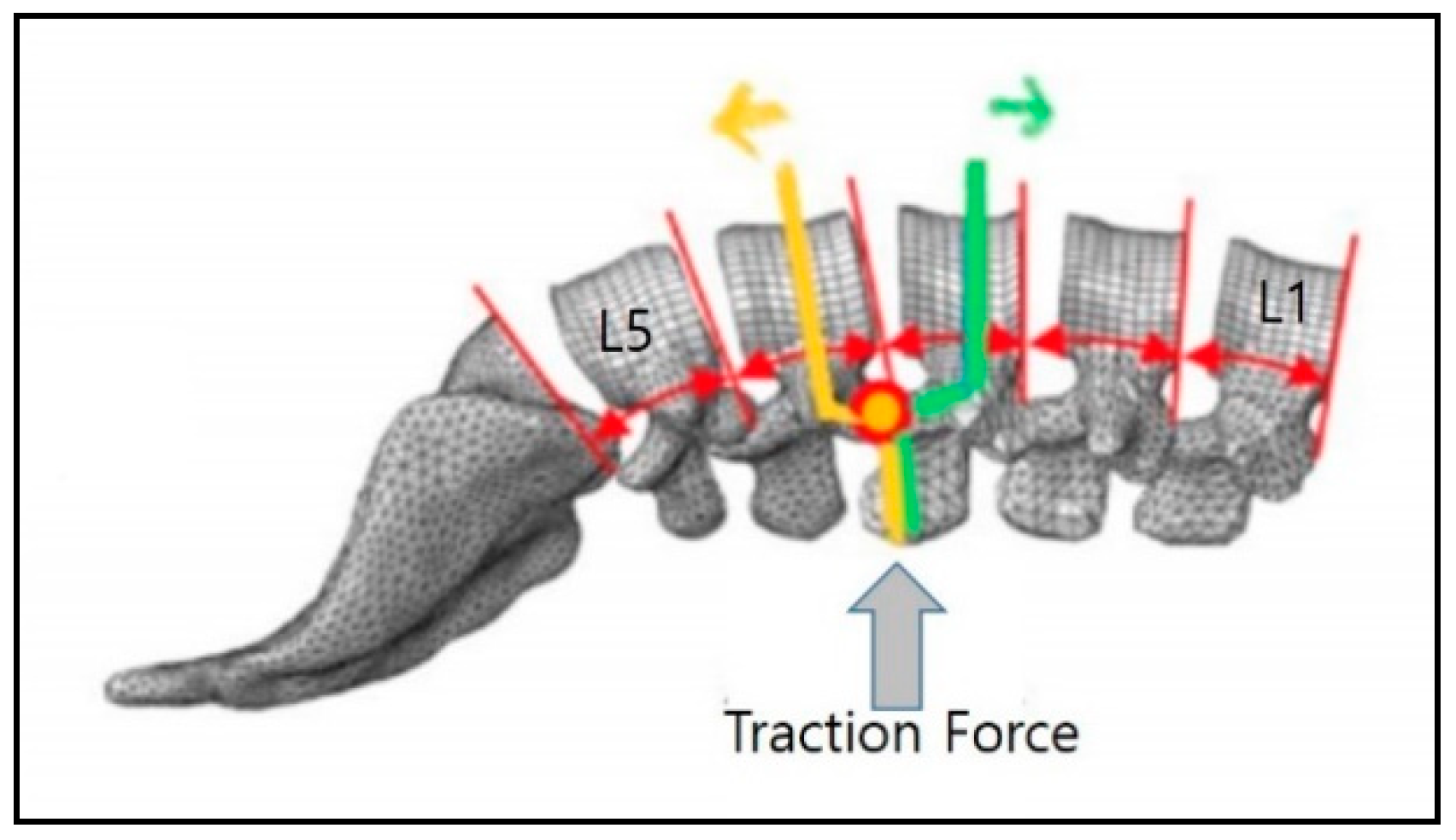
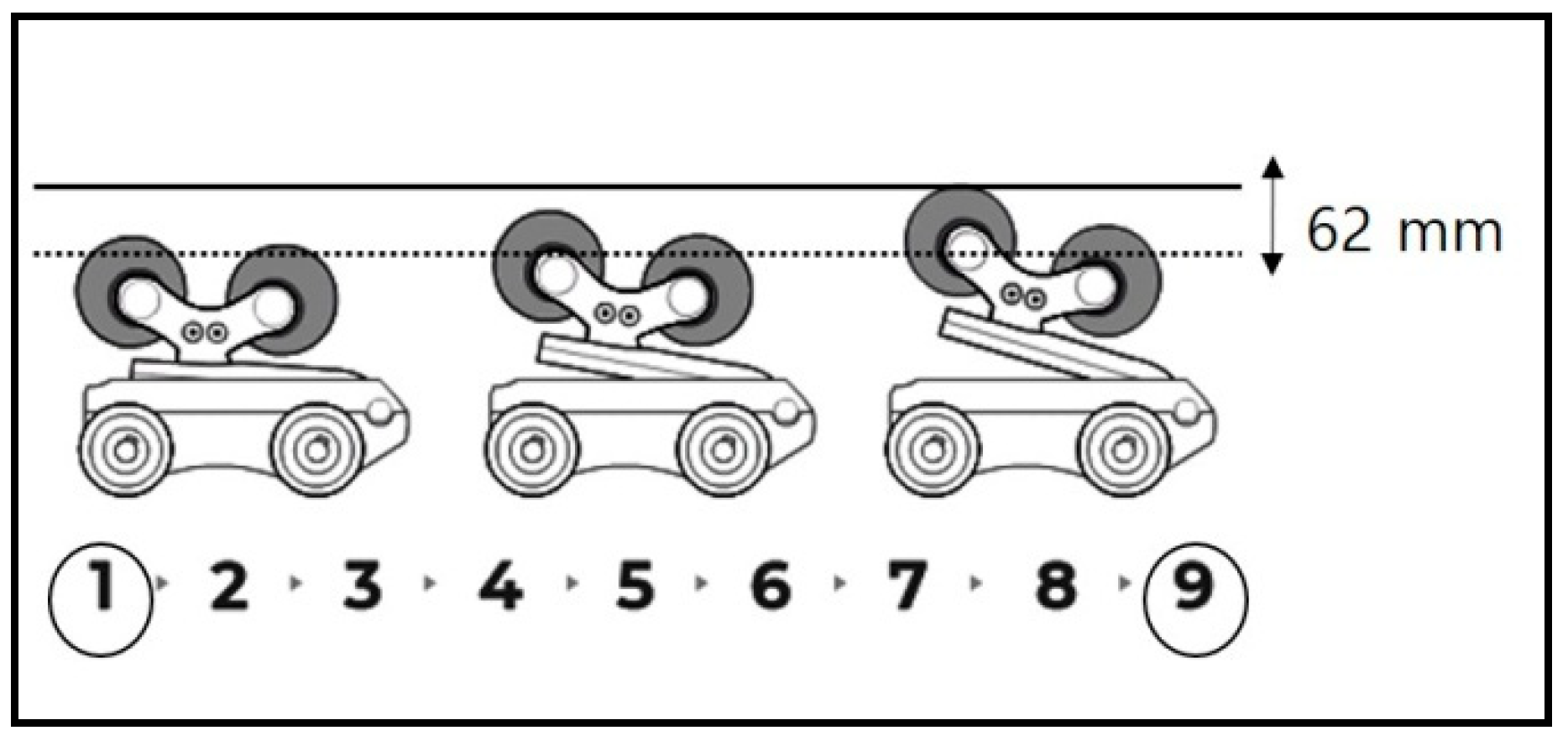
2.2. Measurement Tools and Research Design
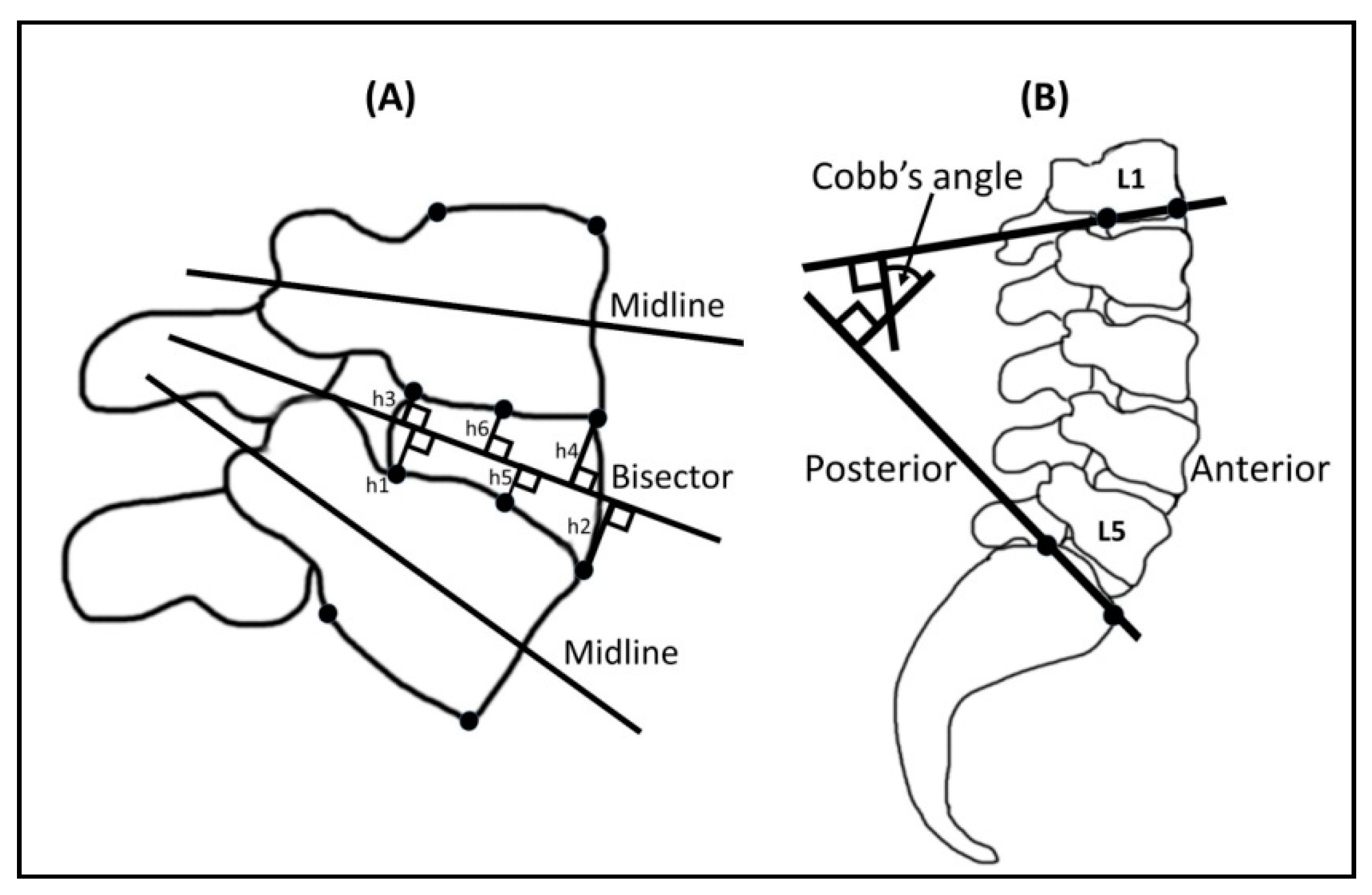
2.3. Measurements of Intervertebral Height and Lumbar Cobb’s Angle under Traction Mode
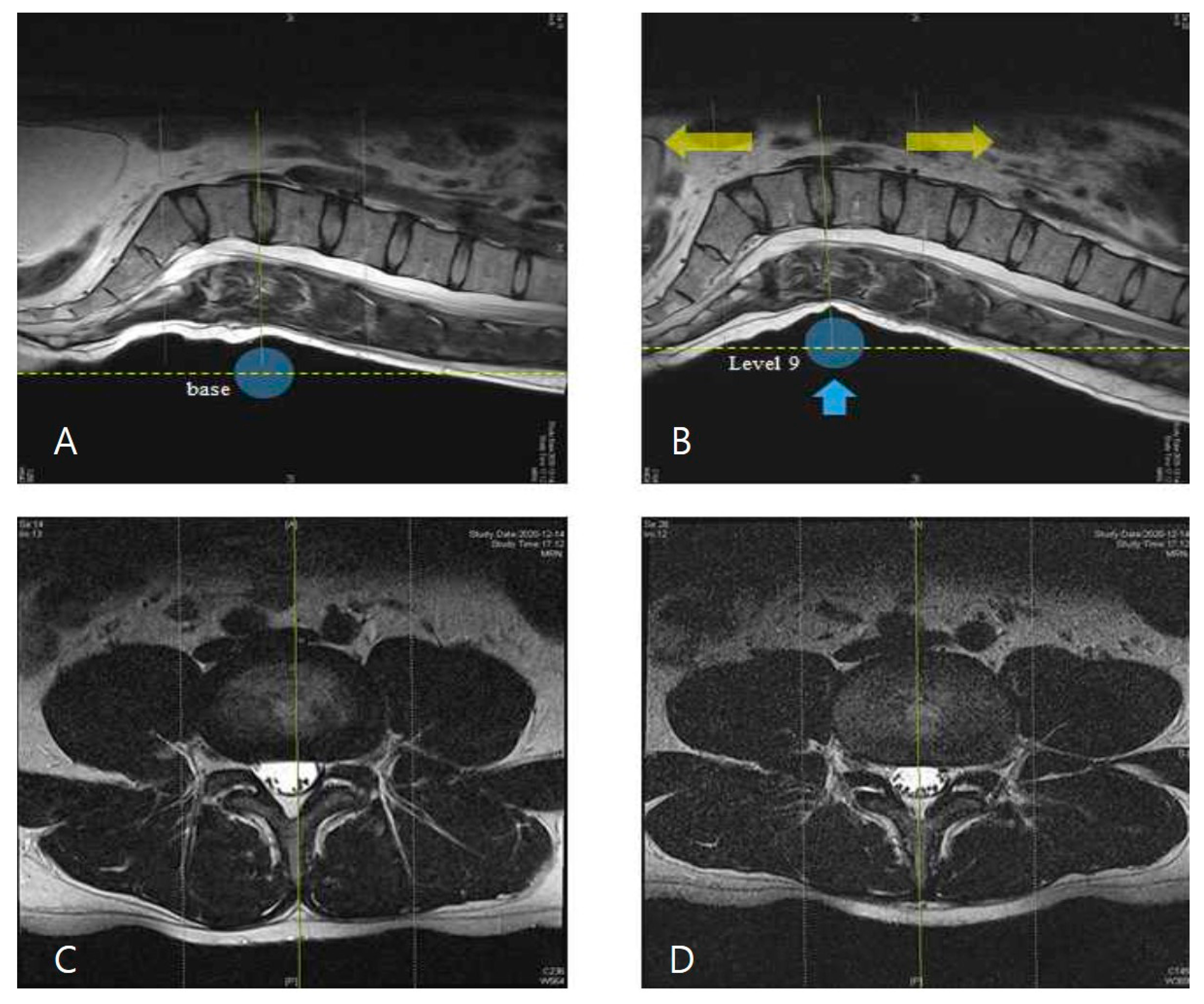
2.4. Morphological Observation of Spinal Structures in Axial View of L4–5 Disc
2.5. Statistics
3. Results
3.1. Changes in Height of the Intervertebral Space in L3–4 and L4–5 Sections between Baseline and Traction Mode
3.2. Changes in Lordotic Curve in L3–4 and L4–5 Sections in Baseline and Traction Mode
3.3. Observation of MR Images of the Central Spinal Canal Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitchell, U.H.; Helgeson, K.; Mintken, P. Physiological effects of physical therapy interventions on lumbar intervertebral discs: A systematic review. Physiother. Theory Pract. 2017, 33, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Farajpour, H.; Jamshidi, N. Effects of different angles of the traction table on lumbar spine ligaments: A finite element study. Clin. Orthop. Surg. 2017, 9, 480–488. [Google Scholar] [CrossRef]
- Brisby, H. Pathology and possible mechanisms of nervous system response to disc degeneration. J. Bone Jt. Surg. Am. 2006, 88, 68–71. [Google Scholar] [CrossRef]
- Kroeber, M.; Unglaub, F.; Guegring, T.; Nerlich, A.; Hadi, T.; Lotz, J.; Carstens, C. Effects of controlled dynamic disc distraction on degenerated intervertebral discs—An in vivo study on the rabbit lumbar spine model. Spine 2005, 30, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Guehring, T.; Omlor, G.W.; Lorenz, H.; Engelleiter, K.; Richter, W.; Carstens, C.; Kroeber, M. Disc distraction shows evidence of regenerative potential in degenerated intervertebral discs as evaluated by protein expression, magnetic resonance imaging, and messenger ribonucleic acid expression analysis. Spine 2006, 31, 1658–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balague, F.; Mannion, A.F.; Pellise, F.; Cedraschi, C. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef] [Green Version]
- Katz, J.N. Lumbar disc disorders and low-back pain: Socioeconomic factors and consequences. J. Bone Jt. Surg. Am. 2006, 88, 21–24. [Google Scholar] [CrossRef]
- Jhun, H.J.; Park, J.Y. Estimated number of korean adults with back pain and population-based associated factors of back pain: Data from the fourth Korea national health and nutrition examination survey. J. Korean Neurosurg. Soc. 2009, 46, 443–450. [Google Scholar] [CrossRef]
- Hestbaek, L.; Leboeuf-Yde, C.; Kyvik, K.O.; Manniche, C. The course of low back pain from adolescence to adulthood: Eight-year follow-up of 9600 twins. Spine 2006, 31, 468–472. [Google Scholar] [CrossRef]
- Pellise, F.; Balague, F.; Rajmil, L.; Cedraschi, C.; Aguirre, M.; Fontecha, C.G.; Pasarin, M.; Ferrer, M. Prevalence of low back pain and its effect on health-related quality of life in adolescents. Arch. Pediatr. Adolesc. Med. 2009, 163, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Stamenkovic, A.; Clark, B.C.; Pidcoe, P.E.; van der Veen, S.M.; France, C.R.; Russ, D.W.; Kinser, P.A.; Thomas, J.S. Distinguishing chronic low back pain in young adults with mild to moderate pain and disability using trunk compliance. Sci. Rep. 2021, 11, 7592. [Google Scholar] [CrossRef]
- Been, E.; Kalichman, L. Lumbar lordosis. Spine J. 2014, 14, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Been, E.; Barash, A.; Marom, A.; Kramer, P.A. Vertebral bodies or discs: Which contributes more to human-like lumbar lordosis? Clin. Orthop. Relat. Res. 2010, 468, 1822–1829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, A.; Chow, D.H.K. Effects of traction on structural properties of degenerated disc using an in vivo rat-tail model. Spine 2010, 35, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Chung, T.S.; Yang, H.E.; Ahn, S.J.; Park, J.H. Herniated lumbar disks: Real-time MR imaging evaluation during continuous traction. Radiology 2015, 275, 755–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krause, M.; Refshauge, K.M.; Dessen, M.; Boland, R. Lumbar spine traction: Evaluation of effects and recommended application for treatment. Man. Ther. 2000, 5, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Onel, D.; Tuzlaci, M.; Sari, H.; Demir, K. Computed tomographic investigation of the effect of traction on lumbar disc herniations. Spine 1989, 14, 82–90. [Google Scholar] [CrossRef]
- Cevik, R.; Bilici, A.; Gur, A.; Sarac, A.J.; Yildiz, H.; Nas, K.; Ceviz, A.; Bukte, Y. Effect of new traction technique of prone position on distraction of lumbar vertebrae and its relation with different application of heating therapy in low back pain. J. Back Musculoskelet. Rehabil. 2007, 20, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Delacerda, F.G. Effect of angle of traction pull on upper trapezius muscle activity. J. Orthop. Sports Phys. Ther. 1980, 1, 205–209. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Heo, S.J.; Park, S.H. The real time geometric effect of a lordotic curve-controlled spinal traction device: A randomized cross over study. Healthcare 2021, 9, 125. [Google Scholar] [CrossRef]
- Ozturk, B.; Gunduz, O.H.; Ozoran, K.; Bostanoglu, S. Effect of continuous lumbar traction on the size of herniated disc material in lumbar disc herniation. Rheumatol. Int. 2006, 26, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Kim, K.E.; Jang, H.Y.; Cho, I.Y. The effectiveness of using a spinal column thermal massage device on muscle pain. J. Korea. Converg. Soc. 2020, 11, 361–368. [Google Scholar] [CrossRef]
- Lee, C.H.; Heo, S.J.; Park, S.H.; Jeong, H.S.; Kim, S.Y. Functional changes in patients and morphological changes in the lumbar intervertebral disc after applying lordotic curve-controlled traction: A double-blind randomized controlled study. Medicina 2019, 56, 4. [Google Scholar] [CrossRef] [Green Version]
- Park, W.M.; Kim, K.; Kim, Y.H. Biomechanical analysis of two-step traction therapy in the lumbar spine. Man. Ther. 2014, 19, 527–533. [Google Scholar] [CrossRef]
- Frobin, W.; Brinckmann, P.; Biggemann, M.; Tillotson, M.; Burton, K. Precision measurement of disc height, vertebral height and sagittal plane displacement from lateral radiographic views of the lumbar spine. Clin. Biomech. 1997, 12, S1–S63. [Google Scholar] [CrossRef]
- Atchison, J.W.; Tolchin, R.B.; Ross, B.S.; Eubanks, J.E. Manipulation, traction and massage. In Branddom’s Physical Medicine and Rehabilitation, 6th ed.; Cifu, D.X., Ed.; Elsevier Saunders: Philadelphia, PA, USA, 2021; pp. 316–337. [Google Scholar]
- Madson, T.J.; Hollman, J.H. Lumbar traction for managing low back pain: A survey of physical therapists in the United States. J. Orthop. Sports Phys. Ther. 2015, 45, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Chow, D.H.K.; Yuen, E.M.K.; Xiao, L.; Leung, M.C.P. Mechanical effects of traction on lumbar intervertebral discs: A magnetic resonance imaging study. Musculoskelet. Sci. Pract. 2017, 29, 78–83. [Google Scholar] [CrossRef]
- Hay, O.; Dar, G.; Abbas, J.; Stein, D.; May, H.; Masharawi, Y.; Peled, N.; Hershkovitz, I. The lumbar lordosis in males and females, revisited. PLoS ONE 2015, 10, e0133685. [Google Scholar] [CrossRef] [Green Version]
- Cobb, J.R. Outline for the study of scoliosis. Instr. Course. Lect. AAOS. 1948, 5, 261–275. [Google Scholar]
- Dawood, R.S.; Kattabei, O.M.; Nasef, S.A.; Battarjee, K.A.; Abdelraouf, O.R. Effectiveness of kinesio taping versus cervical traction on mechanical neck dysfunction. Int. J. Ther. Rehab. Res. 2013, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Oakley, P.A.; Harrison, D.E. Lumbar extension traction alleviates symptoms and facilitates healing of disc herniation/sequestration in 6-weeks, following failed treatment from three previous chiropractors: A CBP((R)) case report with an 8 year follow-up. J. Phys. Ther. Sci. 2017, 29, 2051–2057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moustafa, I.M.; Diab, A.A. Extension traction treatment for patients with discogenic lumbosacral radiculopathy: A randomized controlled trial. Clin. Rehabil. 2013, 27, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Saunders, H.D. Lumbar traction. J. Orthop. Sports Phys. Ther. 1979, 1, 36–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judovich, B.; Nobel, G.R. Traction therapy, a study of resistance forces; preliminary report on a new method of lumbar traction. Am. J. Surg. 1957, 93, 108–114. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria |
|
| Exclusion criteria |
|
| Lumbar Segments | Measurement Location | Baseline (mm) | Traction Mode (mm) | p-Value |
|---|---|---|---|---|
| L3–4 | Anterior | 12.97 ± 1.90 | 14.26 ± 1.42 | <0.001 |
| Central | 12.66 ± 1.53 | 13.30 ± 1.14 | <0.001 | |
| Posterior | 8.80 ± 1.64 | 9.06 ± 1.77 | 0.286 | |
| Average | 11.48 ± 1.27 | 12.21 ± 1.03 | <0.001 | |
| L4–5 | Anterior | 15.01 ± 2.5 | 15.77 ± 2.48 | <0.001 |
| Central | 11.97 ± 1.77 | 12.67 ± 1.61 | <0.01 | |
| Posterior | 7.72 ± 1.64 | 8.19 ± 1.12 | 0.120 | |
| Average | 11.57 ± 1.60 | 12.21 ± 1.39 | <0.001 |
| Variable | Baseline (°) | Traction Mode (°) | p-Value |
|---|---|---|---|
| L3–4 | 53.48 ± 8.21 | 68.55 ± 4.60 | <0.001 |
| L4–5 | 55.17 ± 10.38 | 67.95 ± 5.44 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, Y.-S.; Lee, J.-H.; Lee, M.; Kim, K.-E.; Jang, H.-Y.; Lee, K.-J.; Bajgai, J.; Kim, C.-S.; Cho, I.-Y. Mechanical Changes of the Lumbar Intervertebral Space and Lordotic Angle Caused by Posterior-to-Anterior Traction Using a Spinal Thermal Massage Device in Healthy People. Healthcare 2021, 9, 900. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070900
Yoon Y-S, Lee J-H, Lee M, Kim K-E, Jang H-Y, Lee K-J, Bajgai J, Kim C-S, Cho I-Y. Mechanical Changes of the Lumbar Intervertebral Space and Lordotic Angle Caused by Posterior-to-Anterior Traction Using a Spinal Thermal Massage Device in Healthy People. Healthcare. 2021; 9(7):900. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070900
Chicago/Turabian StyleYoon, Yong-Soon, Jong-Hoo Lee, Mihyun Lee, Ka-Eun Kim, Hong-Young Jang, Kyu-Jae Lee, Johny Bajgai, Cheol-Su Kim, and Il-Young Cho. 2021. "Mechanical Changes of the Lumbar Intervertebral Space and Lordotic Angle Caused by Posterior-to-Anterior Traction Using a Spinal Thermal Massage Device in Healthy People" Healthcare 9, no. 7: 900. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070900