Applications of Electronic-Nose Technologies for Noninvasive Early Detection of Plant, Animal and Human Diseases


Southern Hardwoods Laboratory, Pathology Department, Center for Bottomland Hardwoods Research, Southern Research Station, USDA Forest Service, 432 Stoneville Road, Stoneville, MS 38776, USA
Chemosensors 2018, 6(4), 45; https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors6040045
Submission received: 27 August 2018
/
Revised: 21 September 2018
/
Accepted: 26 September 2018
/
Published: 4 October 2018
(This article belongs to the Special Issue Electronic nose’s, Machine Olfaction and Electronic Tongue’s)
Abstract
:The development of electronic-nose (e-nose) technologies for disease diagnostics was initiated in the biomedical field for detection of biotic (microbial) causes of human diseases during the mid-1980s. The use of e-nose devices for disease-diagnostic applications subsequently was extended to plant and animal hosts through the invention of new gas-sensing instrument types and disease-detection methods with sensor arrays developed and adapted for additional host types and chemical classes of volatile organic compounds (VOCs) closely associated with individual diseases. Considerable progress in animal disease detection using e-noses in combination with metabolomics has been accomplished in the field of veterinary medicine with new important discoveries of biomarker metabolites and aroma profiles for major infectious diseases of livestock, wildlife, and fish from both terrestrial and aquaculture pathology research. Progress in the discovery of new e-nose technologies developed for biomedical applications has exploded with new information and methods for diagnostic sampling and disease detection, identification of key chemical disease biomarkers, improvements in sensor designs, algorithms for discriminant analysis, and greater, more widespread testing of efficacy in clinical trials. This review summarizes progressive advancements in utilizing these specialized gas-sensing devices for numerous diagnostic applications involving noninvasive early detections of plant, animal, and human diseases.
1. Introduction
The development of electronic-nose (e-nose) technologies and devices for disease diagnostic applications has accelerated rapidly over the past decade. The impressive rate of progress in e-nose technological developments, specifically for disease-detection applications, has been achieved largely through discoveries of new electronic methods and associated operational mechanisms for chemical detection of complex gaseous mixtures, primarily consisting of volatile organic compounds (VOCs). Improvements in sensor technologies and arrays, machine-learning methods such as artificial neural networks (ANN), disease-specific reference libraries and databases, data-analysis software, and identification of disease biomarkers also have contributed to advancements in e-nose diagnostic methods [1,2,3,4,5,6,7,8]. These key advances have resulted in numerous new applications of e-nose technologies useful for the detection and identification of diseases with many different causes (biotic, abiotic, and genetic) which occur in various forms of living organisms including plants, animals, and humans [7,9,10]. Applications of e-nose devices for identification of biotic causes of disease primarily involve detection of microbial pathogens on or within diseased organisms [11,12,13].
Electronic-nose devices have been used extensively since the 1980s by a wide range of governmental agencies and commercial industries from aerospace [14,15,16,17], agricultural and forestry [10,13,18,19], biomedical for point-of-care testing (POCT) [8,12,20,21], cosmetics, drug and pharmaceutical [5], environmental protection [18,22,23,24], food science and technologies [12,25,26], to many other specialized uses for biosecurity, disaster operations and recovery, forensics, military operations, regulatory, law enforcement, transportation safety, and for scientific research [5,27]. One of the most important e-nose applications common among various industrial uses has been for quality assurance and quality control (QA/QC). E-nose devices are used to continually evaluate manufacturing processes and methods to measure and maintain the quality of commercial products and to ensure that products and services consistently meet consumer expectations. Assessments of quality controls in manufacturing processes are essential for maintaining product uniformity and consistency for brand recognition and consumer satisfaction [13]. In the biomedical and related drug industries, applications of e-nose devices have increased dramatically over the past decade due to the need for new, simpler and easy to use technologies with the capabilities of providing rapid, noninvasive accurate diagnoses with minimal costs [20].
Electronic-nose devices also are potentially useful for confirming patient identity and determining the necessity for nonreversible, critical medical procedures (e.g., biopsies, corrective surgeries, organ and limb removals, or implantations of devices or prosthetics) applied to specific locations or parts of the human body [28,29]. The greater ease-of-use of e-nose devices by doctors and clinical technicians has made e-nose clinical trials and instrument-training operations simpler, allowing shorter startup times for the development and initiation of electronic nose-based diagnostic clinical applications and procedures.
Chemical studies of disease metabolomics have provided critical information explaining the effects of disease-developmental processes (pathogenesis, mechanisms of disease, and effects on host metabolic processes and pathways) on host pathophysiology which have provided effective chemical clues into the identities (chemical classes) of disease-associated target molecules (chemical biomarkers of disease) most indicative of and strongly correlated with the presence of disease within living organisms [1,6,7,30,31,32]. The widely varying chemical composition of different living organisms affected by disease processes (whether plant, animal, or human host types), has presented unique and different challenges to diagnosticians in using e-nose devices for disease detection.
Most key advances in the development of e-nose instruments and applications for disease diagnostics predominantly have been related to improvements in refining e-nose sensor arrays, development and use of new sensor types (with novel operational mechanisms), pattern recognition algorithms and analysis software, application-specific reference databases, and more effective data-analyses procedures. A recent emerging trend in next-generation disease diagnostics has been the use of e-nose devices for initial preliminary diagnoses, followed by confirmations (if necessary) through detection and identification of key chemical disease biomarkers most correlated with or established as chemical indicators of specific disease states found within a host body. The area of metabolic- chemistry diagnostics known as metabolomics involves the identification and quantification of metabolites found in clinical samples. This area of study is largely responsible for identifying disease biomarkers. Specific chemical biomarkers have been determined for many types of diseases. A short list of disease biomarkers discovered for specific diseases of plant, animal, and human hosts are summarized with particular examples for each disease-type category and biomarker chemical class in Table 1. More details on biomarkers will be covered in Section 2 on Biomarker Metabolite E-nose Signatures. Volatile chemical biomarkers of disease occur in a wide range of chemical classes that generally provide clues to the types of host metabolic pathways affected by individual diseases [7]. Studies in physiopathology attempt to determine the pathways affected by disease in order to understand the precise mechanisms by which unique diagnostic biomarkers are produced.
An important controversy in disease diagnostics, debated among pathologists, diagnosticians, physicians and other healthcare experts, involves determining which technologies are most useful for facilitating the development of more efficient, rapid, and reliable clinical diagnostic procedures for the future. Choices in selecting improved diagnostic technologies must take into account the trend toward newer medical goals of achieving more rapid diagnostic results and effective disease treatment solutions through accelerated clinical procedures, but with cheaper total healthcare costs. Among the two major categories of noninvasive diagnostic technologies being most debated are the use of: (1) sophisticated chemical-analysis instruments and (2) simpler sensor-array type devices (such as e-noses) that do not identify specific chemical components in diagnostic samples. The salient facts and details of viewpoints and arguments surrounding this debate will be considered here based on new research findings. The ultimate aim for determining which new technologies are likely to improve on disease diagnostic methods and procedures is to ascertain which approaches are most likely to meet the needs and progressive goals of modern medical services.
The development of disease-detection methodologies utilizing e-nose devices requires a thorough understanding of host physiology and metabolic pathways affected by disease processes, different mechanisms of disease caused by biotic and abiotic causal agents, and chemical classes of abnormal VOCs released due to effects of pathogenesis on host metabolisms. These unique characteristics of host-pathogen chemical interactions are considered and explored for each type of living host (plants, animals, and humans) to provide details and examples of how e-nose devices have been modified and developed specifically as diagnostic tools for different host-disease systems. This approach takes into account the particular chemical nature of disease interactions in living organisms that vary depending on the unique biochemical characteristics of the host and those of disease etiological (causal) agents. Knowledge of specific gaseous mixtures of VOCs produced in association with individual hosts in response to different disease types and processes provides essential information about target compounds (often referred to as chemical disease biomarkers) needed for developing the most effective approaches for e-nose disease detection.
This review provides a detailed summary of recent electronic-nose technologies developed over the past decade for specific applications in detecting and diagnosing diseases found in plant, animal, and human living hosts. The literature search strategy adopted for this review was based on selection criteria that are different from those specified by preferred reporting items for systematic reviews and meta-analyses (PRISMA) or quality of reporting of meta-analysis (QUOROM) guidelines. The use of these particular guidelines, relevant to reviews of diagnostic practices, are designed to provide information for evaluating the safety, risks, benefits, efficacy, and potential harm or adverse effects associated with the use of medical procedures, diagnostic methods, results or conclusions drawn from research studies. Reporting such information is beyond the scope and objectives of this review because of the potential for introducing bias in implied judgments of the significance or potential usefulness of discoveries and in recognizing the inherent value of scientific contributions. For these reasons, the author has selected papers for inclusion and reported information based on objective criteria indicative of the absolute scientific value of presented information, including usefulness of individual papers in: (1) providing new information relating to the full-range of e-nose detection methods and techniques available, (2) offering new concepts associated with disease diagnostics and theory relating to disease detection, (3) indicating potential improvements on existing diagnostic methods, and (4) summarizing new (recent) potential applications for clinical diagnosis of diseases, particularly those not previously treated or covered in the literature.
2. Biomarker Metabolite Electronic-Nose Signatures
Most forms of human cancers, and other terminal illnesses, often are detected in advanced stages of the disease, resulting in poor patient survival rates. Consequently, there is an imminent need for the development of prophylactic disease-screening procedures that provide means for detecting major life-threatening diseases at early stages of disease development [8,21]. There is a growing trend over the past decade to develop dual approaches to disease diagnostics that utilize more rapid disease-screening methods (e.g., electronic chemical sensors or sensor arrays) in combination with procedures based on the detection of disease-specific chemical biomarkers to confirm diagnoses [7,43,44]. Diagnostic clinical procedures allowing efficient, noninvasive, painless, and affordable disease-screenings with high specificity and sensitivity are essential for achieving effective disease prevention. In order for early disease-detection systems to be possible, specific and effective chemical biomarkers, most highly correlated with disease incidence, must to be identified for individual diseases and detected at early presymptomatic stages of pathogenesis within complex headspace volatiles (VOC-metabolite mixtures) derived from diagnostic samples obtained from diseased individuals.
A recent study of urinary VOC headspace metabolites associated with head and neck cancer (HNC) patients was performed using headspace solid phase microextraction (SPME) coupled to gas chromatography mass spectrometry (GC–MS) to identify and characterize urinary VOC alterations specific to HNC [45]. Univariate and multivariate statistical analyses revealed 28 metabolites with highest contribution towards discrimination of HNC patients from healthy controls. Furthermore, four VOC metabolites in the urine headspace volatile profile, including 2,6-dimethyl-7-octen-2-ol, 1-butanol, p-xylene and 4-methyl-2-heptanone, were identified as possible chemical biomarker metabolites with highest sensitivity and specificity to HNC. This information provided biochemical clues to several dysregulated metabolic pathways in HNC patients which could potentially help unravel novel mechanistic insights into HNC-disease pathophysiology by improving understanding of HNC disease mechanisms to facilitate non-invasive biomarker-based approaches to HNC diagnosis. The development of rapid analytical strategies for detecting and identifying urine and other disease biomarkers, including determining limits of detection and limits of quantification of potential biomarkers, have played a vital role in research, discovery and confirmation of biomarker metabolites most associated with specific diseases [46]. The identification of tumor-specific VOC emission signatures from clinical samples of diseased patients has increased significantly in recent years due to studies focusing on the development of a cancer-characteristic “odor fingerprints”. This work has been conducted through application of sensorial or senso-instrumental analyses that chemically characterize associated complex headspace VOC mixtures of biological fluids, such as to identify prostate cancer (PCa)-specific biomarkers in urine, to improve on traditional diagnostic procedures. [47].
The search for improved, more rapid and effective methods for accurate disease diagnoses have led many researchers, physicians, and diagnosticians toward two newer approaches to disease diagnostics for clinical POCT that differ considerably from conventional diagnostic methods that utilize expensive time-consuming laboratory tests [7,8]. These two major approaches involve the use of electronic-nose devices and metabolomic analyses. Recent reviews summarized the advantages and disadvantages of e-nose vs. metabolomics approaches to disease diagnostics [7,44]. Metabolomics, relative to disease diagnostics, involves the study of changes in the composition and concentrations of cellular volatile and nonvolatile, primary and secondary metabolites produced as a result of disease processes (pathogenesis). Metabolomic methods, such as proton and carbon nuclear magnetic resonance (NMR) spectroscopy, are used to determine the precise chemical composition and quantitation of components present in diagnostic clinical samples, including identifying disease-specific chemical VOC-biomarkers.
Studies of animal and human pulmonary diseases have identified potential biomarkers from analyses of VOC profiles in exhaled breath which may be used to determine the cause of specific diseases and improve the accuracy of disease diagnostic processes for pneumonia and other respiratory diseases [48]. A summary of metabolomic data collected from several studies on pneumonia showed the same consistent VOCs with changes in concentrations of healthy vs. diseased patients based on VOC profiles based on breathomics. The study of ‘breathomics’ involves the analysis of VOCs in exhaled breath that result from cellular metabolism. Analyses of the exhaled breath of pneumonia vs. healthy patients indicated consistent increases or decreases in twenty-five VOCs derived from eleven chemical classes [49,50,51,52]. Although the occurrence of changes in levels or concentrations of VOCs were consistent, the direction of change was not always consistent. Some volatile metabolites increased or decreased in concentration within the breath of pneumonia patients compared to healthy patients, but the involvement of the same VOCs indicated effects on certain metabolic pathways.
Different types of chemical biomarkers are produced that may serve as indicators or evidence of specific disease. Disease biomarkers have been classified by different classification systems that generally base the chemical biomarker type on the origin of the chemical species being detected. The highest hierarchical categories of chemical biomarkers are divided into two primary groups. The endogenous biomarkers include those that originate from within the body and are formed from either normal physiological processes or from abnormal metabolic processes caused by disease. Exogenous biomarkers originate from sources outside of the body and enter the body through inhalation, ingestion, absorption through the skin, or by some other means [7,8]. Endogenous biomarkers may be subdivided into additional categories including disease-predisposition biomarkers, disease biomarkers, pathogen biomarkers, and gut-microbiome (microflora) biomarkers [7]. Exogenous biomarkers generally are not considered direct indicators of infectious diseases, but may potentially serve as predisposition indicators of disease [53,54].
A recent analysis of chemical biomarkers produced by the six most frequent pathogenic bacteria causing human sepsis, including Staphylococcus aureus, Streptococcus pneumoniae, Enterococcus faecalis, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli, indicated that specific VOCs could be used as potential biological markers to diagnose sepsis in critically ill patients [1]. A systematic review revealed that all six bacteria produced specific VOCs (in common) such as isopentanol, formaldehyde, methyl mercaptan, and trimethylamine. Although humans do not produce these VOCs, they are of microbial origin (pathogen biomarkers) and serve as sepsis-indicative chemical markers for these six bacterial pathogens. Other different types of volatile biomarkers were found to be useful for identifying and discriminating between each bacterial species: (1) isovaleric acid and 2-methylbutanal for Staphylococcus aureus; (2) 1-undecene, 2,4-dimethyl-1-heptane, 2-butanone, 4-methylquinazoline, hydrogen cyanide, and methyl thiocyanide for Pseudomonas aeruginosa; and (3) methanol, pentanol, ethyl acetate, and indole for Escherichia coli.
3. Electronic-Nose Detection of Biotic Diseases
Most electronic-nose devices do not have the capability of identifying or quantifying individual VOCs present in complex gaseous mixtures [9]. Nevertheless, e-nose devices have been used to identify individual VOCs in simple mixtures and provide many advantages over complex analytical instruments because they are easily operated at relatively low costs, have rapidly responding sensor arrays with fast recoveries after analysis, good precision, and the flexibility of detecting a very large variety of VOCs from many different chemical classes. A large number of e-nose instruments have been developed based on a wide range of operating (VOC sensor-detection) principles [5,6]. Sensor responses from an e-nose sensor array are digitally translated by a transducer to generate a characteristic response pattern (for all VOCs present in sample headspace) that indicates the source of the volatile chemical emissions when compared to reference databases of response patterns from known sample types [5,10,55]. Thus, differences in VOCs compositions are indicated by unique e-nose profiles, which may be compared to the overall variation of a pool of reference gas samples.
Electronic-nose technologies previously have been developed for numerous applications in a wide range of fields, including human and animal diagnostics, food quality, and environmental safety [5,26,56,57]. More recent uses of e-nose instruments in agriculture, botany, forestry and related plant sciences have included plant and cultivar identification, wood identification, and detection of pesticide residuals on the foliage of crop plants [13,19,22,23,24,58]. Additionally, e-noses have been tested for diagnostic applications on a wide variety of plant pathosystems with excellent performances comparable to GC-MS in terms of efficacy while requiring lower analytical and post-analysis time and with lower operating costs [9]. The e-nose methods developed and used for diagnosis of diseases in plant hosts vary significantly from the methods used for detection of human and animal diseases. For example, methods of sample preparation and analysis required for e-nose detection of plant diseases are significantly different due to structural and chemical differences in plant cell components within plant tissue samples.
3.1. Plant Disease Detection
Conventional methods used for disease diagnosis in plants have been based on host symptomology, pathogen morphology (direct microscopic identification), serological tests, and disease-associated metabolic assays [59,60,61]. These approaches are not sufficient or useful for disease detection and identification when disease-associated symptoms occur in late phases of infection (pathogenesis), pathogen identification is difficult, or when curative disease-control treatments are largely ineffective [62,63]. Molecular techniques for direct detection of pathogens by their intra- or extra-genomic DNA-sequences, such as polymerase chain reaction (PCR) for DNA-amplification followed by sequencing, have been widely adopted internationally to achieve early diagnosis from plant materials independently of host symptomology. Polymerase chain reaction has been recognized universally as a well-established, often first method of choice for relatively quick diagnoses of numerous plant and animal diseases largely because of the very large number of known DNA sequences now available from GenBank at the National Center for Biotechnology Information (NCBI), and other genetic sequence databases, for identification of specific pathogens associated with known biotic diseases. Pathogen-specific detection by PCR and DNA sequencing is possible due to the high specificity of the method, high sensitivity (achievable due to pathogen DNA-amplification), and low operational costs now possible due to robotics, high throughput DNA-sequencing apparati available, and associated automatization [59]. However, there are a number of drawbacks to PCR such as: (1) requirements for the design and validation of PCR-primers for targeted DNA sequences of specific phytopathogens, (2) the unavailability of reference DNA sequences for certain pathogens, (3) insufficient pathogen template DNA available at early stages of infection (requiring high host tissue-sampling rates), (4) devising effective pathogen DNA-extraction methods for isolation from host tissue, (5) involves destructive sampling of host tissue with potential associated economic losses (impacts on crop salability), particularly if for post-harvest products (crops), (6) DNA-detection (especially with quantitative, qPCR) does not necessarily indicate that the pathogen is alive within a host (it is a non-viability test of pathogen DNA presence), and (7) many steps in PCR can potentially fail to amplify pathogen DNA (precluding the yield of a product for sequencing), and (8) the always ubiquitous and numerous opportunities for contamination of diagnostic samples (from many sources prior to PCR) may invalidate the results; all of which can preclude effective diagnosis. These limitations have prompted pathologists and diagnosticians to look for other diagnostic tools and methods with different, non-DNA-dependent approaches to disease detection that are noninvasive (do not require destructive sampling).
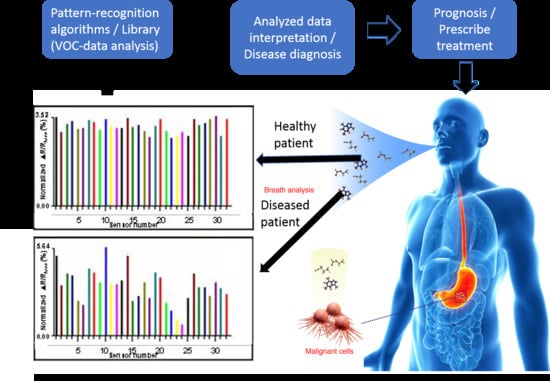
New alternative methods for early diagnosis of plant diseases, besides the often cumbersome traditional molecular techniques, have been developed to improve, simplify, increase effectiveness of early detection, and minimize damage to sampled plant material. Many alternative methods of disease detection have been reviewed previously [59,64,65]. Electronic-nose devises are particularly well suited for noninvasive early disease detection due to their low cost, high precision, and sensitivity to precise complex mixtures of VOCs [6,44]. E-nose detection of gaseous emissions, containing abnormal VOCs released from diseased host tissues (in sampled headspace), provide opportunities for effective noninvasive detection of specific diseases that have been previously correlated and closely associated with the production of particular combinations of volatile metabolites. Aroma signature databases of different plant sample types (healthy vs. diseased), contained within reference libraries of e-nose instruments, are generated from prior analysis of known clinical samples of specific host plants (usually from particular healthy or diseased plant parts—i.e., from roots, stems, leaves, flower or other reproductive parts) using neural net or similar training algorithms. These signature (VOC-profile) databases consist of diagnostic patterns produced from the collective multisensory array outputs assembled together to form a signature smellprint pattern with the outputs of each sensor type usually represented by a bar graph [10]. The strength or intensity of each sensor response (from the sensor array), represented by the smellprint pattern, is determined by the collective effects of all VOC components within the sampled headspace. Validation of e-nose training databases of known sample types in reference libraries, using samples not used for training, is required to assure that classification algorithms provide effective sample discriminations [66,67].
The main advantages of using e-nose instruments and methods for early disease detections are that these allow for: (1) noninvasive (nondestructive) diagnostic sampling, (2) disease detection in bulk host samples, (3) capabilities of detecting multiple diseases, (4) levels of detection can be adjusted (through training and specification of discrimination levels), (5) sensor array selection for targeting specific classes of disease-associated VOCs being detected, and (6) multiple classes of pathogens may be detected using different reference databases with the same e-nose instrument [9]. The key characteristics of e-nose devices which make them advantageous to disease-diagnostic applications are portability, affordability, ease of use (with relatively minimal training), and effectiveness in detecting, identifying and classifying the types and digital signature patterns of complex VOC mixtures released from tissues of specific living (organic) sources without identifying individual chemical species in diagnostic sample [10,44].
Initial investigations to assess biochemical changes in plant physiology associated with disease have involved studying changes in VOC-emissions of fruit and vegetable crop plants using GC-MS [34,62,68,69,70,71,72,73,74,75,76]. These studies were done with metabolomics analyses to assess both qualitative and quantitative changes in specific volatile metabolites of diseased plants compared with healthy plants. This work also included searches for specific chemical biomarkers compounds that may be indicative of specific diseases.
Research investigating changes in plant VOC-emissions associated with plant diseases eventually led to a new approach of collective-VOC analysis (of all volatile metabolites released from diseased plant parts) using sensor arrays in electronic-nose devices. The first pioneering work to demonstrate applications of e-nose devices and methods for detection of plant diseases was done based on research of root and bole-rot fungi that cause diseases and decays of forest and landscape trees and other woody plants [10,77]. Part of this initial work required developing the capabilities of discriminating between volatiles from different species of plant hosts because host volatiles are essential background VOC components present in addition to abnormal VOCs produce from pathogens themselves and host-induced plant volatiles produced as a result of disease [19]. The importance of maintaining low relative humidity (RH) in sampling air was found to be a key requirement for effective e-nose detection and discriminations of headspace VOCs from different sample types. This work eventually led to investigations of e-nose plant disease detection in woody, small fruit and vine plants (blueberries, kiwis, grapes), herbaceous fruits (strawberries, pineberry), vegetables (potatoes, onions, carrots), and field crop plants (corn, wheat, barley, cotton). An abbreviated list of a wide variety of plant disease types detected using e-nose devices in various plant hosts are summarized in Table 2. The e-nose applications developed for detection of individual diseases are organized based on an alphabetical listing of plant hosts by common name. Some additional information provided includes the plant part or location where the disease occurs on the host, the name of the disease, the pathogen or pest known to cause the disease, the e-nose model (along with type and number of sensors within the sensor array) used for disease detection, individual references documenting these results. A number of variable factors may affect the performance and effectiveness of e-nose discriminations in plant disease diagnoses. Some of the most important sources of variability in VOC profiles include RH of sampling air, type of background VOCs that may enter into sampling air, level of disease severity, age of plant and disease tissues sampled, plant physiological states, environmental factors affecting VOC emissions (light, temperature, humidity, photoperiod), and occurrence of secondary opportunistic microbes and infections. The VOC profiles of biological samples change and constantly evolve over time as a result of natural ageing processes, plant hormone levels, and plant physiological activities [9]. The simplest, natural plant hormone (ethylene), which regulates many plant physiological activities, controls the release of many plant VOC emissions associated with fruit ripening, senescence, abscission, and host-defense metabolic pathways [26,78,79]. Factors that affect leaf stomatal closure also may affect the plant’s VOCs profile [80].
Some key VOCs induced in plants due to microbial exposure to plant growth-promoting fungi (PGPF) and plant pathogens may result in the induction of systemic resistance to specific plant diseases and corresponding concomitant changes in the physiology of the entire plant. Previous studies have shown that VOC mixtures emitted from Ampelomyces sp. and Cladosporium sp. (potential fungal biocontrol agents) significantly reduced disease severity in Arabidopsis plants against the bacterial plant pathogen Pseudomonas syringae pv. tomato [110]. Two VOCs, m-cresol and methyl benzoate, were identified as major active VOCs of Ampelomyces sp. and Cladosporium sp., respectively, that elicited induction of systemic resistance against the pathogen. Systemic resistance-induced defense-associated VOCs significantly affect the VOC signature of diseased plants compared with diseased plants that lack the systemic PGPF-induced resistance response. Volatile plant defense and protective compounds include terpenoids, essential oils, plant hormones, secondary metabolites as well as other metabolic byproducts, and compounds associated with cell damage [68,111,112,113].
3.2. Animal Disease Detection
The volatilome is defined as the entire set of VOCs produced by an organism, including animals and higher vertebrates with complex metabolic processes that occur in various complex organs and tissue systems [114]. The unique metabolic state of an organism, whether it is healthy or diseased, is constantly changing, but is always reflected by the current accumulation of VOC-metabolites present inside and continually released from the body to the outside through various excretory processes. Scientists are developing e-nose technologies to non-invasively detect VOCs present in clinical samples for purposes of medical diagnoses, disease monitoring, patient therapeutic recovery, disease outbreak containment, and disease prevention. Thus, the analysis of volatilomic omissions from animals, using gas-sensor arrays within e-nose instruments, provides an effective means of detecting disease states in animals just as effectively as in higher mammals and humans.
Measured differences in concentrations of several specific VOC-metabolites previously have been used in metabolomic studies with complex statistical models to discriminate between healthy and diseased states within individuals. The advantages and disadvantages of using e-noses vs. metabolomics in disease detection have been reviewed previously [44]. An important relevant inquiry regarding the use of e-nose devices for this purpose, rather than metabolomics instruments, is whether e-nose devices can be developed with sensor arrays capable of sensing differences or changes in concentrations of only one or a few specific VOCs, particularly principal components of complex headspace volatile mixtures which might serve as potential disease biomarkers. Traditionally-defined e-nose devices provide only semi-quantitative indications of total collective VOC concentration variations by proportional changes in sensor-output intensity responses (from sensor arrays) to all VOCs present in sample analytes. If some sensors in the array are particularly sensitive to one or more individual VOCs present in the sample, then the output pattern from the sensor array can vary substantially. E-nose designers can take advantage of this fact by selecting sensors for the sensor array (from a large library of available sensors) that are most sensitive to known healthy or disease-specific VOC-biomarkers from very specific chemical classes. Consequently, e-nose sensor arrays can be made capable of detecting changes in concentrations of specific types of VOCs due to recordable changes in the molar ratios and concentrations of VOC constituents in the gas sample analyzed [10]. Cumulative or collective differences in several major component VOCs and significant biomarkers of disease vs. healthy states are accordingly measurable in VOC profiles and smellprint patterns of conventional e-nose instrument outputs.
Other strategies are available for developing and using e-nose instruments having greater capabilities of measuring changes or differences in VOC concentrations between sample types, similar to metabolomic instruments. E-nose instruments may be used in tandem with metabolomic instruments targeted to detect specific known VOC-biomarkers as was recently proposed [44]. Newer generation e-nose instruments, having a much small number of sensors, rather than a sensor array, are now available for identifying and quantifying individual potential biomarkers for disease diagnoses. These instrument types are described in Section 3.3. Combination-technology and dual-technology e-nose devices that provide similar chemical-identification data are covered in more detail in Section 4. Future e-nose technologies for improved disease diagnostics.
The recent use of e-nose technologies and devices in veterinary medicine for the detection of animal diseases has aided in the diagnosis of diseases of great importance and significance in both domesticated animals and wildlife, particularly because many animal diseases are caused by very similar or identical pathogens to those that cause related human diseases and therefore the methods useful for early disease detection are quite similar to comparable diseases in humans. Electronic-nose devices have been used to detect different types of diseases in a wide diversity of animal species including tuberculosis (TB) in badgers and cattle, white-nose syndrome (WNS) in bats, and cutaneous myiasis (CM) in sheep as presented in Table 3. Tuberculosis is an example of an exceptionally important disease that occurs worldwide and affects a wide variety of wild animal species such as badgers, birds, deer, possums, rodents, reptiles, various wild carnivores (foxes and coyotes) and omnivores (common brushtail possum, mustelids and rodents) [115,116,117]. Previous attempts at eradicating bovine TB (caused by Mycobacterium bovis) in New Zealand cattle and deer herds was relatively successful, but eradication treatments in the Great Britain have been only marginally successful [118,119,120]. Tuberculosis was widespread in the U.S. among captive elephants in 2015 due to purported transmission from humans by reverse zoonosis. Because TB microbes can be transmitted through the air to infect both humans and animals, there is public health concern for high-hazard zones for TB infections in circuses and zoos [121,122]. Bovine TB also causes a chronic infectious disease in several domesticated mammalian hosts, including cattle, pigs, and house cats, but rarely affects equids (horses, donkeys, and zebras) or sheep [123,124]. Besides transmission by direct contact with excreta of an infected animal, TB pathogens also may be transmitted in water droplets from exhaled air, sputum, urine, feces and pus through inhalation of aerosols.
Tuberculosis is an infectious disease caused by Mycobacteria (Mycobacterium species) which are classified as mycoplasmas, characterized as prokaryotes that do not have cell walls and are therefore not susceptible to cell wall-acting antibiotics such as Beta lactams (e.g., penicillin, cephalosporins etc.) with modes of action that inhibit bacterial cell wall biosynthesis. Consequently, TB generally is considered a consumptive disease due to its persistence and difficulty of control with traditional antibiotics. The term “consumptive” refers to the common loss of body weight in the infected host over time as the disease runs its course and continues to cause damage to affected tissues, eventually leading to the shutdown of organs in the body if not controlled by an effective treatment [123]. Tuberculosis infections usually warrant pre-symptomatic treatment when detected early by e-nose devices or other diagnostic methods. Antibiotics that have been used specifically for control of TB through inhibition of growth causing death of mycobacterial pathogens. Streptomycin, the most effective secondary metabolite antibiotic derived from an Actinobacteria species (Streptomyces griseus), was first used as a cure for TB in 1946. Streptomycin is often given together with isoniazid, rifampicin, and pyrazinamide for more effective TB control [125].
The Mycobacterium tuberculosis complex (MTBC) of species includes four other TB-causing mycobacteria (in addition to M. tuberculosis) in humans including M. africanum, M. bovis, M. canetti, and M. microti [135]. Mycobacterium africanum is a significant cause of TB only in certain regions of Africa [136,137]. Mycobacterium tuberculosis rarely occurs in wild animals [138]. Mycobacterium bovis was previously a very common and major cause of TB in developed countries, but this health problem was almost completely eliminated, except in developing countries, with the introduction of pasteurized milk, precluding bovine to human transmission via consumption of M. bovis-contaminated milk [139,140]. Mycobacterium canetti rarely causes TB within the limited southern geographical region of the Horn of Africa, although some cases also occur in African emigrants [141,142]. Mycobacterium microti also rarely causes TB and it primarily occurs only in immunodeficient people, especially those with human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS), although its prevalence may be significantly underestimated [143].
The highest risk factors of TB in humans are malnutrition, high population densities, and HIV. Other known pathogenic mycobacteria include M. leprae, M. avium, and M. kansasii. Mycobacterium leprae causes leprosy whereas the latter two species are classified as “nontuberculous mycobacteria” (NTM) that neither cause TB nor leprosy, but they are capable of causing lung diseases that resemble TB [144].
Attempts at diagnosing active tuberculosis based on signs and symptoms alone or in patients who have a weakened immune system is difficult [145,146,147]. Initial evaluations of potential TB infections in individuals with signs or symptoms of lung disease usually involve a chest X-ray and multiple sputum cultures for acid-fast bacilli with a definitive diagnosis indicated by identifying M. tuberculosis in a clinical sample (e.g., sputum, pus, or a tissue biopsy), although the culturing process is slow and may take 2-6 weeks [146,148]. Consequently, treatment is normally begun before cultures are confirmed to avoid unnecessary risks of no treatment [149]. Polymerase chain reaction and adenosine deaminase testing, although not routinely recommended, may allow rapid TB diagnosis, but these tests rarely alter how a patient is treated [145,149]. Detection of TB-antibody production using blood tests usually are not recommended [150]. Other tests such as Interferon-γ release assays and tuberculin skin tests are of limited use in the developing world [147,151,152]. All of these methods of TB-detection have considerable limitations due to the long time requirements for determinations and confirmations of diagnosis. The need for early, more rapid detection methods became obvious and the early developments of noninvasive e-nose devises arrived fortuitously at the right time.
E-nose instruments, utilized hitherto for early diagnosis of TB, caused by M. bovis, in badgers and cattle contained sensor arrays, consisted of a conducting polymer (CP) and gold nanoparticle (GNP) sensor arrays, respectively [37,126,131]. In both cases, the instruments detected unique mixtures of VOC-metabolites characteristic of the disease in different animal species. Blood serum empirically was found to be most useful for detecting TB detection in badgers and cattle using the Bloodhound BH-114 e-nose with 14 CP sensors. By contrast, VOCs in exhaled breath samples were the preferred sample types used in the diagnosis of TB in cattle using the Nano Artificial NOSE (NA-NOSE) with six gold nanoparticle (GNP) sensors. Other wildlife diseases such as WNS in bats, ALS in rats, and CM in sheep were preferentially detected in headspace volatiles from either culture, breath, or skin VOC samples, respectively, using e-noses with metal oxide semiconductor (MOS) sensor arrays [127,128,133,134]. The clinical sample types best suitable for e-nose detection of disease related volatiles depend on the nature of the pathogen, the classes and volatility of organic compounds produced, the host metabolic pathways affected, and the ease with which disease-associated VOCs are translocated and concentrated in different parts of the body.
The discovery of disease biomarkers in veterinary and aquaculture sciences has facilitated diagnosis of animal diseases and provided clues to the identity of possible biomarkers of similar diseases in humans [44]. Research in the field of veterinary medicine has been credited with the identification of new potential disease biomarkers of bovine TB disease. Peled et al. [37] analyzed VOCs in breath samples of healthy (TB-negative) and M. bovis-infected (TB-positive) cattle based on GC-MS and e-nose signature patterns. They utilized a nanotechnology-based on an e-nose sensor array, an artificial olfactory system called the NA-NOSE, tailored for detection of TB disease from exhaled breath. The NA-NOSE correctly identified and discriminated between cattle naturally infected with M. bovis and 79% of TB-negative animals. Three potential VOC-biomarkers for bovine TB were identified by GC-MS, including 2,2-dimethylundecane, octadecanoic acid, and hexadecanoic acid [37]. In addition, nonanal appeared to be a strong, relatively abundant VOC-metabolite produced by uninfected cattle, indicative of a healthy metabolism. Profile analysis of headspace VOCs from cattle serum samples previously was used to distinguish between diseased cattle infected with Brucella, (MAP), and M. bovis using an e-nose [126,153]. Tuberculosis also has been detected in humans by breath analysis of VOCs with some success [154,155]. A study by du Preez and Loots [156] provided evidence that TB-detection could be accomplished based on detection of tentative VOC-biomarkers in four chemical classes including amino sugars, monosaccharides, sugar alcohols, and glycoside derivatives. Bruins et al. [157] detected TB in humans by analysis of exhaled breath with a DiagNose e-nose that contained a sensor array with 12 MOS sensors.
Disease biomarkers identified for catfish, livestock, and several wildlife diseases may facilitate e-nose early disease detections in aquatic and terrestrial environments [37,126,127,128,129,130,131,134]. The discovery of geosmin (1,10-trans-dimethyl-trans-(9)-decanol) and 2-methylisoborneol (MIB), VOC-biomarker secondary metabolites associated with systemic infection of live catfish by aquatic Actinobacteria, were determined to be the main VOCs present or absent in the headspace of raw skinless catfish flesh [158,159]. These effective VOC-biomarker detections were found to be responsible for the effective e-nose discriminations between “off-flavor” and “good-flavor” catfish meat fillets [129].
3.3. Human Disease Detection
A variety of e-nose technology types have been used for detection of a wide range of human diseases which are summarized in Table 4. The e-nose instrument types most frequently tested for diagnostic applications in detecting human diseases include devices with carbon black polymer composite (CBPC), CP, electrochemical sensor (EC), MOS, GNP, and quartz crystal microbalance (QMB) sensor arrays. Some non-traditional newer technology types investigated for used in human disease diagnoses have included field asymmetric ion mobility spectroscopy (FAIMS); ion molecule reaction-mass spectrometry (IMR-MS), ion mobility spectrometry (IMS), non-dispersive infra-red (NDIR) and photo-ionization detector (PID) instruments that do not contain multisensory arrays.
The Cyranose 320 (C320) e-nose (Sensigent, Baldwin Park, CA, USA) has been tested for efficacy in detecting more human diseases than probably any other portable electronic aroma detection (EAD) device. Over 100 biomedical and related journal articles have been published using this device. It contains a sensor array with 32 CBPC sensors that are sensitive to a wide range of VOCs. This instrument in somewhat unique in that the CBPC sensors are not highly responsive to moisture and therefore have an advantage in being able to discriminate between VOCs in gas samples with high moisture content. This feature enhances the capabilities and options of using the instrument for analysis of diagnostic samples containing high relative humidity, such as for breath and liquid excretory samples. Consequently, the C320 instrument may be used to diagnose a wide range of diseases that are detectable from VOC profiling and analysis of air expelled from the lungs.
Diagnosis of invasive pulmonary aspergillosis (IPA) in patients, particularly those with prolonged chemotherapy-induced neutropenia (PCIN), remains a difficult challenge due to nonspecific signs and symptoms [160,161,162,163,164,165]. High patient mortality often occurs when IPA-diagnoses are delayed [163,166,167]. The acquisition of bronchoalveolar lavage-fluid clinical samples for the Platelia galactomannan assay, the only test with sufficient sensitivity and specificity to rule out IA, is invasive and highly uncomfortable to patients [168,169,170,171,172,173].
Recent analyses of exhaled breath VOC-profiles (breathprints) of IA patients using the C320 e-nose showed that they have a distinct aroma signature profile that can be discriminated from non-IPA patients within minutes [160]. In this study, Aspergillus fumigatus- colonization was detected using the e-nose on 27 cystic fibrosis (CF) patients. E-nose data were classified using canonical discriminant analysis after principal component reduction. Cross-validated accuracy of e-nose determinations, defined as the percentage of correctly classified subjects using the leave-one-out method, were conducted with cultures of sputum samples. Results showed that only three subjects were misclassified as IPA positive, resulting in a cross-validated accuracy for the C320 detecting IA of 89% (p < 0.004; sensitivity, 78%; specificity, 94%). Receiver operating characteristic (ROC) curve analysis showed an area under the curve (AUC) of 0.89. These results indicated that A. fumigatus colonization produced a distinctive breathprint in CF patients that could be detected noninvasively for the first time using a Cyranose C320 e-nose (Sensigent, Baldwin Park, CA, USA).
Lung diseases are ranked as the third most common cause of death worldwide [218]. Approximately 15% of lung diseases are attributed to pneumoconiosis, a lung disease attributed to occupational exposure to various types of dust, asbestos, or smoke [219,220]. Diagnosis of early-stage pneumoconiosis is difficult in clinical practice using conventional methods [221]. Yang et al. [206] analyzed the exhaled breath VOCs of 34 subjects with pneumoconiosis and 64 healthy patients using a C320 e-nose. Performance of the e-nose using a prediction model based on linear discriminant analysis (LDA) indicated that C320-discriminations of sample types had high specificity (88.0%), acceptable sensitivity (67.9%), and good accuracy (80.8%) in the training set. In the test set, sensitivity was 66.7%, specificity was 71.4%, and accuracy was 70.0% by LDA suggesting that C320 e-nose-based breath tests may have good potential as a screening tool for pneumoconiosis.
Brekelman et al. [178] investigated the C320 e-nose as a potential diagnostic tool for inflammatory arthritis (IA) to differentiate between inflammatory joint diseases and healthy controls. They analyzed and compared the exhaled breath of 21 rheumatoid arthritis (RA), 18 psoriatic arthritis (PsA) patients with active disease and 21 healthy controls using principal component analysis, discriminant analysis, and area under curve (AUC) of receiver operating characteristics (ROC) curves. VOCs were identified by GC-MS and the relationships between breathprints and potential biomarkers of disease activity were explored. Breathprints of RA patients were distinguished from controls with an accuracy of 71%, sensitivity of 76% and specificity of 67%. Similarly, breathprints from PsA patients were separated from controls with 69% accuracy, sensitivity of 72% and specificity of 71%. Distinction between exhaled breath of RA and PsA patients exhibited an accuracy of 69%, sensitivity 71% and specificity of 72%. There was a positive correlation between RA patients of exhaled breathprints with disease activity score (DAS28) and number of painful joints. Seven key potential VOC-biomarker compounds were identified with GC-MS which significantly differed between the sample types of test groups. These VOCs included four aliphatic alcohols (1-propanol, 2-propanol, 2,2-dimethyl propanol, n-hexanol), and a single aliphatic ketone (2-pentanone).
A recent review provided a thorough summary of human diseases that may be detected by e-nose analysis of urine samples [222]. Urothelial cancer (carcinoma) of the bladder, known as transitional cell carcinoma (TCC), is by far the most common type of bladder cancer which may be detected from urine analysis. A urinary pathology pilot study was initiated in 2015 to examine the potential for noninvasive early detection of bladder cancer (BC) through VOC analysis of urine headspace by aroma or olfactory distinction using an experimental MOS e-nose [223]. Urine samples were collected from 15 patients with clinical suspicion of primary or recurrent bladder cancer and from 21 control patients without BC, but having benign urological conditions (e.g., benign prostatic hyperplasia (BPH), inflammatory disease) were randomly selected and evaluated for the presence of BC by MOS e-nose analysis. In addition, patients with clinical suspicion of BC underwent transurethral resection (TURB) for histopathological verification. Histopathology of resected bladder specimens revealed 53% of patients had urothelial cancer. Of these, 63% had pTa, 2 T1 and 1 Cis only. In addition, 63% of patients had low grade tumors and 38% had high grade tumors. Histopathology findings revealed no cancer in 47% of patients. Among the controls, 13 had BPH, four inflammatory disease, one nephrolithiasis and three other benign diseases. The electronic nose correctly detected cancer in 75% of BC patients, but missed two pTa tumors, resulting in 75% sensitivity. For patients without BC, 86% of patients with negative TURB were correctly diagnosed with a specificity of 86%. False positive tests were found in four patients of whom all four had urocystitis based on histopathology. Considering only the BC-control group all patients were correctly classified with a specificity of 100%. The results suggested the high potential of the experimental MOS e-nose in detection of BC with an overall sensitivity of 75% and specificity of 86%.
Saidi et al. [185] evaluated an experimental MOS e-nose as an exhaled breath VOC-analysis tool for detection of chronic kidney disease (CKD) diabetes mellitus (DM) compared with healthy subjects. They also used gas chromatography quadrupole time-of-flight mass spectrometry (GC/Q-TOF-MS) to identify individual breath volatiles. Urine samples also were collected to measure creatinine levels by UV–vis spectrophotometry as a reference method. E-nose data from 44 test subjects were analyzed using principal component analysis (PCA), support vector machines (SVMs), hierarchical cluster analysis (HCA) and partial least squares-regressions (PLSR). The PLSR model revealed a positive relationship between breath and urinary creatinine levels. The results indicated that e-nose data in combination with pattern recognition algorithms provided an inexpensive basis for non-invasive diagnosis and distinguishing between exhaled breath of CKD and DM patients as well as healthy controls based on breath VOC-analysis.
Inflammatory bowel diseases (IBD) are a group of autoimmune diseases that have been increasing in worldwide incidence, prevalence and severity particularly in children [43,44]. The disease complex of IBD includes Crohn’s disease (CD), ulcerative colitis (UC), and microscopic colitis (including both collagenous colitis and lymphocytic colitis forms). Individuals suffering from these diseases are profoundly affected in terms of quality of life and frequently unpleasant GI-related symptoms. The creation of models based on VOCs profiles, precise instrumentation and advanced statistical methods have been used to develop new relatively inexpensive diagnostic tools for IBD diagnoses with high sensitivity and specificity. Studies involving VOC-profile model development are providing critical information towards better understanding the etiology of IBD through analysis of specific VOCs produced as a result of disease-modifications of host metabolic processes. Analysis of VOC patterns in alveolar air of pediatric patients with IBD was investigated in a recent study of young CD and UC patients compared to controls with and without gastrointestinal symptomatology [196]. Alveolar breath was analyzed by ion molecule reaction mass spectrometry (IMR-MS). Four separate molecular models were built for IBD analyses based on different numbers of specific VOCs included from a list of 81 total molecules plus the age of subjects as independent variables, adopting a penalizing LASSO logistic regression approach. The four models included: (1) IBDs vs. controls, based on 18 VOCs (sensitivity = 95%, specificity = 69%, AUC = 0.925), (2) CD vs. UC based on 13 VOCs (sensitivity = 94%, specificity = 76%, AUC = 0.934), (3) IBDs vs. gastroenterological controls based on 15 VOCs (sensitivity = 94%, specificity = 65%, AUC = 0.918), and (4) IBDs vs. controls, initially based on 21 molecules, but finally on 12 VOCs (sensitivity = 94%, specificity = 71%, AUC = 0.888). The VOCs identified by the models as contributing most to IBD effects were studied relative to concerned outcomes.
The microbial cause of soft tissue wound infections, including post-operative wound infections, are conventionally based on identification of bacterial or fungal pathogens by swab cultures, microscopic examinations, laboratory tests and PCR assays which require several hours to days to obtain a diagnosis [217]. Consequently, broad-spectrum antibiotic treatment generally is administered early as a precautionary measure before a specific diagnosis. This common practice often results in the inappropriate and overuse of antibiotics, based purely on educated guess-work that may be ineffective in treating the particular strain of microbes involved in soft-tissue infections. The need for real-time, rapid and accurate diagnoses, allowing for more effective early targeted pathogen-specific treatments, require the development and use of methods for identifying pathogens much earlier based on chemical surveillance methods that detect the unique microbial metabolite signatures (VOC-profiles) produced by individual microbial species due to their particular use of specific combinations of metabolic pathways [10]. Saviauk et al. [217] recently tested a handheld ion mobility spectrometry (IMS)-type e-nose device for POCT to rapidly differentiate between the most common SSTI and life-threatening pathogens causing gas gangrene infections. They examined the most relevant bacteria causing wound infections by analyzing gaseous headspace VOCs of clinical bacterial blood cultures on standardized culture media. The IMS-e-nose system was capable of distinguishing between methicillin-sensitive Staphylococcus aureus (MSSA), Streptococcus pyogenes, Escherichia coli, Pseudomonas aeruginosa, and Clostridium perfringens with an accuracy of 78%, sensitivity of 83%, and specificity of 100% within minutes without prior sample preparation. With an overall accuracy of 91%, they concluded that this IMS-e-nose methodology could be used for the rapid detection and identification of most bacteria causing wound infections.
Volatile Organic Compound -Biomarkers of Human Diseases
Research involving the discovery of new potential VOC-biomarkers of specific human and animal diseases has accelerated over the past decade as novel metabolomic-type instruments have been invented to assist in the identification of volatile metabolites. Summaries of many putative volatile biomarkers associated with specific diseases, including many gastrointestinal diseases, are available in recent reviews [7,44]. Additional reviews provide extensive information on specific e-nose devices that have been used for detection of complex mixtures of VOC-biomarkers, based on unique smellprint signatures (VOC profiles), found in exhaled breath and headspace gases derived from clinical samples [12,27,32,43,44]. The use of dual-technology e-noses or traditional e-noses in combination with targeted known biomarker detection with metabolomic instruments was recently proposed to improve the accuracy and effectiveness of noninvasive early disease diagnoses [44].
Progress in the discovery of reliable VOC-biomarkers of disease has been slow due to difficulties in identifying single compounds strongly correlated with disease and metabolomic changes in pathophysiological (disease-associated metabolic) pathways that are clearly indicative of specific mechanisms of disease. Isolating the effects and possible roles of single biomarker compounds in pathogenesis is a major challenge particularly when the mechanisms of disease are not fully understood. Nevertheless, some progress in identifying unique, relatively well-established disease biomarkers has been achieved through metabolomic studies of human diseases [7,32]. Other indications of possible disease-associated VOC-biomarkers are tentative and require additional research for confirmation.
The increase in nitric oxide (NO) production throughout the body as a healing response to fight inflammation has been well established [224,225]. As a consequence, many human diseases causing inflammation potentially are detectable by electronic measurements of NO levels in the human breath or blood serum, particularly when used in combination with other disease-specific VOC-biomarkers. Portable NO-sensitive e-noses (eNO devices) are already routinely used in the U.S. to detect asthma severity in clinical patients. Similar elevated exhaled NO levels have been reported to be associated with many other pulmonary diseases besides asthma. Hypoxia associated with acute mountain sickness (AMS) may be a good candidate disease for potential detection by eNO measurements in exhaled breath. Evidence of lung inflammation in AMS patients, most likely mediated by high-altitude hypoxia and associated concomitant increase in NO production, has been suggested as the most plausible physiological mechanism explaining observed differences in e-nose derived VOC profiles between AMS-resistant and AMS-susceptible individuals [226]. Inflammation associated with higher NO production also has been observed for other human diseases including hypertension [227,228], arthritis [229,230], lung diseases such as acute respiratory distress syndrome (ARDS), bronchiectasis, and cystic fibrosis [231], and inflammatory bowel disease (IBD) in the colon and small intestine [232].
A wide range of statistical methods developed for pattern recognition are increasingly being used for data analysis in VOC-emission studies involving detection of disease-related VOC profiles. Univariate methods are not suitable for the investigation of VOC profiles because they consider possible disease biomarker compounds separately and are not able to discover VOC patterns. A controlled-animal study on paratuberculosis recently compared the pattern-recognition approach, using the random forest classification method, to a disease- prediction approach based on single biomarker compounds [233]. A comparison of both strategies, based on VOC data using cross-validation procedures, revealed that random forests achieved higher sensitivities and specificities than predictions based on single compounds. They concluded that the pattern-recognition approach is more likely to be fruitful for disease prediction than single biomarkers for this disease. In situations where a very large number of VOCs are present in clinical samples, such as analysis of exhaled breath, VOC profiles generally are more useful for disease detection unless well-established disease biomarkers have been clearly identified and consistently demonstrated.
Durán-Acevedo et al. [234] recently reported on the development of a new chip-based gold nanoparticle (AuNP) e-nose sensor technology, amenable for early disease screening, which correctly predicted gastric cancer (GC) with 97% accuracy. They identified six new GC VOC-biomarkers using GC-MS analyses, indicating that concentrations of these biomarkers in the breath of patients diagnosed with GC were statistically different from those of a control group of patients diagnosed with other gastric diseases. Four of the biomarkers increased in concentration within the exhaled breath of GC patients, while the other two biomarkers decreased in concentration compared with controls. The putative identities of these GC biomarkers, found in Colombian patients, included trans-2,2-dimethyl-3-decene, octadecane, m-xylene, hexadecane, 1-cyclohexyl-2-(cyclohexylmethyl) pentane, and eicosane. The GC-biomarker compounds found in the breath of Latin American patients were different from those identified previously in individuals from separate populations with high incidence of GC from China (eastern Asia region) and Latvia (a Baltic State) [235,236]. The differences in breath GC biomarkers from different regions of the world were attributed to geographical variations in culture, lifestyle, diet, and genetics differences.
4. Future Electronic-Nose Technologies for Improved Disease Diagnostics
Affordable and portable, electronic-nose devices with multisensory arrays generally do not have the capability of providing analytical (qualitative) identifications of individual VOCs in complex gas mixtures, but are most useful for the recognition and discrimination of differences in VOC-composition of headspace volatile gas mixtures from particular sample types, providing information about the origin, chemical characteristics and aroma classification of the sample [5,6]. Each e-nose type, regardless of operating principle, simultaneously records sensor responses (from all sensors within the array) to all VOCs present in sample analytes to form a collective VOC sample profile or smellprint. E-nose technologies also do not usually provide suitable information for quantitative determinations [9]. The usefulness of having both analytical and quantitative chemical data for disease diagnoses has come to light in numerous metabolomics studies that have elucidated documented changes in host metabolic pathways that occur as a consequence of disease. These changes result in the production and release of different quantities and types of VOCs from diseased tissues, resulting from disease alterations in host metabolic processes, which are detectable in clinical samples [7,27].
Commercial combination-technology e-nose instruments, capable of sensory outputs that provide both VOC aroma signatures and chemical analysis data, recently are becoming more available as new-generation e-noses are designed with greater chemical-identification capabilities. These newer e-nose instruments have been developed to fulfill the need for some chemical analyses associated with VOC profiles. The combined-technology e-noses likely will not totally eliminate the need for analytical metabolomic-type instruments, due to the important function of metabolomics in identifying chemical disease biomarkers and disease-associated changes in metabolite concentrations, but these newer e-nose instruments may serve a role as possible effective and cheaper options in prophylactic screenings for noninvasive early disease detections. One combination-technology instrument, the Heracles II GC/Electronic-nose system (Alpha MOS, Toulouse, France), composed of a dual-column gas chromatograph with a very large metal-oxide (MOS) e-nose sensor array and an extensive (>83,000 organic compounds) searchable Kovats Index chemical reference library database that may be used in combination with analytical standards, provides a means for the tentative identification of VOC metabolites and chemical biomarkers associated with disease as well as smellprint signatures of VOC profiles that may be compared using PCA and other statistical methods. Other dual-technology e-nose systems have been described previously [5]. Some advantages of combining an e-nose instrument combined with GC capabilities is the potential for determining not only how many VOCs are present in the clinical sample analyte, their relative molecular weights and amounts produced, but also tentative compound identities, gas chromatograms for peak-pattern comparisons of sample types, and similar e-nose aroma signature patterns (VOC profiles) of headspace analyte composition.
The development of smaller, lightweight and more portable electronic-nose devices provide more effective means of achieving early disease diagnoses in field situations where access to hospitals is difficult in geographically isolated locations. The continued development of improved portable e-noses also increases the potential for using analytical tools that help to simplify and accelerate POCT clinical diagnostic processes that facilitate more rapid noninvasive early disease detection. The result of using an accelerated approach to disease diagnostics is to achieve a more efficient healthcare system with greater potential for administering earlier more effective and targeted disease-control treatments that improve disease prognoses and significantly shorten patient recovery times following disease treatments.
5. Conclusions
Electronic noses are EAD devices with the capability of high-throughput analysis of complex gaseous VOC mixtures as composite metabolite profiles [21,22]. These instruments are innovative diagnostic tools with great potential for non-invasive earlier detection of numerous types of plant, animal and human diseases based on analysis of headspace VOC-metabolites derived from clinical samples. They are affordable, have low operation and maintenance costs and provide real-time measurement capabilities [44].
The need for simpler and portable e-nose devices to provide rapid, accurate diagnostic results and replace conventional cumbersome and time-consuming clinical and laboratory methods have resulted from the growing demand for improved healthcare instruments and procedures that are noninvasive and speed up POCT, allowing faster treatments for diseases, improved prognoses, shorter hospital stays, more rapid disease recovery and reduced healthcare costs [6,8]. Continued advances and POCT of new e-nose technologies along with development of standardized diagnostic methodologies will continue to help bring these instruments into routine clinical practice [44].
A significant portion of cited papers, reporting test results of diagnostic methods (primarily for disease detection) in this review, are proof-of-concept pilot studies utilizing diagnostic models based on relatively few (a small subset) of the total VOCs derived from clinical samples. It should be noted that external validation studies must use identical VOC-models when evaluating these methods by efficacy tests in clinical trials. Such evaluations usually require that scientists or clinicians (testing the methods) consult the advice of the paper’s authors to assure precise duplication of diagnostic models and methods used in external validation tests. Acquisition of model-input and statistical data as well as test results from the original model-development studies also is recommended because this information is particularly useful in facilitating duplication of identical test methods.
Electronic-nose devices are attracting increasingly more interest from healthcare providers due to the many advantages and versatility these instruments provide for a wide range of clinical applications. Over time, improvements in the designs of e-nose systems for specific biomedical applications have advanced the accuracy, reliability and effectiveness of these instruments as diagnostic tools [8,12]. Important issues need to be addressed before VOC analysis with e-nose instruments can achieve their full potential as effective disease detection and monitoring tools for clinical diagnoses. Additional priority research should focus on developing universal standardization of e-nose instruments, sampling protocols, sample transport and storage conditions and analytical methodologies to allow inter-study data comparisons [237,238]. The future development of specific disease-associated e-nose databases (with worldwide accessibility by healthcare professionals and researchers based on specific standardized diagnostic methods and instrument types) [239], the identification of additional effective VOC-biomarkers of specific diseases for confirming diagnoses, the development of new potential clinical e-nose applications for detecting additional diseases (e.g., epilepsy) [240], and improvements in electronics miniaturization, ergonomics and diagnostic software should permit e-nose instruments and methods to be fully accepted and integrated into clinical procedures.
Funding
This literature review and associated research project was not funded by an external funding source. All funding was provided by special White-nose Syndrome (WNS) dedicated funds, a national strategic priority research topic, from the USDA Forest Service, Southern Research Station, for research involving animal pathology and associated early, noninvasive disease-diagnostics research. The author has received allocated research funds from the USDA Forest Service, available for technology transfer of new disease detection and diagnostic technologies, and to cover the costs of publishing in open access journals.
Acknowledgments
The author appreciates the assistance of Lisa B. Forse for collecting references, performing technical work tasks, and proofreading the manuscript.
Conflicts of Interest
The author declares no conflict of interest.
References
- Bos, L.D.; Sterk, P.J.; Schultz, M.J. Volatile metabolites of pathogens: A systematic review. PLoS Pathog. 2013, 9, e1003311. [Google Scholar] [CrossRef] [PubMed]
- Santini, G.; Mores, N.; Penas, A.; Capuano, R.; Mondino, C.; Trové, A.; Macagno, F.; Zini, G.; Cattani, P.; Martinelli, E.; et al. Electronic nose and exhaled breath NMR-based metabolomics applications in airways disease. Curr. Top. Med. Chem. 2016, 16, 1610–1630. [Google Scholar] [CrossRef] [PubMed]
- Spaněl, P.; Smith, D. Progress in SIFT-MS: Breath analysis and other applications. Mass Spectrom. Rev. 2011, 30, 236–267. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Sahay, P. Breath analysis using laser spectroscopic techniques: Breath biomarkers, spectral fingerprints, and detection limits. Sensors 2009, 9, 8230–8262. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Baietto, M. Applications and advances in electronic-nose technologies. Sensors 2009, 9, 5099–5148. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Recent progress in the design and clinical development of electronic-nose technologies. Nanobiosens. Dis. Diagn. 2016, 5, 15–27. [Google Scholar] [CrossRef]
- Wilson, A.D. Biomarker metabolite signatures pave the way for electronic-nose applications in early clinical disease diagnoses. Curr. Metabolomics 2017, 5, 90–101. [Google Scholar] [CrossRef]
- Wilson, A.D. Electronic-nose devices—Potential for noninvasive early disease-detection applications. Ann. Clin. Case Rep. 2017, 2, 1401. Available online: http://www.anncaserep.com/full-text/accr-v2-id1401.php (accessed on 14 July 2017).
- Cellini, A.; Blasioli, S.; Biondi, E.; Bertaccini, A.; Braschi, I.; Spinelli, F. Potential applications and limitations of electronic nose devices for plant disease diagnosis. Sensors 2017, 17, 2596. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Lester, D.G.; Oberle, C.S. Development of conductive polymer analysis for the rapid detection and identification of phytopathogenic microbes. Phytopathology 2004, 94, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Casalinuovo, I.A.; Di Pierro, D.; Coletta, M.; Di Francesco, P. Application of electronic noses for disease diagnosis and food spoilage detection. Sensors 2006, 6, 1428–1439. [Google Scholar] [CrossRef]
- Wilson, A.D.; Baietto, M. Advances in electronic-nose technologies developed for biomedical applications. Sensors 2011, 11, 1105–1176. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Diverse applications of electronic nose technologies in agriculture and forestry. Sensors 2013, 13, 2295–2348. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.A.; Shevade, A.V.; Taylor, C.J.; Homer, M.L.; Jewell, A.D.; Kisor, A.; Manatt, K.S.; Yen, S.P.S.; Blanco, M.; Goddard, W.A. Expanding the Capabilities of the JPL Electronic Nose for an International Space Station Technology Demonstration; SAE Technical Paper 2006-01-2179; Jet Propulsion Laboratory, National Aeronautics and Space Administration: Pasadena, CA, USA, 2006.
- Shevade, A.V.; Homer, M.L.; Zhou, H.; Jewell, A.D.; Kisor, A.K.; Manatt, K.S.; Torres, J.; Soler, J.; Yen, S.P.S.; Ryan, M.A.; et al. Development of the Third Generation JPL Electronic Nose for International Space Station Technology Demonstration; SAE Technical Paper 2007-01-3149; Jet Propulsion Laboratory, California Institute of Technology: Pasadena, CA, USA, 2007. [Google Scholar]
- Ryan, M.A.; Manatt, K.S.; Gluck, S.E.; Shevade, A.V.; Kisor, A.K.; Zhou, H.; Lara, L.M.; Homer, M.L. Operation of Third Generation JPL Electronic Nose on the International Space Station; SAE Technical Paper 2009-01-2522; Jet Propulsion Laboratory, California Institute of Technology: Pasadena, CA, USA, 2009. [Google Scholar]
- Kateb, B.; Ryan, M.A.; Homer, M.L.; Lara, L.M.; Yin, Y.; Higa, K.; Chen, M.Y. Sniffing out cancer using the JPL electronic nose: A pilot study of a novel approach to detection and differentiation of brain cancer. NeuroImage 2009, 47, T5–T9. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Review of electronic-nose technologies and algorithms to detect hazardous chemicals in the environment. Procedia Technol. 2012, 1, 453–463. [Google Scholar] [CrossRef]
- Wilson, A.D.; Lester, D.G.; Oberle, C.S. Application of conductive polymer analysis for wood and woody plant identifications. For. Ecol. Manag. 2005, 209, 207–224. [Google Scholar] [CrossRef]
- Wilson, A.D. Future applications of electronic‑nose technologies in healthcare and biomedicine. In Wide Spectra of Quality Control; Akyar, I., Ed.; InTech Publishing: Rijeka, Croatia, 2011; ISBN 978-953-307-683-6. [Google Scholar]
- Wilson, A.D. Finding Aroma Clues in the Human Breath to Diagnose Diseases. Atlas of Science 29 February 2016. Available online: http://atlasofscience.org/finding-aroma-clues-in-the-human-breath-to-diagnose-diseases (accessed on 20 August 2018).
- Wilson, A.D. Identification of insecticide residues with a conducting-polymer electronic nose. Chem. Sens. 2014, 4, 1–10. [Google Scholar]
- Wilson, A.D. Fungicide residue identification and discrimination using a conducting polymer electronic-nose. In Proceedings of the IV International Conference on Sensor Device Technologies and Applications, Barcelona, Spain, 25–31 August 2013; Yurish, S., Chilibon, I., Carvalho, V., Gervais-Ducouret, S., Eds.; Xpert Publishing Services: Wilmington, DE, USA, 2013; pp. 116–121. [Google Scholar]
- Wilson, A.D. Identification and discrimination of herbicide residues using a conducting polymer electronic nose. In Proceedings of the VII International Conference on Sensor Device Technologies and Applications, Nice, France, 24–28 July 2016; International Academy, Research, and Industry Association (IARIA): Wilmington, DE, USA, 2016; pp. 4–7. [Google Scholar]
- Baldwin, E.A.; Bai, J.; Plotto, A.; Dea, S. Electronic noses and tongues: Application for the food and pharmaceutical industries. Sensors 2011, 11, 4744–4766. [Google Scholar] [CrossRef] [PubMed]
- Baietto, M.; Wilson, A.D. Electronic-nose applications for fruit identification, ripeness and quality grading. Sensors 2015, 15, 899–931. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Electronic-nose applications in forensic science and for analysis of volatile biomarkers in the human breath. J. Forensic Sci. Criminol. 2014, 1, S103. [Google Scholar] [CrossRef]
- Wilson, A.D. Theoretical and practical considerations for teaching diagnostic electronic-nose technologies to clinical laboratory technicians. Proc. Soc. Behav. Sci. 2012, 31, 262–274. [Google Scholar] [CrossRef]
- Wilson, A.D. Advanced methods for teaching electronic-nose technologies to diagnosticians and clinical laboratory technicians. Proc. Soc. Behav. Sci. 2012, 46, 4544–4554. [Google Scholar] [CrossRef]
- Li, H.; Tang, H.; Wang, Y. Advances in metabonomics on infectious diseases. Curr. Metabolomics 2013, 1, 318–334. [Google Scholar] [CrossRef]
- Emwas, A.M.; Salek, R.M. NMR-based metabolomics in human disease diagnosis: Applications, limitations, and recommendations. Metabolomics 2013, 9, 1048–1072. [Google Scholar] [CrossRef]
- Wilson, A.D. Advances in electronic-nose technologies for the detection of volatile biomarker metabolites in the human breath. Metabolites 2015, 5, 140–163. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, F.; Cellini, A.; Vanneste, J.L.; Rodriguez-Estrada, M.T.; Costa, G.; Savioli, S.; Harren, F.J.M.; Cristescu, S.M. Emission of volatile compounds by Erwinia amylovora biological activity in vitro and possible exploitation for bacterial identification. Trees 2012, 26, 141–152. [Google Scholar] [CrossRef]
- Cellini, A.; Biondi, E.; Blasioli, S.; Rocchi, L.; Farneti, B.; Braschi, I.; Savioli, S.; Rodriguez-Estrada, M.T.; Biasioli, F.; Spinelli, F. Early detection of bacterial diseases in apple plants by analysis of volatile organic compounds profiles and use of electronic nose. Ann. Appl. Biol. 2016, 168, 409–420. [Google Scholar] [CrossRef]
- Thelen, J.; Harbinson, J.; Jansen, R.; Van Straten, G.; Posthumus, M.A.; Woltering, E.J.; Bouwmeester, H.J. The sesquiterpene α-copaene is induced in tomato leaves infected by Botrytis cinerea. J. Plant Interact. 2005, 1, 163–170. [Google Scholar] [CrossRef]
- Laothawornkitkul, J.; Moore, J.P.; Taylor, J.E.; Possell, M.; Gibson, T.D.; Hewett, C.N.; Paul, N.D. Discrimination of plant volatile signatures by an electronic nose: A potential technology for plant pest and disease monitoring. Environ. Sci. Technol. 2008, 42, 8433–8439. [Google Scholar] [CrossRef] [PubMed]
- Peled, N.; Koslow, M.; Ryan, J.; Haick, H. Detection of volatile organic compounds in cattle naturally infected with Mycobacterium bovis. Sens. Actuators B 2012, 171–172, 588–594. [Google Scholar] [CrossRef]
- Van den Velde, S.; van Steenberghe, D.; van Hee, P.; Quirynen, M. Detection of odorous compounds in breath. J. Dent. Res. 2009, 88, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Okell, C.C.; Elliott, S.D. Bacteraemia and oral sepsis with special reference to the aetiology of subacute endocarditis. Lancet 1935, 2, 869–872. [Google Scholar] [CrossRef]
- Drangsholt, M.T. A new causal model of dental diseases associated with endocarditis. Ann. Periodontol. 1998, 3, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Lacassin, F.; Hoen, B.; Leport, C.; Selton-Suty, C.; Delahaye, F.; Goulet, V.; Etienne, J.; Briançon, S. Procedures associated with infective endocarditis in adults: A case-control study. Eur. Heart J. 1995, 16, 1968–1974. [Google Scholar] [CrossRef] [PubMed]
- Balint, B.; Kharitonov, S.A.; Hanazawa, T.; Donnelly, L.E.; Shah, P.L.; Hodson, M.E.; Barnes, P.J. Increased nitrotyrosine in exhaled breath condensate in cystic fibrosis. Eur. Respir. J. 2001, 17, 1201–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, A.D. Recent applications of electronic-nose technologies for the noninvasive early diagnosis of gastrointestinal diseases. Proceedings 2018, 2, 147. [Google Scholar] [CrossRef]
- Wilson, A.D. Application of electronic-nose technologies and VOC-biomarkers for the noninvasive early diagnosis of gastrointestinal diseases. Sensors 2018, 18, 2613. [Google Scholar] [CrossRef] [PubMed]
- Taware, R.; Taunk, K.; Pereira, JA.; Dhakne, R.; Kannan, N.; Soneji, D.; Câmara, J.; Nagara, H.A.; Rapole, S. Investigation of urinary volatomic alterations in head and neck cancer: A non-invasive approach towards diagnosis and prognosis. Metabolomics 2017, 13, 111. [Google Scholar] [CrossRef]
- Paredes, R.M.G.; Pinto, C.G.; Pavón, J.L.P.; Cordero, B.M. Headspace-gas chromatography-mass spectrometry for the rapid determination of possible biomarkers in urine samples. Anal. Methods 2017, 9, 5784–5790. [Google Scholar] [CrossRef]
- Bax, C.; Taverna, G.; Eusebio, L.; Sironi, S.; Grizzi, F.; Guazzoni, G.; Capelli, L. Innovative diagnostic methods for early prostate cancer detection through urine analysis: A review. Cancers 2018, 10, 123. [Google Scholar] [CrossRef] [PubMed]
- Van Oort, P.; Povoa, P.; Schnabel, R.; Dark, P.M.; Artigas, A.; Bergmans, D.C.J.-J.; Felton, T.W.; Coelho, L.; Schultz, M.J.; Fowler, S.J.; et al. The potential role of exhaled breath analysis in the diagnostic process of pneumonia—A systematic review. J. Breath Res. 2018, 12, 024001. [Google Scholar] [CrossRef] [PubMed]
- Bos, L.D.; Sterk, P.J.; Fowler, S.J. Breathomics in the setting of asthma and chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2016, 138, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.; Fijten, R.; Smolinska, A.; Dallinga, J.; Boumans, M.-L.; Stobberingh, E.; Boots, A.; Roekaerts, P.; Bergmans, D.; van Schooten, F.J. Analysis of volatile organic compounds in exhaled breath to diagnose ventilator-associated pneumonia. Sci. Rep. 2015, 5, 17179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, S.J.; Basanta-Sanchez, M.; Xu, Y.; Goodacre, R.; Dark, P.M. Surveillance for lower airway pathogens in mechanically ventilated patients by metabolomic analysis of exhaled breath: A case-control study. Thorax 2015, 70, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Van Oort, P.M.P.; De Bruin, S.; Weda, H.; Knobel, H.H.; Schultz, M.J.; Bos, L.D. Exhaled breath metabolomics for the diagnosis of pneumonia in intubated and mechanically-ventilated intensive care unit (ICU)-patients. Int. J. Mol. Sci. 2017, 18, 449. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Lindon, J.C.; Holmes, E. ‘Metabonomics’: Understanding the metabolic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica 1999, 29, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.R.; Wang, Y.L. Metabonomics: A revolution in progress. Prog. Biochem. Biophys. 2006, 33, 401–417. [Google Scholar]
- Pardo, M.; Sberveglieri, G. Electronic olfactory systems based on metal oxide semiconductor sensor arrays. MRS Bull. 2004, 29, 703–708. [Google Scholar] [CrossRef]
- Loutfi, A.; Coradeschi, S.; Mani, G.K.; Shankar, P.; Rayappan, J.B.B. Electronic noses for food quality: A review. J. Food Eng. 2015, 144, 103–111. [Google Scholar] [CrossRef]
- Peris, M.; Escuder-Gilabert, L. A 21st century technique for food control: Electronic noses. Anal. Chim. Acta 2009, 638, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Application of a conductive polymer electronic-nose device to identify aged woody samples. In Proceedings of the 3rd International IARIA Conference on Sensor Device Technologies and Applications, Rome, Italy, 19–24 August 2012; Xpert Publishing Services: Wilmington, DE, USA, 2012; pp. 77–82, ISBN 978-1-61208-208-0. [Google Scholar]
- Martinelli, F.; Scalenghe, R.; Davino, S.; Panno, S.; Scuderi, G.; Ruisi, P.; Villa, P.; Stroppiana, D.; Boschetti, M.; Goulart, L.R.; et al. Advanced methods of plant disease detection. A review. Agron. Sustain. Dev. 2015, 35, 1–25. [Google Scholar] [CrossRef]
- Sankaran, S.; Mishra, A.; Ehsani, R.; Davis, C. A review of advanced techniques for detecting plant diseases. Comput. Electron. Agric. 2010, 72, 1–13. [Google Scholar] [CrossRef]
- Ray, M.; Ray, A.; Dash, S.; Mishra, A.; Achary, K.G.; Nayak, S.; Singh, S. Fungal disease detection in plants: Traditional assays, novel diagnostic techniques and biosensors. Biosens. Bioelectron. 2017, 87, 708–723. [Google Scholar] [CrossRef] [PubMed]
- Markom, M.A.; Shakaff, A.Y.M.; Adom, A.H.; Ahmad, M.N.; Hidayat, W.; Abdullah, A.H.; Fikri, N.A. Intelligent electronic nose system for basal stem rot disease detection. Comput. Electron. Agric. 2009, 66, 140–146. [Google Scholar] [CrossRef]
- Rizzolo, A.; Bianchi, G.; Lucido, P.; Cangelosi, B.; Pozzi, L.; Villa, G.; Clematis, F.; Pasini, C.; Curir, P. Electronic nose for the early detection of red palm weevil (Rhynchophorus ferrugineous Olivier) infestation in palms: Preliminary results. Acta Hortic. 2015, 1099, 347–355. [Google Scholar] [CrossRef]
- Fang, Y.; Ramasamy, R.P. Current and prospective methods for plant disease detection. Biosensors 2015, 4, 537–561. [Google Scholar] [CrossRef] [PubMed]
- Mahlein, A.-K. Plant disease detection by imaging sensors—Parallels and specific demands for precision agriculture and plant phenotyping. Plant Dis. 2016, 100, 241–251. [Google Scholar] [CrossRef]
- Ghaffari, R.; Laothawornkitkul, J.; Zhang, F.; Iliescu, D.; Hines, E.; Leeson, M.; Napier, R.; Moore, J.P.; Paul, N.D.; Hewitt, C.N.; et al. Plant pest and disease diagnosis: Electronic nose and support vector machine approach. J. Plant Dis. Protect. 2012, 119, 200–207. [Google Scholar] [CrossRef]
- Li, G.; Fu, J.; Zhang, J.; Zheng, J. Progress in bionic information processing techniques for an electronic nose based on olfactory models. Chin. Sci. Bull. 2009, 54, 521–534. [Google Scholar] [CrossRef]
- Dudareva, N.; Negre, F.; Nagegowda, D.A.; Orlova, I. Plant volatiles: Recent advances and future perspectives. Crit. Rev. Plant Sci. 2006, 25, 417–440. [Google Scholar] [CrossRef]
- De Lacy Costello, B.P.J.; Evans, P.; Ewen, R.J.; Gunson, H.E.; Jones, P.R.H.; Ratcliffe, N.M.; Spencer-Phillips, P.T.N. Gas chromatography-mass spectrometry analyses of volatile organic compounds from potato tubers inoculated with Phytophthora infestans or Fusarium coeruleum. Plant Pathol. 2001, 50, 489–496. [Google Scholar] [CrossRef]
- Kushalappa, A.C.; Lui, L.H.; Chen, C.R.; Lee, B. Volatile fingerprinting (SPME-GC FID) to detect and discriminate diseases of potato tubers. Plant Dis. 2002, 86, 131–137. [Google Scholar] [CrossRef]
- Blasioli, S.; Biondi, E.; Samudrala, D.; Spinelli, F.; Cellini, A.; Bertaccini, A.; Cristescu, S.M.; Braschi, I. Identification of volatile markers in potato brown rot and ring rot by combined GC-MS and PTR-MS techniques: Study on in vitro and in vivo samples. J. Agric. Food Chem. 2014, 62, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Vikram, A.; Prithiviraj, B.; Hamzehzarghani, H.; Kushalappa, A.C. Volatile metabolite profiling to discriminate diseases of McIntosh apple inoculated with fungal pathogens. J. Sci. Food Agric. 2004, 84, 1333–1340. [Google Scholar] [CrossRef]
- Prithiviraj, B.; Vikram, A.; Kushalappa, A.C.; Yaylayan, V. Volatile metabolite profiling for the discrimination of onion bulbs infected by Erwinia carotovora ssp. carotovora, Fusarium oxysporum and Botrytis allii. Eur. J. Plant Pathol. 2004, 110, 371–377. [Google Scholar] [CrossRef]
- Spinelli, F.; Noferini, M.; Costa, G. Near infrared spectroscopy (NIRS): Perspective of fire blight detection in asymptomatic plant material. Acta Hortic. 2006, 704, 87–91. [Google Scholar] [CrossRef]
- Spinelli, F.; Costa, G.; Rondelli, E.; Vanneste, J.L.; Rodriguez Estrada, M.T.; Busi, S.; Savioli, S.; Cristescu, S. Volatile compounds produced by Erwinia amylovora and their potential exploitation for bacterial identification. Acta Hortic. 2011, 896, 77–84. [Google Scholar] [CrossRef]
- Cellini, A.; Biondi, E.; Buriani, G.; Farneti, B.; Rodriguez-Estrada, M.T.; Braschi, I.; Savioli, S.; Blasioli, S.; Rocchi, L.; Biasioli, F.; et al. Characterization of volatile organic compounds emitted by kiwifruit plants infected with Pseudomonas syringae pv. actinidiae and their effects on host defenses. Trees 2016, 30, 795–806. [Google Scholar] [CrossRef]
- Baietto, M.; Wilson, A.D.; Bassi, D.; Ferrini, F. Evaluation of three electronic noses for detecting incipient wood decay. Sensors 2010, 10, 1062–1092. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Khan, N.A.; Ferrante, A.; Trivellini, A.; Francini, A.; Khan, M.I.R. Ethylene role in plant growth, development and senescence: Interaction with other phytohormones. Front. Plant Sci. 2017, 8, 475. [Google Scholar] [CrossRef] [PubMed]
- Von Dahl, C.C.; Baldwin, I.T. Deciphering the role of ethylene in plant–herbivore interactions. J. Plant Growth Regul. 2007, 26, 201–209. [Google Scholar] [CrossRef]
- Niinemets, U.; Loreto, F.; Reichstein, M. Physiological and physicochemical controls on foliar volatile organic compound emissions. Trends Plant Sci. 2004, 9, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Baldwin, E.A.; Fortuny, R.C.S.; Mattheis, J.P.; Stanley, R.; Perera, C.; Brecht, J.K. Effect of pretreatment of intact ‘Gala’ apple with ethanol vapor, hear, or 1-methylcyclopropene on quality and shelf life of fresh-cut slices. J. Am. Soc. Hortic. Sci. 2004, 129, 583–593. [Google Scholar]
- Olsson, J.; Borjesson, T.; Lundstedt, T.; Schnurer, J. Detection and quantification of ochratoxin A and deoxynivalenol in barley grains by GC–MS and electronic nose. Int. J. Food. Microbiol. 2002, 72, 203–214. [Google Scholar] [CrossRef]
- Wilson, A.D. Detection and diagnosis of bacterial wetwood in Tilia americana and Ulmus americana sapwood using a CP electronic-nose. In Industrial, Medical and Environmental Applications of Microorganisms: Current Status and Trends; Méndez-Vilas, A., Ed.; Wageningen Academic Publishers: Wageningen, The Netherlands, 2014; pp. 209–214. ISBN 978-90-8686-243-6. [Google Scholar]
- Wilson, A.D. Bacterial wetwood detection in Fagus grandifolia and Prunus serotina sapwood using a conducting polymer electronic-nose device. In Proceedings of the V International Conference on Sensor Device Technologies and Applications, Lisbon, Portugal, 16–20 November 2014; International Academy, Research, and Industry Association (IARIA): Wilmington, DE, USA, 2014; pp. 109–113. [Google Scholar]
- Li, C.; Krewer, G.W.; Ji, P.; Scherm, H.; Kays, S.J. Gas sensor array for blueberry fruit disease detection and classification. Postharvest Biol. Technol. 2010, 55, 144–149. [Google Scholar] [CrossRef]
- Simon, J.E.; Hetzroni, A.; Bordelon, B.; Miles, G.E.; Charles, D.J. Electronic sensing of aromatic volatiles for quality sorting of blueberries. J. Food Sci. 1996, 61, 967–972. [Google Scholar] [CrossRef]
- Cheli, F.; Campagnoli, A.; Pinotti, L.; Savoini, G.; Dell’Orto, V. Electronic nose for determination of aflatoxins in maize. Biotechnol. Agron. Soc. Environ. 2009, 13, 39–43. [Google Scholar]
- Campagnoli, A.; Cheli, F.; Savoini, G.; Crotti, A.; Pastori, A.G.M.; Dell’Orto, V. Application of an electronic nose to detection of aflatoxins in corn. Vet. Res. Commun. 2009, 33, S273–S275. [Google Scholar] [CrossRef] [PubMed]
- Falasconi, M.; Gobbi, E.; Pardo, M.; Della Torre, M.; Bresciani, A.; Sberveglieri, G. Detection of toxigenic strains of Fusarium verticillioides in corn by electronic olfactory system. Sens. Actuators B 2005, 108, 250–257. [Google Scholar] [CrossRef]
- Henderson, W.G.; Khalilian, A.; Han, Y.J.; Greene, J.K.; Degenhardt, D.C. Detecting stink bugs/damage in cotton utilizing a portable electronic nose. Comput. Electron. Agric. 2010, 70, 157–162. [Google Scholar] [CrossRef]
- Blasioli, S.; Biondi, E.; Braschi, I.; Mazzucchi, U.; Bazzi, C.; Gessa, C.E. Electronic nose as an innovative tool for the diagnosis of grapevine crown gall. Anal. Chim. Acta 2010, 672, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Biondi, E.; Blasioli, S.; Fantini, M.; Braschi, I.; Bertaccini, A. Grapevine crown gall detection by electronic nose. In Proceedings of the 16th International Symposium on Olfaction and Electronic Noses, Dijon, France, 28 June–1 July 2015. [Google Scholar]
- Spinelli, F.; Noferini, M.; Vanneste, J.L.; Costa, G. Potential of the electronic-nose for the diagnosis of bacterial and fungal diseases in fruit trees. Bull. OEPP/EPPO Bull. 2010, 40, 59–67. [Google Scholar] [CrossRef]
- Wilson, A.D.; Lester, D.G. Application of aromascan analysis to detect and diagnose oak wilt in live oaks. Phytopathology 1998, 88, S97. [Google Scholar]
- Baietto, M.; Pozzi, L.; Wilson, A.D.; Bassi, D. Evaluation of a portable MOS electronic nose to detect root rots in shade tree species. Comput. Electron. Agric. 2013, 96, 117–125. [Google Scholar] [CrossRef]
- Sinha, R.; Khot, L.R.; Schroeder, B.K. FAIMS based sensing of Burkholderia cepacia caused sour skin in onions under bulk storage condition. Food Meas. 2017, 11, 1578–1585. [Google Scholar] [CrossRef]
- Baldwin, E.; Plotto, A.; Manthey, J.; McCollum, G.; Bai, J.; Irey, M.; Cameron, R.; Luzio, G. Effect of Liberibacter infection (Huanglongbing disease) of citrus on orange fruit physiology and fruit/fruit juice quality: Chemical and physical analyses. J. Agric. Food Chem. 2010, 58, 1247–1262. [Google Scholar] [CrossRef] [PubMed]
- Pallottino, F.; Costa, C.; Antonucci, F.; Strano, M.C.; Calandra, M.; Solaini, S.; Menesatti, P. Electronic nose application for determination of Penicillium digitatum in Valencia oranges. J. Sci. Food Agric. 2012, 92, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, S.; Hepher, M.J.; Sommerville, J. Detection of Serpula lacrymans infestation with a polypyrrole sensor array. Sens. Actuator B Chem. 2006, 113, 989–997. [Google Scholar] [CrossRef]
- Stinson, J.A.; Persaud, K.C.; Bryning, G. Generic system for the detection of statutory potato pathogens. Sens. Actuators B Chem. 2006, 116, 100–106. [Google Scholar] [CrossRef]
- Biondi, E.; Blasioli, S.; Galeone, A.; Spinelli, F.; Cellini, A.; Lucchese, C.; Braschi, I. Detection of potato brown rot and ring rot by electronic nose: From laboratory to real scale. Talanta 2014, 129, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Rutolo, M.F.; Clarkson, J.P.; Covington, J.A. The use of an electronic nose to detect early signs of soft-rot infection in potatoes. Biosyst. Eng. 2018, 167, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.; Wang, J. Use of electronic nose technology for identifying rice infestation by Nilaparvata lugens. Sens. Actuators B Chem. 2011, 160, 15–21. [Google Scholar] [CrossRef]
- Xu, S.; Zhou, Z.; Lu, H.; Luo, X.; Lan, Y.; Zhang, Y.; Li, Y. Estimation of the age and amount of brown rice plant hoppers based on bionic electronic nose use. Sensors 2014, 14, 18114–18130. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Zhang, W.; Zhu, N.; Mao, S.; Tu, K. Early detection and classification of pathogenic fungal disease in post-harvest strawberry fruit by electronic nose and gas chromatography–mass spectrometry. Food Res. Int. 2014, 62, 162–168. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, J.; Cheng, S. Predicting attacked time of tomato seedling by e-nose based on kernel principal component analysis. In Proceedings of the ASABE Annual International Meeting, Orlando, FL, USA, 17–20 July 2016. [Google Scholar]
- Paolesse, R.; Alimelli, A.; Martinelli, E.; Di Natale, C.; D’Amico, A.; D’Egidio, M.G.; Aureli, G.; Ricelli, A.; Fanelli, C. Detection of fungal contamination of cereal grain samples by an electronic nose. Sens. Actuators B Chem. 2006, 119, 425–430. [Google Scholar] [CrossRef]
- Eifler, J.; Martinelli, E.; Santonico, M.; Capuano, R.; Schild, D.; Di Natale, C. Differential detection of potentially hazardous Fusarium species in wheat grains by an electronic nose. PLoS ONE 2011, 6, e21026. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, J. Detection of age and insect damage incurred by wheat, with an electronic nose. J. Stored Prod. Res. 2007, 43, 489–495. [Google Scholar] [CrossRef]
- Naznin, H.A.; Kiyohara, D.; Kimura, M.; Miyazawa, M.; Shimizu, M.; Hyakumachi, M. Systemic resistance induced by volatile organic compounds emitted by plant growth-promoting fungi in Arabidopsis thaliana. PLoS ONE 2014, 9, e86882. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.M.; Wildt, J.; Kappers, I.F.; Bouwmeester, H.J.; Hofstee, J.W.; van Henten, E.J. Detection of diseased plants by analysis of volatile organic compound emission. Annu. Rev. Phytopathol. 2011, 49, 157–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanchiswamy, C.N.; Malnoy, M.; Maffei, M.E. Chemical diversity of microbial volatiles and their potential for plant growth and productivity. Front. Plant Sci. 2015, 6, 151. [Google Scholar] [CrossRef] [PubMed]
- Bitas, V.; Kim, H.; Bennett, J.W.; Kang, S. Sniffing on microbes: Diverse roles of microbial volatile organic compounds in plant health. Mol. Plant-Microbe Interact. 2013, 26, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Angle, C.; Waggoner, L.P.; Ferrando, A.; Haney, P.; Passler, T. Canine detection of the volatilome: A review of implications for pathogen and disease detection. Front. Vet. Sci. 2016, 3, 47. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, D.; Yttri, J. Antibiotics: When Science and Wishful Thinking Collide. Health Affairs Blogg. Available online: http://www.center4research.org/antibiotics-science-wishful-thinking-collide (accessed on 21 August 2018).
- Shivaprasad, H.L.; Palmieri, C. Pathology of mycobacteriosis in birds. The Veterinary Clinics of North America. Exot. Anim. Pract. 2012, 15, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Reavill, D.R.; Schmidt, R.E. Mycobacterial lesions in fish, amphibians, reptiles, rodents, lagomorphs, and ferrets with reference to animal models. The Veterinary Clinics of North America. Exot. Anim. Pract. 2012, 15, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Wobeser, G.A. Essentials of Disease in Wild Animals, 1st ed.; Blackwell Publishing: Ames, IA, USA, 2006; p. 170. ISBN 978-0-8138-0589-4. [Google Scholar]
- Ryan, T.J.; Livingstone, P.G.; Ramsey, D.S.; de Lisle, G.W.; Nugent, G.; Collins, D.M.; Buddle, B.M. Advances in understanding disease epidemiology and implications for control and eradication of tuberculosis in livestock: The experience from New Zealand. Vet. Microbiol. 2006, 112, 211–219. [Google Scholar] [CrossRef] [PubMed]
- White, P.C.; Böhm, M.; Marion, G.; Hutchings, M.R. Control of bovine tuberculosis in British livestock: There is no ‘silver bullet’. Trends Microbiol. 2008, 16, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Ward, A.I.; Judge, J.; Delahay, R.J. Farm husbandry and badger behaviour: Opportunities to manage badger to cattle transmission of Mycobacterium bovis? Prev. Vet. Med. 2010, 93, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Holt, N. The Infected Elephant in the Room. Slate’s Animal Blog. Available online: http://www.slate.com/blogs/wild_things/2015/03/24/elephant_tuberculosis_epidemic_zoo_and_circus_animals_passing_tb_to_humans.html (accessed on 24 August 2018).
- Schwarz, C.M. The Chambers Dictionary; Allied Chambers India Ltd.: Edinburg, UK, 1998; p. 352. ISBN 978-81-86062-25-8. [Google Scholar]
- Mandell, G.; Bennett, J.; Dolin, R. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 7th ed.; Churchill Livingstone; Elsevier: Philadelphia, PA, USA, 2010; Chapter 250; ISBN 978-0-443-06839-3. [Google Scholar]
- WHO Model Formulary. Available online: http://apps.who.int/medicinedocs/documents/s16879e/s16879e.pdf (accessed on 21 August 2018).
- Fend, R.; Geddes, R.; Lesellier, S.; Vordermeier, H.-M.; Corner, L.A.L.; Gormley, E.; Costello, E.; Hewinson, R.G.; Marlin, D.J.; Woodman, A.C.; et al. Use of an electronic nose to diagnose Mycobacterium bovis infection in badgers and cattle. J. Clin. Microbiol. 2005, 43, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Forse, L.B. Discrimination between Pseudogymnoascus destructans, other dermatophytes of cave-dwelling bats, and related innocuous keratinophilic fungi based on electronic-nose/GC signatures of VOC-metabolites produced in culture. In Proceedings of the VIII International Conference on Sensor Device Technologies and Applications, Rome, Italy, 10–14 September 2017; International Academy, Research, and Industry Association (IARIA): Wilmington, DE, USA, 2017; pp. 5–11. [Google Scholar]
- Wilson, A.D.; Forse, L.B. Differences in VOC-metabolite profiles of Pseudogymnoascus destructans and related fungi by electronic-nose/GC analyses of headspace volatiles derived from axenic cultures. Sens. Transducers 2018, 220, 9–19. [Google Scholar]
- Wilson, A.D.; Oberle, C.S.; Oberle, D.F. Detection of off-flavor in catfish using a conducting polymer electronic-nose technology. Sensors 2013, 13, 15968–15984. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.B.; Wang, S.Z.; Yin, Y.G.; Hoffmann, W.C.; Zheng, X.Z. Using a surface plasmon resonance biosensor for rapid detection of Salmonella typhimurium in chicken carcass. J. Bionic Eng. 2008, 5, 239–246. [Google Scholar] [CrossRef]
- Knobloch, H.; Schroedl, W.; Turner, C.; Chambers, M.; Reinhold, P. Electronic nose responses and acute phase proteins correlate in blood using a bovine model of respiratory infection. Sens. Actuators B 2010, 144, 81–87. [Google Scholar] [CrossRef]
- Mottram, T.T.; Dobbelaar, P.; Schukken, Y.H.; Hobbs, P.J.; Bartlett, P.N. An experiment to determine the feasibility of automatically detecting hyperketonaemia in dairy cows. Livest. Prod. Sci. 1999, 61, 7–11. [Google Scholar] [CrossRef]
- Wlodzimirow, K.A.; Abu-Hanna, A.; Schultz, M.J.; Maas, M.A.; Bos, L.D.; Sterk, P.J.; Knobel, H.H.; Soers, R.J.; Chamuleau, R.A. Exhaled breath analysis with electronic nose technology for detection of acute liver failure in rats. Biosens. Bioelectron. 2014, 53, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Cramp, A.P.; Sohn, J.H.; James, P.J. Detection of cutaneous myiasis in sheep using an ‘electronic nose’. Vet. Parasitol. 2009, 166, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Van Soolingen, D.; Hoogenboezem, T.; de Haas, P.E.; Hermans, P.W.; Koedam, M.A.; Teppema, K.S.; Brennan, P.J.; Besra, G.S.; Portaels, F.; Top, J.; et al. A novel pathogenic taxon of the Mycobacterium tuberculosis complex, Canetti: Characterization of an exceptional isolate from Africa. Int. J. Syst. Bacteriol. 1997, 47, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Niemann, S.; Rüsch-Gerdes, S.; Joloba, M.L.; Whalen, C.C.; Guwatudde, D.; Ellner, J.J.; Eisenach, K.; Fumokong, N.; Johnson, J.L.; Aisu, T.; et al. Mycobacterium africanum subtype II is associated with two distinct genotypes and is a major cause of human tuberculosis in Kampala, Uganda. J. Clin. Microbiol. 2002, 40, 3398–3405. [Google Scholar] [CrossRef] [PubMed]
- Niobe-Eyangoh, S.N.; Kuaban, C.; Sorlin, P.; Cunin, P.; Thonnon, J.; Sola, C.; Rastogi, N.; Vincent, V.; Gutierrez, M.C. Genetic biodiversity of Mycobacterium tuberculosis complex strains from patients with pulmonary tuberculosis in Cameroon. J. Clin. Microbiol. 2003, 41, 2547–2553. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.A. Mycobacterial infections in reptiles. Vet. Clin. Exot. Anim. 2012, 15, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Abbas, A.K.; Fausto, N.; Mitchell, R.N. Robbins Basic Pathology, 8th ed.; Saunders; Elsevier: Philadelphia, PA, USA, 2007; pp. 516–522. ISBN 978-1-4160-2973-1. [Google Scholar]
- Thoen, C.; Lobue, P.; de Kantor, I. The importance of Mycobacterium bovis as a zoonosis. Vet. Microbiol. 2006, 112, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Acton, Q.A. Mycobacterium Infections: New Insights for the Healthcare Professional; ScholarlyEditions: Atlanta, GA, USA, 2011; p. 1968. ISBN 978-1-4649-0122-5. [Google Scholar]
- Pfyffer, G.E.; Auckenthaler, R.; van Embden, J.D.; van Soolingen, D. Mycobacterium canettii, the smooth variant of M. tuberculosis, isolated from a Swiss patient exposed in Africa. Emerg. Infect. Dis. 1998, 4, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Panteix, G.; Gutierrez, M.C.; Boschiroli, M.L.; Rouviere, M.; Plaidy, A.; Pressac, D.; Porcheret, H.; Chyderiotis, G.; Ponsada, M.; Van Oortegem, K.; et al. Pulmonary tuberculosis due to Mycobacterium microti: A study of six recent cases in France. J. Med. Microbiol. 2010, 59, 984–989. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. American Thoracic Society, Medical Section of the American Lung Association. Am. J. Respir. Crit. Care Med. 1997, 156, S1–S25. [Google Scholar] [CrossRef] [PubMed]
- Bento, J.; Silva, A.S.; Rodrigues, F.; Duarte, R. Diagnostic tools in tuberculosis. Acta Med. Port. 2011, 24, 145–154. [Google Scholar] [PubMed]
- Escalante, P. In the clinic. Tuberculosis. Ann. Intern. Med. 2009, 150, ITC61-614, quiz ITV616. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhang, R.; Wang, J.; Liu, L.; Zheng, Y.; Shen, Y.; Qi, T.; Lu, H. Interferon-gamma release assays for the diagnosis of active tuberculosis in HIV-infected patients: A systematic review and meta-analysis. PLoS ONE 2011, 6, e26827. [Google Scholar] [CrossRef] [PubMed]
- Foundation for Innovative New Diagnostics. Diagnostics for Tuberculosis: Global Demand and Market Potential; Special Programme for Research and Training in Tropical Diseases; World Health Organization: Geneva, Switzerland, 2006; pp. 36–37. ISBN 978-92-4-156330-7. [Google Scholar]
- National Collaborating Centre for Chronic Conditions (UK). Tuberculosis: Clinical Diagnosis and Management of Tuberculosis, and Measures for Its Prevention and Control; TB Clinical Guideline 117; National Institute for Health and Clinical Excellence: London, UK, 2011; pp. 42–121. ISBN 978-1-84936-537-6. [Google Scholar]
- Steingart, K.R.; Flores, L.L.; Dendukuri, N.; Schiller, I.; Laal, S.; Ramsay, A.; Hopewell, P.C.; Pai, M. Commercial serological tests for the diagnosis of active pulmonary and extrapulmonary tuberculosis: An updated systematic review and meta-analysis. PLoS Med. 2011, 8, e1001062. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, J.Z.; Everett, C.K.; Steingart, K.R.; Cattamanchi, A.; Huang, L.; Hopewell, P.C.; Pai, M. Interferon-γ release assays for active pulmonary tuberculosis diagnosis in adults in low- and middle-income countries: Systematic review and meta-analysis. J. Infect. Dis. 2011, 204 (Suppl. 4), S1120–S1129. [Google Scholar] [CrossRef] [PubMed]
- Sester, M.; Sotgiu, G.; Lange, C.; Giehl, C.; Girardi, E.; Migliori, G.B.; Bossink, A.; Dheda, K.; Diel, R.; Dominguez, J.; et al. Interferon-γ release assays for the diagnosis of active tuberculosis: A systematic review and meta-analysis. Eur. Respir. J. 2011, 37, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, H.; Köhler, N.; Reinhold, P.; Turner, C.; Chambers, M. Volatile organic compound (VOC) analysis for disease detection: Proof of principle for field studies detecting paratuberculosis and brucellosis. AIP Conf. Proc. 2009, 1137, 195–197. [Google Scholar] [CrossRef]
- Phillips, M.; Cataneo, R.N.; Condos, R.; Ring Erickson, G.A.; Greenberg, J.; La Bombardi, V.; Munawar, M.I.; Tietje, O. Volatile biomarkers of pulmonary tuberculosis in the breath. Tuberculosis 2007, 87, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Basa-Dalay, V.; Bothamley, G.; Cataneo, R.N.; Lam, P.K.; Natividad, M.P.; Schmitt, P.; Wai, J. Breath biomarkers of active pulmonary tuberculosis. Tuberculosis 2010, 90, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Du Preez, I.; Loots, D.T. New sputum metabolite markers implicating adaptations of the host to Mycobacterium tuberculosis, and vice versa. Tuberculosis 2013, 93, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Bruins, M.; Rahim, Z.; Bos, A.; van de Sande, W.W.J.; Endtz, H.P.; van Belkum, A. Diagnosis of active tuberculosis by e-nose analysis of exhaled air. Tuberculosis 2013, 93, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Gerber, N.N.; Lechevalier, H.A. Geosmin, an earthy-smelling compound isolated from actinomycetes. Appl. Microbiol. 1965, 13, 935–938. [Google Scholar] [PubMed]
- Grimm, C.C.; Lloyd, S.W.; Batista, R.; Zimba, P.V. Using microwave distillation-solid-phase-microextraction-gas chromatography-mass spectrometry for analyzing fish tissue. J. Chromatogr. Sci. 2000, 38, 289–296. [Google Scholar] [CrossRef] [PubMed]
- de Heer, K.; Kok, M.G.M.; Fens, N.; Weersink, E.J.M.; Zwinderman, A.H.; van der Schee, M.P.C.; Visser, C.E.; van Oers, M.H.J.; Sterk, P.J. Detection of airway colonization by Aspergillus fumigatus by use of electronic nose technology in patients with cystic fibrosis. J. Clin. Microbiol. 2016, 54, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Dettenkofer, M.; Wenzler-Röttele, S.; Babikir, R.; Bertz, H.; Ebner, W.; Meyer, E.; Rüden, H.; Gastmeier, P.; Daschner, F.D. Surveillance of nosocomial sepsis and pneumonia in patients with a bone marrow or peripheral blood stem cell transplant: A multicenter project. Clin. Infect. Dis. 2005, 40, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Cornillet, A.; Camus, C.; Nimubona, S.; Gandemer, V.; Tattevin, P.; Belleguic, C.; Chevrier, S.; Meunier, C.; Lebert, C.; Aupe, M.; et al. Comparison of epidemiological, clinical, and biological features of invasive aspergillosis in neutropenic and nonneutropenic patients: A 6-year survey. Clin. Infect. Dis. 2006, 43, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Robenshtok, E.; Gafter-Gvili, A.; Goldberg, E.; Weinberger, M.; Yeshurun, M.; Leibovici, L.; Paul, M. Antifungal prophylaxis in cancer patients after chemotherapy or hematopoietic stem-cell transplantation: Systematic review and meta-analysis. J. Clin. Oncol. 2007, 25, 5471–5489. [Google Scholar] [CrossRef] [PubMed]
- Barth, P.J.; Rossberg, C.; Koch, S.; Ramaswamy, A. Pulmonary aspergillosis in an unselected autopsy series. Pathol. Res. Pract. 2000, 196, 73–80. [Google Scholar] [CrossRef]
- Groll, A.H.; Shah, P.M.; Mentzel, C.; Schneider, M.; Just-Nuebling, G.; Huebner, K. Trends in the postmortem epidemiology of invasive fungal infections at a university hospital. J. Infect. 1996, 33, 23–32. [Google Scholar] [CrossRef]
- Aisner, J.; Wiernik, P.H.; Schimpff, S.C. Treatment of invasive aspergillosis: Relation of early diagnosis and treatment to response. Ann. Intern. Med. 1977, 86, 539–543. [Google Scholar] [CrossRef] [PubMed]
- von Eiff, M.; Roos, N.; Schulten, R.; Hesse, M.; Zuhlsdorf, M.; van de Loo, J. Pulmonary aspergillosis: Early diagnosis improves survival. Respiration 1995, 62, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.L.; Chen, Y.Q.; Wang, K.; Qin, S.M.; Wu, C.; Kong, J.L. Accuracy of BAL galactomannan in diagnosing invasive aspergillosis: A bivariate metaanalysis and systematic review. Chest 2010, 138, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Tukey, M.H.; Wiener, R.S. Population-based estimates of transbronchial lung biopsy utilization and complications. Respir. Med. 2012, 106, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Carr, I.M.; Koegelenberg, C.F.N.; von Groote-Bidlingmaier, F.; Mowlana, A.; Silos, K.; Haverman, T.; Diacon, A.H.; Bolliger, C.T. Blood loss during flexible bronchoscopy: A prospective observational study. Respiration 2012, 84, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Facciolongo, N.; Patelli, M.; Gasparini, S.; Lazzari, A.L.; Salio, M.; Simonassi, C.; Del Prato, B.; Zanoni, P. Incidence of complications in bronchoscopy: Multicentre prospective study of 20,986 bronchoscopies. Monaldi Arch. Chest Dis. 2009, 71, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Jin, F.; Mu, D.; Chu, D.; Fu, E.; Xie, Y.; Liu, T. Severe complications of bronchoscopy. Respiration 2008, 76, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Pue, C.A.; Pacht, E.R. Complications of fiberoptic bronchoscopy at a university hospital. Chest 1995, 107, 430–432. [Google Scholar] [CrossRef] [PubMed]
- Sibila, O.; Garcia-Bellmunt, L.; Giner, J.; Merino, J.L.; Suarez-Cuartin, G.; Torrego, A.; Solanes, I.; Castillo, D.; Valera, J.L.; Cosio, B.G.; et al. Identification of airway bacterial colonization by an electronic nose in chronic obstructive pulmonary disease. Respir. Med. 2014, 108, 1608–1614. [Google Scholar] [CrossRef] [PubMed]
- Shafiek, H.; Fiorentino, F.; Merino, J.L.; López, C.; Oliver, A.; Segura, J.; de Paul, I.; Sibila, O.; Agustí, A.; Cosío, B.G. Using the electronic nose to identify airway infection during COPD exacerbations. PLoS ONE 2015, 10, e0135199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragonieri, S.; Quaranta, V.N.; Carratu, P.; Ranieri, T.; Marra, L.; D’Alba, G.; Resta, O. An electronic nose may sniff out amyotrophic lateral sclerosis. Resp. Physiol. Neurobiol. 2016, 232, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Chapman, E.A.; Thomas, P.S.; Stone, E.; Lewis, C.; Yates, D.H. A breath test for malignant mesothelioma using an electronic nose. Eur. Respir. J. 2012, 40, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Brekelmans, M.P.; Fens, N.; Brinkman, P.; Bos, L.D.; Sterk, P.J.; Tak, P.P.; Gerlag, D.M. Smelling the Diagnosis: The Electronic Nose as Diagnostic Tool in Inflammatory Arthritis. A Case-Reference Study. PLoS ONE 2016, 11, e0151715. [Google Scholar] [CrossRef] [PubMed]
- Dragonieri, S.; Schot, R.; Mertens, B.J.; Le Cessie, S.; Gauw, S.A.; Spanevello, A.; Resta, O.; Willard, N.P.; Vink, T.J.; Rabe, K.F.; et al. An electronic nose in the discrimination of patients with asthma and controls. J. Allergy Clin. Immunol. 2007, 120, 856–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montuschi, P.; Santonico, M.; Mondino, C.; Pennazza, G.; Mantini, G.; Martinelli, E.; Capuano, R.; Ciabattoni, G.; Paolesse, R.; Di Natale, C.; et al. Diagnose performance of an electronic nose, fractional exhaled nitric oxide and lung function testing in asthma. Chest 2010, 137, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Aathithan, S.; Plant, J.C.; Chaudry, A.N.; French, G.L. Diagnosis of bacteriuria by detection of volatile organic compounds in urine using an automated headspace analyzer with multiple conducting polymer sensors. J. Clin. Microbiol. 2001, 39, 2590–2593. [Google Scholar] [CrossRef] [PubMed]
- Covington, J.A.; Westenbrink, E.W.; Ouaret, N.; Harbord, R.; Bailey, C.; O’Connell, N.; Cullis, J.; Williams, N.; Nwokolo, C.U.; Bardhan, K.D.; et al. Application of a novel tool for diagnosing bile acid diarrhoea. Sensors 2013, 13, 11899–11912. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.; Tummon, A.; Ogunfile, M.; Adebiyi, A.; Adefowora, A. Evaluation of a novel diagnostic test for bacterial vaginosis: The electronic nose. Int. J. STD AIDS 2003, 14, 114–118. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.; Pennazza, G.; Santonico, M.; Martinelli, E.; Roscioni, C.; Galluccio, G.; Paolesse, R.; Di Natale, C. An investigation on electronic nose diagnosis of lung cancer. Lung Cancer 2010, 68, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Joensen, O.; Paff, T.; Haarman, E.G.; Skovgaard, I.M.; Jensen, P.Ø.; Bjarnsholt, T.; Nielsen, K.G. Exhaled breath analysis using electronic nose in cystic fibrosis and primary ciliary dyskinesia patients with chronic pulmonary infections. PLoS ONE 2014, 9, e115584. [Google Scholar] [CrossRef] [PubMed]
- Saidi, T.; Zaima, O.; Moufida, M.; El Barib, N.; Ionescuc, R.; Bouchikhi, B. Exhaled breath analysis using electronic nose and gas chromatography–mass spectrometry for non-invasive diagnosis of chronic kidney disease, diabetes mellitus and healthy subjects. Sens. Actuators B 2018, 257, 178–188. [Google Scholar] [CrossRef]
- Westenbrink, E.; Arasaradnam, R.P.; O’Connell, N.O.; Bailey, C.; Nwokolo, C.; Bardhan, K.D.; Covington, J.A. Development and application of a new electronic nose instrument for the detection of colorectal cancer. Biosens. Bioelectron. 2015, 67, 733–738. [Google Scholar] [CrossRef] [PubMed]
- De Meij, T.G.; Larbi, I.B.; van der Schee, M.P.; Lentferink, Y.E.; Paff, T.; Terhaar Sive Droste, J.S.; Mulder, C.J.; van Bodegraven, A.A.; de Boer, N.K. Electronic nose can discriminate colorectal carcinoma and advanced adenomas by fecal volatile biomarker analysis: Proof of principle study. Int. J. Cancer 2014, 134, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Hakim, M.; Broza, Y.Y.; Billan, S.; Abdah-Bortnyak, R.; Kuten, A.; Tisch, U.; Haick, H. Detection of lung, breast, colorectal, and prostate cancers from exhaled breath using a single array of nanosensors. Br. J. Cancer 2010, 103, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, N.; Zakaria, A.; Omar, M.I.; Shakaff, A.Y.; Masnan, M.J.; Kamarudin, L.M.; Rahim, N.A.; Zakaria, N.Z.I.; Abdullah, A.A.; Othman, A.; et al. In-vitro diagnosis of single and poly microbial species targeted for diabetic foot infection using e-nose technology. BMC Bioinform. 2015, 16, 158. [Google Scholar] [CrossRef] [PubMed]
- Boilot, P.; Hines, E.; Gardner, J.; Pitt, R.; John, S.; Mitchell, J.; Morgan, D.W. Classification of bacteria responsible for ENT and eye infections using the Cyranose system. IEEE Sens. J. 2002, 2, 247–253. [Google Scholar] [CrossRef]
- Hakim, M.; Billan, S.; Tisch, U.; Peng, G.; Dvrokind, I.; Marom, O.; Abdah-Bortnya, R.; Kuten, A.; Haick, H. Diagnosis of head-and-neck cancer from exhaled breath. Br. J. Cancer 2011, 104, 1649–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covington, J.; Harbord, R.; Westenbrink, E.W.; Bailey, C.; O’Connell, N.; Dhaliwal, A.; Nwokolo, C.; Foley, A.; Marya, N.B.; Baptista, V.; et al. Detection of urinary volatile organic compounds in patients with inflammatory bowel disease and controls by an electronic nose—A transatlantic study. Gastroenterology 2014, 146, S795–S796. [Google Scholar] [CrossRef]
- De Meij, T.G.J.; de Boer, N.K.H.; Benninga, M.A.; Lentferink, Y.E.; de Groot, E.F.J.; van de Velde, M.E.; van Bodegraven, A.A.; van der Scheea, M.P. Faecal gas analysis by electronic nose as a novel, non-invasive method for assessment of active and quiescent paediatric inflammatory bowel disease: Proof of principle study. J. Crohn’s Colitis 2014, 8, 91–106. [Google Scholar] [CrossRef]
- Shepherd, S.F.; McGuire, N.D.; de Lacy Costello, B.P.; Ewen, R.J.; Jayasena, D.H.; Vaughan, K.; Ahmed, I.; Probert, C.S.; Ratcliffe, N.M. The use of a gas chromatograph coupled to a metal oxide sensor for rapid assessment of stool samples from irritable bowel syndrome and inflammatory bowel disease patients. J. Breath Res. 2014, 8, 026001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monasta, L.; Pierobon, C.; Princivalle, A.; Martelossi, S.; Marcuzzi, A.; Pasini, F.; Perbellini, L. Inflammatory bowel disease and patterns of volatile organic compounds in the exhaled breath of children: A case-control study using Ion Molecule Reaction-Mass Spectrometry. PLoS ONE 2017, 12, e0184118. [Google Scholar] [CrossRef] [PubMed]
- McGuire, N.D.; Ewen, R.J.; Costello, C.D.; Garner, C.E.; Probert, C.S.J.; Vaughan, K.; Ratcliffe, N.M. Towards point of care testing for C. difficile infection by volatile profiling, using the combination of a short multi-capillary gas chromatography column with metal oxide detection. Meas. Sci. Technol. 2014, 25, 065108. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Anguri, H.; Nonaka, A.; Kataoka, K.; Nagata, H.; Kita, J.; Shizukuishi, S. Clinical assessment of oral malodor by the electronic nose system. J. Dent. Res. 2004, 83, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Kharitonov, S. Exhaled markers of inflammatory lung disease, ready for routine monitoring. Swiss Med. Wkly. 2004, 134, 175–192. [Google Scholar] [PubMed]
- De Heer, K.; van der Schee, M.P.; Zwinderman, K.; van den Berk, I.A.; Visser, C.E.; van Oers, R.; Sterk, P.J. Invasive pulmonary aspergillosis in prolonged chemotherapy-induced neutropenia: A proof-of-principle study. J. Clin. Microbiol. 2013, 51, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Takahashi, Y.; Konishi, K.; Katsuumi, I. Association of odor from infected root canal analyzed by an electronic nose with isolated bacteria. J. Endod. 2007, 33, 1106–1109. [Google Scholar] [CrossRef] [PubMed]
- Berkhout, D.J.C.; Niemark, H.J.; Buijck, M.; van Weissenbruch, M.M.; Brinkman, P.; Benninga, M.A.; van Kaam, A.H.; Kramer, B.W.; Andriessen, P.; de Boer, N.K.H.; et al. Detection of sepsis in preterm infants by fecal volatile organic compounds analysis: A proof of principle study. J. Pediatr. Gastroenterol. Nutr. 2017, 65, e47–e52. [Google Scholar] [CrossRef] [PubMed]
- De Gennaro, G.; Dragonieri, S.; Longobardi, F.; Musti, M.; Stallone, G.; Trizio, L.; Tutino, M. Chemical characterization of exhaled breath to differentiate between patients with malignant pleural mesothelioma from subjects with similar professional asbestos exposure. Anal. Bioanal. Chem. 2010, 398, 3043–3050. [Google Scholar] [CrossRef] [PubMed]
- De Meij, T.G.; van der Schee, M.P.; Berkhout, D.J.; van de Velde, M.E.; Jansen, A.E.; Kramer, B.W.; van Weissenbruch, M.M.; van Kaam, A.H.; Andriessen, P.; van Goudoever, J.B.; et al. Early detection of necrotizing enterocolitis by fecal volatile organic compounds analysis. J. Pediatr. 2015, 167, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Finberg, J.P.M.; Schwartz, M.; Jeries, R.; Badarny, S.; Nakhleh, M.K.; Abu Daoud, E.; Ayubkhanov, Y.; Aboud-Hawa, M.; Broza, Y.Y.; Haick, H. Sensor array for detection of early stage Parkinson’s disease before medication. ACS Chem. Neurosci. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-Y.; Peng, H.-Y.; Chang, C.-J.; Chen, P.-C. Diagnostic accuracy of breath tests for pneumoconiosis using an electronic nose. J. Breath Res. 2017, 12, 016001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hockstein, N.G.; Thaler, E.R.; Torigian, D.; Miller, W.T., Jr.; Deffenderfer, O.; Hanson, C.W. Diagnosis of pneumonia with an electronic nose: Correlation of vapor signature with chest computed tomography scan findings. Laryngoscope 2004, 114, 1701–1705. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.W., III; Thaler, E.R. Electronic nose prediction of a clinical pneumonia score: Biosensors and microbes. Anesthesiology 2005, 102, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Dragonieri, S.; Brinkman, P.; Mouw, E.; Zwinderman, A.H.; Carratu´, P.; Resta, O.; Sterk, P.J.; Jonkers, R.E. An electronic nose discriminates exhaled breath of patients with untreated pulmonary sarcoidosis from controls. Respir. Med. 2013, 107, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Dutta, R.; Morgan, D.; Baker, N.; Gardner, J.W.; Hines, E.L. Identification of Staphylococcus aureus infections in hospital environment: Electronic nose based approach. Sens. Actuators B 2005, 109, 335–362. [Google Scholar] [CrossRef]
- Vaira, D.; Holton, J.; Ricci, C.; Basset, C.; Gatta, L.; Perna, F.; Tampieri, A.; Miglioli, M. Helicobacter pylori infection from pathogenesis to treatment: A critical reappraisal. Aliment. Pharm. Ther. 2002, 16, 105–113. [Google Scholar] [CrossRef]
- Lai, S.Y.; Deffenderfer, O.F.; Hanson, W.; Phillips, M.P.; Thaler, E.R. Identification of upper respiratory bacterial pathogens with the electronic nose. Laryngoscope 2002, 112, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Roine, A.; Saviauk, T.; Kumpulainen, P.; Karjalainen, M.; Tuokko, A.; Aittoniemi, J.; Vuento, R.; Lekkala, J.; Lehtima, T.; Tammela, T.L.; et al. Rapid and accurate detection of urinary pathogens by mobile IMS-based electronic nose: A Proof-of-principle study. PLoS ONE 2014, 9, e114279. [Google Scholar] [CrossRef] [PubMed]
- Hockstein, N.G.; Thaler, E.R.; Lin, Y.; Lee, D.D.; Hanson, C.W. Correlation of pneumonia score with electronic nose signature: A prospective study. Ann. Otol. Rhinol. Laryngol. 2005, 114, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.M.; Boumans, M.L.L.; Smolinska, A.; Stobberingh, E.E.; Kaufmann, R.; Roekaerts, P.M.H.J.; Bergmans, D.C.J.J. Electronic nose analysis of exhaled breath to diagnose ventilator associated pneumonia. Respir. Med. 2015, 109, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Xu, X.; Shen, Y.; Yan, J.; He, Q.; Ma, J.; Liu, T. Detection of wound pathogen by an intelligent electronic nose. Sens. Mater. 2009, 21, 155–166. [Google Scholar]
- Saviauk, T.; Kiiski, J.P.; Nieminen, M.K.; Tamminen, N.N.; Roine, A.N.; Kumpulainen, P.S.; Hokkinen, L.J.; Karjalainen, M.T.; Vuento, R.E.; Aittoniemi, J.J.; et al. Electronic nose in the detection of wound infection bacteria from bacterial cultures: A proof-of-principle study. Eur. Surg. Res. 2018, 59, 1–11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Surveillance, Prevention and Control of Chronic Respiratory Diseases: A Comprehensive Approach. Available online: http://www.who.int/respiratory/publications/global_surveillance/en (accessed on 27 August 2018).
- Balmes, J.; Becklakem, M.; Blanc, P.; Henneberger, P.; Kreiss, K.; Mapp, C.; Milton, D.; Schwartz, D.; Toren, K.; Viegi, G. American Thoracic Society statement: Occupational contribution to the burden of airway disease. Am. J. Respir. Crit. Care Med. 2003, 167, 787–797. [Google Scholar] [CrossRef]
- Cohen, R.A. Resurgent coal mine dust lung disease: Wave of the future or a relic of the past? Occup. Environ. Med. 2016, 73, 715–716. [Google Scholar] [CrossRef] [PubMed]
- Joshi, T.K.; Gupta, R.K. Asbestos in developing countries: Magnitude of risk and its practical implications. Int. J. Occup. Med. Environ. Health 2004, 17, 179–185. [Google Scholar] [CrossRef]
- Capelli, L.; Taverna, G.; Bellini, A.; Eusebio, L.; Buffi, N.; Lazzeri, M.; Guazzoni, G.; Bozzini, G.; Seveso, M.; Mandressi, A.; et al. Application and uses of electronic noses for clinical diagnosis on urine samples: A review. Sensors 2016, 16, 1708. [Google Scholar] [CrossRef] [PubMed]
- Horstmann, M.; Steinbach, D.; Fischer, C.; Enkelmann, A.; Grimm, M.; Voss, A. An electronic nose system detects bladder cancer in urine specimen: First results of a pilot study. J. Urol. 2015, 193, 560–561. [Google Scholar] [CrossRef]
- Pendharkar, S.; Mehta, S. The clinical significance of exhaled nitric oxide in asthma. Can. Respir. J. 2008, 15, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Martins, M.A.; Tibério, I.F. Nitric oxide in asthma physiopathology. ISRN Allergy 2011, 19, 832560. [Google Scholar] [CrossRef] [PubMed]
- Lacey, J.N.; Kidel, C.; van der Kaaij, J.M.; Brinkman, P.; Gilbert-Kawai, E.T.; Grocott, M.P.W.; Mythen, M.G.; Martin, D.S. The Smell of Hypoxia: Using an electronic nose at altitude and proof of concept of its role in the prediction and diagnosis of acute mountain sickness. Physiol. Rep. 2018, 6, e13854. [Google Scholar] [CrossRef] [PubMed]
- Lüscher, T.F.; Barton, M. Biology of the endothelium. Clin. Cardiol. 1997, 20, 3–10. [Google Scholar]
- Ma, F.X.; Zhou, B.; Chen, Z.; Ren, Q.; Lu, S.H.; Sawamura, T.; Han, Z.C. Oxidized low density lipoprotein impairs endothelial progenitor cells by regulation of endothelial nitric oxide synthase. J. Lipid Res. 2006, 47, 1227–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abramson, S.B. Nitric oxide in inflammation and pain associated with osteoarthritis. Arthritis Res. Ther. 2008, 10, S2. [Google Scholar] [CrossRef] [PubMed]
- Maki-Petaja, K.M.; Cheriyan, J.; Booth, A.D.; Hall, F.C.; Brown, J.; Wallace, S.M.; Ashby, M.J.; McEniery, C.M.; Wilkinson, I.B. Inducible nitric oxide synthase activity is increased in patients with rheumatoid arthritis and contributes to endothelial dysfunction. Int. J. Cardiol. 2008, 129, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Van der Vliet, A.; Eiserich, J.P.; Cross, C.E. Nitric oxide: A pro-inflammatory mediator in lung disease? Respir. Res. 2000, 1, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhillon, S.S.; Mastropaolo, L.A.; Murchie, R.; Griffiths, C.; Thöni, C.; Elkadri, A.; Xu, W.; Mack, A.; Walters, T.; Guo, C.; et al. Higher activity of the inducible nitric oxide synthase contributes to very early onset inflammatory bowel disease. Clin. Transl. Gastroenterol. 2014, 5, e46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasbohm, E.; Fischer, S.; Küntzel, A.; Oertel, P.; Bergmann, A.; Trefz, P.; Miekisch, W.; Schubert, J.K.; Reinhold, P.; Ziller, M.; et al. Strategies for the identification of disease-related patterns of volatile organic compounds: Prediction of paratuberculosis in an animal model using random forests. J. Breath Res. 2017, 11, 047105. [Google Scholar] [CrossRef] [PubMed]
- Durán-Acevedo, C.M.; Jaimes-Mogollón, A.L.; Gualdrón-Guerrero, O.E.; Welearegay, T.G.; Martinez-Marín, J.D.; Caceres-Tarazona, J.M.; Sánchez-Acevedo, Z.C.; Beleño-Saenz, K.J.; Cindemir, U.; Österlund, L.; et al. Exhaled breath analysis for gastric cancer diagnosis in Colombian patients. Oncotarget 2018, 9, 28805–28817. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.Q.; Broza, Y.Y.; Ionsecu, R.; Tisch, U.; Ding, L.; Liu, H.; Song, Q.; Pan, Y.Y.; Xiong, F.X.; Gu, K.S.; et al. A nanomaterial-based breath test for distinguishing gastric cancer from benign gastric conditions. Br. J. Cancer 2013, 108, 941–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amal, H.; Leja, M.; Broza, Y.Y.; Tisch, U.; Funka, K.; Liepniece-Karele, I.; Skapars, R.; Xu, Z.Q.; Liu, H.; Haick, H. Geographical variation in the exhaled volatile organic compounds. J. Breath Res. 2013, 7, 047102. [Google Scholar] [CrossRef] [PubMed]
- El Manouni El Hassani, S.; Berkhout, D.J.C.; Bosch, S.; Benninga, M.A.; de Boer, N.K.H.; de Meij, T.G.J. Application of fecal volatile organic compound analysis in clinical practice: Current state and future perspectives. Chemosensors 2018, 6, 29. [Google Scholar] [CrossRef]
- Bosch, S.; El Manouni El Hassani, S.; Covington, J.A.; Wicaksono, A.N.; Bomers, M.K.; Benninga, M.A.; Mulder, C.J.J.; de Boer, N.K.H.; de Meij, T.G.J. Optimized sampling conditions for fecal volatile organic compound analysis by means of field asymmetric ion mobility spectrometry. Anal. Chem. 2018, 90, 7972–7981. [Google Scholar] [CrossRef] [PubMed]
- Kou, L.; Zhang, D.; Liu, D. A novel medical e-nose signal analysis system. Sensors 2017, 17, 402. [Google Scholar] [CrossRef] [PubMed]
- Electronic ‘Nose’ Offers Rapid Epilepsy Diagnosis. Available online: https://www.medscape.com/viewarticle/889666 (accessed on 24 August 2018).

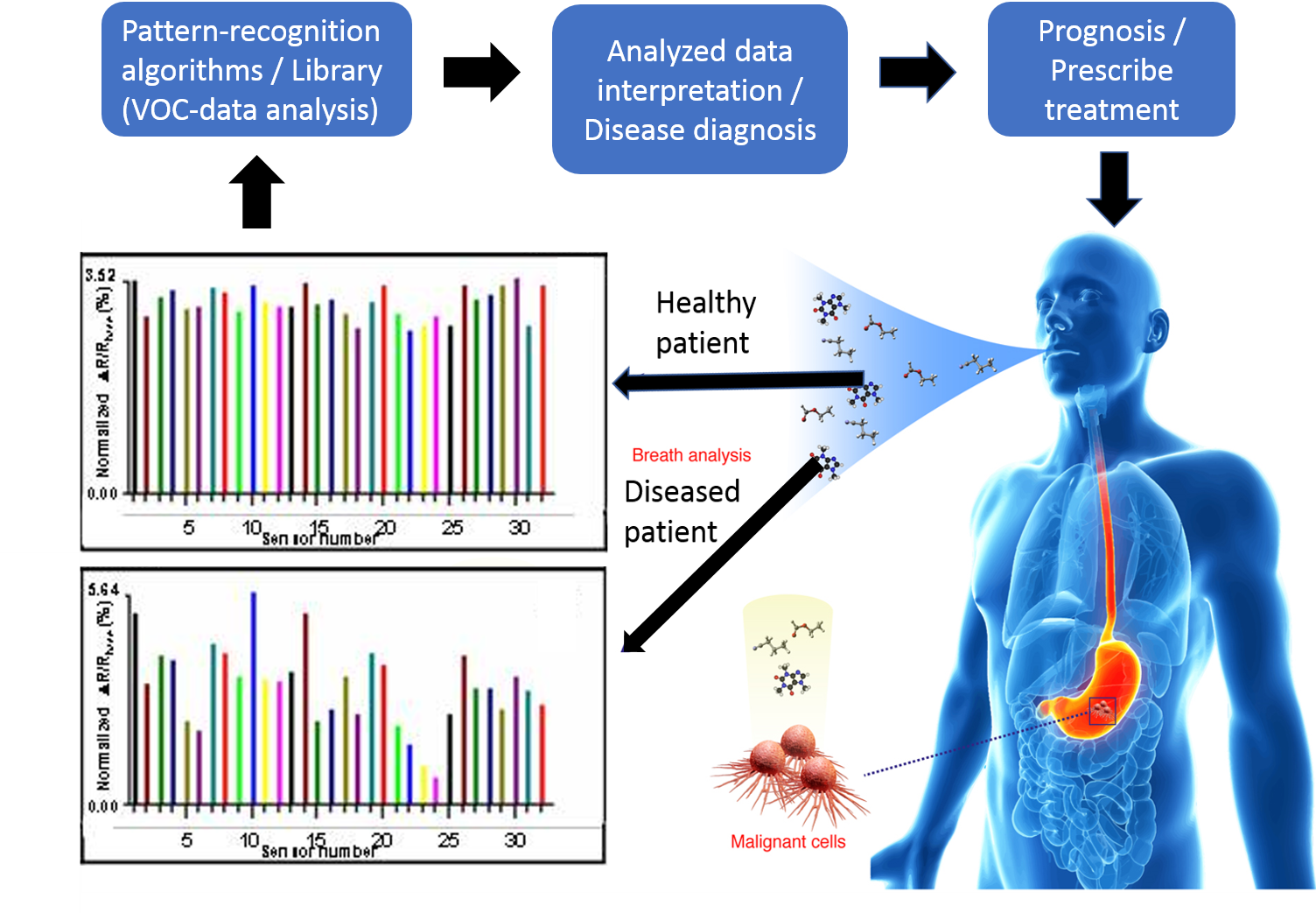{kind=link}
Table 1.
Chemical classes and molecular structures of representative volatile organic compounds (VOCs) biomarker metabolites associated with specific plant, animal, and human diseases.
Table 1.
Chemical classes and molecular structures of representative volatile organic compounds (VOCs) biomarker metabolites associated with specific plant, animal, and human diseases.
| Disease 1 | Pathogen | Host 2 | Location | Biomarkers | Chemical Class | Molecular Structure | References |
|---|---|---|---|---|---|---|---|
| Fire blight | Erwinia amylovora | Apple | Leaves | Phenylethyl alcohol | Benzene alcohol |  | [33,34] |
| Gray mold | Botrytis cinerea | Tomato | Leaves | α-Copaene | Tricyclic sesquiterpene |  | [35] |
| Powdery mildew | Oidium neolycopersici | Tomato | Leaves | 1-Fluorododecane | Fluoro-aliphatic HC |  | [36] |
| Bovine tuberculosis | Mycobacterium bovis | Cattle | Lungs | 1,3-Dimethylbutyl cycloalkane | Cycloalkane |  | [37] |
| Infective endocarditis | Staphylococcus spp. | Human | Heart | Methanethiol | Organosulfur |  | [38,39,40,41] |
| COPD, CF | Abiotic, noninfectious | Human | Lungs | Nitrotyrosine | Tyrosine deriv. |  | [42] |
1 Disease name abbreviations: CF = cystic fibrosis; COPD = chronic obstructive pulmonary disease; 2 Plant host scientific names: Apple (Malus domestica); Tomato (Lycopersicon esculentum).
Table 2.
Applications of electronic-nose devices to detect plant diseases associated with specific host-pathogen and pest combinations.
Table 2.
Applications of electronic-nose devices to detect plant diseases associated with specific host-pathogen and pest combinations.
| Plant Hosts 1 | Plant Part/Location | Disease Type | Pathogens/Pests | E-nose Model | E-nose Type/Sensor No. 2 | References |
|---|---|---|---|---|---|---|
| Apple | Fruit | Post-harvest rot | Unspecified | FOX 4000 | MOS 18 | [81] |
| Leaves; shoots | Fire blight, Bacterial blast | Erwinia amylovora, Pseudomonas syringae | EOS-507C/PEN3 | MOS 6, MOS 10 | [34] | |
| Leaves | Fire blight | Erwinia amylovora | EOS-835 | MOS 6 | [74] | |
| Barley | Grain | Toxigenic infestation | Aspergillus ochraceus, Aspergillus carbonarius, Penicillium verrucosum, Fusarium. graminearum, Fusarium culmorum | VCM 422 | MOSFET 10, MOS 6, Gascard CO2 1 | [82] |
| Basswood | Wood | Bacterial wetwood | Anaerobic bacteria | Aromascan A32S | CP 32 | [83] |
| Beech, Black cherry | Wood | Bacterial wetwood | Anaerobic bacteria | Aromascan A32S | CP 32 | [84] |
| Blueberry | Fruit | Fruit rot | Botrytis cinerea, Colletotrichum gloeosporioides, Alternaria species | Cyranose 320 | CBPC 32 | [85] |
| Fruit | Quality rating | unspecified | TGS 822 | MOS 2 | [86] | |
| Corn | Grain | Aflatoxins | Aspergillus flavus | PEN 2 | MOS 10 | [87,88] |
| Toxigenic infestation | Fusarium verticillioides | EOS 835 | MOS 6 | [89] | ||
| Cotton | Bolls | Wounding | Anthonomus grandis | Cyranose 320 | CBPC 32 | [90] |
| Cottonwood | Wood | Bacterial wetwood | Clostridium spp. | Aromascan A32S | CP 32 | [10] |
| Cucumber | Leaves | Spider mite | Unidentified | Bloodhound ST214 | CP 14 | [66] |
| Elm | Wood | Bacterial wetwood | Anaerobic bacteria | Aromascan A32S | CP 32 | [83] |
| Grape | Root | Root galls | Agrobacterium vitis | PEN 3 | MOS 10 | [91,92] |
| Kiwi | Fruit | Bacterial canker | Pseudomonas syringae pv. actinidiae | EOS-507C/PEN3 | MOS 6, MOS10 | [76] |
| Fruit rot | Botrytis cinerea, Sclerotinia sclerotiorum | EOS 835 | MOS 6 | [93] | ||
| Oaks | Sapwood | Oak wilt | Ceratocystis fagacearum | Aromascan A32S | CP 32 | [10,94] |
| Roots | Root rots | Armillaria mellea, Ganoderma lucidum, Heterobasidion annosum | PEN3 | MOS 10 | [95] | |
| Bole | Wood decay | Many wood decay fungi | Aromascan A32S, LibraNose 2.1, PEN 3 | CP 32, QMB 8, MOS 10 | [10,77] | |
| Oil palm | Lower bole | Basal stem rot | Ganoderma boninense | Cyranose 320 | CBPC 32 | [62] |
| Onion | Bulbs | Sour skin | Burkholderiacepacia | Owlstone | FAIMS | [96] |
| Orange | Fruit | Citrus greening | Liberibacter asiaticus | Agilent 6890 GC | MS 1 | [97] |
| Fruit rot | Penicillium spp. | LibraNose 2.1 | QMB 8 | [98] | ||
| Ornamental palm | Crown, trunk, leaves | Wounding | Rhynchophorus ferrugineous | PEN 3 | MOS 10 | [63] |
| Pear | Fruit | Post-harvest rot | Unspecified | FOX 4000 | MOS 18 | [81] |
| Pepper | Plants | Wounding | Unidentified | Bloodhound ST214 | CP 14 | [66] |
| Pine | Wood in service | Wood decay | Serpula lacrymans | Prototype | CP 10 | [99] |
| Potato | Tubers | Storage soft rot | Ralstonia solanacearum, Clavibacter michiganensis spp. sepedonicus, Pectobacterium species | Prototype | MOS 8 | [100] |
| Ralstonia solanacearum, Clavibacter michiganensis spp. sepedonicus | PEN 3 | MOS 10 | [101] | |||
| Pectobacterium carotovorum | WOLF 4.1 | EC 9, NDIR 2 | [102] | |||
| Rice | Stalks | Wilting | Nilaparvata lugens | PEN 2 | MOS 10 | [103,104] |
| Strawberry | Fruit | Fruit rot | Botrytis, Fusarium, and Penicillium spp. | PEN 3 | MOS 10 | [105] |
| Tomato | Leaves | Powdery mildew | Oidium neolycopersici | Bloodhound ST214 | CP 14 | [66] |
| Seedling | Gray mold | Botrytis cinerea | PEN 2 | MOS 10 | [106] | |
| Wheat | Grain | Decay | Penicillium chrysogenum, Fusarium verticillioides | LibraNose 2.1 | QMB 8 | [107] |
| Fusarium spp. | Prototype | QMB 8 | [108] | |||
| Rhyzopertha dominica | PEN 2 | MOS 10 | [109] |
1 Plant host scientific names: Apple (Malus domestica), Barley (Hordeum vulgare), Basswood (Tilia americana), Beech (Fagus grandifolia), Black cherry (Prunus serotina), Blueberry (Vaccinium spp.), Corn (Zea mays), Cotton (Gossypium hirsutum), Cottonwood (Populus deltoides), Cucumber (Cucumis sativus), Elm (Ulmus americana), Grape (Vitis vinifera), Kiwi (Actinidia deliciosa), Oaks (Quercus spp.), Oil palm (Elaeis guineensis), Onion (Allium cepa); Orange (Citrus sinensis), Ornamental palm (Phoenix canariensis), Pear (Prunus communis), Pepper (Capsicum annuum), Pine (Pinus spp.), Potato (Solanum tuberosum), Rice (Secale cereale), Strawberry (Fragaria ananassa), Tomato (Lycopersicon esculentum), Wheat (Triticum aestivum); 2 Electronic nose (e-nose) sensor types and numbers (in sensor array): CBPC = carbon black polymer composite; CO2 = carbon dioxide; CP = conducting polymer; EC = electrochemical; FAIMS = field asymmetric ion mobility spectroscopy; GC-FID = gas chromatography using flame ionization detector; GNP = gold nanoparticle; MOS = metal oxide semiconductor; MOSFET = membrane-oxide semiconductor field-effect transistor; MS = mass spectroscopy; NDIR = nondispersive infrared; QMB = quartz crystal microbalance.
Table 3.
Applications of electronic-nose devices used in veterinary diagnostic pathology to detect animal diseases.
Table 3.
Applications of electronic-nose devices used in veterinary diagnostic pathology to detect animal diseases.
| Animal 1 | Disease 2 | VOC Sample Type | Pathogens/Pests/Disorder | E-nose Model | E-nose Type, Sensor No. 3 | References |
|---|---|---|---|---|---|---|
| Badgers (Eurasian) | Bovine TB | Blood serum | Mycobacterium bovis | Bloodhound BH-114 | CP 14 | [126] |
| Bats (cave-dwelling) | White-nose syndrome (WNS) | Pure culture of pathogen isolated from bat skin | Pseudogymnoascus destructans | Heracles II | GC-FID 1, MOS 100s | [127,128] |
| Catfish | Flesh off-flavor | Filleted meat | Geosmin-producing aquatic Actinomycetes | Aromascan A32S | CP 32 | [129] |
| Chicken | Salmonella contamination (SC) | Meat product | Salmonella typhimurium | Spreeta | SPRB | [130] |
| Cows (cattle) | BRD | Blood serum | Mannheimia haemolytica | Bloodhound ST-214 | CP 13 | [131] |
| Bovine TB | Blood serum | Mycobacterium bovis | Bloodhound BH-114 | CP 14 | [126] | |
| Exhaled breath | Mycobacterium bovis | NA-NOSE | GNP 6 | [37] | ||
| Hyperketonaemia | Exhaled breath, milk | Metabolic disorder | Metabolomics | MS | [132] | |
| Rats | ALF | Exhaled breath | Liver cell necrosis, ischemia | eNose | MOS 8 | [133] |
| Sheep | CM | Skin | Lucilia cuprina (fly larvae) | Prototype | MOS 6 | [134] |
1 Animal host scientific names: Badgers (Meles meles); Bats (Eptesicus spp., Myotis spp., Perimyotis spp.), Catfish (Ictalurus punctatus); Chicken (Gallus gallus subsp. domesticus); Cows (Bos taurus); Rats (Rattus norvegicus); Sheep (Ovis aries); 2 Disease name abbreviations: ALF = acute liver failure; BRD = bovine respiratory disease; CM = cutaneous myiasis; SC = Salmonella contamination and infection; TB = tuberculosis; WNS = white-nose syndrome; 3 Electronic-nose sensor types and numbers (in sensor array): CP = conducting polymer; GC-FID = gas chromatography using flame ionization detector; GNP = gold nanoparticle; MOS = metal oxide semiconductor; MS = mass spectroscopy; SPRB = surface plasmon resonance biosensor; Model NA-NOSE = Nano Artificial NOSE.
Table 4.
Clinical applications of electronic-nose devices for detection of human diseases in Point-Of-Care (POC) testing.
Table 4.
Clinical applications of electronic-nose devices for detection of human diseases in Point-Of-Care (POC) testing.
| Disease Name 1 | Location 2 | VOC Sample Type | Pathogen/Disorder 2 | e-Nose Model | e-Nose Type, Sensor No. 3 | References |
|---|---|---|---|---|---|---|
| ABI | Lung | Exhaled-air cultures | Pseudomonas aeruginosa, Haemophilus influenza, Streptococcus pneumoniae, Moraxella catarrhalis, Staphylococcus aureus | Cyranose 320 | CBPC 32 | [174,175] |
| ALS | Muscles | Exhaled breath | Neurodegenerative muscular disease | Cyranose 320 | CBPC 32 | [176] |
| ARDS | Lung | Exhaled breath | Lung inflammation | Cyranose 320 | CBPC 32 | [177] |
| Arthritis | Joints | Exhaled breath | Joint inflammation | Cyranose 320 | CBPC 32 | [178] |
| Asthma | Lung | Exhaled breath | Bronchial inflammation & obstruction | Cyranose 320 | CBPC 32 | [179] |
| Lung | Exhaled breath | Bronchial inflammation & obstruction | Prototype, NIOX | QMB 8, NOS 1 | [180] | |
| Bacteriuria | Urinary tract | Urine | Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Staphylococcus aureus, Staphylococcus saprophyticus, Enterococcus faecalis | Osmetech Microbial Analyzer | CP 4 | [181] |
| BAD | Bowel | Urine | Bile acid malabsorption | Fox 4000 | MOS 18 | [182] |
| BV | Vagina | Intravaginal swab culture | Neisseria gonorrhoeae, Chlamydia trachomatis, Trichomonas vaginalis | Osmetech Microbial Analyzer | CP 4 | [183] |
| Cancer | Lung | Exhaled breath | Abnormal cell growth | Prototype | QMB 8 | [184] |
| CF | Lung | Exhaled breath | Genetic disease of the mucus and sweat glands | Cyranose 320 | CBPC 32 | [185] |
| COPD | Lung | Lung bacterial cultures | Hemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis, gram negative-bacilli, Pseudomonas aeruginosa, Staphylococcus aureus, Streptococcus viridans, Candida species, Corynebacterium spp., Staphylococcus epidermidis | Cyranose 320 | CBPC 32 | [174] |
| CKD | Kidney | Exhaled breath | Multiple causes | Prototype | MOS 6 | [186] |
| CRC | Colon | Urine | Abnormal cell growth | WOLF | EC 8, NDIR 2, PID 1 | [187] |
| Colon | Fecal | Abnormal cell growth | Cyranose 320 | CBPC 32 | [188] | |
| Colon | Breath | Abnormal cell growth | Prototype | GNP 14 | [189] | |
| DFI | Foot | Wound bacterial cultures | Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli | Cyranose 320 | CBPC 32 | [190] |
| DM | Systemic | Exhaled breath | Insufficient insulin production | Prototype | MOS 6 | [186] |
| EI | Eye | Eye swab broth cultures | Staphylococcus aureus, Haemophilus influenzae, Streptococcus pneumoniae, Escherichia coli, Pseudomonas aeruginosa, Moraxella catarrhalis | Cyranose 320 | CBPC 32 | [191] |
| ENT | Ear, nose, & throat | Sputum swab cultures | Staphylococcus aureus, Staphylococcus epidermis, Streptococcus pneumoniae, Pseudomonas aeruginosa | Cyranose 320 | CBPC 32 | [191] |
| HNC | Head, neck | Breath | Cancer | NA-NOSE | GNP 5 | [192] |
| IBD | Intestine | Urine | Unknown cause | Owlstone | FAIMS | [193] |
| Colon | Fecal | Unknown cause | Cyranose 320 | CBPC 32 | [194] | |
| Colon | Urine | Unknown cause | WOLF | EC 8, NDIR 2, PID 1 | [186] | |
| IBS | Colon | Fecal | Gastrointestinal disorder | Prototype | GC-MOS 1 | [195] |
| Colon | Aveolar breath | Gastrointestinal disorder | V&F Airsense | IMR-MS | [196] | |
| ID | Colon | Fecal | Gastroenteritis | Prototype | GC-MOS 1 | [197] |
| IEC | Heart | Oral cavity air | Bacterial inflammation of the endocardium | Prototype | MOS 6 | [198] |
| ILD | Lung | Exhaled breath | Unknown cause | NIOX | NOS 1 | [199] |
| IPA | Lungs | Exhaled breath | Aspergillus species | Cyranose 320 | CBPC 32 | [160,200] |
| IRC | Teeth | Root canal culture | Prevotella, Porphyromonas, Fusobacterium, and Bacteroides species | Shimadzu FF-1 | MOS 10 | [201] |
| LOS | Systemic | Fecal | Bacteremia | Cyranose 320 | CBPC 32 | [202] |
| MPM | Lung | Exhaled breath | Cancer of pleura tissue caused by inhalation of asbestos fibers | Cyranose 320 | CBPC 32 | [177,203] |
| NEC | Colon | Fecal | Unknown cause | Cyranose 320 | CBPC 32 | [204] |
| PA | Joints | Exhaled breath | Inflammatory joint disease | Cyranose 320 | CBPC 32 | [178] |
| PD | Systemic | Exhaled breath | Neurodegenerative disease | Prototype | GNP, CNT 40 | [205] |
| Pneumoconiosis | Lung | Exhaled breath | Occupational inhalation of dust causing inflammation | Cyranose 320 | CBPC 32 | [206] |
| Pneumonia (bacterial) | Lung | Exhaled breath | Bacterial lung infection | Cyranose 320 | CBPC 32 | [207] |
| Lung | Exhaled breath | Bacterial lung infection | Prototype | BS | [208] | |
| PS | Lung | Exhaled breath | Systemic granulomatous disease | Cyranose 320 | CBPC 32 | [209] |
| RA | Joints | Exhaled breath | Inflammatory joint disease | Cyranose 320 | CBPC 32 | [178] |
| SI | Skin, others | Skin swab culture | Staphylococcus aureus | Cyranose 320 | CBPC 32 | [210] |
| TB | Lung | Exhaled air | Mycobacterium tuberculosis | DiagNose | MOS 12 | [157] |
| Ulcer | Stomach | Exhaled breath | Helicobacter pylori | Prototype | NH4 | [211] |
| URTI | Upper respiratory tract | Exhaled breath | Bacterial pathogens | Cyranose 320 | CBPC 32 | [212] |
| UTI | Urinary tract | Urine | Staphylococcus saprophyticus, Escherichia coli, Enterococcus faecalis, Klebsiella species | ChemPro 100i | IMS 8, MOS 6 | [213] |
| VAP | Lung | Exhaled air | Bacterial pathogens | Cyranose 320 | CBPC 32 | [207,214] |
| Lung | Exhaled breath | Bacterial pathogens | DiagNose | MOS 3 | [215] | |
| WI | Skin | Skin wound cultures | Staphylococcus aureus, Staphylococcus epidermis, Streptococcus pyogenes, Acinetobacter baumannii, Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa | Prototype | MOS 6, EC 1 | [216] |
| Skin | Skin wound cultures | Staphylococcus aureus (MSSA), methicillin-resistant Staphylococcus aureus (MRSA), Streptococcus pyogenes, Escherichia coli, Pseudomonas aeruginosa, Clostridium perfringens | ChemPro 100i | IMS 8, MOS 6 | [217] |
1 Disease name abbreviations: ABI = Airway bacterial infection; ALS = amyotrophic lateral sclerosis; ARDS = acute respiratory distress syndrome; BAD = Bile acid diarrhea; BV = bacterial vaginosis; CF = cystic fibrosis; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; CRC = colorectal cancer; DFI = diabetic foot infection; DM = diabetes mellitus; EI = eye infections; ENT = ear, nose and throat infections; HNC = head and neck cancer; IBD = inflammatory bowel disease; IBS = irritable bowel syndrome; ID = Infectious diarrhea; IEC = infective endocarditis; ILD = inflammatory lung disease; IPA = invasive pulmonary aspergillosis; IRC = infected root canal; LOS = late-onset sepsis; MPM = malignant pleural mesothelioma; NEC = Necrotizing enterocolitis; PA = psoriatic arthritis; PD = Parkinson’s disease; PS = pulmonary sarcoidosis; RA = rheumatoid arthritis; SI = Staphylococcus infection; TB = tuberculosis (active); URTI = upper respiratory tract infection; UTI = urinary tract infections; VAP = Ventilator-associated pneumonia; WI = wound infection; 2 Pathogen/Disorder indicates the biotic causal agent (microbe) of infectious diseases or abiotic disorders and their disease mechanism or category; 3 Electronic-nose gas sensor type symbol abbreviations: BS = biosensor; CBPC = carbon black polymer composite; CNT = carbon nanotubes; CP = conducting polymer; EC = electrochemical sensor; FAIM = field asymmetric ion mobility spectroscopy; GNP = gold nanoparticles; IMR-MS = Ion Molecule Reaction-Mass Spectrometry; IMS = ion mobility spectrometry; MOS = metal oxide semiconductor, NH4 = ammonia sensor; NDIR = Non-Dispersive Infra-red (optical devices); NOS = nitric oxide sensor, PID = Photo-Ionization Detector; QMB = quartz crystal microbalance.
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wilson, A.D. Applications of Electronic-Nose Technologies for Noninvasive Early Detection of Plant, Animal and Human Diseases. Chemosensors 2018, 6, 45. https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors6040045
AMA Style
Wilson AD. Applications of Electronic-Nose Technologies for Noninvasive Early Detection of Plant, Animal and Human Diseases. Chemosensors. 2018; 6(4):45. https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors6040045
Chicago/Turabian StyleWilson, Alphus Dan. 2018. "Applications of Electronic-Nose Technologies for Noninvasive Early Detection of Plant, Animal and Human Diseases" Chemosensors 6, no. 4: 45. https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors6040045
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.