
Are Neurophysiological Biomarkers Able to Discriminate Multiple Sclerosis Clinical Subtypes?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
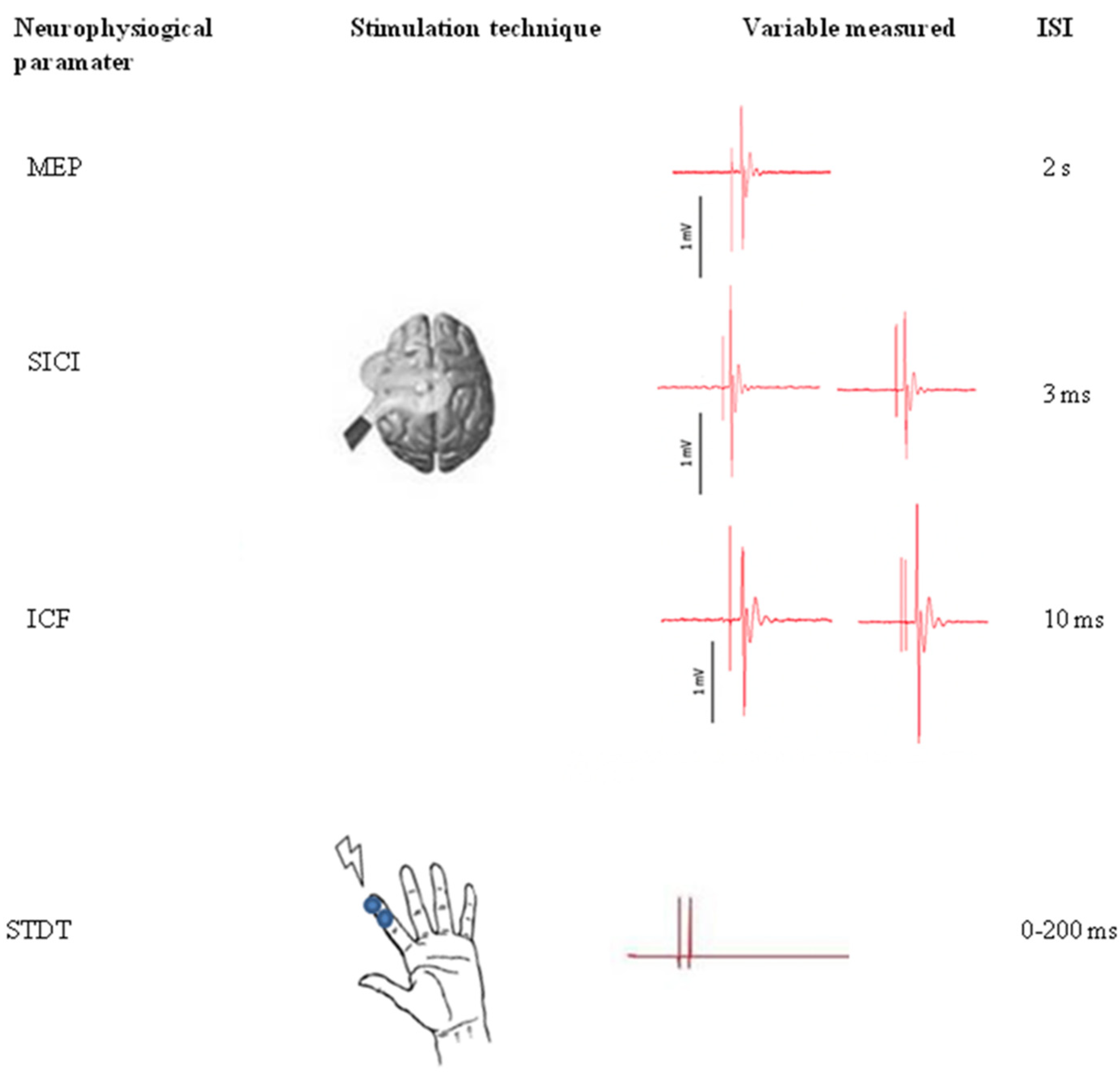
2.2. Neurophysiological Assessment
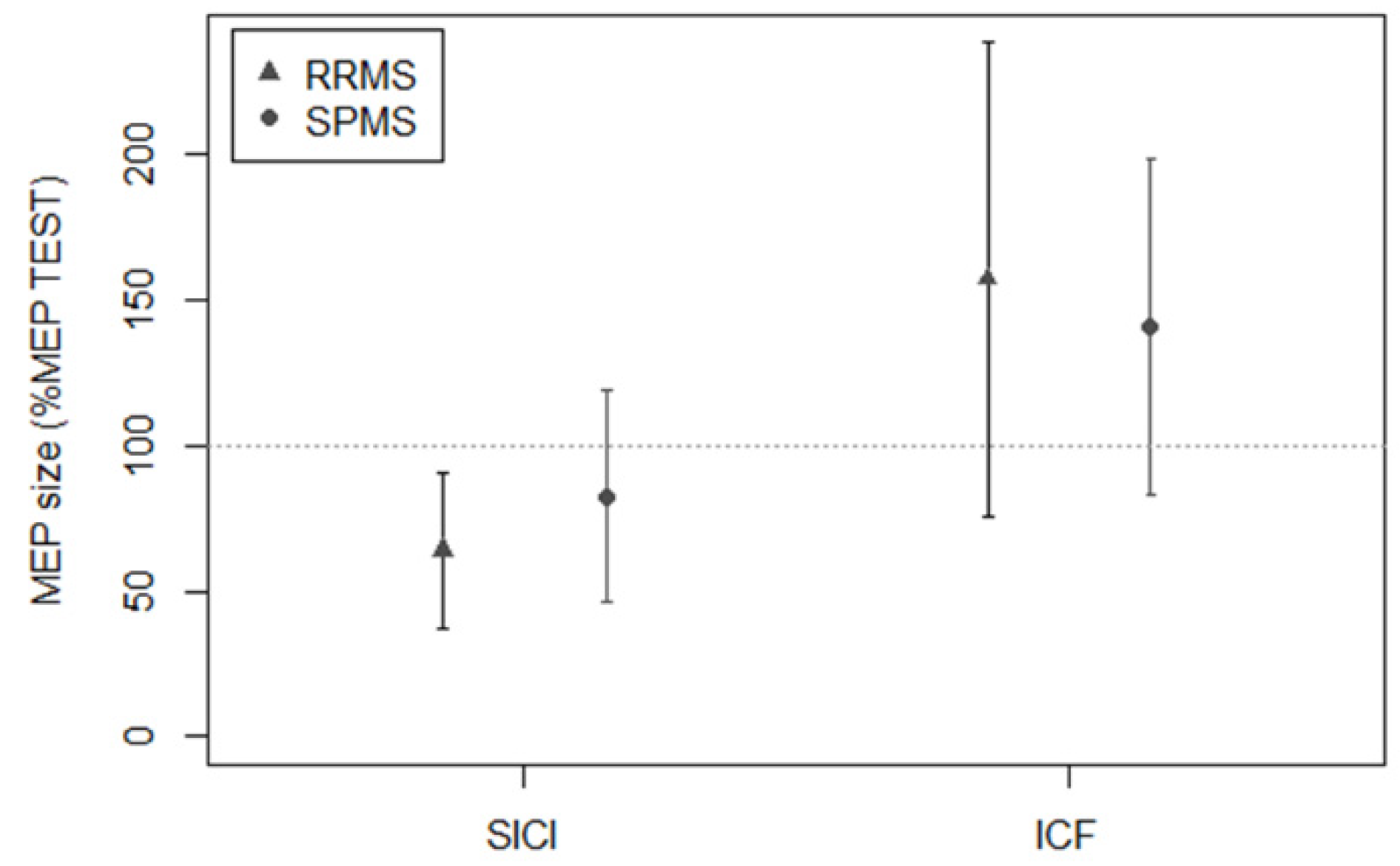
2.2.1. Paired-Pulse TMS to Test M1 Intracortical Interneuron Excitability
2.2.2. STDT to Test S1 Intracortical and Deep Grey Matter Nuclei Interneuron Excitability
2.3. Statistical Analysis
3. Results
3.1. Logistic Regression Model
3.2. Cross-Sectional and Longitudinal Clinical Correlates of SICI and STDT in People with MS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dobson, R.; Giovannoni, G. Multiple Sclerosis—A Review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Kantarci, O.H. Phases and Phenotypes of Multiple Sclerosis. Contin. Lifelong Learn. Neurol. 2019, 25, 636–654. [Google Scholar] [CrossRef]
- Lorscheider, J.; Buzzard, K.; Jokubaitis, V.; Spelman, T.; Havrdova, E.; Horakova, D.; Trojano, M.; Izquierdo, G.; Girard, M.; Duquette, P.; et al. Defining Secondary Progressive Multiple Sclerosis. Brain 2016, 139, 2395–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz Sand, I.; Krieger, S.; Farrell, C.; Miller, A.E. Diagnostic Uncertainty during the Transition to Secondary Progressive Multiple Sclerosis. Mult. Scler. 2014, 20, 1654–1657. [Google Scholar] [CrossRef]
- Filippi, M.; Preziosa, P.; Langdon, D.; Lassmann, H.; Paul, F.; Rovira, À.; Schoonheim, M.M.; Solari, A.; Stankoff, B.; Rocca, M.A. Identifying Progression in Multiple Sclerosis: New Perspectives. Ann. Neurol. 2020, 88, 438–452. [Google Scholar] [CrossRef] [PubMed]
- Rocca, M.A.; Valsasina, P.; Meani, A.; Gobbi, C.; Zecca, C.; Rovira, A.; Sastre-Garriga, J.; Kearney, H.; Ciccarelli, O.; Matthews, L.; et al. Association of Gray Matter Atrophy Patterns with Clinical Phenotype and Progression in Multiple Sclerosis. Neurology 2021, 96, e1561–e1573. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, Z.; Li, Y.; Duan, Y.; Cao, G.; Zheng, F.; Ding, J.; Tian, D.; Wang, X.; Wang, J.; Zhang, X.; et al. Subtyping Relapsing-Remitting Multiple Sclerosis Using Structural MRI. J. Neurol. 2021, 268, 1808–1817. [Google Scholar] [CrossRef]
- O’Connor, P.; Marchetti, P.; Lee, L.; Perera, M. Evoked Potential Abnormality Scores Are a Useful Measure of Disease Burden in Relapsing-Remitting Multiple Sclerosis. Ann. Neurol. 1998, 44, 404–407. [Google Scholar] [CrossRef]
- Ferrazzano, G.; Crisafulli, S.G.; Baione, V.; Tartaglia, M.; Cortese, A.; Frontoni, M.; Altieri, M.; Pauri, F.; Millefiorini, E.; Conte, A. Early Diagnosis of Secondary Progressive Multiple Sclerosis: Focus on Fluid and Neurophysiological Biomarkers. J. Neurol. 2020, 268, 3626–3645. [Google Scholar] [CrossRef]
- Chen, R.; Cros, D.; Curra, A.; Di Lazzaro, V.; Lefaucheur, J.-P.; Magistris, M.R.; Mills, K.; Rösler, K.M.; Triggs, W.J.; Ugawa, Y.; et al. The Clinical Diagnostic Utility of Transcranial Magnetic Stimulation: Report of an IFCN Committee. Clin. Neurophysiol. 2008, 119, 504–532. [Google Scholar] [CrossRef]
- Ziemann, U. Pharmacology of TMS. Suppl. Clin. Neurophysiol. 2003, 56, 226–231. [Google Scholar] [PubMed]
- Conte, A.; Ferrazzano, G.; Belvisi, D.; Manzo, N.; Suppa, A.; Fabbrini, G.; Berardelli, A. Does the Somatosensory Temporal Discrimination Threshold Change over Time in Focal Dystonia? Neural Plast. 2017, 2017, 9848070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artieda, J.; Pastor, M.A.; Lacruz, F.; Obeso, J.A. Temporal Discrimination Is Abnormal in Parkinson’s Disease. Brain 1992, 115 Pt 1, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Matsuhashi, M.; Lin, P.; Ou, B.; Vorbach, S.; Kakigi, R.; Hallett, M. Impaired Intracortical Inhibition in the Primary Somatosensory Cortex in Focal Hand Dystonia. Mov. Disord. 2008, 23, 558–565. [Google Scholar] [CrossRef]
- Rocchi, L.; Conte, A.; Bologna, M.; Li Voti, P.; Millefiorini, E.; Cortese, A.; Pontecorvo, S.; Berardelli, A. Somatosensory Temporal Discrimination Threshold Is Impaired in Patients with Multiple Sclerosis. Clin. Neurophysiol. 2016, 127, 1940–1941. [Google Scholar] [CrossRef]
- Leodori, G.; Formica, A.; Zhu, X.; Conte, A.; Belvisi, D.; Cruccu, G.; Hallett, M.; Berardelli, A. The Third-Stimulus Temporal Discrimination Threshold: Focusing on the Temporal Processing of Sensory Input within Primary Somatosensory Cortex. J. Neurophysiol. 2017, 118, 2311–2317. [Google Scholar] [CrossRef] [Green Version]
- Conte, A.; Giannì, C.; Belvisi, D.; Cortese, A.; Petsas, N.; Tartaglia, M.; Cimino, P.; Millefiorini, E.; Berardelli, A.; Pantano, P. Deep Grey Matter Involvement and Altered Sensory Gating in Multiple Sclerosis. Mult. Scler. 2020, 26, 786–794. [Google Scholar] [CrossRef] [Green Version]
- Giannì, C.; Belvisi, D.; Conte, A.; Tommasin, S.; Cortese, A.; Petsas, N.; Baione, V.; Tartaglia, M.; Millefiorini, E.; Berardelli, A.; et al. Altered Sensorimotor Integration in Multiple Sclerosis: A Combined Neurophysiological and Functional MRI Study. Clin. Neurophysiol. 2021, 132, 2191–2198. [Google Scholar] [CrossRef]
- Berardelli, A.; Abbruzzese, G.; Chen, R.; Orth, M.; Ridding, M.C.; Stinear, C.; Suppa, A.; Trompetto, C.; Thompson, P.D. Consensus Paper on Short-Interval Intracortical Inhibition and Other Transcranial Magnetic Stimulation Intracortical Paradigms in Movement Disorders. Brain Stimul. 2008, 1, 183–191. [Google Scholar] [CrossRef]
- Pastor, M.A.; Day, B.L.; Macaluso, E.; Friston, K.J.; Frackowiak, R.S.J. The Functional Neuroanatomy of Temporal Discrimination. J. Neurosci. 2004, 24, 2585–2591. [Google Scholar] [CrossRef] [Green Version]
- Bradley, D.; Whelan, R.; Walsh, R.; Reilly, R.B.; Hutchinson, S.; Molloy, F.; Hutchinson, M. Temporal Discrimination Threshold: VBM Evidence for an Endophenotype in Adult Onset Primary Torsion Dystonia. Brain 2009, 132, 2327–2335. [Google Scholar] [CrossRef]
- Bradley, D.; Whelan, R.; Kimmich, O.; O’Riordan, S.; Mulrooney, N.; Brady, P.; Walsh, R.; Reilly, R.B.; Hutchinson, S.; Molloy, F.; et al. Temporal Discrimination Thresholds in Adult-Onset Primary Torsion Dystonia: An Analysis by Task Type and by Dystonia Phenotype. J. Neurol. 2012, 259, 77–82. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sorensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F.; et al. Defining the Clinical Course of Multiple Sclerosis: The 2013 Revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Inojosa, H.; Proschmann, U.; Akgün, K.; Ziemssen, T. A Focus on Secondary Progressive Multiple Sclerosis (SPMS): Challenges in Diagnosis and Definition. J. Neurol. 2019, 268, 1210–1221. [Google Scholar] [CrossRef]
- D’Antonio, F.; De Bartolo, M.I.; Ferrazzano, G.; Trebbastoni, A.; Amicarelli, S.; Campanelli, A.; de Lena, C.; Berardelli, A.; Conte, A. Somatosensory Temporal Discrimination Threshold in Patients with Cognitive Disorders. J. Alzheimers Dis. 2019, 70, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Kurtzke, J.F. Rating Neurologic Impairment in Multiple Sclerosis: An Expanded Disability Status Scale (EDSS). Neurology 1983, 33, 1444. [Google Scholar] [CrossRef] [Green Version]
- Conte, A.; Rocchi, L.; Nardella, A.; Dispenza, S.; Scontrini, A.; Khan, N.; Berardelli, A. Theta-Burst Stimulation-Induced Plasticity over Primary Somatosensory Cortex Changes Somatosensory Temporal Discrimination in Healthy Humans. PLoS ONE 2012, 7, e32979. [Google Scholar] [CrossRef]
- Rocchi, L.; Conte, A.; Nardella, A.; Li Voti, P.; Di Biasio, F.; Leodori, G.; Fabbrini, G.; Berardelli, A. Somatosensory Temporal Discrimination Threshold May Help to Differentiate Patients with Multiple System Atrophy from Patients with Parkinson’s Disease. Eur. J. Neurol. 2013, 20, 714–719. [Google Scholar] [CrossRef]
- Conte, A.; Rocchi, L.; Ferrazzano, G.; Leodori, G.; Bologna, M.; Li Voti, P.; Nardella, A.; Berardelli, A. Primary Somatosensory Cortical Plasticity and Tactile Temporal Discrimination in Focal Hand Dystonia. Clin. Neurophysiol. 2014, 125, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Baione, V.; Belvisi, D.; Crisafulli, S.G.; Tartaglia, M.; Leodori, G.; Ferrazzano, G.; Conte, A. Is Somatosensory Temporal Discrimination Threshold a Biomarker of Disease Progression in Multiple Sclerosis? Clin. Neurophysiol. 2020, 131, 2935–2936. [Google Scholar] [CrossRef]
- Scontrini, A.; Conte, A.; Fabbrini, G.; Colosimo, C.; Di Stasio, F.; Ferrazzano, G.; Berardelli, A. Somatosensory Temporal Discrimination Tested in Patients Receiving Botulinum Toxin Injection for Cervical Dystonia. Mov. Disord. 2011, 26, 742–746. [Google Scholar] [CrossRef]
- Ridding, M.C.; Taylor, J.L.; Rothwell, J.C. The Effect of Voluntary Contraction on Cortico-Cortical Inhibition in Human Motor Cortex. J. Physiol. 1995, 487 Pt 2, 541–548. [Google Scholar] [CrossRef]
- Conte, A.; Belvisi, D.; Manzo, N.; Bologna, M.; Barone, F.; Tartaglia, M.; Upadhyay, N.; Berardelli, A. Understanding the Link between Somatosensory Temporal Discrimination and Movement Execution in Healthy Subjects. Physiol. Rep. 2016, 4, e12899. [Google Scholar] [CrossRef]
- Filippi, M.; Rocca, M.A.; Barkhof, F.; Brück, W.; Chen, J.T.; Comi, G.; DeLuca, G.; De Stefano, N.; Erickson, B.J.; Evangelou, N.; et al. Association between Pathological and MRI Findings in Multiple Sclerosis. Lancet Neurol. 2012, 11, 349–360. [Google Scholar] [CrossRef]
- Pagani, E.; Rocca, M.A.; Gallo, A.; Rovaris, M.; Martinelli, V.; Comi, G.; Filippi, M. Regional Brain Atrophy Evolves Differently in Patients with Multiple Sclerosis According to Clinical Phenotype. AJNR Am. J. Neuroradiol. 2005, 26, 341–346. [Google Scholar]
- Magliozzi, R.; Howell, O.W.; Reeves, C.; Roncaroli, F.; Nicholas, R.; Serafini, B.; Aloisi, F.; Reynolds, R. A Gradient of Neuronal Loss and Meningeal Inflammation in Multiple Sclerosis. Ann. Neurol. 2010, 68, 477–493. [Google Scholar] [CrossRef]
- Azevedo, C.J.; Kornak, J.; Chu, P.; Sampat, M.; Okuda, D.T.; Cree, B.A.; Nelson, S.J.; Hauser, S.L.; Pelletier, D. In Vivo Evidence of Glutamate Toxicity in Multiple Sclerosis. Ann. Neurol. 2014, 76, 269–278. [Google Scholar] [CrossRef]
- Moccia, M.; Ciccarelli, O. Molecular and Metabolic Imaging in Multiple Sclerosis. Neuroimaging Clin. N Am. 2017, 27, 343–356. [Google Scholar] [CrossRef] [Green Version]
- MacMillan, E.L.; Tam, R.; Zhao, Y.; Vavasour, I.M.; Li, D.K.B.; Oger, J.; Freedman, M.S.; Kolind, S.H.; Traboulsee, A.L. Progressive Multiple Sclerosis Exhibits Decreasing Glutamate and Glutamine over Two Years. Mult. Scler. 2016, 22, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Opie, G.M.; Semmler, J.G. Age-Related Differences in Short- and Long-Interval Intracortical Inhibition in a Human Hand Muscle. Brain Stimul. 2014, 7, 665–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belvisi, D.; Canevelli, M.; Baione, V.; Buscarinu, M.C.; Pellicciari, G.; Fantozzi, R.; Creta, A.; Cecchi, G.; Cola, G.; Nicoletti, C.G.; et al. Operationalization of a Frailty Index in Patients with Multiple Sclerosis: A Cross-Sectional Investigation. Mult. Scler. 2021, 1352458520987541. [Google Scholar] [CrossRef] [PubMed]
- Iaffaldano, P.; Lucisano, G.; Patti, F.; Brescia Morra, V.; De Luca, G.; Lugaresi, A.; Zaffaroni, M.; Inglese, M.; Salemi, G.; Cocco, E.; et al. Transition to Secondary Progression in Relapsing-Onset Multiple Sclerosis: Definitions and Risk Factors. Mult. Scler. 2021, 27, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Ramos, V.F.M.L.; Esquenazi, A.; Villegas, M.A.F.; Wu, T.; Hallett, M. Temporal Discrimination Threshold with Healthy Aging. Neurobiol. Aging 2016, 43, 174–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audoin, B.; Zaaraoui, W.; Reuter, F.; Rico, A.; Malikova, I.; Confort-Gouny, S.; Cozzone, P.J.; Pelletier, J.; Ranjeva, J.-P. Atrophy Mainly Affects the Limbic System and the Deep Grey Matter at the First Stage of Multiple Sclerosis. J. Neurol. Neurosurg. Psychiatry 2010, 81, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Eshaghi, A.; Prados, F.; Brownlee, W.J.; Altmann, D.R.; Tur, C.; Cardoso, M.J.; De Angelis, F.; van de Pavert, S.H.; Cawley, N.; De Stefano, N.; et al. Deep Gray Matter Volume Loss Drives Disability Worsening in Multiple Sclerosis. Ann. Neurol. 2018, 83, 210–222. [Google Scholar] [CrossRef] [Green Version]
- Eshaghi, A.; Marinescu, R.V.; Young, A.L.; Firth, N.C.; Prados, F.; Jorge Cardoso, M.; Tur, C.; De Angelis, F.; Cawley, N.; Brownlee, W.J.; et al. Progression of Regional Grey Matter Atrophy in Multiple Sclerosis. Brain 2018, 141, 1665–1677. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pwMS | Healthy Controls | p Value | |
|---|---|---|---|
| Age | 45.2 ± 9.2 years | 41.1 ± 6.9 years | 0.521 |
| Sex, n | F: 33 M: 22 | F: 16 M: 15 | 0.461 |
| Age at onset | 32.1 ± 8.7 years | - | |
| Disease duration | 13.1 ± 9.1 years | - | |
| Baseline EDSS score | 2.5 (range: 1.5–4.5) | - | |
| Follow-up EDSS score | 3.0 (range: 1.5–5.0) | - |
| RR | SP | |
|---|---|---|
| EDSS score | 2.0 (range: 1.0–3.0) | 5.0 (range: 4.5–6.0) |
| 9HPT dominant hand (s) | 22 ± 3.2 | 30.4 ± 9.5 |
| 9HPT nondominant hand (s) | 22.1 ± 2.9 | 31 ± 10.2 |
| T25FW (s) | 5.9 ± 1.5 | 9.3 ± 2.5 |
| Brain lesion load (mL) | 9.926 ± 8.555 | 17.816 ± 11.850 |
| pwMS Mean Values | HC Mean Values | p Value | |
|---|---|---|---|
| MEP | 0.95 ± 0.85 | 1.09 ± 0.23 | 0.287 |
| SICI (%) | 71.02 ± 31.65 | 27.33 ± 13.21 | 2.00 × 10−10 |
| ICF (%) | 151.26 ± 73.47 | 184.32 ± 51.55 | 0.051 |
| STDT | 114.83 ± 51.99 | 53.20 ± 20.17 | 4.95 × 10−11 |
| Estimate | p Value | Odds Ratio | 95% Confidence Interval | |
|---|---|---|---|---|
| Intercept | −5.95503 | 1.53 × 10−5 | 0.00259 | −9.09252–3.58799 |
| SICI (%) * age | 0.00056 | 1.84 × 10−4 | 1.00056 | 1.00013–1.00114 |
| STDT * age | 0.00073 | 2.71 × 10−2 | 1.00073 | 1.00040–1.00117 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belvisi, D.; Tartaglia, M.; Borriello, G.; Baione, V.; Crisafulli, S.G.; Zuccoli, V.; Leodori, G.; Ianniello, A.; Pasqua, G.; Pantano, P.; et al. Are Neurophysiological Biomarkers Able to Discriminate Multiple Sclerosis Clinical Subtypes? Biomedicines 2022, 10, 231. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10020231
Belvisi D, Tartaglia M, Borriello G, Baione V, Crisafulli SG, Zuccoli V, Leodori G, Ianniello A, Pasqua G, Pantano P, et al. Are Neurophysiological Biomarkers Able to Discriminate Multiple Sclerosis Clinical Subtypes? Biomedicines. 2022; 10(2):231. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10020231
Chicago/Turabian StyleBelvisi, Daniele, Matteo Tartaglia, Giovanna Borriello, Viola Baione, Sebastiano Giuseppe Crisafulli, Valeria Zuccoli, Giorgio Leodori, Antonio Ianniello, Gabriele Pasqua, Patrizia Pantano, and et al. 2022. "Are Neurophysiological Biomarkers Able to Discriminate Multiple Sclerosis Clinical Subtypes?" Biomedicines 10, no. 2: 231. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10020231