
Distress and Sensitization as Main Mediators of Severity in Women with Fibromyalgia: A Structural Equation Model

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Severity Variables
2.3. Sensitization Variables
2.4. Sensitivity Variable
2.5. Distress Variables
2.6. Statistical Analysis
2.6.1. Packages
2.6.2. Missing Data Management
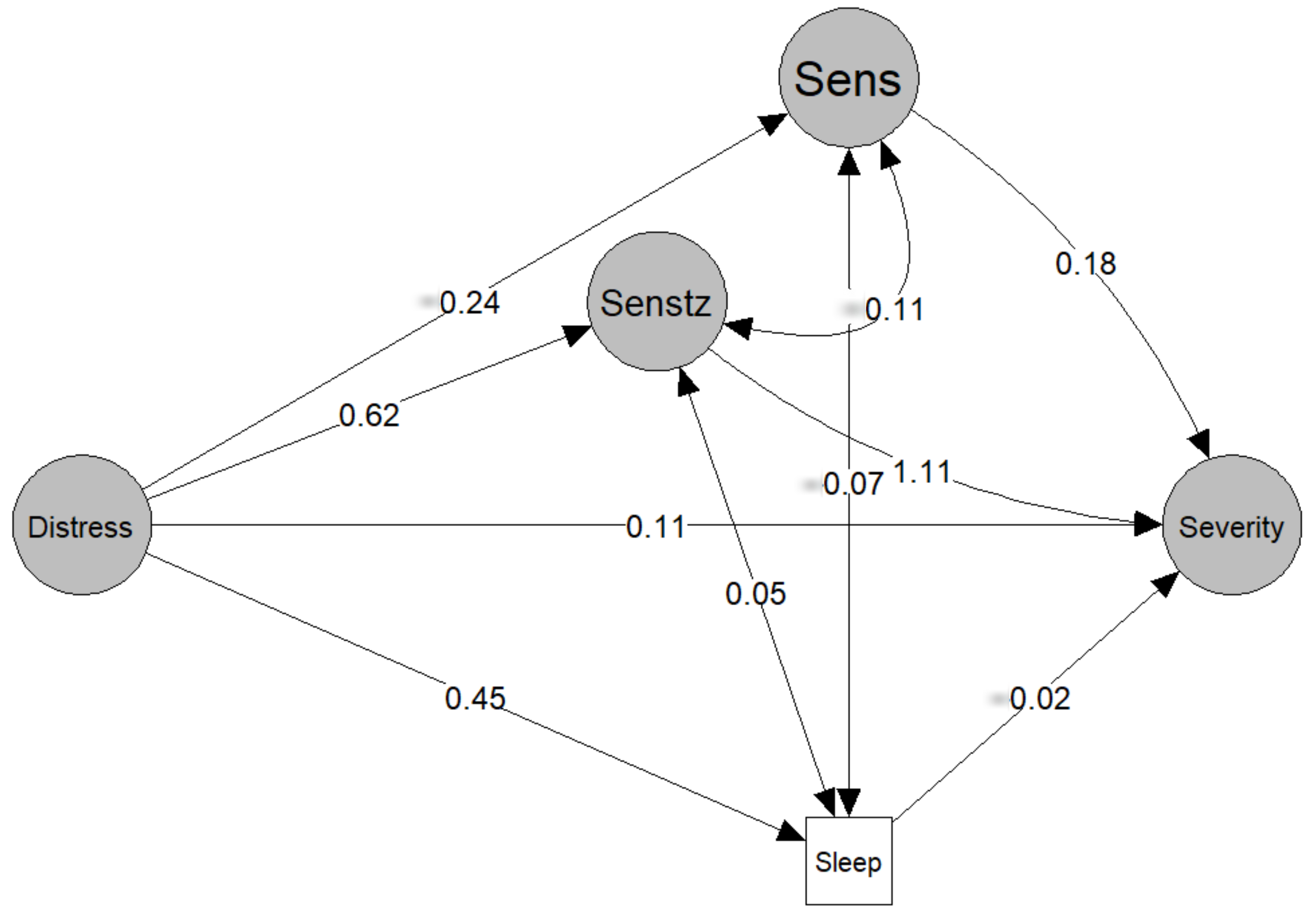
2.6.3. Structural Equation Modelling (SEM)
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marques, A.P.; Santo, A.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. Engl. Ed. 2017, 57, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Creed, F. A review of the incidence and risk factors for fibromyalgia and chronic widespread pain in population-based studies. Pain 2020, 161, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Gostine, M.; Davis, F.; Roberts, B.A.; Risko, R.; Asmus, M.; Cappelleri, J.C.; Sadosky, A. Clinical Characteristics of Fibromyalgia in a Chronic Pain Population. Pain Pract. 2018, 18, 67–78. [Google Scholar] [CrossRef] [PubMed]
- D’Agnelli, S.; Arendt-Nielsen, L.; Gerra, M.C.; Zatorri, K.; Boggiani, L.; Baciarello, M.; Bignami, E. Fibromyalgia: Genetics and epigenetics insights may provide the basis for the development of diagnostic biomarkers. Mol. Pain 2019, 15, 1744806918819944. [Google Scholar] [CrossRef] [PubMed]
- Gerra, M.C.; Carnevali, D.; Ossola, P.; González-Villar, A.; Pedersen, I.S.; Triñanes, Y.; Donnini, C.; Manfredini, M.; Arendt-Nielsen, L.; Carrillo-De-La-Peña, M.T. DNA Methylation Changes in Fibromyalgia Suggest the Role of the Immune-Inflammatory Response and Central Sensitization. J. Clin. Med. 2021, 10, 4992. [Google Scholar] [CrossRef] [PubMed]
- Polli, A.; Ghosh, M.; Bakusic, J.; Ickmans, K.; Monteyne, D.; Velkeniers, B.; Bekaert, B.; Godderis, L.; Nijs, J. DNA Methylation and Brain-Derived Neurotrophic Factor Expression Account for Symptoms and Widespread Hyperalgesia in Patients With Chronic Fatigue Syndrome and Comorbid Fibromyalgia. Arthritis Rheumatol. 2020, 72, 1936–1944. [Google Scholar] [CrossRef] [PubMed]
- Wilson, H.D.; Starz, T.W.; Robinson, J.P.; Turk, D.C. Heterogeneity within the fibromyalgia population: Theoretical implications of variable tender point severity ratings. J. Rheumatol. 2009, 36, 2795–2801. [Google Scholar] [CrossRef]
- Yim, Y.-R.; Lee, K.-E.; Park, D.-J.; Kim, S.-H.; Nah, S.-S.; Lee, J.; Lee, Y.-A.; Hong, S.-J.; Kim, H.-S.; Lee, H.-S.; et al. Identifying fibromyalgia subgroups using cluster analysis: Relationships with clinical variables. Eur. J. Pain 2017, 21, 374–384. [Google Scholar] [CrossRef]
- Martínez, M.P.; Sánchez, A.I.; Prados, G.; Lami, M.J.; Villar, B.; Miró, E. Fibromyalgia as a Heterogeneous Condition: Subgroups of Patients Based on Physical Symptoms and Cognitive-Affective Variables Related to Pain. Span. J. Psychol. 2021, 24, e33. [Google Scholar] [CrossRef]
- Plazier, M.; Ost, J.; Stassijns, G.; De Ridder, D.; Vanneste, S. Pain characteristics in fibromyalgia: Understanding the multiple dimensions of pain. Clin. Rheumatol. 2015, 34, 775–783. [Google Scholar] [CrossRef]
- Kumbhare, D.; Tesio, L. A theoretical framework to improve the construct for chronic pain disorders using fibromyalgia as an example. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720x20966490. [Google Scholar] [CrossRef] [PubMed]
- Droppert, K.M.; Knowles, S.R. The role of pain acceptance, pain catastrophizing, and coping strategies: A Validation of the common sense model in females living with fibromyalgia. J. Clin. Psychol. Med. Settings 2022. [Google Scholar] [CrossRef] [PubMed]
- Segura-Jiménez, V.; Aparicio, V.A.; Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Estévez-López, F.; Delgado-Fernández, M.; Carbonell-Baeza, A. Validation of the modified 2010 American College of Rheumatology diagnostic criteria for fibromyalgia in a Spanish population. Rheumatology 2014, 53, 1803–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Fisher, L.D. Comparative reliability and validity of chronic pain intensity measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef]
- Barbero, M.; Navarro-Santana, M.J.; Palacios-Ceña, M.; Ortega-Santiago, R.; Cescon, C.; Falla, D.; Fernández-De-Las-Peñas, C. Clinical Significance and Diagnostic Value of Pain Extent Extracted from Pain Drawings: A Scoping Review. Diagnostics 2020, 10, 604. [Google Scholar] [CrossRef]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Bennett, M.I.; Smith, B.H.; Torrance, N.; Potter, J. The S-LANSS score for identifying pain of predominantly neuropathic origin: Validation for use in clinical and postal research. J. Pain 2005, 6, 149–158. [Google Scholar] [CrossRef]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef]
- Úbeda-D’Ocasar, E.; Valera-Calero, J.A.; Hervás-Pérez, J.P.; Caballero-Corella, M.; Ojedo-Martín, C.; Gallego-Sendarrubias, G.M. Pain Intensity and Sensory Perception of Tender Points in Female Patients with Fibromyalgia: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 1461. [Google Scholar] [CrossRef]
- Herrmann-Lingen CBUSRP. HADS-D: Hospital Anxiety and Depression Scale: Deutsche Version; Huber: Bern, Switzerland, 2011. [Google Scholar]
- Pilar Martínez, M.; Miró, E.; Sánchez, A.I.; Lami, M.J.; Prados, G.; Ávila, D. Spanish version of the Pain Vigilance and Awareness Questionnaire: Psychometric properties in a sample of women with fibromyalgia. Span. J. Psychol. 2015, 17, E105. [Google Scholar] [CrossRef]
- Woby, S.R.; Roach, N.K.; Urmston, M.; Watson, P.J. Psychometric properties of the TSK-11, a shortened version of the Tampa Scale for Kinesiophobia. Pain 2005, 117, 137–144. [Google Scholar] [CrossRef] [PubMed]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Epskamp, S. semPlot: Path Diagrams and Visual Analysis of Various SEM Packages; 1.1.2 ed. 2019. Available online: https://www.scirp.org/(S(i43dyn45teexjx455qlt3d2q))/reference/referencespapers.aspx?referenceid=3012616 (accessed on 15 November 2021).
- Jorgensen, T.; Pornprasertmanit, S.; Schoemann, A.; Rosseel, Y. semTools: Useful Tools for Structural Equation Modeling; 0.5-5 ed.: R package; 2021. Available online: https://cran.r-project.org/web/packages/semTools/semTools.pdf (accessed on 15 November 2021).
- Gates, K.M.; Molenaar, P.C. Group search algorithm recovers effective connectivity maps for individuals in homogeneous and heterogeneous samples. Neuroimage 2012, 63, 310–319. [Google Scholar] [CrossRef]
- Belda, X.; Fuentes, S.; Daviu, N.; Nadal, R.; Armario, A. Stress-induced sensitization: The hypothalamic-pituitary-adrenal axis and beyond. Stress 2015, 18, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Van Wilgen, C.P.; Vuijk, P.J.; Kregel, J.; Voogt, L.; Meeus, M.; Descheemaeker, F.; Keizer, D.; Nijs, J. Psychological Distress and Widespread Pain Contribute to the Variance of the Central Sensitization Inventory: A Cross-Sectional Study in Patients with Chronic Pain. Pain Pract. 2018, 18, 239–246. [Google Scholar] [CrossRef]
- Angarita-Osorio, N.; Pérez-Aranda, A.; Feliu-Soler, A.; Andrés-Rodríguez, L.; Borràs, X.; Suso-Ribera, C.; Slim, M.; Herrera-Mercadal, P.; Fernández-Vergel, R.; Blanco, M.E.; et al. Patients with Fibromyalgia Reporting Severe Pain but Low Impact of the Syndrome: Clinical and Pain-Related Cognitive Features. Pain Pract. 2020, 20, 255–261. [Google Scholar] [CrossRef]
- İnal, Ö.; Aras, B.; Salar, S. Investigation of the relationship between kinesiophobia and sensory processing in fibromyalgia patients. Somatosens. Mot. Res. 2020, 37, 92–96. [Google Scholar] [CrossRef]
- do Nascimento, B.; Franco, K.; Franco, Y.; Nunes Cabral, C. Can psychological factors be associated with the severity of pain and disability in patients with fibromyalgia? A cross-sectional study. Physiother. Theory Pract. 2022, 3s8, 431–440. [Google Scholar] [CrossRef]
- Williams, A.C.C.; Fisher, E.; Hearn, L.; Eccleston, C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2020, 8, Cd007407. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.H. The role of sleep in pain and fibromyalgia. Nat. Rev. Rheumatol. 2015, 11, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Chang, L.Y.; Lee, H.C.; Fang, S.C.; Tsai, P.S. Sleep disturbances in fibromyalgia: A meta-analysis of case-control studies. J. Psychosom. Res. 2017, 96, 89–97. [Google Scholar] [CrossRef]
- Palagini, L.; Carmassi, C.; Conversano, C.; Gesi, C.; Bazzichi, L.; Giacomelli, C.; Dell’Osso, L. Transdiagnostic factors across fibromyalgia and mental disorders: Sleep disturbances may play a key role. A clinical review. Clin. Exp. Rheumatol. 2016, 34, S140–S144. [Google Scholar] [PubMed]
- Staffe, A.T.; Bech, M.W.; Clemmensen, S.L.K.; Nielsen, H.T.; Larsen, D.B.; Petersen, K.K. Total sleep deprivation increases pain sensitivity, impairs conditioned pain modulation and facilitates temporal summation of pain in healthy participants. PLoS ONE 2019, 14, e0225849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Babiloni, A.H.; Beetz, G.; Tang, N.K.; Heinzer, R.; Nijs, J.; Martel, M.O.; Lavigne, G.J. Towards the endotyping of the sleep-pain interaction: A topical review on multitarget strategies based on phenotypic vulnerabilities and putative pathways. Pain 2021, 162, 1281–1288. [Google Scholar] [CrossRef]
- Nijs, J.; Mairesse, O.; Neu, D.; Leysen, L.; Danneels, L.; Cagnie, B.; Meeus, M.; Moens, M.; Ickmans, K.; Goubert, D. Sleep Disturbances in Chronic Pain: Neurobiology, Assessment, and Treatment in Physical Therapist Practice. Phys. Ther. 2018, 98, 325–335. [Google Scholar] [CrossRef]
- Othman, R.; Jayakaran, P.; Swain, N.; Dassanayake, S.; Tumilty, S.; Mani, R. Relationships Between Psychological, Sleep, and Physical Activity Measures and Somatosensory Function in People With Peripheral Joint Pain: A Systematic Review and Meta-Analysis. Pain Pract. 2021, 21, 226–261. [Google Scholar] [CrossRef]
- Scerbo, T.; Colasurdo, J.; Dunn, S.; Unger, J.; Nijs, J.; Cook, C. Measurement Properties of the Central Sensitization Inventory: A Systematic Review. Pain Pract. 2018, 18, 544–554. [Google Scholar] [CrossRef]
- Nijs, J.; Huysmans, E. Clinimetrics: The Central Sensitisation Inventory: A useful screening tool for clinicians, but not the gold standard. J. Physiother. 2021, S1836-9553(21)00119-3. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, H.; Smart, K.M.; Moloney, N.A.; Doody, C.M. Nervous System Sensitization as a Predictor of Outcome in the Treatment of Peripheral Musculoskeletal Conditions: A Systematic Review. Pain Pract. 2017, 17, 249–266. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-De-Las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Hübscher, M.; Moloney, N.; Leaver, A.; Rebbeck, T.; McAuley, J.H.; Refshauge, K.M. Relationship between quantitative sensory testing and pain or disability in people with spinal pain-a systematic review and meta-analysis. Pain 2013, 154, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.-A.; Rice, A.S.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Belavy, D.L.; Van Oosterwijck, J.; Clarkson, M.; Dhondt, E.; Mundell, N.L.; Miller, C.T.; Owen, P.J. Pain sensitivity is reduced by exercise training: Evidence from a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 120, 100–108. [Google Scholar] [CrossRef]
- Estévez-López, F.; Maestre-Cascales, C.; Russell, D.; Álvarez-Gallardo, I.C.; Rodriguez-Ayllon, M.; Hughes, C.M.; Davison, G.W.; Sañudo, B.; McVeigh, J.G. Effectiveness of Exercise on Fatigue and Sleep Quality in Fibromyalgia: A Systematic Review and Meta-analysis of Randomized Trials. Arch. Phys. Med. Rehabil. 2021, 102, 752–761. [Google Scholar] [CrossRef]
- Ferro Moura Franco, K.; Lenoir, D.; Dos Santos Franco, Y.R.; Jandre Reis, F.J.; Nunes Cabral, C.M.; Meeus, M. Prescription of exercises for the treatment of chronic pain along the continuum of nociplastic pain: A systematic review with meta-analysis. Eur. J. Pain 2021, 25, 51–70. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Kundakci, B.; Kaur, J.; Goh, S.L.; Hall, M.; Doherty, M.; Zhang, W.; Abhishek, A. Efficacy of nonpharmacological interventions for individual features of fibromyalgia: A systematic review and meta-analysis of randomised controlled trials. Pain 2021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Summary Value |
|---|---|
| Age (years) | 52.5(11) |
| Weight (kg) | 71.4 (16.6) |
| Height (m) | 1.60 (0.1) |
| BMI | 27.5 (6.2) |
| Numbers of years diagnosed | 10.2 (8.9) |
| Mean pain (NPRS, 0–10) | 6.4 (1.7) |
| Worst pain (NPRS, 0–10) | 7.3 (2.2) |
| Pain activity (NPRS, 0–10) | 8.1 (1.9) |
| Pain extent ventral (%) | 26.5 (24.7) |
| Pain extent dorsal (%) | 31.3 (26.1) |
| PPT mastoid (kPa) | 151.2 (90.8) |
| PPT trapezius (kPa) | 125.5 (60.4) |
| PPT elbow (kPa) | 149.0 (87.1) |
| PPT hand (kPa) | 120.2 (59.1) |
| PPT posterior iliac (kPa) | 233.9 (130.7) |
| PPT trochanter (kPa) | 257.7 (123.9) |
| PPT knee (kPa) | 148.1 (107.1) |
| PPT tibialis (kPa) | 187.1 (108.7) |
| S-LANSS (0–24) | 17.45 (5.45) |
| PainDETECT (0–38) | 19.9 (7.1) |
| CSI (0–100) | 70.7 (11.55) |
| HADS-A (0–21) | 11.4 (3.7) |
| HADS-D (0–21) | 10.0 (4.1) |
| Pain hypervigilance (PVAQ) | 27.0 (8.2) |
| Catastrophizing (PCS, 0–52) | 22.45 (12.25) |
| Kinesiophobia (Fear, TSK-11, 0–44) | 24.9 (7.5) |
| Sleep quality (PSQI, 0–21) | 13.8 (3.9) |
| DV | IV | Coef | SE | LB | UB | Pval | Sig | Type |
|---|---|---|---|---|---|---|---|---|
| Indirect effect of sensitization | 0.687 | 0.212 | 0.259 | 1.146 | 0.001 | s | Med | |
| Indirect effect of sensitivity | −0.042 | 0.048 | −0.170 | 0.036 | 0.382 | ns | Med | |
| Indirect effect of sleep (PSQI) | −0.008 | 0.036 | −0.095 | 0.069 | 0.826 | ns | Med | |
| Total | 0.745 | 0.196 | 0.296 | 1.115 | 0.000 | s | Med | |
| Sensitivity | Distress | −0.239 | 0.123 | −0.479 | 0.002 | 0.052 | ns | Reg |
| Sensitization | Distress | 0.618 | 0.191 | 0.244 | 0.993 | 0.001 | s | Reg |
| Severity | Sensitization | 1.113 | 0.317 | 0.496 | 1.734 | 0.000 | s | Reg |
| Severity | Sensitivity | 0.176 | 0.170 | −0.157 | 0.512 | 0.300 | ns | Reg |
| Severity | Sleep (PSQI) | −0.017 | 0.078 | −0.170 | 0.136 | 0.825 | ns | Reg |
| Severity | Distress | 0.108 | 0.222 | −0.327 | 0.543 | 0.627 | ns | Reg |
| Sleep | Distress | 0.452 | 0.209 | 0.041 | 0.863 | 0.031 | s | Reg |
| Distress | Anx (HADS-A) | 1.000 | 0.000 | LV | ||||
| Distress | Dep (HADS-D) | 1.114 | 0.235 | 0.654 | 1.575 | 0.000 | s | LV |
| Distress | Hypervigil (PVAQ) | 1.170 | 0.274 | 0.636 | 1.706 | 0.000 | s | LV |
| Distress | Catas (PCS) | 2.069 | 0.421 | 1.248 | 2.898 | 0.000 | s | LV |
| Distress | Fear (TSK-11) | 1.463 | 0.331 | 0.814 | 2.113 | 0.000 | s | LV |
| Sensitivity | PPTmast | 1.000 | 0.000 | LV | ||||
| Sensitivity | PPTtrapz | 1.237 | 0.224 | 0.798 | 1.676 | 0.000 | s | LV |
| Sensitivity | PPTelb | 1.518 | 0.145 | 1.232 | 1.803 | 0.000 | s | LV |
| Sensitivity | PPThand | 1.338 | 0.265 | 0.821 | 1.858 | 0.000 | s | LV |
| Sensitivity | PPTiliac | 1.380 | 0.134 | 1.117 | 1.641 | 0.000 | s | LV |
| Sensitivity | PPTtroc | 1.461 | 0.262 | 0.948 | 1.974 | 0.000 | s | LV |
| Sensitivity | PPTknee | 1.056 | 0.183 | 0.696 | 1.415 | 0.000 | s | LV |
| Sensitivity | PPTtib | 1.592 | 0.231 | 1.140 | 2.043 | 0.000 | s | LV |
| Sensitization | S-LANSS | 1.000 | 0.000 | LV | ||||
| Sensitization | PainDETECT | 1.423 | 0.225 | 0.979 | 1.863 | 0.000 | s | LV |
| Sensitization | CSI | 1.705 | 0.434 | 0.855 | 2.554 | 0.000 | s | LV |
| Severity | P_ext_Dor | 1.000 | 0.000 | LV | ||||
| Severity | P_ext_Vent | 0.723 | 0.212 | 0.308 | 1.139 | 0.001 | s | LV |
| Severity | P_act | 0.925 | 0.618 | -0.284 | 2.143 | 0.134 | ns | LV |
| Severity | Worst_P | 0.423 | 0.338 | -0.240 | 1.087 | 0.211 | ns | LV |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liew, B.X.W.; Valera-Calero, J.A.; Varol, U.; Nijs, J.; Arendt-Nielsen, L.; Plaza-Manzano, G.; Fernández-de-las-Peñas, C. Distress and Sensitization as Main Mediators of Severity in Women with Fibromyalgia: A Structural Equation Model. Biomedicines 2022, 10, 1188. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051188
Liew BXW, Valera-Calero JA, Varol U, Nijs J, Arendt-Nielsen L, Plaza-Manzano G, Fernández-de-las-Peñas C. Distress and Sensitization as Main Mediators of Severity in Women with Fibromyalgia: A Structural Equation Model. Biomedicines. 2022; 10(5):1188. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051188
Chicago/Turabian StyleLiew, Bernard X. W., Juan Antonio Valera-Calero, Umut Varol, Jo Nijs, Lars Arendt-Nielsen, Gustavo Plaza-Manzano, and César Fernández-de-las-Peñas. 2022. "Distress and Sensitization as Main Mediators of Severity in Women with Fibromyalgia: A Structural Equation Model" Biomedicines 10, no. 5: 1188. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051188