
Point-of-Care Wound Blotting with Alcian Blue Grading versus Fluorescence Imaging for Biofilm Detection and Predicting 90-Day Healing Outcomes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Wound Evaluation and Outcome Measurement
2.4. Bacterial Culturing and Identification Methods
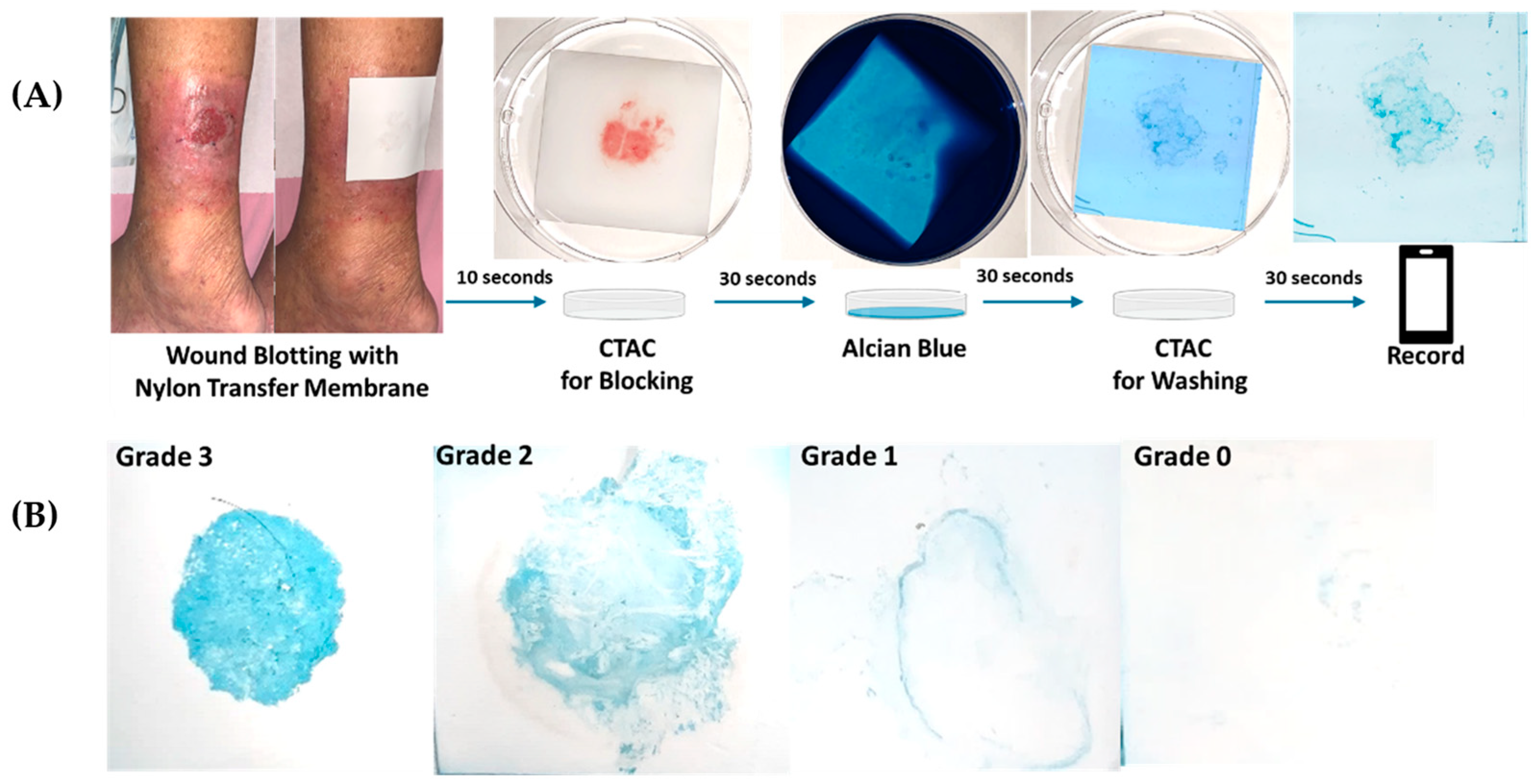
2.5. Modified Wound Blotting with Alcian Blue Grading Protocol
2.6. Bacterial Florescence Imaging with MolecuLight i:X
2.7. Statistical Analysis
3. Results
3.1. Biofilm Detection by Modified Wound Blotting with Alcian Blue Grading versus MolecuLight i:X
3.2. Predicting 90-Day Wound-Healing Outcomes by Modified Wound Blotting with Alcian Blue Grading Versus MolecuLight i:X
3.3. Correlation between Modified Wound Blotting with Alcian Blue Grading and Post-Debridement Wound Decreased Size
3.4. Risk Factor Analysis in 90-Day Wound-Healing Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malone, M.; Bjarnsholt, T.; McBain, A.J.; James, G.A.; Stoodley, P.; Leaper, D.; Tachi, M.; Schultz, G.; Swanson, T.; Wolcott, R.D. The prevalence of biofilms in chronic wounds: A systematic review and meta-analysis of published data. J. Wound Care 2017, 26, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, G.A.; Swogger, E.; Wolcott, R.; Pulcini, E.D.; Secor, P.; Sestrich, J.; Costerton, J.W.; Stewart, P.S. Biofilms in chronic wounds. Wound Repair Regen. 2008, 16, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-K.; Cheng, N.-C.; Cheng, C.-M. Cheng. Biofilms in chronic wounds: Pathogenesis and diagnosis. Trends Biotechnol. 2019, 37, 505–517. [Google Scholar]
- Siddiqui, A.R.; Bernstein, J.M. Chronic wound infection: Facts and controversies. Clin. Dermatol. 2010, 28, 519–526. [Google Scholar] [CrossRef]
- Schultz, G.; Bjarnsholt, T.; James, G.A.; Leaper, D.J.; McBain, A.J.; Malone, M.; Stoodley, P.; Swanson, T.; Tachi, M.; Wolcott, R.D.; et al. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017, 25, 744–757. [Google Scholar] [CrossRef] [PubMed]
- Høiby, N.; Bjarnsholt, T.; Moser, C.; Bassi, G.L.; Coenye, T.; Donelli, G.; Hall-Stoodley, L.; Holá, V.; Imbert, C.; Kirketerp-Møller, K.; et al. ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 2015, 21, S1–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angel, D.E.; Lloyd, P.; Carville, K.; Santamaria, N. The clinical efficacy of two semi-quantitative wound-swabbing techniques in identifying the causative organism (s) in infected cutaneous wounds. Int. Wound J. 2011, 8, 176–185. [Google Scholar] [CrossRef]
- Stallard, Y. When and how to perform cultures on chronic wounds? J. Wound Ostomy Cont. Nurs. 2018, 45, 179–186. [Google Scholar] [CrossRef]
- Ramamurthy, T.; Ghosh, A.; Pazhani, G.P.; Shinoda, S. Current perspectives on viable but non-culturable (VBNC) pathogenic bacteria. Front. Public Health 2014, 2, 103. [Google Scholar] [CrossRef]
- Cole, W.; Coe, S. Use of a bacterial fluorescence imaging system to target wound debridement and accelerate healing: A pilot study. J. Wound Care 2020, 29 (Suppl. 7), S44–S52. [Google Scholar] [CrossRef]
- Lopez, A.J.; Jones, L.M.; Reynolds, L.; Diaz, R.C.; George, I.K.; Little, W.; Fleming, D.; D’Souza, A.; Rennie, M.Y.; Rumbaugh, K.P.; et al. Detection of bacterial fluorescence from in vivo wound biofilms using a point-of-care fluorescence imaging device. Int. Wound J. 2021, 18, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Schultz, G.S.; Phillips, P.L.; Sampson, E.M. Materials and Methods for Assessing and Mapping Microbes and Microbial Biofilms on Wounds. U.S. Patent 9145574B2, 29 September 2015. [Google Scholar]
- Nakagami, G.; Schultz, G.; Gibson, D.; Phillips, P.; Kitamura, A.; Minematsu, T.; Miyagaki, T.; Hayashi, A.; Sasaki, S.; Sugama, J.; et al. Biofilm detection by wound blotting can predict slough development in pressure ulcers: A prospective observational study. Wound Repair Regen. 2017, 25, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Nakagami, G.; Kitamura, A.; Minematsu, T.; Kinoshita, M.; Suga, H.; Kurita, M.; Hayashi, C.; Kawasaki, A.; Sanada, H. Effectiveness of biofilm-based wound care system on wound healing in chronic wounds. Wound Repair Regen. 2019, 27, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Nakagami, G.; Schultz, G.; Kitamura, A.; Minematsu, T.; Akamata, K.; Suga, H.; Kurita, M.; Hayashi, C.; Sanada, H. Rapid detection of biofilm by wound blotting following sharp debridement of chronic pressure ulcers predicts wound healing: A preliminary study. Int. Wound J. 2019, 17, 191–196. [Google Scholar] [CrossRef]
- Wu, Y.; Ms, T.L.; Bs, W.L.; Chuan, H.; Cheng, N.; Cheng, C. Rapid detection of biofilm with modified alcian blue staining: In-vitro protocol improvement and validation with clinical cases. Wound Repair Regen. 2020, 28, 834–843. [Google Scholar] [CrossRef]
- Giuliano, C.; Patel, C.R.; Kale-Pradhan, P.B. A guide to bacterial culture identification and results interpretation. Pharm. Ther. 2019, 44, 192. [Google Scholar]
- Martinengo, L.; Olsson, M.; Bajpai, R.; Soljak, M.; Upton, Z.; Schmidtchen, A.; Car, J.; Järbrink, K. Prevalence of chronic wounds in the general population: Systematic review and meta-analysis of observational studies. Ann. Epidemiol. 2019, 29, 8–15. [Google Scholar] [CrossRef]
- Goh, O.Q.; Ganesan, G.; Graves, N.; Ng, Y.Z.; Harding, K.; Tan, K.B. Incidence of chronic wounds in Singapore, a multiethnic Asian country, between 2000 and 2017: A retrospective cohort study using a nationwide claims database. BMJ Open 2020, 10, e039411. [Google Scholar] [CrossRef]
- Rennie, M.; Lindvere-Teene, L.; Tapang, K.; Linden, R. Point-of-care fluorescence imaging predicts the presence of pathogenic bacteria in wounds: A clinical study. J. Wound Care 2017, 26, 452–460. [Google Scholar] [CrossRef]
- Price, N. Routine fluorescence imaging to detect wound bacteria reduces antibiotic use and antimicrobial dressing expenditure while improving healing rates: Retrospective analysis of 229 foot ulcers. Diagnostics 2020, 10, 927. [Google Scholar] [CrossRef]
- Pijpe, A.; Ozdemir, Y.; Sinnige, J.C.; Kwa, K.A.; Middelkoop, E.; Vries, A.M.-D. Detection of bacteria in burn wounds with a novel handheld autofluorescence wound imaging device: A pilot study. J. Wound Care 2019, 28, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Raizman, R.; Little, W.; Smith, A. Rapid diagnosis of Pseudomonas aeruginosa in wounds with point-of-care fluorescence imaging. Diagnostics 2021, 11, 280. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.M.; Dunham, D.; Rennie, M.Y.; Kirman, J.; Lopez, A.J.; Keim, K.C.; Little, W.; Gomez, A.; Bourke, J.; Ng, H.; et al. In vitro detection of porphyrin-producing wound bacteria with real-time fluorescence imaging. Future Microbiol. 2020, 15, 319–332. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, P.; Jones, P.; Caselli, A.; Giurini, J.M.; Veves, A. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care 2003, 26, 1879–1882. [Google Scholar] [CrossRef] [Green Version]
- Frykberg, R.G.; Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 2015, 4, 635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snyder, R.J.; Cardinal, M.; Dauphinée, D.M.; Stavosky, J. A post-hoc analysis of reduction in diabetic foot ulcer size at 4 weeks as a predictor of healing by 12 weeks. Ostomy Wound Manag. 2010, 56, 44. [Google Scholar]
- Cardinal, M.; Eisenbud, D.E.; Phillips, T.; Harding, K. Early healing rates and wound area measurements are reliable predictors of later complete wound closure. Wound Repair Regen. 2008, 16, 19–22. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Age (years) | 65.1 (18.4) |
| Gender (Male:Female) | 24:29 |
| Diabetes | 19 (35.9) |
| Etiology of wound | |
| Diabetic | 19 (35.9) |
| Arterial insufficiency | 11 (20.8) |
| Venous ulcer | 4 (7.5) |
| Pressure injury | 5 (9.4) |
| Trauma | 19 (35.9) |
| Other | 2 (3.8) |
| Location of wound | |
| Forefoot | 17 (32.1) |
| Midfoot | 3 (5.7) |
| Hindfoot | 7 (13.2) |
| Leg | 19 (35.9) |
| Hip | 4 (7.5) |
| Perineum | 1 (1.9) |
| Hand | 2 (3.8) |
| Wound Size | |
| Initial wound size (cm2) | 9.51 (14.40) |
| 2-Week Wound Size (cm2) | 5.13 (7.91) |
| 4-Week Wound Size (cm2) | 3.46 (7.06) |
| 2-Week Decreased Size (%) | 33.96 (31.31) |
| 4-Week Decreased Size (%) | 63.00 (44.72) |
| Wound Culture (+) | 40 (75.5) |
| Mono-microbial | 15 (37.5) |
| Poly-microbial | 25 (62.5) |
| 2 species | 12 (30.0) |
| ≥3 species | 13 (32.5) |
| Grade of Wound Blotting | |
| Grade 0 | 9 (17.0) |
| Grade 1 | 7 (13.2) |
| Grade 2 | 16 (30.2) |
| Grade 3 | 21 (39.6) |
| MolecuLight i:X (+) | 19 (35.8) |
| Wound-Healing Time | |
| <30 Days | 8 (15.1) |
| 30–90 Days | 25 (47.2) |
| >90 Days | 20 (37.7) |
| Alcian Blue Grading | Wound Culture (+) | Wound Culture (−) | Case No. |
|---|---|---|---|
| Grade 3 | 20 (95.2) | 1 (4.8) | 21 |
| Grade 2 | 15 (93.8) | 1 (6.3) | 16 |
| Grade 1 | 5 (71.4) | 2 (28.6) | 7 |
| Grade 0 | 0 (0) | 9 (100) | 9 |
| Wound Culture (+) | Wound Culture (−) | Case No. | |
| MolecuLight i:X (+) | 18 (94.7) | 1 (5.3) | 19 |
| MolecuLight i:X (−) | 22 (64.7) | 12 (35.3) | 34 |
| MolecuLight i:X in Biofilm Detection | |||
| Sensitivity | 45% | ||
| Specificity | 92.3% | ||
| Positive Predictive Value | 94.7% | ||
| Negative Predictive Value | 35.3% | ||
| Alcian Blue Grading | <30 Days Healing | 30–90 Days Healing | >90 Days Healing | Case No. |
| Grade 3 | 0 (0) | 9 (42.9) | 12 (57.1) | 21 |
| Grade 2 | 0 (0) | 8 (50.0) | 8 (50.0) | 16 |
| Grade 1 | 1 (14.3) | 6 (85.7) | 0 (0) | 7 |
| Grade 0 | 7 (77.8) | 2 (22.2) | 0 (0) | 9 |
| <30 Days Healing | 30–90 Days Healing | >90 Days Healing | Case No. | |
| Wound Culture (+) | 1 (2.5) | 20 (50.0) | 19 (47.5) | 40 |
| Wound Culture (−) | 7 (53.8) | 5 (38.5) | 1 (7.7) | 13 |
| <30 Days Healing | 30–90 Days Healing | >90 Days Healing | Case No. | |
| MolecuLight i:X (+) | 0 (0) | 11 (57.9) | 8 (42.1) | 19 |
| MolecuLight i:X (−) | 8 (23.5) | 14 (41.2) | 12 (35.3) | 34 |
| Alcian Blue Grading | Post-Debridement 2-Week Decreased Size (%) | Post-Debridement 4-Week Decreased Size (%) | Case No. |
| Grade 3 | 34.0 | 48.1 | 21 |
| Grade 2 | 36.6 | 53.0 | 16 |
| Grade 1 | 55.3 | 86.9 | 7 |
| Grade 0 | 79.4 | 94.5 | 9 |
| Alcian Blue Grading | Post-Debridement 2-Week Decreased Size (%) | Post-Debridement 4-Week Decreased Size (%) | |
| Grade 3 vs. Grade 0 | p = 0.013 | p = 0.002 | |
| Grade 2 vs. Grade 0 | p = 0.018 | p = 0.001 |
| Variables | 90-Day Healed | 90-Day Unhealed | p-Value |
|---|---|---|---|
| Age (year) | 61.9 (19.4) | 70.5 (15.6) | 0.102 |
| Gender (Male:Female) | 15:18 | 10:10 | |
| Diabetes (%) | 27.3 | 50.0 | <0.001 |
| Wound Size | |||
| Initial Wound Size (cm2) | 9.56 (16.11) | 9.41 (11.73) | 0.970 |
| 2-Week Decreased Size (cm2) | 5.96 (2.39) | 1.62 (1.50) | <0.001 |
| 2-Week Decreased Size (%) | 63.14 (25.41) | 18.41 (17.05) | <0.001 |
| 4-Week Decreased Size (cm2) | 8.05 (1.54) | 2.56 (5.61) | <0.001 |
| 4-Week Decreased Size (%) | 86.14 (16.43) | 22.81 (50.01) | <0.001 |
| Wound Culture (+) | 21 (63.6%) | 19 (95%) | <0.001 |
| Alcian Blue Grading (+) | 24 (72.7%) | 20 (100%) | <0.001 |
| Grade 0 | 9 | 0 | |
| Grade 1 | 7 | 0 | |
| Grade 2 | 8 | 8 | |
| Grade 3 | 9 | 12 | |
| MolecuLight i:X (+) | 11 (33.3%) | 8 (40%) | <0.001 |
| Healing Duration (day) | 45.1 (23.1) | >90 | |
| Total No. | 33 | 20 | |
| 90-Day Healed | 90-Day Unhealed | Case No. | |
| 4-Week Decreased Size > 50% | 32 (88.9%) | 4 (11.1%) | 36 |
| 4-Week Decreased Size < 50% | 1 (5.9%) | 16 (94.1%) | 17 |
| “4-Week Decreased Size > 50%” in predicting 90-Day Healing | |||
| Sensitivity | 96.96% | ||
| Specificity | 80.0% | ||
| Positive Predictive Value | 88.9% | ||
| Negative Predictive Value | 94.1% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.-F.; Lin, Y.-C.; Yang, H.-W.; Cheng, N.-C.; Cheng, C.-M. Point-of-Care Wound Blotting with Alcian Blue Grading versus Fluorescence Imaging for Biofilm Detection and Predicting 90-Day Healing Outcomes. Biomedicines 2022, 10, 1200. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051200
Wu Y-F, Lin Y-C, Yang H-W, Cheng N-C, Cheng C-M. Point-of-Care Wound Blotting with Alcian Blue Grading versus Fluorescence Imaging for Biofilm Detection and Predicting 90-Day Healing Outcomes. Biomedicines. 2022; 10(5):1200. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051200
Chicago/Turabian StyleWu, Yu-Feng, Yu-Chen Lin, Hung-Wei Yang, Nai-Chen Cheng, and Chao-Min Cheng. 2022. "Point-of-Care Wound Blotting with Alcian Blue Grading versus Fluorescence Imaging for Biofilm Detection and Predicting 90-Day Healing Outcomes" Biomedicines 10, no. 5: 1200. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051200