
The Mediating Effect of Cytokines on the Association between Fungal Sensitization and Poor Clinical Outcome in Asthma

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Collection of Clinical Information
2.3. Pulmonary Function Assessment
2.4. Detection of Allergen Sensitization
2.5. Serum Levels of Cytokines
2.6. Statistical Analysis
3. Results
3.1. Clinical Features of Patients with Asthma
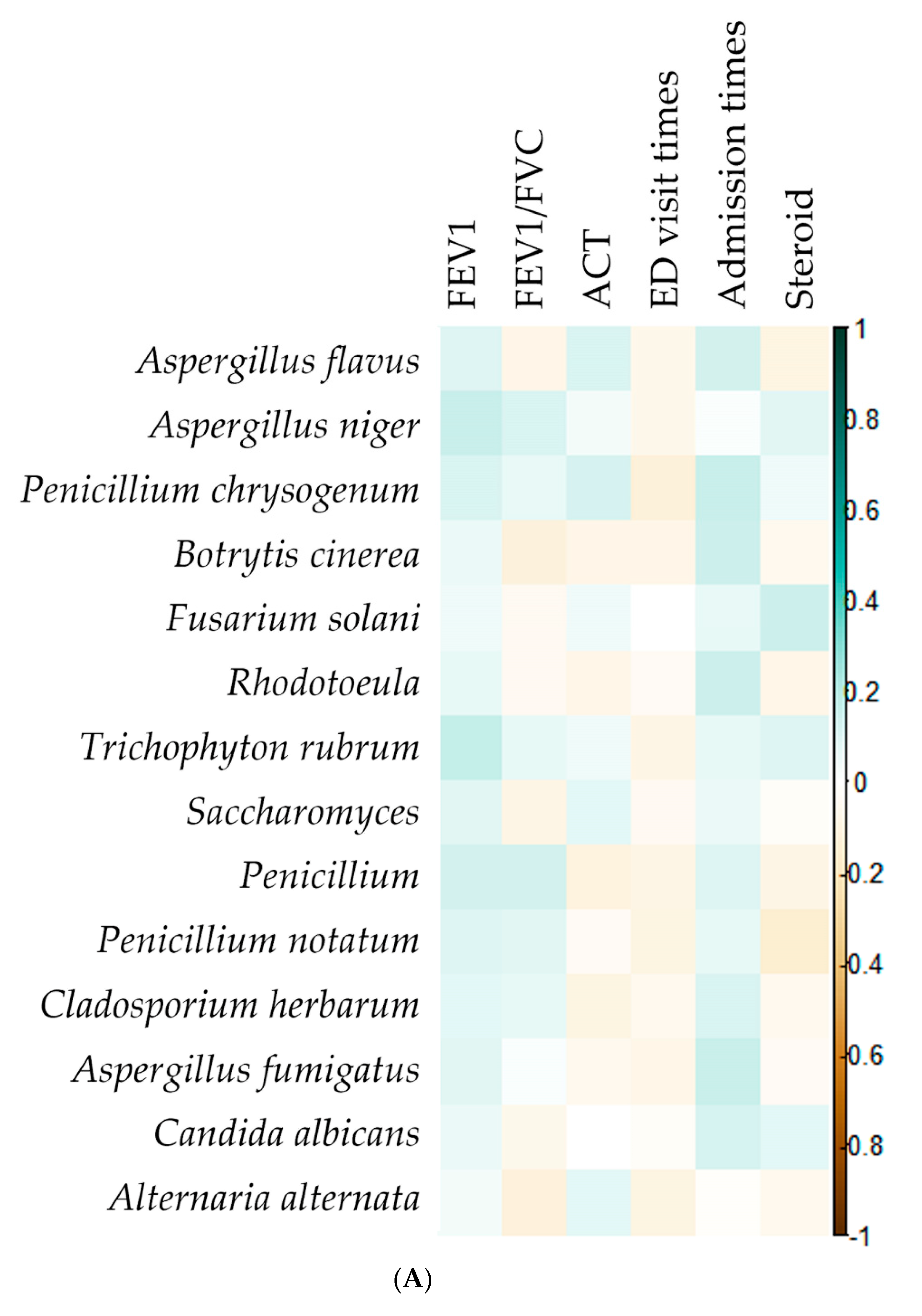
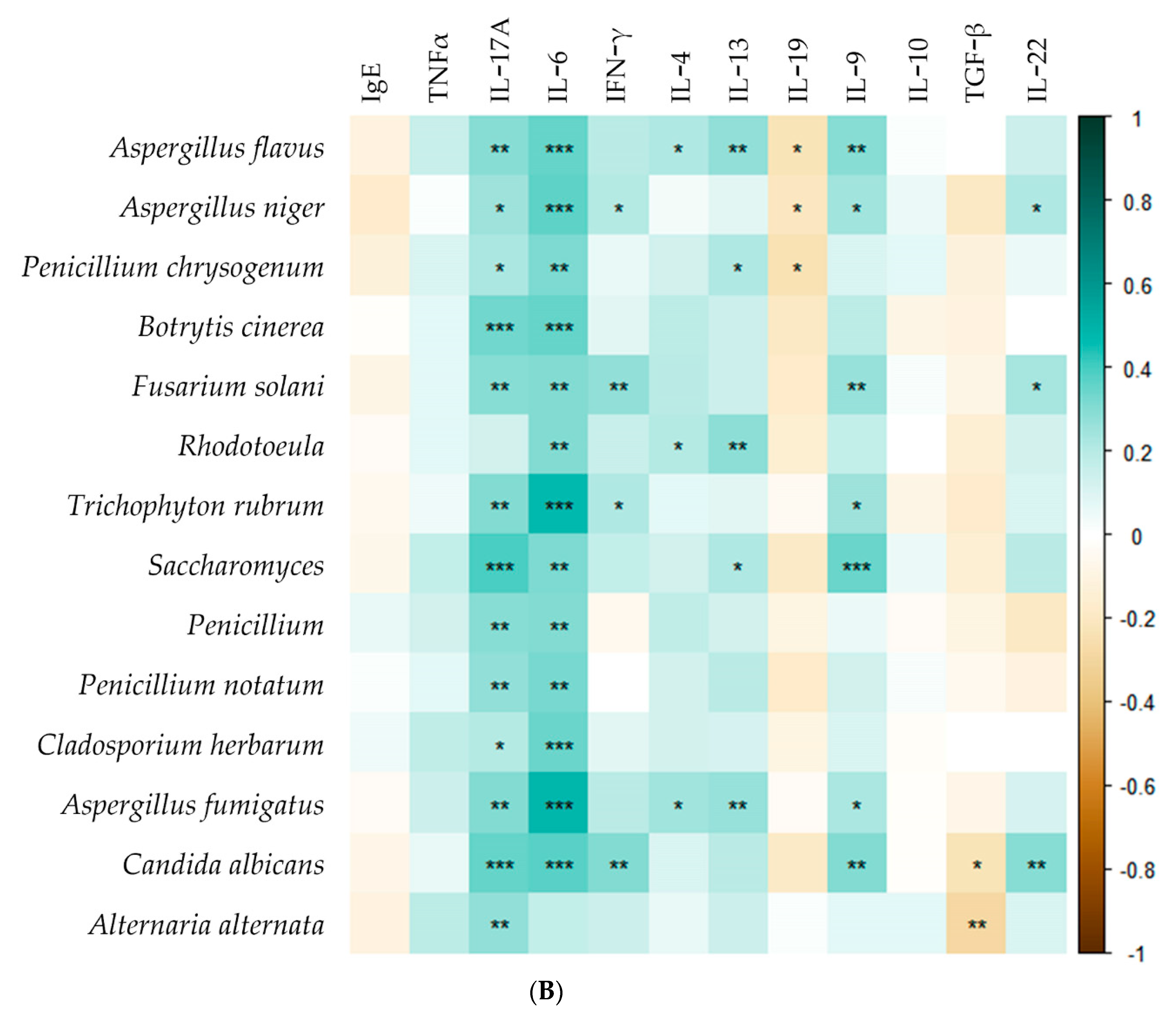
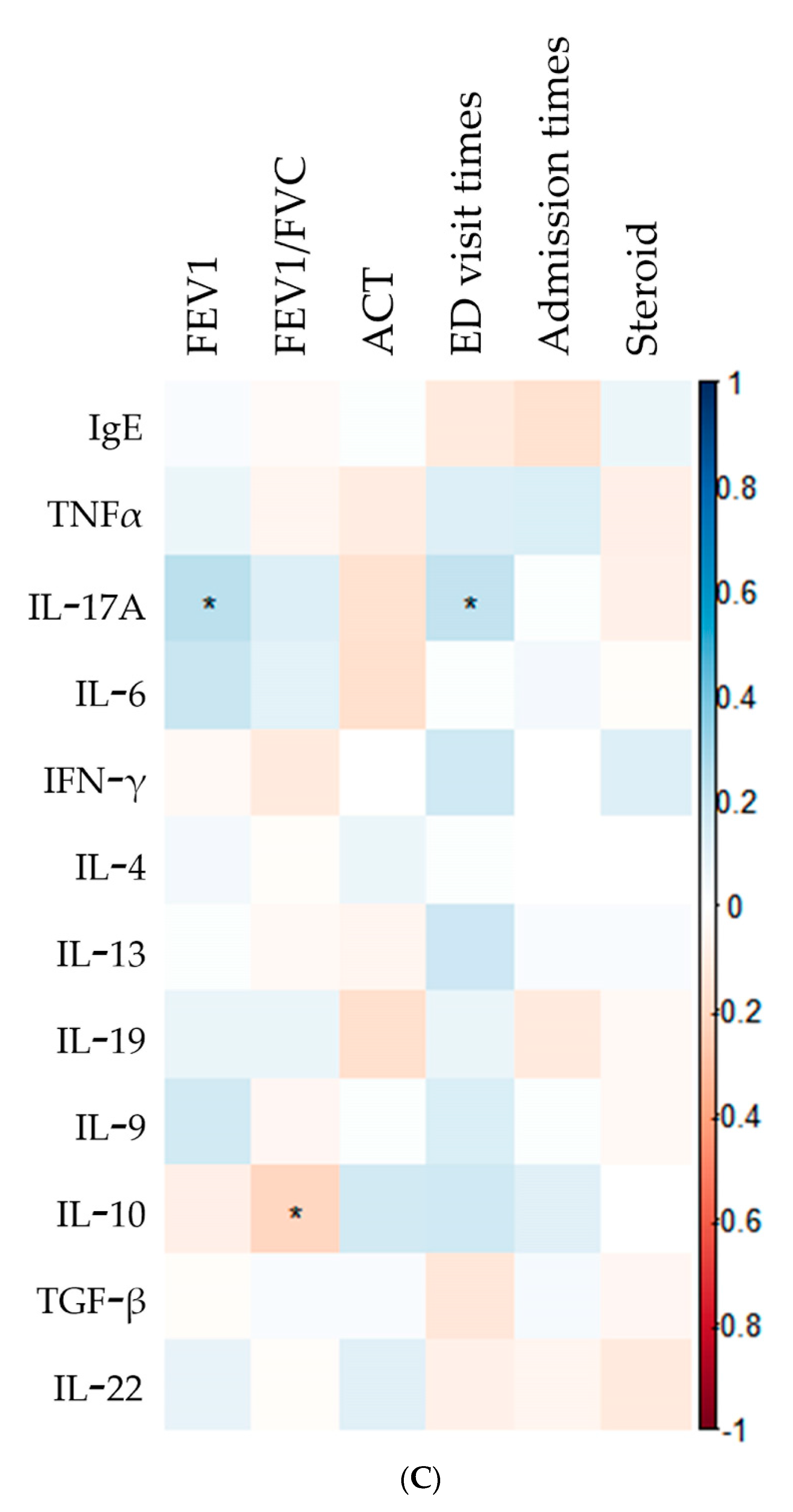
3.2. Correlation among Fungi, Clinical Outcome of Asthmatic Patients, and Cytokines
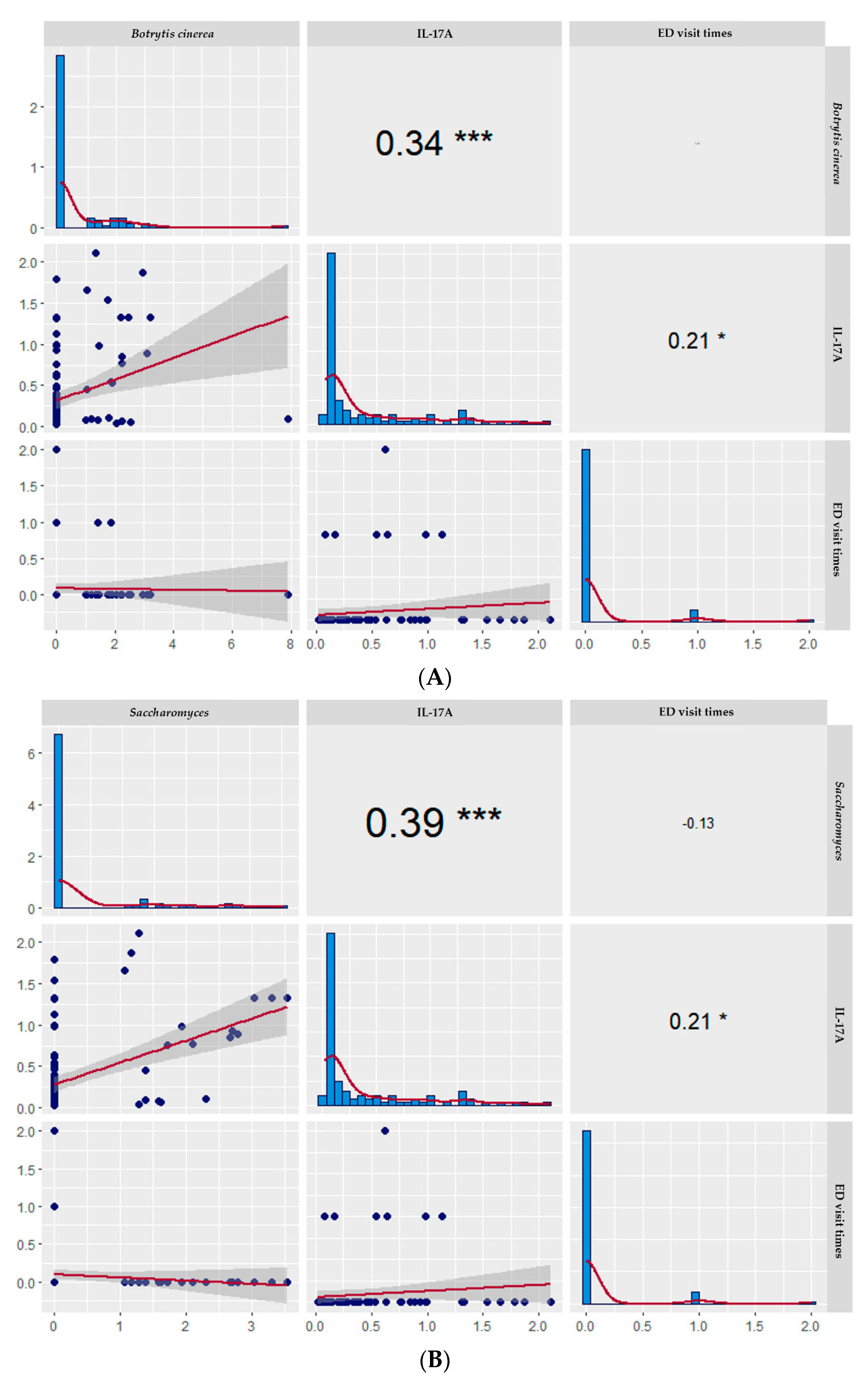
3.3. Correlation among Botrytis cinerea, Saccharomyces, and Candida albicans and ED Times and IL-17A
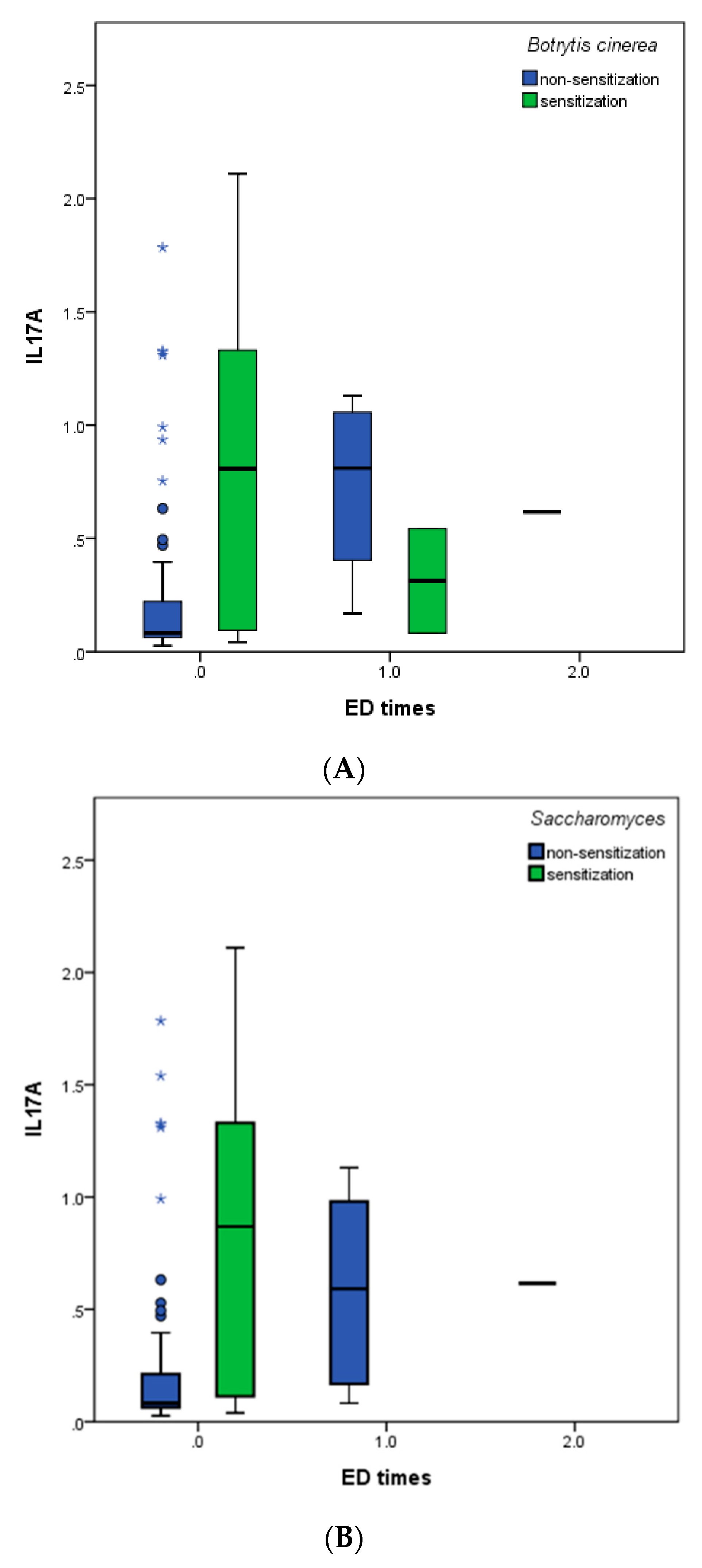
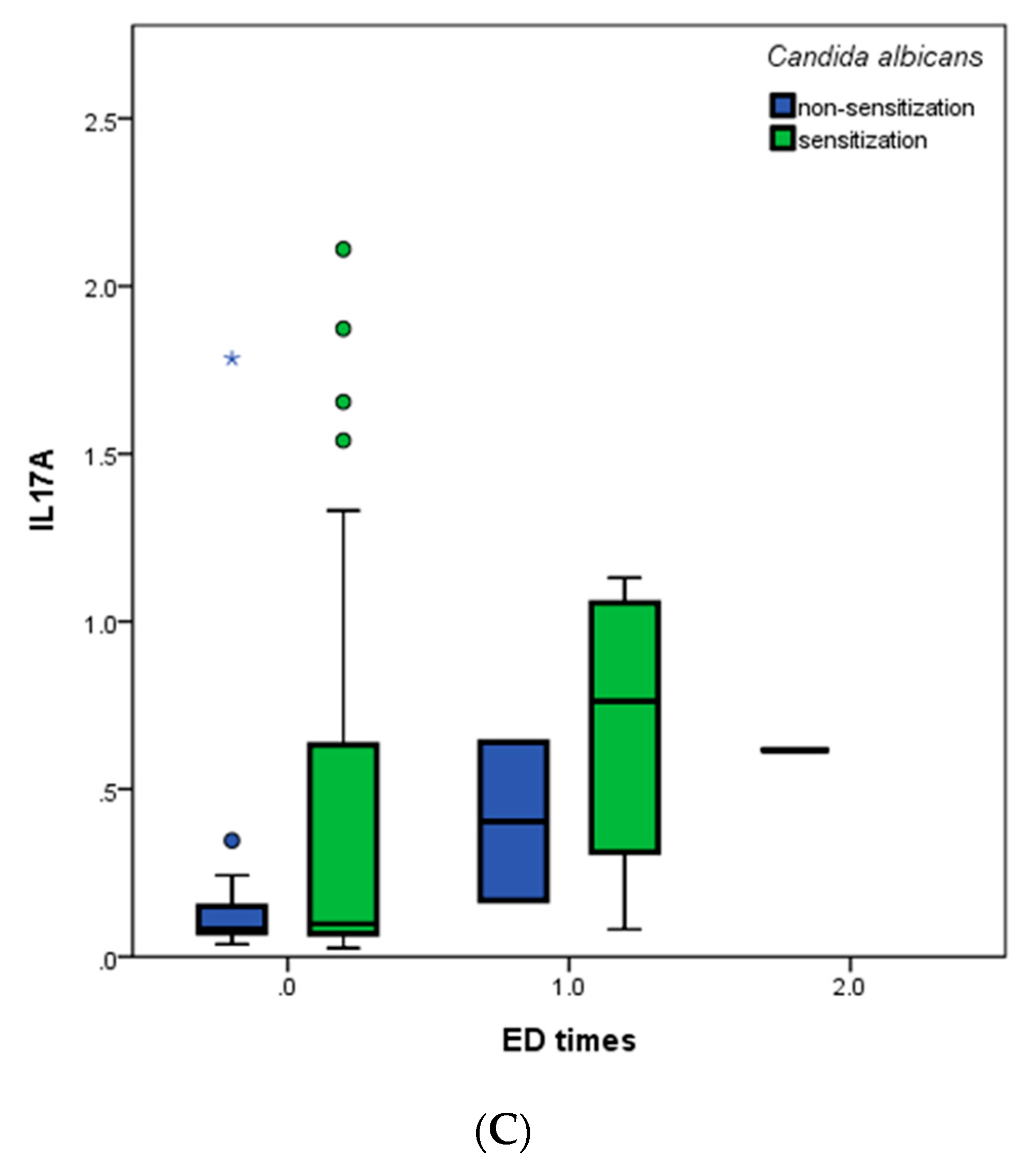
3.4. IL-17A Levels in Asthmatic Patients with and without Fungal Sensitization Grouped by ED Visit Times
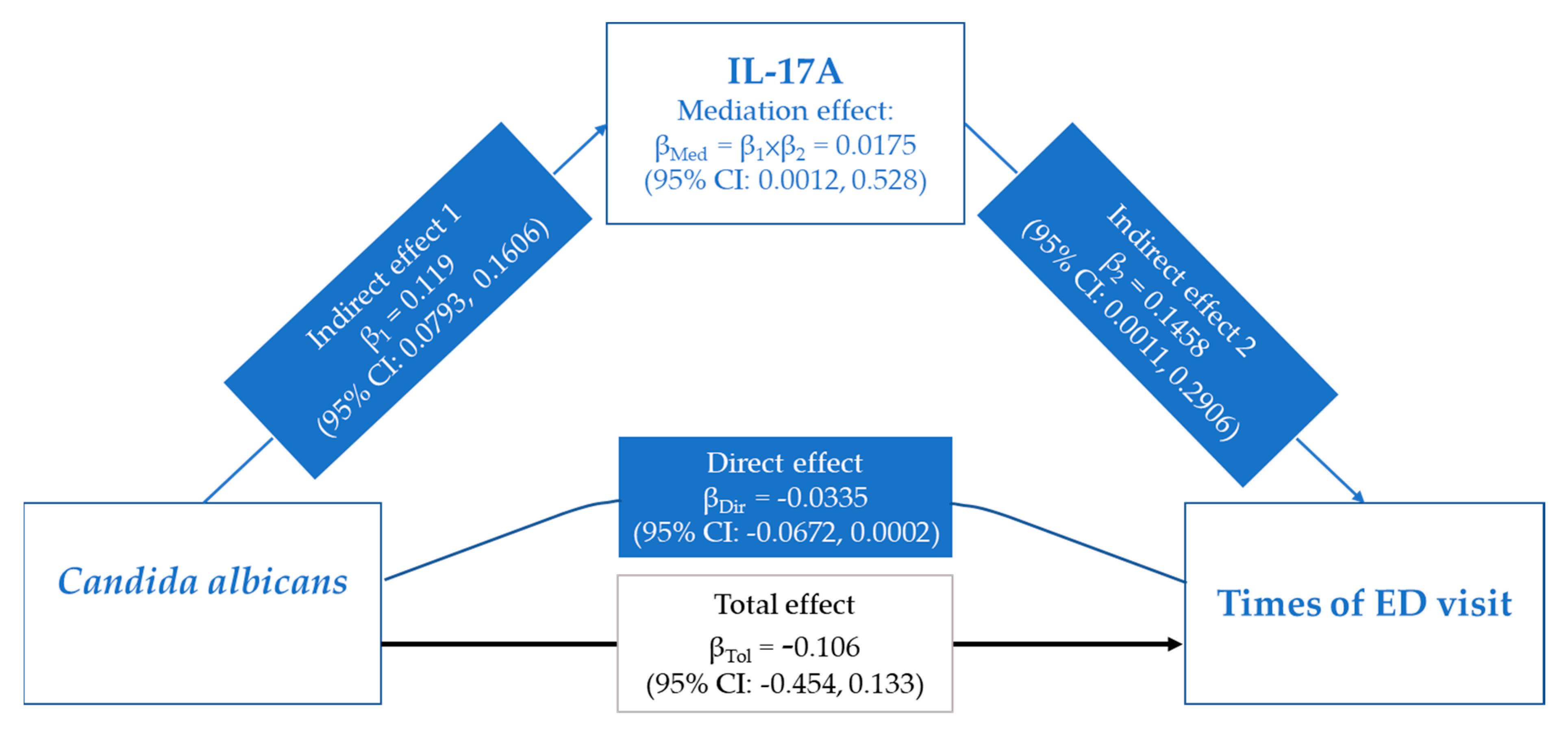
3.5. Role of IL-17A in the Associations between Candida albicans and ED Visit Times
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holgate, S.T.; Wenzel, S.; Postma, D.S.; Weiss, S.T.; Renz, H.; Sly, P.D. Asthma. Nat. Rev. Dis. Primers 2015, 1, 15025. [Google Scholar] [CrossRef]
- Levy, B.D.; Noel, P.J.; Freemer, M.M.; Cloutier, M.M.; Georas, S.N.; Jarjour, N.N.; Ober, C.; Woodruff, P.G.; Barnes, K.C.; Bender, B.G.; et al. Future Research Directions in Asthma. An NHLBI Working Group Report. Am. J. Respir. Crit. Care Med. 2015, 192, 1366–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denning, D.W.; O’Driscoll, B.R.; Hogaboam, C.M.; Bowyer, P.; Niven, R.M. The link between fungi and severe asthma: A summary of the evidence. Eur. Respir. J. 2006, 27, 615–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, C.C.; Hanania, N.A.; Parulekar, A.D. The impact of fungal allergic sensitization on asthma. Curr. Opin. Pulm. Med. 2021, 27, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Fujiwara, A.; Uchida, Y.; Yamaguchi, M.; Ohta, S.; Homma, T.; Watanabe, Y.; Yamamoto, M.; Suzuki, S.; Yokoe, T. Evaluation of the association between sensitization to common inhalant fungi and poor asthma control. Ann. Allergy Asthma Immunol. 2016, 117, 163–168.e161. [Google Scholar] [CrossRef] [PubMed]
- Fairs, A.; Agbetile, J.; Hargadon, B.; Bourne, M.; Monteiro, W.R.; Brightling, C.E.; Bradding, P.; Green, R.H.; Mutalithas, K.; Desai, D.; et al. IgE sensitization to Aspergillus fumigatus is associated with reduced lung function in asthma. Am. J. Respir. Crit. Care Med. 2010, 182, 1362–1368. [Google Scholar] [CrossRef] [Green Version]
- O’Driscoll, B.R.; Hopkinson, L.C.; Denning, D.W. Mold sensitization is common amongst patients with severe asthma requiring multiple hospital admissions. BMC Pulm. Med. 2005, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- O’Hollaren, M.T.; Yunginger, J.W.; Offord, K.P.; Somers, M.J.; O’Connell, E.J.; Ballard, D.J.; Sachs, M.I. Exposure to an aeroallergen as a possible precipitating factor in respiratory arrest in young patients with asthma. N. Engl. J. Med. 1991, 324, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Sehgal, I.S.; Dhooria, S.; Aggarwal, A.N. Challenging cases in fungal asthma. Med. Mycol. 2019, 57 (Suppl. 2), S110–S117. [Google Scholar] [CrossRef]
- Godwin, M.S.; Reeder, K.M.; Garth, J.M.; Blackburn, J.P.; Jones, M.; Yu, Z.; Matalon, S.; Hastie, A.T.; Meyers, D.A.; Steele, C. IL-1RA regulates immunopathogenesis during fungal-associated allergic airway inflammation. JCI Insight 2019, 4, e129055. [Google Scholar] [CrossRef]
- Griffiths, J.S.; Camilli, G.; Kotowicz, N.K.; Ho, J.; Richardson, J.P.; Naglik, J.R. Role for IL-1 Family Cytokines in Fungal Infections. Front. Microbiol. 2021, 12, 633047. [Google Scholar] [CrossRef] [PubMed]
- Guerra, E.S.; Lee, C.K.; Specht, C.A.; Yadav, B.; Huang, H.; Akalin, A.; Huh, J.R.; Mueller, C.; Levitz, S.M. Central Role of IL-23 and IL-17 Producing Eosinophils as Immunomodulatory Effector Cells in Acute Pulmonary Aspergillosis and Allergic Asthma. PLoS Pathog. 2017, 13, e1006175. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Barnes, P.J. Cytokines in asthma. Thorax 1999, 54, 825–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, A. Th1 and Th2 responses: What are they? BMJ 2000, 321, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.-M.; An, J. Cytokines, inflammation and pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Masaki, K.; Fukunaga, K.; Matsusaka, M.; Kabata, H.; Tanosaki, T.; Mochimaru, T.; Kamatani, T.; Ohtsuka, K.; Baba, R.; Ueda, S.; et al. Characteristics of severe asthma with fungal sensitization. Ann. Allergy Asthma Immunol. 2017, 119, 253–257. [Google Scholar] [CrossRef]
- Hayes, A. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 16 May 2016).
- O’Driscoll, B.R.; Powell, G.; Chew, F.; Niven, R.; Miles, J.F.; Vyas, A.; Denning, D. Comparison of skin prick tests with specific serum immunoglobulin e in the diagnosis of fungal sensitization in patients with severe asthma. Clin. Exp. Allergy. 2009, 39, 1677–1683. [Google Scholar] [CrossRef]
- Medrek, S.K.; Kao, C.C.; Yang, D.H.; Hanania, N.A.; Parulekar, A.D. Fungal sensitization is associated with increased risk of life-threatening asthma. J. Allergy Clin. Immunol. Pract. 2017, 5, 1025–1031.e2. [Google Scholar] [CrossRef]
- Woolnough, K.F.; Richardson, M.; Newby, C.; Craner, M.; Bourne, M.; Monteiro, W.; Siddiqui, S.; Bradding, P.; Pashley, C.; Wardlaw, A.J. The relationship between biomarkers of fungal allergy and lung damage in asthma. Clin. Exp. Allergy 2017, 47, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Wardlaw, A.; Howarth, P.H.; Israel, E.; Taillé, C.; Quirce, S.; Mallett, S.; Bates, S.; Albers, F.C.; Kwon, N. Fungal sensitization and its relationship to mepolizumab response in patients with severe eosinophilic asthma. Clin. Exp. Allergy 2020, 50, 869–872. [Google Scholar] [CrossRef]
- Virchow, J.C., Jr.; Kroegel, C.; Walker, C.; Matthys, H. Cellular and immunological markers of allergic and intrinsic bronchial asthma. Lung 1994, 172, 313–334. [Google Scholar] [CrossRef] [PubMed]
- Sherrill, D.L.; Lebowitz, M.D.; Halonen, M.; Barbee, R.A.; Burrows, B. Longitudinal evaluation of the association between pulmonary function and total serum IgE. Am. J. Respir. Crit. Care Med. 1995, 152, 98–102. [Google Scholar] [CrossRef]
- Burrows, B.; Martinez, F.D.; Halonen, M.; Barbee, R.A.; Cline, M.G. Association of asthma with serum IgE levels and skin-test reactivity to allergens. N. Engl. J. Med. 1989, 320, 271–277. [Google Scholar] [CrossRef]
- Neveu, W.A.; Allard, J.B.; Dienz, O.; Wargo, M.J.; Ciliberto, G.; Whittaker, L.A.; Rincon, M. IL-6 is required for airway mucus production induced by inhaled fungal allergens. J. Immunol. 2009, 183, 1732–1738. [Google Scholar] [CrossRef]
- Ghosh, S.; Hoselton, S.A.; Asbach, S.V.; Steffan, B.N.; Wanjara, S.B.; Dorsam, G.P.; Schuh, J.M. B lymphocytes regulate airway granulocytic inflammation and cytokine production in a murine model of fungal allergic asthma. Cell Mol. Immunol. 2015, 12, 202–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakir, J.; Shannon, J.; Molet, S.; Fukakusa, M.; Elias, J.; Laviolette, M.; Boulet, L.; Hamid, Q. Airway remodeling-associated mediators in moderate to severe asthma: Effect of steroids on TGF-beta, IL-11, IL-17, and type I and type III collagen expression. J. Allergy Clin. Immunol. 2003, 111, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Molet, S.; Hamid, Q.; Davoine, F.; Nutku, E.; Tahaa, R.; Pagé, N.; Olivenstein, R.; Elias, J.; Chakir, J. IL-17 is increased in asthmatic airways and induces human bronchial fibroblasts to produce cytokines. J. Allergy Clin. Immunol. 2001, 108, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Matsuse, H.; Yamagishi, T.; Kodaka, N.; Nakano, C.; Fukushima, C.; Obase, Y.; Mukae, H. Therapeutic modality of plasmacytoid dendritic cells in a murine model of Aspergillus fumigatus sensitized and infected asthma. AIMS Allergy Immunol. 2017, 1, 232–241. [Google Scholar] [CrossRef]
- Bacher, P.; Hohnstein, T.; Beerbaum, E.; Röcker, M.; Blango, M.G.; Kaufmann, S.; Röhmel, J.; Eschenhagen, P.; Grehn, C.; Seidel, K.; et al. Human Anti-fungal Th17 Immunity and Pathology Rely on Cross-Reactivity against Candida albicans. Cell 2019, 176, 1340–1355.e15. [Google Scholar] [CrossRef] [Green Version]
- Conti, H.R.; Gaffen, S.L. IL-17-Mediated Immunity to the Opportunistic Fungal Pathogen Candida albicans. J. Immunol. 2015, 195, 780–788. [Google Scholar] [CrossRef] [Green Version]
- Lagree, K.; Underhill, D.M. Candida-induced asthma steps up to the plate-lets. Immunity 2021, 54, 2442–2444. [Google Scholar] [CrossRef] [PubMed]
- Sandquist, I.; Kolls, J. Update on regulation and effector functions of Th17 cells. F1000Res 2018, 7, 205. [Google Scholar] [CrossRef]
- Zhang, M.A.; Rego, D.; Moshkova, M.; Kebir, H.; Chruscinski, A.; Nguyen, H.; Akkermann, R.; Stanczyk, F.Z.; Prat, A.; Steinman, L.; et al. Peroxisome proliferator-activated receptor (PPAR)α and -γ regulate IFNγ and IL-17A production by human T cells in a sex-specific way. Proc. Natl. Acad. Sci. USA 2012, 109, 9505–9510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newcomb, D.C.; Cephus, J.Y.; Boswell, M.G.; Fahrenholz, J.M.; Langley, E.W.; Feldman, A.S.; Zhou, W.; Dulek, D.E.; Goleniewska, K.; Woodward, K.B.; et al. Estrogen and progesterone decrease let-7f microRNA expression and increase IL-23/IL-23 receptor signaling and IL-17A production in patients with severe asthma. J. Allergy Clin. Immunol. 2015, 136, 1025–1034.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasarte, S.; Elsner, D.; Guía-González, M.; Ramos-Medina, R.; Sánchez-Ramón, S.; Esponda, P.; Muñoz-Fernández, M.A.; Relloso, M. Female sex hormones regulate the Th17 immune response to sperm and Candida albicans. Hum. Reprod. 2013, 28, 3283–3291. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients With Asthma (N = 97) | |
|---|---|
| Age (mean ± SD) | 49.1 ± 18.2 |
| BMI (kg/m2) (mean ± SD) | 24.8 ± 4.2 |
| Gender (N, %) | |
| Male | 39 (40.2%) |
| Female | 58 (59.8%) |
| Smoking status | |
| Never smoker | 82 (84.5%) |
| Ever smoker | 5 (5.2%) |
| Current smoker | 10 (10.3%) |
| Steroid use | |
| No | 41 (42.3%) |
| Yes | 56 (57.7%) |
| ACT (mean ± SD) | 20.3 ± 3.9 |
| FEV1% (mean ± SD) | 71.3 ± 19.3 |
| FEV1/FVC (mean ± SD) | 72.2 ± 12.9 |
| ED visit times (N, %) | |
| 0 times | 90 (92.8%) |
| 1 times | 6 (6.2%) |
| 2 times | 1 (1.0%) |
| Admission times (N, %) | |
| 0 times | 85 (87.6%) |
| 1 times | 9 (9.3%) |
| 2 times | 3 (3.1%) |
| Fungal sensitization (N,%) | |
| Without sensitization | 7 (7.2%) |
| With sensitization | 90 (92.8%) |
| Aspergillus flavus (mean ± SD) | 0.4 ± 0.82 |
| Aspergillus niger (mean ± SD) | 1.26 ± 1.72 |
| Penicillium chrysogenum (mean ± SD) | 0.66 ± 3.32 |
| Botrytis cinerea (mean ± SD) | 3.66 ± 31.35 |
| Fusarium solani (mean ± SD) | 1.34 ± 1.32 |
| Rhodotoeula (mean ± SD) | 2.03 ± 3.46 |
| Trichophyton rubrum (mean ± SD) | 1.12 ± 1.95 |
| Saccharomyces (mean ± SD) | 0.38 ± 0.86 |
| Penicillium (mean ± SD) | 0.22 ± 1 |
| Penicillium notatum (mean ± SD) | 0.2 ± 0.6 |
| Cladosporium herbarum (mean ± SD) | 1.09 ± 3.41 |
| Aspergillus fumigatus (mean ± SD) | 1.6 ± 3.45 |
| Candida albicans (mean ± SD) | 2.23 ± 2.15 |
| Alternaria alternata (mean ± SD) | 0.19 ± 0.6 |
| IgE (mean ± SD) | 394.08 ± 947.1 |
| IL-4 (0.0125–1 ng/mL) (mean ± SD) | 0.025 ± 0.096 |
| IL-6 (ng/mL) (mean ± SD) | 0.446 ± 0.503 |
| IL-9 (0.04–3 ng/mL) (mean ± SD) | 0.258 ± 0.386 |
| IL-10 (0.04–2.5 ng/mL) (mean ± SD) | 0.05 ± 0.089 |
| IL-17 A (0.03125–2 ng/mL) (mean ± SD) | 0.381 ± 0.501 |
| IL-13 (0.0625–4 ng/mL) (mean ± SD) | 0.137 ± 0.394 |
| IL-19 (0.0625–2 ng/mL) (mean ± SD) | 0.195 ± 0.147 |
| IL-22 (0.0125–1 ng/mL) (mean ± SD) | 0.023 ± 0.092 |
| IFN-γ (0.047–1.5 ng/mL) (mean ± SD) | 0.209 ± 0.462 |
| TGF-β (0.03–2 ng/mL) (mean ± SD) | 0.091 ± 0.079 |
| TNF-α (0.03125–2 ng/mL) (mean ± SD) | 0.408 ± 0.602 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Li, Y.-R.; Kor, C.-T.; Lin, S.-H.; Ji, B.-C.; Lin, M.-T.; Chai, W.-H. The Mediating Effect of Cytokines on the Association between Fungal Sensitization and Poor Clinical Outcome in Asthma. Biomedicines 2022, 10, 1452. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061452
Lin C-H, Li Y-R, Kor C-T, Lin S-H, Ji B-C, Lin M-T, Chai W-H. The Mediating Effect of Cytokines on the Association between Fungal Sensitization and Poor Clinical Outcome in Asthma. Biomedicines. 2022; 10(6):1452. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061452
Chicago/Turabian StyleLin, Ching-Hsiung, Yi-Rong Li, Chew-Teng Kor, Sheng-Hao Lin, Bin-Chuan Ji, Ming-Tai Lin, and Woei-Horng Chai. 2022. "The Mediating Effect of Cytokines on the Association between Fungal Sensitization and Poor Clinical Outcome in Asthma" Biomedicines 10, no. 6: 1452. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061452