Chronic Periodontitis and Immunity, Towards the Implementation of a Personalized Medicine: A Translational Research on Gene Single Nucleotide Polymorphisms (SNPs) Linked to Chronic Oral Dysbiosis in 96 Caucasian Patients



 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Enrollment and Inclusion/Exclusion Criteria
2.2. Collection of Subgingival Samples and Characterization of Bacterial DNA Responsible of Periodontitis
2.3. RT-PCR for Bacteria, Viruses, and Fungi
2.4. Analysis of Total Bacteremia Procedure Performed by RT-PCR on V3–V4 in the 16S Ribosomal RNA (rRNA)
2.5. Genotype Frequencies and Statistical Analysis
3. Results
3.1. IL-10 Correlations with VDRs, COLIA1, IL-1α (−889), IL-1β (+3954), IL-1RN (+2018), and TNF-α
3.2. IL-10 Production and Bacteria Presence
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Conflicts of Interest
References
- Fuller, J.; Donos, N.; Suvan, J.; Tsakos, G.; Nibali, L. Association of oral health-related quality of life measures with aggressive and chronic periodontitis. J. Periodontal Res. 2020. [Google Scholar] [CrossRef]
- Patini, R.; Gallenzi, P.; Spagnuolo, G.; Cordaro, M.; Cantiani, M.; Amalfitano, A.; Arcovito, A.; Callà, C.; Mingrone, G.; Nocca, G. Correlation between Metabolic Syndrome, Periodontitis and Reactive Oxygen Species Production. A Pilot Study. Open Dent J. 2017, 11, 621–627. [Google Scholar] [CrossRef] [Green Version]
- Patini, R.; Cattani, P.; Marchetti, S.; Isola, G.; Quaranta, G.; Gallenzi, P. Evaluation of Predation Capability of Periodontopathogens Bacteria by Bacteriovorus HD100. An in Vitro Study. Materials (Basel) 2019, 12, 2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, H.; Varoni, E.M.; Cochis, A.; Cordaro, M.; Gallenzi, P.; Patini, R.; Staderini, E.; Lajolo, C.; Rimondini, L.; Rocchetti, V. Oral dysbiosis in pancreatic cancer and liver cirrhosis: A review of the literature. Biomedicines 2018, 6, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Gruttola, A.K.; Low, D.; Mizoguchi, A.; Mizoguchi, E. Current Understanding of Dysbiosis in Disease in Human and Animal Models. Inflamm. Bowel Dis. 2016, 22, 1137–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, F.R.; Ciccolella, F.; D’Apolito, G.; Papa, F.; Iuso, A.; Salzo, A.E.; Trentadue, R.; Nardi, G.M.; Scivetti, M.; De Matteo, M.; et al. Effect of low-level laser irradiation on osteoblast proliferation and bone formation. J. Biol. Regul. Homeost. Agents 2011, 25, 603–614. [Google Scholar] [PubMed]
- Øvrevik, J.; Refsnes, M.; Låg, M.; Holme, J.A.; Schwarze, P.E. Activation of Proinflammatory Responses in Cells of the Airway Mucosa by Particulate Matter: Oxidant- and Non-Oxidant-Mediated Triggering Mechanisms. Biomolecules 2015, 5, 1399–1440. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Lo Giudice, A.; Polizzi, A.; Alibrandi, A.; Patini, R.; Ferlito, S. Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study. Genes (Basel) 2019, 10, 1022. [Google Scholar] [CrossRef] [Green Version]
- Larsson, L.; Thorbert-Mros, S.; Rymo, L.; Berglundh, T. Influence of epigenetic modifications of the interleukin-10 promoter on IL-10 gene expression. Eur. J Oral. Sci. 2012, 120, 14–20. [Google Scholar] [CrossRef]
- Andersen, V.; Egeberg, R.; Tjønneland, A.; Vogel, U. Interaction between interleukin-10 (IL-10) polymorphisms and dietary fibre in relation to risk of colorectal cancer in a Danish case-cohort study. BMC Cancer 2012, 12, 183. [Google Scholar] [CrossRef] [Green Version]
- Moudi, B.; Heidari, Z.; Mahmoudzadeh-Sagheb, H.; Moudi, M. Analysis of interleukin-10 gene polymorphisms in patients with chronic periodontitis and healthy control. Dent. Res. J. (Isfahan) 2018, 15, 71–79. [Google Scholar] [CrossRef]
- Engelhardt, K.R.; Grimbacher, B. IL-10 in humans: Lessons from the gut, IL-10/IL-10 receptor deficiencies, and IL-10 polymorphisms. Curr. Top Microbiol. Immunol. 2014, 380, 1–18. [Google Scholar] [CrossRef]
- Lovreglio, P.; Bukvic, N.; Fustinoni, S.; Ballini, A.; Drago, I.; Foà, V.; Guanti, G.; Soleo, L. Lack of genotoxic effect in workers exposed to very low doses of 1,3-butadiene. Arch Toxicol. 2006, 80, 378–381. [Google Scholar] [CrossRef]
- Aruni, A.W.; Roy, F.; Fletcher, H.M. Filifactor alocis has virulence attributes that can enhance its persistence under oxidative stress conditions and mediate invasion of epithelial cells by porphyromonas gingivalis. Infect. Immun. 2011, 79, 3872–3886. [Google Scholar] [CrossRef] [Green Version]
- Devine, D.A.; Marsh, P.D.; Meade, J. Modulation of host responses by oral commensal bacteria. J. Oral Microbiol. 2015, 7, 26941. [Google Scholar] [CrossRef]
- Foti, C.; Romita, P.; Rigano, L.; Zimerson, E.; Sicilia, M.; Ballini, A.; Ghizzoni, O.; Antelmi, A.; Angelini, G.; Bonamonte, D.; et al. Isobornyl acrylate: an impurity in alkyl glucosides. Cutan Ocul Toxicol. 2016, 35, 115–119. [Google Scholar] [CrossRef]
- Bouladoux, N.; Hall, J.A.; Grainger, J.R.; dos Santos, L.M.; Kann, M.G.; Nagarajan, V.; Verthelyi, D.; Belkaid, Y. Regulatory role of suppressive motifs from commensal DNA. Mucosal Immunol. 2012, 5, 623–634. [Google Scholar] [CrossRef]
- Cantore, S.; Mirgaldi, R.; Ballini, A.; Coscia, M.F.; Scacco, S.; Papa, F.; Inchingolo, F.; Dipalma, G.; De Vito, D. Cytokine gene polymorphisms associate with microbiogical agents in periodontal disease: Our experience. Int. J. Med. Sci. 2014, 11, 674–679. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Lamont, R.J.; Wu, J.; Xie, H. Role of differential expression of streptococcal arginine deiminase in inhibition of fimA expression in Porphyromonas gingivalis. J. Bacteriol. 2008, 190, 4367–4371. [Google Scholar] [CrossRef] [Green Version]
- Cantore, S.; Ballini, A.; Mori, G.; Dibello, V.; Marrelli, M.; Mirgaldi, R.; De Vito, D.; Tatullo, M. Anti-plaque and antimicrobial efficiency of different oral rinses in a 3-day plaque accumulation model. J. Biol. Regul. Homeost. Agents 2016, 30, 1173–1178. [Google Scholar]
- Xie, H.; Hong, J.; Sharma, A.; Wang, B.Y. Streptococcus cristatus ArcA interferes with Porphyromonas gingivalis pathogenicity in mice. J. Periodontal Res. 2012, 47, 578–583. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Scacco, S.; Coletti, D.; Pluchino, S.; Tatullo, M. Mesenchymal stem cells as promoters, enhancers, and playmakers of the translational regenerative medicine. Stem. Cells Int. 2017, 2017, 3292810. [Google Scholar] [CrossRef] [Green Version]
- Chatzopoulos, G.; Doufexi, A.E.; Wolff, L.; Kouvatsi, A. Interleukin-6 and interleukin-10 gene polymorphisms and the risk of further periodontal disease progression. Braz. Oral Res. 2018, 32, e11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Chen, B.; Yan, F.; Guo, J.; Zhu, X.; Ma, S.; Yang, W. Interleukin-10 inhibits bone resorption: A potential therapeutic strategy in periodontitis and other bone loss diseases. Biomed. Res. Int. 2014, 2014, 284836. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Dipalma, G.; Cirulli, N.; Cantore, S.; Saini, R.S.; Altini, V.; Santacroce, L.; Ballini, A.; Saini, R. Microbiological results of improvement in periodontal condition by administration of oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1323–1328. [Google Scholar]
- Couper, K.N.; Blount, D.G.; Riley, E.M. IL-10: The master regulator of immunity to infection. J. Immunol. 2008, 180, 5771–5777. [Google Scholar] [CrossRef]
- Demangel, C.; Bertolino, P.; Britton, W.J. Autocrine IL-10 impairs dendritic cell (DC)-derived immune responses to mycobacterial infection by suppressing DC trafficking to draining lymph nodes and local IL-12 production. Eur. J. Immunol. 2002, 32, 994–1002. [Google Scholar] [CrossRef]
- Silva, N.; Abusleme, L.; Bravo, D.; Dutzan, N.; Garcia-Sesnich, J.; Vernal, R.; Hernández, M.; Gamonal, J. Host response mechanisms in periodontal diseases. J. Appl. Oral Sci. 2015, 23, 329–355. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Capodiferro, S.; Toia, M.; Cantore, S.; Favia, G.; De Frenza, G.; Grassi, F.R. Evidence-based dentistry: What’s new? Int. J. Med. Sci. 2007, 4, 174–178. [Google Scholar] [CrossRef] [Green Version]
- Hajishengallis, G.; Lamont, R.J. Breaking bad: Manipulation of the host response by Porphyromonas gingivalis. Eur. J. Immunol. 2014, 44, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Cantore, S.; Dedola, A.; Santacroce, L.; Laino, L.; Cicciù, M.; Mastrangelo, F. IL-1 haplotype analysis in periodontal disease. J. Biol. Regul. Homeost. Agents 2018, 32, 433–437. [Google Scholar]
- Crincoli, V.; Ballini, A.; Fatone, L.; Di Bisceglie, M.B.; Nardi, G.M.; Grassi, F.R. Cytokine genotype distribution in patients with periodontal disease and rheumatoid arthritis or diabetes mellitus. J. Biol. Regul. Homeost. Agents 2016, 30, 863–866. [Google Scholar]
- Ballini, A.; Cantore, S.; Farronato, D.; Cirulli, N.; Inchingolo, F.; Papa, F.; Malcangi, G.; Inchingolo, A.D.; Dipalma, G.; Sardaro, N.; et al. Periodontal disease and bone pathogenesis: The crosstalk between cytokines and Porphyromonas Gingivalis. J. Biol. Regul. Homeost. Agents 2015, 29, 273–281. [Google Scholar]
- Mori, G.; Brunetti, G.; Colucci, S.; Oranger, A.; Ciccolella, F.; Sardone, F.; Pignataro, P.; Mori, C.; Karapanou, V.; Ballini, A.; et al. Osteoblast apoptosis in periodontal disease: Role of TNF-related apoptosis-inducing ligand. Int. J. Immunopathol. Pharmacol. 2009, 22, 95–103. [Google Scholar] [CrossRef]
- Ballini, A.; Santacroce, L.; Cantore, S.; Bottalico, L.; Dipalma, G.; Topi, S.; Saini, R.; De Vito, D.; Inchingolo, F. Probiotics Efficacy on Oxidative Stress Values in Inflammatory Bowel Disease: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 373–381. [Google Scholar] [CrossRef]
- Mori, G.; Brunetti, G.; Colucci, S.; Ciccolella, F.; Coricciati, M.; Pignataro, P.; Oranger, A.; Ballini, A.; Farronato, D.; Mastrangelo, F.; et al. Alteration of activity and survival of osteoblasts obtained from human periodontitis patients: Role of TRAIL. J. Biol. Regul. Homeost. Agents 2007, 21, 105–114. [Google Scholar]
- Ballini, A.; Tetè, S.; Scattarella, A.; Cantore, S.; Mastrangelo, F.; Papa, F.; Nardi, G.M.; Perillo, L.; Crincoli, V.; Gherlone, E.; et al. The role of anti-cyclic citrullinated peptide antibody in periodontal disease. Int. J. Immunopathol. Pharmacol. 2010, 23, 677–681. [Google Scholar] [CrossRef]
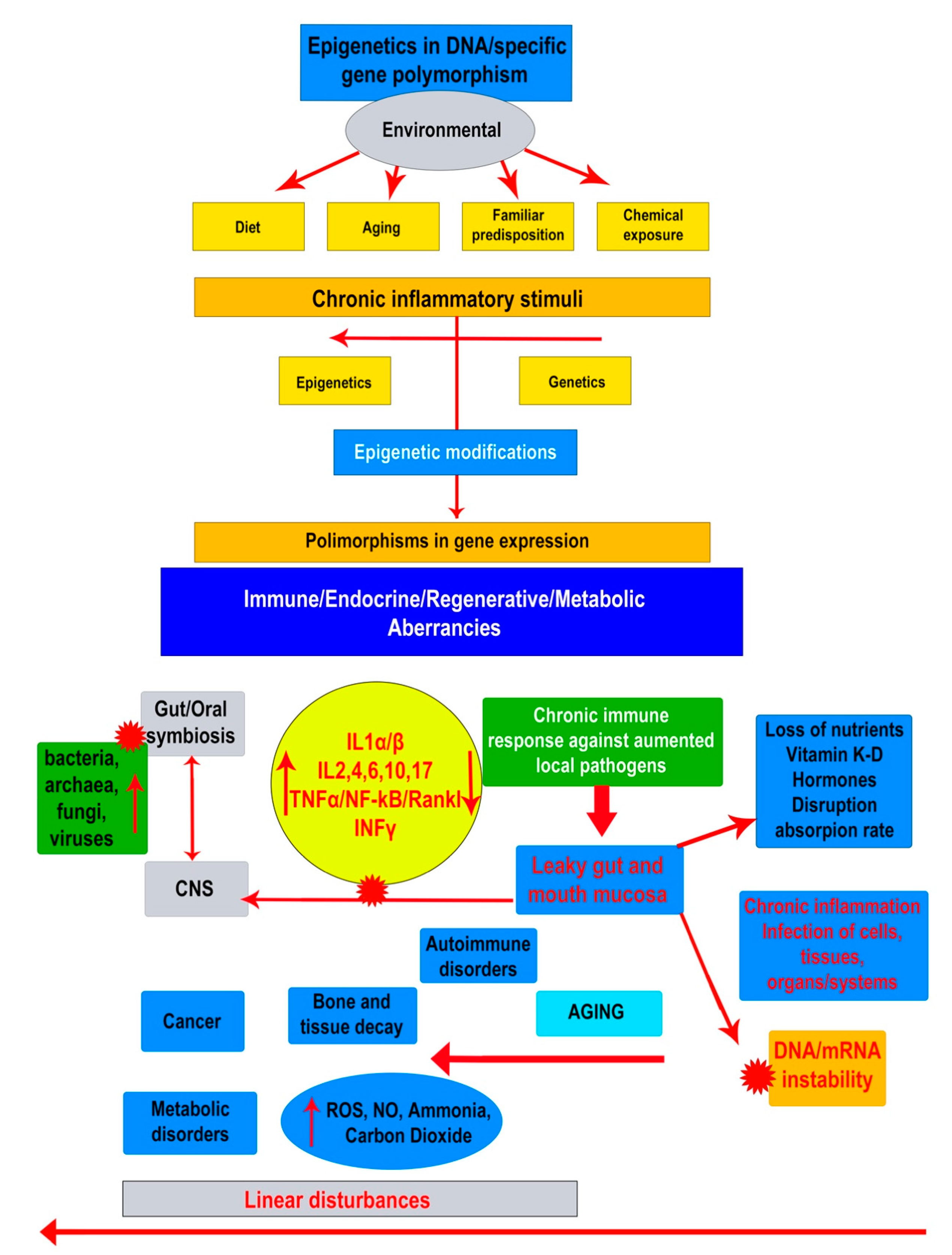
 Indicates the high negative impact of agent or group of agents on a different system or another compound, as bacteria, viruses and fungi on oral/gut eubiosis.
Indicates the high negative impact of agent or group of agents on a different system or another compound, as bacteria, viruses and fungi on oral/gut eubiosis.
Indicates the high negative impact of agent or group of agents on a different system or another compound, as bacteria, viruses and fungi on oral/gut eubiosis.
Indicates the high negative impact of agent or group of agents on a different system or another compound, as bacteria, viruses and fungi on oral/gut eubiosis.

{kind=link}
| SNPs | Effects of Polymorphisms Variants |
|---|---|
| IL-10 (−1082 G > A, −819 C > T, −592 C > A) | -ATA/ATA-ATA/ACC-ACC/ACC: Low production; -ACC/GCC-ATA/GCC: Reduced production; -GCC/GCC: High production. |
| TNF-α (−308 G > A) | -AA-AG: Predisposition to a higher level of inflammation; -GG: Normal level of inflammation |
| IL-1α (−889) IL-1β (+3954) IL-1RN (+2018) | No alteration Low alteration/Moderate alteration Severe alteration |
| TaqI VDR (−1056 T > C) | -tt: Not associated with increased susceptibility of developing periodontal disease and associated with normal serum levels of Vitamin D; -Tt: Greater susceptibility to develop the periodontal disease unrelated to reduced serum levels of Vitamin D; -TT: Greater susceptibility to develop the periodontal disease correlated with reduced serum levels of Vitamin D, with effects on the bone metabolism and immune response |
| ApaI VDR (+64,978 G > T) | -AA-Aa: Predisposition to osteoporosis; -aa: No predisposition to osteoporosis |
| BsmI VDR (+63,980 G > A) | -BB-Bb: Predisposition to decrease BMD and to reduce intestinal calcium absorption; -bb: No predisposition to decrease of BMD and to reduce intestinal calcium absorption |
| FokI VDR (+30,920 T > C) | -FF-Ff: Predisposition to decrease BMD; -ff: No predisposition to decrease BMD |
| COLIA1 (polymorphism in collagen type-lα) (2046 G > T) | -ss-Ss: Predisposition to osteoporosis; -SS: No predisposition to osteoporosis |
| Strain Name and Phenotypes | Status of Aggression |
|---|---|
| Aggregatibacter actinomycetemcomitans G−, Ana (fac) | Highly aggressive |
| Tannerella forsythensys G−, Ana | Aggressive |
| Porphyromonas gingivalis G−, Ana | Aggressive |
| Treponema denticola G−, Ana | Aggressive |
| Peptostreptococcus micros (Micromonas) G+, Ana | Aggressive |
| Filifactor alocis G+, Ana | Aggressive |
| Synergistetes G−, Ana | Aggressive |
| Porphyromonas endodontalis G−, Ana | Aggressive |
| Fusobacterium nucleatum ssp. G−, Ana | Medium aggressive |
| Campylobacter rectus G−, Ana (fac) | Medium aggressive |
| Prevotella intermedia G−, Ana | Medium aggressive |
| Leptotrichia hofstadii G−, Ana | Medium aggressive |
| Rothia dentocariosa D+, Aer | Medium aggressive |
| Eikenella corrodens G−, Ana (fac), oral, gut | Low aggressive |
| Cardiobacterium hominis G−, Aer | Low aggressive |
| Bacteria | Nucleotide Primer Sequence |
|---|---|
| Porphyromonas gingivalis FW Porphyromonas gingivalis PROBE Porphyromonas gingivalis REV | 5′ GCG CTC AAC GGT TCA GCC 3′ 5′ CACTGAACTCAAGCCGGCAGTTTC 3′ 5′ CAC GAA TTC CGC CTG C 3′ |
| A. actinomycetemcomitans FW A. actinomycetemcomitans PROBE A. actinomycetemcomitans REV | 5′ GAACCT TACCTACTCTTGACATCC GAA 3′ 5′ AGACTCAGAGATGGGTTTGTGCCTTAGGG 3′ 5′ TGCAGCACCTGTCTCAAAGC 3′ |
| Tannerella forsythia FW Tannerella forsythia PROBE | 5′ACATCGTGCAGGAAGGTGTA 3′ 5′ ACTCGGCAATGACAGGAAGT 3′ |
| Tannerella forsythia REV | 5′ ACAGGGCGGAGTTGATTACA 3′ |
| Peptostreptococcus micros FW Peptostreptococcus micros PROBE Peptostreptococcus micros REV | 5′AGCCATTGAAGACACTTTGGT 3′ 5′AGTGCAGATGTAAAAGTC 3′ 5′ TGCCGAAGTTTCTAGCCAAA 3′ |
| Fusobacterium nucleatum FW Fusobacterium nucleatum REV | 5′ CAACCATTACTTTAACTCTACCATGTTCA 3′ 5′ GTTGACTTTACAGAAGGAGATTATGTAAAAATC 3′ |
| Prevotella intermedia FW Prevotella intermedia REV | 5′ CCTGAGGTCTTCGATGCGTG’ 3′ 5′ TGGGCAAGCATAGACCAAGA 3′ |
| Campylobacter rectus FW Campylobacter rectus REV | 5′ AGCGCAACCCACGTG’3′ 5′ CGCCATTGTAGCACG 3′ |
| Eikenella corrodens FW Eikenella corrodens PROBE Eikenella corrodens REV | 5′ ATGTGAAATCCCCGGGCTTA 3′ 5′ CCCTGGGATAACACTGAC 3′ 5′ CTGTTTGCTACCCACGCTTT 3′ |
| Treponema denticola FW Treponema denticola PROBE Treponema denticola REV | 5′ ATTTCGACTTTATGCGGGCC 3′ 5′ TCGGCAACAGAAGCATTGTC 3′ 5′ AGGGGATAATTATGGGGCGG 3′ |
| Bacteria | Sequence (FAM) | Size |
|---|---|---|
| Rothia dentocariosa FW Rothia dentocariosa PROBE Rothia dentocariosa REV | 5′ ATGATGCAGAACCCCGTACA 3′ 5′ ACACCGAAAAATCGCCCTTC 3′ 5′ TGGGCCTGATGACCTTTTCT 3′ | 215 pb |
| Synergistetes FW Synergistetes PROBE Synergistetes REV | 5′ TTGAGACTGAGGTGCTGGAG 3′ 5′ TCCCAGTGTAGCGGTGAAAT 3′ 5′ TCTAATCCCGTTCGCTACCC 3′ | 156 pb |
| Filifactor Alocis FW Filifactor Alocis PROBE Filifactor Alocis REV | 5′ ATACAGTCCGTTTCCACCGT 3′ 5′ ACTCGGCAATGACAGGAAGT 3′ 5′ ACTGATCCTGACCGTTCCTC 3′ | 172 pb |
| Porphyromonas endodontalis FW Porphyromonas endodontalis PROBE Porphyromonas endodontalis REV | 5′ GCTCAACTGTAGTCTTGCCG 3′ 5′ TGCTAGAGAGGAGACGAGGT 3′ 5′ TGTTTGATCCCCACGCTTTC 3′ | 168 pb |
| Cardiobacterium hominis FW Cardiobacterium hominis PROBE Cardiobacterium hominis REV | 5′ GAGCCAATCTGAGAAAGCCG 3′ 5′ TACGTTCCCGGGTCTTGTAC 3′ 5′ GCGCCCTCCTAAGTTAAGCT 3′ | 187 pb |
| Leptotrichia buccalis FW Leptotrichia buccalis REV | 5 TTGTAAAGGGGATGGCGACT 3′ 5′ GTCCCGCTCCAACAACAATT 3′ | 248 pb |
| Capnocytophaga sputigena FW Capnocytophaga sputigena REV | 5′ GCAAGTCGAGGGAGAGGTTA 3′ 5′ GAGCCGTTACCTCTCCAACT 3′ | 208 pb |
| Gene Expression | Count (Subjects): | IL-10 | ||
|---|---|---|---|---|
| 22 | 40 | 34 | ||
| GCC/GCC | ATA/GCC | All Severity = 2 | ||
| Grade of SNPs and Haplotype | 0 | 1 | 2 | |
| IL-1 α/β/RN | 0 | 32% = 7 | 35% = 14p | 21% = 7p |
| 1 | 55% = 12p | 35% = 14p | 50% = 17p | |
| 2 | 14% = 3p | 30% = 12p | 29% = 10p | |
| TNF-α | 0 GG | 77% = 17p | 78% = 31p | 65% = 22p |
| 1 AG | 23% = 5p | 23% = 9p | 32% = 11p | |
| 2 AA | 0% = 0p | 0% = 0p | 3% = 1p | |
| Tagl VDR | 0 tt | 5% = 1p | 8% = 3p | 18% = 6p |
| 1 Tt | 59% = 13p | 50% = 20p | 41% = 14p | |
| 2 TT | 36% = 8p | 43% = 17p | 41% = 14p | |
| Apal VDR | 0 aa | 14% = 3p | 25% = 10p | 6% = 2p |
| 1 Aa | 55% = 12p | 45% = 18p | 71% = 24p | |
| 2 AA | 32% = 7p | 30% = 12p | 24% = 8p | |
| Bsml VDR | 0 bb | 32% = 7p | 50% = 20p | 44% = 15p |
| 1Bb | 23% = 15p | 45% = 18p | 50% = 18p | |
| 2 BB | 45% = 0p | 5% = 2p | 6% = 2p | |
| Fokl VDR | 0 ff | 9% = 2p | 13% = 5p | 3% = 1p |
| 1 Ff | 50% = 11p | 55% = 22p | 50% = 17p | |
| 2 FF | 41% = 9p | 33% = 13p | 47% = 16p | |
| COLIA 1 | 0 SS | 32% = 10p | 35% = 15p | 21% = 19p |
| 1 Ss | 55% = 9p | 35% = 14p | 50% = 9p | |
| 2ss | 14% = 3p | 30% = 1p | 29% = 2p | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, F.; Martelli, F.S.; Gargiulo Isacco, C.; Borsani, E.; Cantore, S.; Corcioli, F.; Boddi, A.; Nguyễn, K.C.D.; De Vito, D.; Aityan, S.K.; et al. Chronic Periodontitis and Immunity, Towards the Implementation of a Personalized Medicine: A Translational Research on Gene Single Nucleotide Polymorphisms (SNPs) Linked to Chronic Oral Dysbiosis in 96 Caucasian Patients. Biomedicines 2020, 8, 115. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8050115
Inchingolo F, Martelli FS, Gargiulo Isacco C, Borsani E, Cantore S, Corcioli F, Boddi A, Nguyễn KCD, De Vito D, Aityan SK, et al. Chronic Periodontitis and Immunity, Towards the Implementation of a Personalized Medicine: A Translational Research on Gene Single Nucleotide Polymorphisms (SNPs) Linked to Chronic Oral Dysbiosis in 96 Caucasian Patients. Biomedicines. 2020; 8(5):115. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8050115
Chicago/Turabian StyleInchingolo, Francesco, Francesco Saverio Martelli, Ciro Gargiulo Isacco, Elisa Borsani, Stefania Cantore, Fabiana Corcioli, Anna Boddi, Kieu C.D. Nguyễn, Danila De Vito, Sergey K. Aityan, and et al. 2020. "Chronic Periodontitis and Immunity, Towards the Implementation of a Personalized Medicine: A Translational Research on Gene Single Nucleotide Polymorphisms (SNPs) Linked to Chronic Oral Dysbiosis in 96 Caucasian Patients" Biomedicines 8, no. 5: 115. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8050115