
Pathological Significance of Macrophages in Erectile Dysfunction Including Peyronie’s Disease

 , , and
, , and
Abstract
:1. Introduction
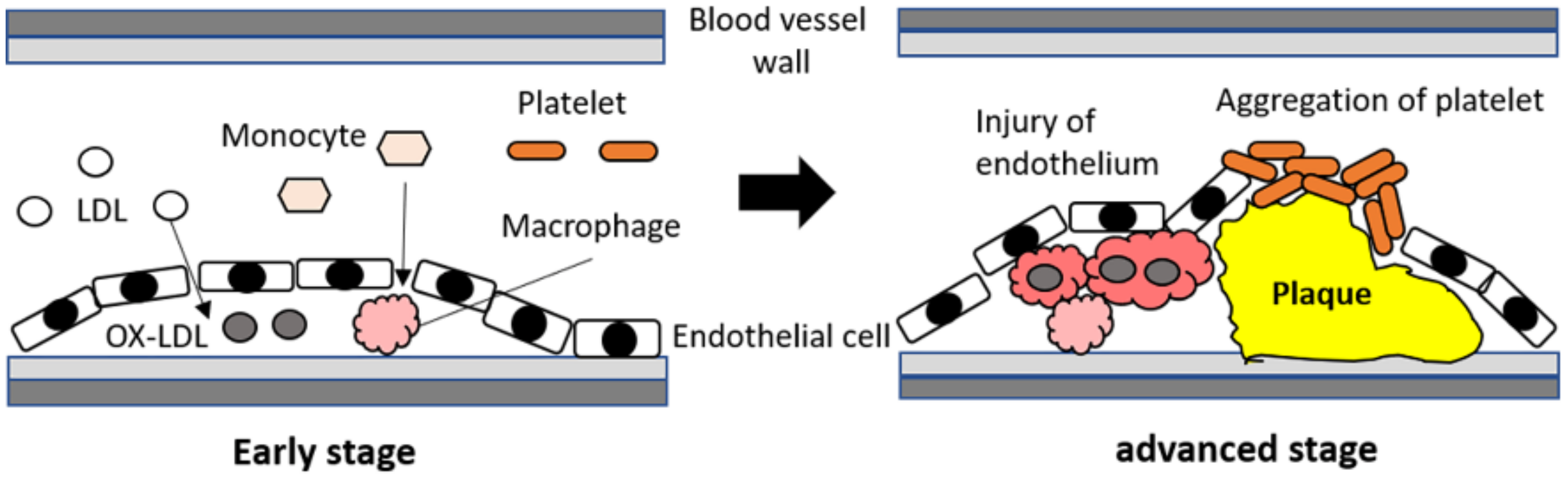
2. Vasculogenic Erectile Dysfunction
3. Neurogenic Erectile Dysfunction
4. Obesity-Related Erectile Dysfunction and Macrophages
4.1. High-Fat Diet and Erectile Dysfunction
4.2. Cytokines and Macrophages in High-Fat Diet-Related Erectile Dysfunction
4.3. Physical Activity
5. Stem Cell Therapy and Macrophages
5.1. Stem Cells and Erectile Dysfunction
5.2. Adipose Tissue-Derived Stem Cell Therapy and Macrophages
5.3. Mesenchymal Stem Cell Therapy and Macrophages
6. Phosphodiesterase Type 5 Inhibitors and Macrophages
6.1. Phosphodiesterase Type 5 Inhibitors and Macrophages in Inflammatory Diseases
6.2. Phosphodiesterase Type 5 Inhibitors and Macrophages in the Treatment
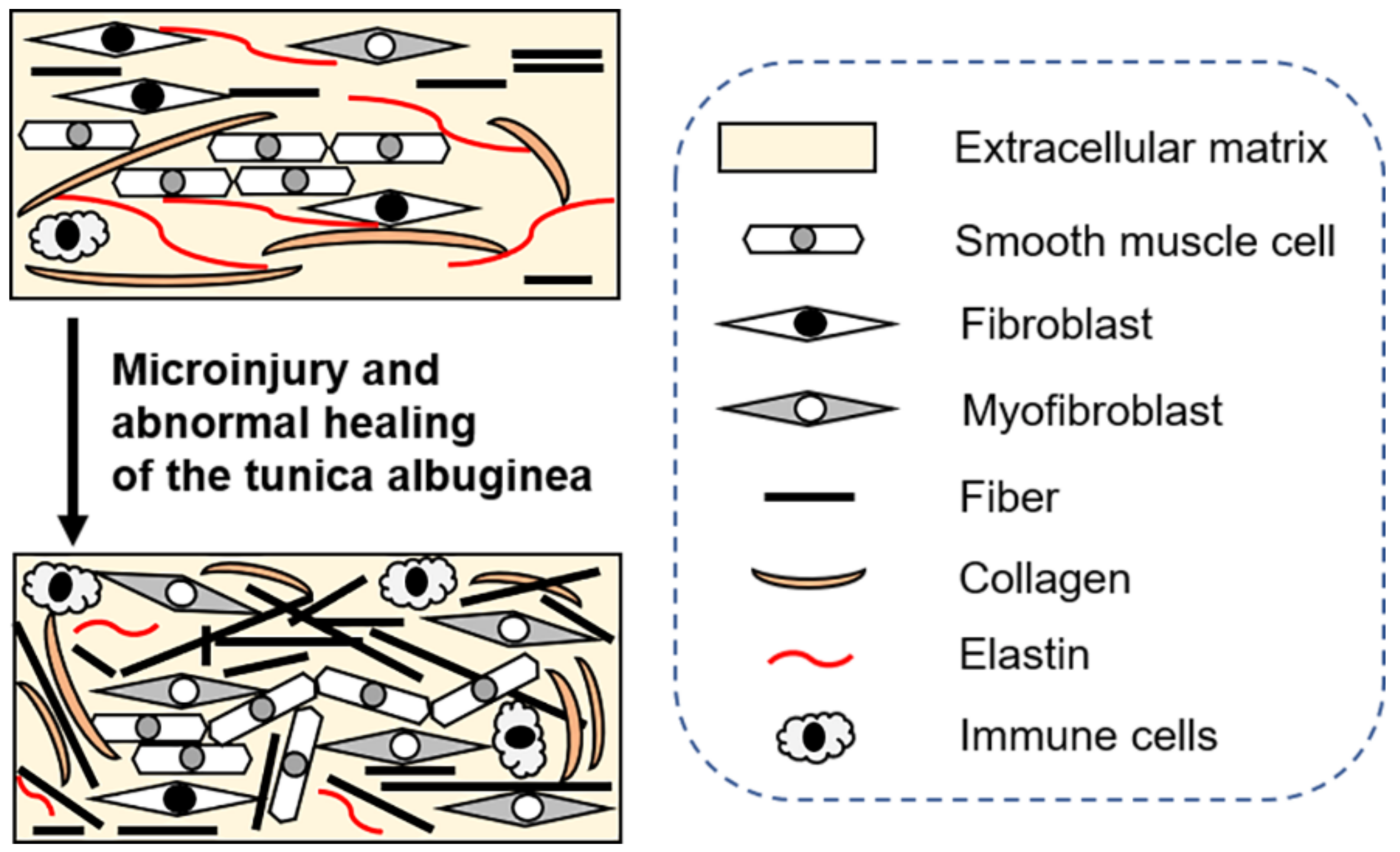
7. Peyronie’s Disease and Macrophages
7.1. Peyronie’s Disease and Erectile Dysfunction
7.2. Molecular Mechanisms Underlying Peyronie’s Disease
7.2.1. Fibrosis and Macrophages
7.2.2. Other Factors and Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ralph, D.J. Normal erectile function. Clin. Cornerstone 2005, 7, 13–18. [Google Scholar] [CrossRef]
- Ghalayini, I.F. Nitric oxide-cyclic GMP pathway with some emphasis on cavernosal contractility. Int. J. Impot. Res. 2004, 16, 459–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simsek, A.; Tugcu, V.; Erturkuner, P.; Alkan, F.; Ozbek, E.; Tasci, A.I. Effects of the recreational use of PDE5 inhibitors on the corpus cavernosum of young, healthy rats. Int. Urol. Nephrol. 2014, 46, 1889–1893. [Google Scholar] [CrossRef]
- Dean, R.C.; Lue, T.F. Physiology of penile erection and pathophysiology of erectile dysfunction. Urol. Clin. N. Am. 2005, 32, 379–395. [Google Scholar] [CrossRef]
- Barbonetti, A.; D’Andrea, S.; Castellini, C.; Totaro, M.; Muselli, M.; Cavallo, F.; Felzani, G.; Necozione, S.; Francavilla, S. Erectile Dysfunction Is the Main Correlate of Depression in Men with Chronic Spinal Cord Injury. J. Clin. Med. 2021, 10, 2090. [Google Scholar] [CrossRef]
- Francis, S.H.; Corbin, J.D. Phosphodiesterase-5 inhibition: The molecular biology of erectile function and dysfunction. Urol. Clin. N. Am. 2005, 32, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Montorsi, F.; Brock, G.; Stolzenburg, J.U.; Mulhall, J.; Moncada, I.; Patel, H.R.; Chevallier, D.; Krajka, K.; Henneges, C.; Dickson, R.; et al. Effects of tadalafil treatment on erectile function recovery following bilateral nerve-sparing radical prostatectomy: A randomised placebo-controlled study (REACTT). Eur. Urol. 2014, 65, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Delporte, C.; Van Antwerpen, P.; Vanhamme, L.; Roumeguère, T.; Zouaoui Boudjeltia, K. Low-density lipoprotein modified by myeloperoxidase in inflammatory pathways and clinical studies. Mediat. Inflamm. 2013, 2013, 971579. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, S.; Minaldi, E.; Castellini, C.; Cavallo, F.; Felzani, G.; Francavilla, S.; Francavilla, F.; Barbonetti, A. Independent Association of Erectile Dysfunction and Low Testosterone Levels With Life Dissatisfaction in Men With Chronic Spinal Cord Injury. J. Sex. Med. 2020, 17, 911–918. [Google Scholar] [CrossRef]
- Abufaraj, M.; Siyam, A.; Ali, M.R.; Suarez-Ibarrola, R.; Yang, L.; Foerster, B.; Shariat, S.F. Functional Outcomes after Local Salvage Therapies for Radiation-Recurrent Prostate Cancer Patients: A Systematic Review. Cancers 2021, 13, 244. [Google Scholar] [CrossRef]
- Milenkovic, U.; Boeckx, B.; Lambrechts, D.; Janky, R.; Hatzichristodoulou, G.; van Renterghem, K.; Gevaert, T.; Cellek, S.; Bivalacqua, T.J.; De Ridder, D.; et al. Single-cell Transcriptomics Uncover a Novel Role of Myeloid Cells and T-lymphocytes in the Fibrotic Microenvironment in Peyronie’s Disease. Eur. Urol. Focus 2021, in press. [Google Scholar] [CrossRef]
- Nicolai, M.; Urkmez, A.; Sarikaya, S.; Fode, M.; Falcone, M.; Albersen, M.; Gul, M.; Hatzichristodoulou, G.; Capogrosso, P.; Russo, G.I. Penile Rehabilitation and Treatment Options for Erectile Dysfunction Following Radical Prostatectomy and Radiotherapy: A Systematic Review. Front. Surg. 2021, 8, 636974. [Google Scholar] [CrossRef]
- Wang, T.D.; Lee, C.K.; Chia, Y.C.; Tsoi, K.; Buranakitjaroen, P.; Chen, C.H.; Cheng, H.M.; Tay, J.C.; Teo, B.W.; Turana, Y.; et al. Hypertension and erectile dysfunction: The role of endovascular therapy in Asia. J. Clin. Hypertens 2021, 23, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.M.; Gallagher, K.A. Epigenetic Mechanisms in Monocytes/Macrophages Regulate Inflammation in Cardiometabolic and Vascular Disease. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 623–634. [Google Scholar] [CrossRef] [Green Version]
- Barrett, T.J. Macrophages in Atherosclerosis Regression. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 20–33. [Google Scholar] [CrossRef]
- Culha, M.G.; Canat, L.; Degirmentepe, R.B.; Albayrak, A.T.; Atalay, H.A.; Merder, E.; Ariman, A.; Altunrende, F. The correlation between atherogenic indexes and erectile dysfunction. Aging Male 2020, 23, 1232–1236. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Ma, Z.; Zhang, X.L.; Guo, L.Q.; Yuan, M.Z. Significance of blood lipid parameters as effective markers for arteriogenic erectile dysfunction. Andrology 2020, 8, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Hartley, A.; Haskard, D.; Khamis, R. Oxidized LDL and anti-oxidized LDL antibodies in atherosclerosis—Novel insights and future directions in diagnosis and therapy. Trends Cardiovasc. Med. 2019, 29, 22–26. [Google Scholar] [CrossRef]
- Marchio, P.; Guerra-Ojeda, S.; Vila, J.M.; Aldasoro, M.; Victor, V.M.; Mauricio, M.D. Targeting Early Atherosclerosis: A Focus on Oxidative Stress and Inflammation. Oxid. Med. Cell Longev. 2019, 2019, 8563845. [Google Scholar] [CrossRef]
- Itabe, H.; Sawada, N.; Makiyama, T.; Obama, T. Structure and Dynamics of Oxidized Lipoproteins In Vivo: Roles of High-Density Lipoprotein. Biomedicines 2021, 9, 655. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.V.; Nikiforov, N.G.; Markin, A.M.; Kashirskikh, D.A.; Myasoedova, V.A.; Gerasimova, E.V.; Orekhov, A.N. Overview of OxLDL and Its Impact on Cardiovascular Health: Focus on Atherosclerosis. Front. Pharmacol. 2021, 11, 613780. [Google Scholar] [CrossRef] [PubMed]
- Helmke, A.; Casper, J.; Nordlohne, J.; David, S.; Haller, H.; Zeisberg, E.M.; von Vietinghoff, S. Endothelial-to-mesenchymal transition shapes the atherosclerotic plaque and modulates macrophage function. FASEB J. 2019, 33, 2278–2289. [Google Scholar] [CrossRef] [Green Version]
- Maretti-Mira, A.C.; Golden-Mason, L.; Salomon, M.P.; Kaplan, M.J.; Rosen, H.R. Cholesterol-Induced M4-Like Macrophages Recruit Neutrophils and Induce NETosis. Front. Immunol. 2021, 3, 671073. [Google Scholar] [CrossRef]
- Randrup, E.; Baum, N.; Feibus, A. Erectile dysfunction and cardiovascular disease. Postgrad. Med. 2015, 127, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Benaragama, K.S.; Singh, A.A.; Taj, T.; Hague, J.; Boyle, J.R.; Richards, T. Erectile Dysfunction in Peripheral Vascular Disease: Endovascular Revascularization as a Potential Therapeutic Target. Vasc. Endovascular. Surg. 2020, 54, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Shim, J.S.; Kim, J.W.; Doo, S.W.; Bae, J.H.; Lee, J.H.; Song, Y.S.; Kim, J.J.; Moon, D.G. Molecular and Histologic Evidence of Novel Erectile Dysfunction Rat Model as an Aging Atherosclerosis Model: A Preliminary Study. World J. Men’s Health 2020, 38, 345–352. [Google Scholar] [CrossRef]
- Nasser, M.I.; Zhu, S.; Huang, H.; Zhao, M.; Wang, B.; Ping, H.; Geng, Q.; Zhu, P. Macrophages: First guards in the prevention of cardiovascular diseases. Life Sci. 2020, 250, 117559. [Google Scholar] [CrossRef] [PubMed]
- Shiomi, M. The History of the WHHL Rabbit, an Animal Model of Familial Hypercholesterolemia (I)—Contribution to the Elucidation of the Pathophysiology of Human Hypercholesterolemia and Coronary Heart Disease. J. Atheroscler. Thromb. 2020, 27, 105–118. [Google Scholar] [CrossRef] [Green Version]
- Giglio, R.V.; Pantea Stoian, A.; Al-Rasadi, K.; Banach, M.; Patti, A.M.; Ciaccio, M.; Rizvi, A.A.; Rizzo, M. Novel Therapeutical Approaches to Managing Atherosclerotic Risk. Int. J. Mol. Sci. 2021, 22, 4633. [Google Scholar] [CrossRef]
- Surdu, A.M.; Pînzariu, O.; Ciobanu, D.M.; Negru, A.G.; Căinap, S.S.; Lazea, C.; Iacob, D.; Săraci, G.; Tirinescu, D.; Borda, I.M.; et al. Vitamin D and Its Role in the Lipid Metabolism and the Development of Atherosclerosis. Biomedicines 2021, 9, 172. [Google Scholar] [CrossRef]
- Zouaoui Boudjeltia, K.; Roumeguere, T.; Delree, P.; Moguilevsky, N.; Ducobu, J.; Vanhaeverbeek, M.; Wespes, E. Presence of LDL modified by myeloperoxidase in the penis in patients with vascular erectile dysfunction: A preliminary study. Eur. Urol. 2007, 51, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Loria, V.; Dato, I.; Graziani, F.; Biasucci, L.M. Myeloperoxidase: A new biomarker of inflammation in ischemic heart disease and acute coronary syndromes. Mediat. Inflamm. 2008, 2008, 135625. [Google Scholar] [CrossRef] [Green Version]
- Karakas, M.; Koenig, W. Myeloperoxidase production by macrophage and risk of atherosclerosis. Curr. Atheroscler. Rep. 2012, 14, 277–283. [Google Scholar] [CrossRef]
- Boudjeltia, K.Z.; Delporte, C.; Van Antwerpen, P.; Franck, T.; Serteyn, D.; Moguilevsky, N.; Raes, M.; Vanhamme, L.; Vanhaeverbeek, M.; Van Meerhaeghe, A.; et al. Myeloperoxidase-dependent LDL modifications in bloodstream are mainly predicted by angiotensin II, adiponectin, and myeloperoxidase activity: A cross-sectional study in men. Mediat. Inflamm. 2013, 2013, 750742. [Google Scholar] [CrossRef] [Green Version]
- Calay, D.; Rousseau, A.; Mattart, L.; Nuyens, V.; Delporte, C.; Van Antwerpen, P.; Moguilevsky, N.; Arnould, T.; Boudjeltia, K.Z.; Raes, M. Copper and myeloperoxidase-modified LDLs activate Nrf2 through different pathways of ROS production in macrophages. Antioxid. Redox Signal. 2010, 13, 1491–1502. [Google Scholar] [CrossRef]
- Rendra, E.; Riabov, V.; Mossel, D.M.; Sevastyanova, T.; Harmsen, M.C.; Kzhyshkowska, J. Reactive oxygen species (ROS) in macrophage activation and function in diabetes. Immunobiology 2019, 224, 242–253. [Google Scholar] [CrossRef]
- Thomas, C.; Konstantinidis, C. Neurogenic Erectile Dysfunction. Where Do We Stand? Medicines 2021, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Basourakos, S.P.; Kowalczyk, K.J.; Moschovas, M.; Dudley, V.; Shoag, J.E.; Patel, V.; Hu, J.C. Robot-Assisted Radical Prostatectomy Maneuvers to Attenuate Erectile Dysfunction: Technical Description and Video Compilation. J. Endourol. 2021. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Liu, S.; Yang, Y.; Bai, Y.; Li, D.; Han, P.; Wei, W. Generating comprehensive comparative evidence on various interventions for penile rehabilitation in patients with erectile dysfunction after radical prostatectomy: A systematic review and network meta-analysis. Transl. Androl. Urol. 2021, 10, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Hunt, A.A.; Choudhury, K.R.; Nukala, V.; Nolan, M.W.; Ahmad, A.; Ashcraft, K.A.; Koontz, B.F. Risk of erectile dysfunction after modern radiotherapy for intact prostate cancer. Prostate Cancer Prostatic Dis. 2021, 24, 128–134. [Google Scholar] [CrossRef]
- Schauer, I.; Keller, E.; Müller, A.; Madersbacher, S. Have rates of erectile dysfunction improved within the past 17 years after radical prostatectomy? A systematic analysis of the control arms of prospective randomized trials on penile rehabilitation. Andrology 2015, 3, 661–665. [Google Scholar] [CrossRef] [Green Version]
- Matsui, H.; Sopko, N.A.; Hannan, J.L.; Reinhardt, A.A.; Kates, M.; Yoshida, T.; Liu, X.; Castiglione, F.; Hedlund, P.; Weyne, E.; et al. M1 Macrophages Are Predominantly Recruited to the Major Pelvic Ganglion of the Rat Following Cavernous Nerve Injury. J. Sex. Med. 2017, 14, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Matsui, H.; Sopko, N.A.; Campbell, J.D.; Liu, X.; Reinhardt, A.; Weyne, E.; Castiglione, F.; Albersen, M.; Hannan, J.L.; Bivalacqua, T.J. Increased Level of Tumor Necrosis Factor-Alpha (TNF-α) Leads to Downregulation of Nitrergic Neurons Following Bilateral Cavernous Nerve Injury and Modulates Penile Smooth Tone. J. Sex. Med. 2021, 18, 1181–1190. [Google Scholar] [CrossRef]
- Cohen, D.J.; Reynaldo, W.V.; Borba, V.B.; Theodoro, T.R.; Petri, G.; Cavalheiro, R.P.; Mader, A.M.; Han, S.W.; Pinhal, M.A.; Glina, S. New in vivo model to assess macroscopic, histological, and molecular changes in Peyronie’s disease. Andrology 2021. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Batlle, E.; Massagué, J. Transforming Growth Factor-β Signaling in Immunity and Cancer. Immunity 2019, 50, 924–940. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Qiu, H.; Xue, M.; Zhang, S.; Zhang, X.; Xu, J.; Chen, J.; Yang, Y.; Xie, J. MSC-secreted TGF-β regulates lipopolysaccharide-stimulated macrophage M2-like polarization via the Akt/FoxO1 pathway. Stem Cell Res. Ther. 2019, 10, 345. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, E.; Fujimori, M.; Kodama, H.; Felsen, D.; Chen, J.; Durack, J.C.; Solomon, S.B.; Coleman, J.A.; Srimathveeravalli, G. Macrophage-secreted TGF-β 1 contributes to fibroblast activation and ureteral stricture after ablation injury. Am. J. Physiol. Ren. Physiol. 2019, 317, F52–F64. [Google Scholar] [CrossRef]
- Ingman, W.V.; McGrath, L.M.; Breed, W.G.; Musgrave, I.F.; Robker, R.L.; Robertson, S.A. The mechanistic basis for sexual dysfunction in male transforming growth factor beta1 null mutant mice. J. Androl. 2010, 31, 95–107. [Google Scholar] [CrossRef]
- Ostfeld, R.J.; Allen, K.E.; Aspry, K.; Brandt, E.J.; Spitz, A.; Liberman, J.; Belardo, D.; O’Keefe, J.H.; Aggarwal, M.; Miller, M.; et al. Vasculogenic Erectile Dysfunction: The Impact of Diet and Lifestyle. Am. J. Med. 2021, 134, 310–316. [Google Scholar] [CrossRef]
- Rodriguez, J.J.; Al Dashti, R.; Schwarz, E.R. Linking erectile dysfunction and coronary artery disease. Int. J. Impot. Res. 2005, 17, S12–S18. [Google Scholar] [CrossRef] [Green Version]
- Calogero, A.E.; Burgio, G.; Condorelli, R.A.; Cannarella, R.; La Vignera, S. Epidemiology and risk factors of lower urinary tract symptoms/benign prostatic hyperplasia and erectile dysfunction. Aging Male 2019, 22, 12–19. [Google Scholar] [CrossRef]
- Odom, M.R.; Hunt, T.C.; Pak, E.S.; Hannan, J.L. High-fat diet induces obesity in adult mice but fails to develop pre-penile and penile vascular dysfunction. Int. J. Impot. Res. 2021, 4, 1–9. [Google Scholar] [CrossRef]
- Nguyen, S.; Mangubat, M.; Eleswarapu, S.; Wilson, J.B.; Molina, J.; Abraham, A.; Artaza, J.N.; Friedman, T.C.; Ferrini, M.G. The Combination of High-Fat Diet and Oral Marijuana Promotes the Development of Fibrosis in the Mouse Corpora Cavernosa. Sex. Med. 2021, 9, 100312. [Google Scholar] [CrossRef] [PubMed]
- Kratz, M.T.; Schirmer, S.H.; Baumhäkel, M.; Böhm, M. Improvement of endothelial function in a murine model of mild cholesterol-induced atherosclerosis by mineralocorticoid antagonism. Atherosclerosis 2016, 251, 291–298. [Google Scholar] [CrossRef]
- Priviero, F.; Calmasini, F.; Justina, V.D.; Wenceslau, C.F.; McCarthy, C.G.; Webb, R.C. Macrophage-Specific Toll Like Receptor 9 (TLR9) Causes Corpus Cavernosum Dysfunction in Mice Fed a High Fat Diet. J. Sex. Med. 2021, 18, 723–731. [Google Scholar] [CrossRef]
- Morelli, A.; Filippi, S.; Comeglio, P.; Sarchielli, E.; Cellai, I.; Pallecchi, M.; Bartolucci, G.; Danza, G.; Rastrelli, G.; Corno, C.; et al. Physical activity counteracts metabolic syndrome-induced hypogonadotropic hypogonadism and erectile dysfunction in the rabbit. Am. J. Physiol. Endocrinol. Metab. 2019, 316, E519–E535. [Google Scholar] [CrossRef]
- Chin, S.H.; Kahathuduwa, C.N.; Binks, M. Physical activity and obesity: What we know and what we need to know. Obes. Rev. 2016, 17, 1226–1244. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The Effects of Exercise and Physical Activity on Weight Loss and Maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Lisevick, A.; Cartmel, B.; Harrigan, M.; Li, F.; Sanft, T.; Fogarasi, M.; Irwin, M.L.; Ferrucci, L.M. Effect of the Lifestyle, Exercise, and Nutrition (LEAN) Study on Long-Term Weight Loss Maintenance in Women with Breast Cancer. Nutrients 2021, 13, 3265. [Google Scholar] [CrossRef]
- Washburn, R.A.; Szabo-Reed, A.N.; Gorczyca, A.M.; Sullivan, D.K.; Honas, J.J.; Mayo, M.S.; Krebill, R.; Goetz, J.; Ptomey, L.T.; Lee, J.; et al. A Randomized Trial Evaluating Exercise for the Prevention of Weight Regain. Obesity 2021, 29, 62–70. [Google Scholar] [CrossRef]
- Noland, R.C. Exercise and Regulation of Lipid Metabolism. Prog. Mol. Biol. Transl. Sci. 2015, 135, 39–74. [Google Scholar] [CrossRef]
- Imierska, M.; Kurianiuk, A.; Błachnio-Zabielska, A. The Influence of Physical Activity on the Bioactive Lipids Metabolism in Obesity-Induced Muscle Insulin Resistance. Biomolecules 2020, 10, 1665. [Google Scholar] [CrossRef] [PubMed]
- Duca, Y.; Calogero, A.E.; Cannarella, R.; Giacone, F.; Mongioi, L.M.; Condorelli, R.A.; La Vignera, S. Erectile dysfunction, physical activity and physical exercise: Recommendations for clinical practice. Andrologia 2019, 51, e13264. [Google Scholar] [CrossRef]
- Muscella, A.; Stefàno, E.; Marsigliante, S. The effects of exercise training on lipid metabolism and coronary heart disease. Am. J. Physiol. Heart Circ. Physiol. 2020, 319, H76–H88. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.T.; Zheng, J.; Peng, H.W.; Cai, X.L.; Pan, X.T.; Li, H.Q.; Hong, Q.Z.; Peng, X.E. Physical activity intervention for non-diabetic patients with non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. BMC Gastroenterol. 2020, 20, 66. [Google Scholar] [CrossRef]
- Song, Y.S.; Lee, H.J.; Park, I.H.; Lim, I.S.; Ku, J.H.; Kim, S.U. Human neural crest stem cells transplanted in rat penile corpus cavernosum to repair erectile dysfunction. BJU Int. 2008, 102, 220–224. [Google Scholar] [CrossRef]
- Achilleos, A.; Trainor, P.A. Neural crest stem cells: Discovery, properties and potential for therapy. Cell Res. 2012, 22, 288–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Demour, S.; Adwan, S.; Jafar, H.; Rahmeh, R.; Alhawari, H.; Awidi, A. Safety and Efficacy of 2 Intracavernous Injections of Allogeneic Wharton’s Jelly-Derived Mesenchymal Stem Cells in Diabetic Patients with Erectile Dysfunction: Phase 1/2 Clinical Trial. Urol. Int. 2021. ahead of print. [Google Scholar] [CrossRef]
- You, D.; Jang, M.J.; Song, G.; Shin, H.C.; Suh, N.; Kim, Y.M.; Ahn, T.Y.; Kim, C.S. Safety of autologous bone marrow-derived mesenchymal stem cells in erectile dysfunction: An open-label phase 1 clinical trial. Cytotherapy 2021, 23, 931–938. [Google Scholar] [CrossRef]
- Towe, M.; Peta, A.; Saltzman, R.G.; Balaji, N.; Chu, K.; Ramasamy, R. The use of combination regenerative therapies for erectile dysfunction: Rationale and current status. Int. J. Impot. Res. 2021, 12, 1–4. [Google Scholar] [CrossRef]
- Pajarinen, J.; Lin, T.; Gibon, E.; Kohno, Y.; Maruyama, M.; Nathan, K.; Lu, L.; Yao, Z.; Goodman, S.B. Mesenchymal stem cell-macrophage crosstalk and bone healing. Biomaterials 2019, 196, 80–89. [Google Scholar] [CrossRef]
- Chazaud, B. Inflammation and Skeletal Muscle Regeneration: Leave It to the Macrophages! Trends Immunol. 2020, 41, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.L.; Gomoll, A.H.; Lattermann, C.; Hernandez, A.J.; Bueno, D.F.; Amano, M.T. Macrophage: A Potential Target on Cartilage Regeneration. Front Immunol. 2020, 11, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokce, A.; Peak, T.C.; Abdel-Mageed, A.B.; Hellstrom, W.J. Adipose Tissue-Derived Stem Cells for the Treatment of Erectile Dysfunction. Curr. Urol. Rep. 2016, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Chen, W.; Zhang, C.; Xie, Y.; Gao, Y.; Deng, C.; Sun, X.; Liu, G.; Deng, C. Combined Transplantation of Adipose Tissue-Derived Stem Cells and Endothelial Progenitor Cells Improve Diabetic Erectile Dysfunction in a Rat Model. Stem Cells Int. 2020, 3, 2154053. [Google Scholar] [CrossRef] [PubMed]
- Masuku, N.P.; Unuofin, J.O.; Lebelo, S.L. Advances in Nanoparticle Delivery System for Erectile Dysfunction: An Updated Review. Sex. Med. 2021, 9, 100420. [Google Scholar] [CrossRef]
- Protogerou, V.; Chrysikos, D.; Karampelias, V.; Spanidis, Y.; Sara, E.B.; Troupis, T. Erectile Dysfunction Treatment Using Stem Cells: A Review. Medicines 2021, 8, 2. [Google Scholar] [CrossRef]
- Zhao, H.; Shang, Q.; Pan, Z.; Bai, Y.; Li, Z.; Zhang, H.; Zhang, Q.; Guo, C.; Zhang, L.; Wang, Q. Exosomes From Adipose-Derived Stem Cells Attenuate Adipose Inflammation and Obesity Through Polarizing M2 Macrophages and Beiging in White Adipose Tissue. Diabetes 2018, 67, 235–247. [Google Scholar] [CrossRef] [Green Version]
- Czapla, J.; Cichoń, T.; Pilny, E.; Jarosz-Biej, M.; Matuszczak, S.; Drzyzga, A.; Krakowczyk, Ł.; Smolarczyk, R. Adipose tissue-derived stromal cells stimulated macrophages-endothelial cells interactions promote effective ischemic muscle neovascularization. Eur. J. Pharmacol. 2020, 15, 883. [Google Scholar] [CrossRef]
- Albersen, M.; Berkers, J.; Dekoninck, P.; Deprest, J.; Lue, T.F.; Hedlund, P.; Lin, C.S.; Bivalacqua, T.J.; Van Poppel, H.; De Ridder, D.; et al. Expression of a Distinct Set of Chemokine Receptors in Adipose Tissue-Derived Stem Cells is Responsible for In Vitro Migration Toward Chemokines Appearing in the Major Pelvic Ganglion Following Cavernous Nerve Injury. Sex. Med. 2013, 1, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.J.; Liu, L.P.; Gu, X.L.; Wang, M.; Liu, L.M. Implantation of adipose-derived stem cells cures the optic nerve injury on rats through inhibiting the expression of inflammation factors in the TLR4 signaling pathway. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1196–1202. [Google Scholar] [CrossRef]
- Kwon, M.J.; Shin, H.Y.; Cui, Y.; Kim, H.; Thi, A.H.; Choi, J.Y.; Kim, E.Y.; Hwang, D.H.; Kim, B.G. CCL2 Mediates Neuron-Macrophage Interactions to Drive Proregenerative Macrophage Activation Following Preconditioning Injury. J. Neurosci. 2015, 35, 15934–15947. [Google Scholar] [CrossRef]
- Nagata, S. Xenopus laevis macrophage-like cells produce XCL-1, an intelectin family serum lectin that recognizes bacteria. Immunol. Cell Biol. 2018, 96, 872–878. [Google Scholar] [CrossRef]
- Helmke, A.; Nordlohne, J.; Balzer, M.S.; Dong, L.; Rong, S.; Hiss, M.; Shushakova, N.; Haller, H.; von Vietinghoff, S. CX3CL1-CX3CR1 interaction mediates macrophage-mesothelial cross talk and promotes peritoneal fibrosis. Kidney Int. 2019, 95, 1405–1417. [Google Scholar] [CrossRef]
- Sica, A.; Mantovani, A. Macrophage plasticity and polarization: In vivo veritas. J. Clin. Investig. 2012, 122, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Kroner, A.; Greenhalgh, A.D.; Zarruk, J.G.; Passos Dos Santos, R.; Gaestel, M.; David, S. TNF and increased intracellular iron alter macrophage polarization to a detrimental M1 phenotype in the injured spinal cord. Neuron 2014, 83, 1098–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, J.F.; Huang, X.N.; Han, X.Y.; Ouyang, X.; Fan, L.; Zhao, X.; Chen, Z.H.; Wei, H.B. Combined Transplantation of Mesenchymal Stem Cells and Endothelial Progenitor Cells Restores Cavernous Nerve Injury-Related Erectile Dysfunction. J. Sex. Med. 2018, 15, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, X.; Han, X.; Chen, Z.; Fang, J.; Huang, X.; Wei, H. MSC-derived exosomes ameliorate erectile dysfunction by alleviation of corpus cavernosum smooth muscle apoptosis in a rat model of cavernous nerve injury. Stem. Cell. Res. Ther. 2018, 9, 246. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Han, X.; Ouyang, X.; Fang, J.; Huang, X.; Wei, H. Transplantation of induced pluripotent stem cell-derived mesenchymal stem cells improved erectile dysfunction induced by cavernous nerve injury. Theranostics 2019, 9, 6354–6368. [Google Scholar] [CrossRef]
- Wu, J.; Chen, Z.; Zhong, F.; Yang, W.; Ouyang, X.; Ma, X.; Zheng, S.; Wei, H. Transplantation of Human Gingiva-Derived Mesenchymal Stem Cells Ameliorates Neurotic Erectile Dysfunction in a Rat Model. Front. Bioeng. Biotechnol. 2021, 21, 630076. [Google Scholar] [CrossRef]
- Ichim, T.E.; Zhong, Z.; Mikirova, N.A.; Jackson, J.A.; Hunninghake, R.; Mansilla, E.; Marín, G.; Núñez, L.; Patel, A.N.; Angle, N.; et al. Circulating endothelial progenitor cells and erectile dysfunction: Possibility of nutritional intervention? Panminerva Med. 2010, 52, 75–80. [Google Scholar]
- Choi, S.S.; Lee, S.R.; Woo, Y.K.; Lee, H.J. Stem Cell Therapies for Neurogenic Erectile Dysfunction. Austin J. Urol. 2014, 1, 1015. [Google Scholar]
- Toward, T.J.; Smith, N.; Broadley, K.J. Effect of phosphodiesterase-5 inhibitor, sildenafil (Viagra), in animal models of airways disease. Am. J. Respir. Crit. Care Med. 2004, 169, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Muimo, R. Classical activation of macrophages and vardenafil. Clin. Sci. 2017, 131, 1141–1145. [Google Scholar] [CrossRef] [Green Version]
- Noel, S.; Panin, N.; Beka, M.; Dhooghe, B.; Huaux, F.; Leal, T. Vardenafil reduces macrophage pro-inflammatory overresponses in cystic fibrosis through PDE5- and CFTR-dependent mechanisms. Clin. Sci. 2017, 131, 1107–1121. [Google Scholar] [CrossRef]
- Bergeron, C.; Cantin, A.M. Cystic Fibrosis: Pathophysiology of Lung Disease. Semin Respir Crit Care Med. 2019, 40, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Delfino, D.; Mori, G.; Rivetti, C.; Grigoletto, A.; Bizzotto, G.; Cavozzi, C.; Malatesta, M.; Cavazzini, D.; Pasut, G.; Percudani, R. Actin-Resistant DNase1L2 as a Potential Therapeutics for CF Lung Disease. Biomolecules 2021, 11, 410. [Google Scholar] [CrossRef]
- Shastri, M.D.; Allam, V.S.R.R.; Shukla, S.D.; Jha, N.K.; Paudel, K.R.; Peterson, G.M.; Patel, R.P.; Hansbro, P.M.; Chellappan, D.K.; Dua, K. Interleukin-13: A pivotal target against influenza-induced exacerbation of chronic lung diseases. Life Sci. 2021, 2, 119871. [Google Scholar] [CrossRef] [PubMed]
- Dormer, R.L.; Harris, C.M.; Clark, Z.; Pereira, M.M.; Doull, I.J.; Norez, C.; Becq, F.; McPherson, M.A. Sildenafil (Viagra) corrects DeltaF508-CFTR location in nasal epithelial cells from patients with cystic fibrosis. Thorax 2005, 60, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Dhooghe, B.; Noël, S.; Bouzin, C.; Behets-Wydemans, G.; Leal, T. Correction of chloride transport and mislocalization of CFTR protein by vardenafil in the gastrointestinal tract of cystic fibrosis mice. PLoS ONE 2013, 8, e77314. [Google Scholar]
- Díaz-Lucena, D.; Gutierrez-Mecinas, M.; Moreno, B.; Martínez-Sánchez, J.L.; Pifarré, P.; García, A. Mechanisms Involved in the Remyelinating Effect of Sildenafil. J. Neuroimmune Pharmacol. 2018, 13, 6–23. [Google Scholar] [CrossRef] [Green Version]
- Bechara, A.; Casabé, A.; De Bonis, W.; Helien, A.; Bertolino, M.V. Recreational use of phosphodiesterase type 5 inhibitors by healthy young men. J. Sex. Med. 2010, 7, 3736–3742. [Google Scholar] [CrossRef] [PubMed]
- Yafi, F.A.; Jenkins, L.; Albersen, M.; Corona, G.; Isidori, A.M.; Goldfarb, S.; Maggi, M.; Nelson, C.J.; Parish, S.; Salonia, A.; et al. Erectile dysfunction. Nat. Rev. Dis. Primers 2016, 2, 16003. [Google Scholar] [CrossRef]
- Miyata, Y.; Mukae, Y.; Harada, J.; Matsuda, T.; Mitsunari, K.; Matsuo, T.; Ohba, K.; Sakai, H. Pathological and Pharmacological Roles of Mitochondrial Reactive Oxygen Species in Malignant Neoplasms: Therapies Involving Chemical Compounds, Natural Products, and Photosensitizers. Molecules 2020, 25, 5252. [Google Scholar] [CrossRef]
- Al-Dashti, Y.A.; Holt, R.R.; Keen, C.L.; Hackman, R.M. Date Palm Fruit (Phoenix dactylifera): Effects on Vascular Health and Future Research Directions. Int. J. Mol. Sci. 2021, 22, 4665. [Google Scholar] [CrossRef]
- Bucciantini, M.; Leri, M.; Nardiello, P.; Casamenti, F.; Stefani, M. Olive Polyphenols: Antioxidant and Anti-Inflammatory Properties. Antioxidants 2021, 10, 1044. [Google Scholar] [CrossRef] [PubMed]
- Sin, V.J.; Anand, G.S.; Koh, H.L. Botanical Medicine and Natural Products Used for Erectile Dysfunction. Sex. Med. Rev. 2020, 9, 568–592. [Google Scholar] [CrossRef] [PubMed]
- Muncey, W.; Sellke, N.; Kim, T.; Mishra, K.; Thirumavalavan, N.; Loeb, A. Alternative Treatment for Erectile Dysfunction: A Growing Arsenal in Men’s Health. Curr. Urol. Rep. 2021, 22, 11. [Google Scholar] [CrossRef]
- Azadzoi, K.M.; Schulman, R.N.; Aviram, M.; Siroky, M.B. Oxidative stress in arteriogenic erectile dysfunction: Prophylactic role of antioxidants. J. Urol. 2005, 174, 386–393. [Google Scholar] [CrossRef]
- Forest, C.P.; Padma-Nathan, H.; Liker, H.R. Efficacy and safety of pomegranate juice on improvement of erectile dysfunction in male patients with mild to moderate erectile dysfunction: A randomized, placebo-controlled, double-blind, crossover study. Int. J. Impot. Res. 2007, 19, 564–567. [Google Scholar] [CrossRef] [Green Version]
- Onal, E.; Yilmaz, D.; Kaya, E.; Bastaskın, T.; Bayatlı, N.; Gur, S. Pomegranate juice causes a partial improvement through lowering oxidative stress for erectile dysfunction in streptozotocin-diabetic rat. Int. J. Impot. Res. 2016, 28, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Gur, S.; Rezk, B.M.; Abd Elmageed, Z.Y.; Kadowitz, P.J.; Sikka, S.C.; Hellstrom, W.J.G. Characterisation of pomegranate juice effects on human corpus cavernosum. Andrologia 2017, 49, 8. [Google Scholar] [CrossRef]
- Nounou, M.I.; Eassa, H.A.; Helal, N.A.; AboulFotouh, K.; Mansoor, I.; Latz, I.K.; Zheng, C.; Eassa, H.A.; Mohamed, D.; Huynh, D.M.; et al. The safety, efficacy and pharmaceutical quality of male enhancement nutraceuticals bought online: Truth versus claim. J. Integr. Med. 2021, 19, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Milenkovic, U.; Ilg, M.; Cellek, S.; Albersen, M. What role do pharmaceuticals play in the treatment of Peyronie’s disease and is there a need for new emerging drugs? Exp. Opin. Emerg. Drugs 2019, 24, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milenkovic, U.; Ilg, M.M.; Cellek, S.; Albersen, M. Pathophysiology and Future Therapeutic Perspectives for Resolving Fibrosis in Peyronie’s Disease. Sex. Med. Rev. 2019, 7, 679–689. [Google Scholar] [CrossRef]
- Gonzalez-Cadavid, N.F.; Magee, T.R.; Ferrini, M.; Qian, A.; Vernet, D.; Rajfer, J. Gene expression in Peyronie’s disease. Int. J. Impot. Res. 2002, 14, 361–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yafi, F.A.; Hatzichristodoulou, G.; DeLay, K.J.; Hellstrom, W.J. Review of Management Options for Patients With Atypical Peyronie’s Disease. Sex. Med. Rev. 2017, 5, 211–221. [Google Scholar] [CrossRef]
- Sherer, B.A.; Godlewski, K.F.; Levine, L.A. Pharmacologic therapy for Peyronie’s disease: What should we prescribe? Expert Opin. Pharmacother. 2015, 16, 1299–1311. [Google Scholar] [CrossRef]
- Hellstrom, W.J.; Bivalacqua, T.J. Peyronie’s disease: Etiology, medical, and surgical therapy. J. Androl. 2000, 21, 347–354. [Google Scholar]
- Ziegelmann, M.J.; Bajic, P.; Levine, L.A. Peyronie’s disease: Contemporary evaluation and management. Int. J. Urol. 2020, 27, 504–516. [Google Scholar] [CrossRef]
- Gonzalez-Cadavid, N.F.; Rajfer, J. Mechanisms of Disease: New insights into the cellular and molecular pathology of Peyronie’s disease. Nat. Clin. Pract. Urol. 2005, 2, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Devine, C.J., Jr.; Somers, K.D.; Jordan, S.G.; Schlossberg, S.M. Proposal: Trauma as the cause of the Peyronie’s lesion. J. Urol. 1997, 157, 285–290. [Google Scholar] [CrossRef]
- Jarow, J.P.; Lowe, F.C. Penile trauma: An etiologic factor in Peyronie’s disease and erectile dysfunction. J. Urol. 1997, 158, 1388–1390. [Google Scholar] [CrossRef]
- Zhang, F.; Qin, F.; Yuan, J. Molecular Mechanisms and Current Pharmacotherapy of Peyronie’s Disease: A Review. Front. Pharmacol. 2021, 12, 643641. [Google Scholar] [CrossRef]
- Patel, D.P.; Christensen, M.B.; Hotaling, J.M.; Pastuszak, A.W. A review of inflammation and fibrosis: Implications for the pathogenesis of Peyronie’s disease. World J. Urol. 2020, 38, 253–261. [Google Scholar] [CrossRef]
- Ilg, M.M.; Mateus, M.; Stebbeds, W.J.; Milenkovic, U.; Christopher, N.; Muneer, A.; Albersen, M.; Ralph, D.J.; Cellek, S. Antifibrotic Synergy Between Phosphodiesterase Type 5 Inhibitors and Selective Oestrogen Receptor Modulators in Peyronie’s Disease Models. Eur. Urol. 2019, 75, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Antoniassi, T.; Júnior, F.N.F.; Spessoto, L.C.F.; Guerra, L.H.; Campos, S.S.; Taboga, S. Anti-fibrotic effect of mycophenolate mofetil on Peyronie’s disease experimentally induced with TGF-β. Int. J. Impot. Res. 2020, 32, 201–206. [Google Scholar] [CrossRef]
- Ryu, J.K.; Kim, W.J.; Choi, M.J.; Park, J.M.; Song, K.M.; Kwon, M.H.; Das, N.D.; Kwon, K.D.; Batbold, D.; Yin, G.N.; et al. Inhibition of histone deacetylase 2 mitigates profibrotic TGF-β1 responses in fibroblasts derived from Peyronie’s plaque. Asian J. Androl. 2013, 15, 640–645. [Google Scholar] [CrossRef] [Green Version]
- Wan, Z.H.; Li, G.H.; Guo, Y.L.; Li, W.Z.; Chen, L.; Zhang, Y.J. Amelioration of Cavernosal Fibrosis and Erectile Function by Lysyl Oxidase Inhibition in a Rat Model of Cavernous Nerve Injury. J. Sex. Med. 2018, 15, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Davila, H.H.; Ferrini, M.G.; Rajfer, J.; Gonzalez-Cadavid, N.F. Fibrin as an inducer of fibrosis in the tunica albuginea of the rat: A new animal model of Peyronie’s disease. BJU Int. 2003, 91, 830–838. [Google Scholar] [CrossRef] [Green Version]
- Haag, S.M.; Hauck, E.W.; Eickelberg, O.; Szardening-Kirchner, C.; Diemer, T.; Weidner, W. Investigation of the antifibrotic effect of IFN-gamma on fibroblasts in a cell culture model of Peyronie’s disease. Eur. Urol. 2008, 53, 425–430. [Google Scholar] [CrossRef]
- Szardening-Kirchner, C.; Konrad, L.; Hauck, E.W.; Haag, S.M.; Eickelberg, O.; Weidner, W. Upregulation of mRNA expression of MCP-1 by TGF-beta1 in fibroblast cells from Peyronie’s disease. World J. Urol. 2009, 27, 123–130. [Google Scholar] [CrossRef]
- Ferrini, M.G.; Rivera, S.; Moon, J.; Vernet, D.; Rajfer, J.; Gonzalez-Cadavid, N.F. The genetic inactivation of inducible nitric oxide synthase (iNOS) intensifies fibrosis and oxidative stress in the penile corpora cavernosa in type 1 diabetes. J. Sex. Med. 2010, 7, 3033–3044. [Google Scholar] [CrossRef]
- Mulhall, J.P.; Nicholson, B.; Pierpaoli, S.; Lubrano, T.; Shankey, T.V. Chromosomal instability is demonstrated by fibroblasts derived from the tunica of men with Peyronie’s disease. Int. J. Impot. Res. 2004, 16, 288–293. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, R.P.; Feil, G.; Bock, C.; Hoeltl, L.; Stenzl, A. Significant alterations of serum cytokine levels in patients with Peyronie’s disease. Int. Braz. J. Urol. 2008, 34, 457–466. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.H.; Ryu, Y.L.; Lee, H.S.; Lee, H.; Son, M.K.; Yan, H.H.; Hong, S.W.; Ryu, J.K.; Hong, S.; Suh, J.K.; et al. A novel PI3K inhibitor alleviates fibrotic responses in fibroblasts derived from Peyronie’s plaques. Int. J. Oncol. 2013, 42, 2001–2008. [Google Scholar] [CrossRef]
- Gelbard, M.K.; Rosenbloom, J. Fibroproliferative disorders and diabetes: Understanding the pathophysiologic relationship between Peyronie’s disease, Dupuytren disease and diabetes. Endocrinol. Diabetes Metab. 2020, 4, e00195. [Google Scholar] [CrossRef]
- Cocci, A.; Ralph, D.; Djinovic, R.; Hatzichristodoulou, G.; Morelli, G.; Salonia, A.; Capogrosso, P.; Romano, A.; Cito, G.; Di Maida, F.; et al. Surgical outcomes after collagenase Clostridium histolyticum failure in patients with Peyronie’s disease in a multicenter clinical study. Sci. Rep. 2021, 11, 166. [Google Scholar] [CrossRef] [PubMed]
- García-Gómez, B.; Aversa, A.; Alonso-Isa, M.; Parnham, A.; Serefoglu, E.C.; Corona, G.; Bettocchi, C.; Reisman, Y.; Romero-Otero, J. The Use of Penile Traction Devices for Peyronie’s Disease: Position Statements from the European Society for Sexual Medicine. Sex. Med. 2021, 9, 100387. [Google Scholar] [CrossRef] [PubMed]
- Li, W.J.; Bao, J.; Zheng, D.C.; Guo, J.; Xie, M.K.; Chen, H.Y.; Wang, Z. Treatments of Peyronie’s disease with Scutellaria baicalensis and surgery according to the disease course: A single-center retrospective study of 261 patients. Ann. Palliat. Med. 2021, 10, 2979–2989. [Google Scholar] [CrossRef] [PubMed]
- Ure, I.; Ozen, A. Intralesional low-dose methylprednisolone for the treatment of active phase Peyronie’s disease: A single-centre, preliminary prospective non-randomised study. Int. J. Clin. Pract. 2021, 75, e13754. [Google Scholar] [CrossRef] [PubMed]
- Mateus, M.; Ilg, M.M.; Stebbeds, W.J.; Christopher, N.; Muneer, A.; Ralph, D.J.; Cellek, S. Understanding the Role of Adenosine Receptors in the Myofibroblast Transformation in Peyronie’s Disease. J. Sex. Med. 2018, 15, 947–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Cause of ED | Pathological Roles | References |
|---|---|---|
| Vasculogenic | Endothelial injury and plaque instability due to endothelial dysfunction | [32,33] |
| Reactive oxygen species production and cytokine secretion | [8,35,36] | |
| Modulation of lipid metabolism (oxidization of low-density lipoprotein) | [8] | |
| Neurogenic | Modulation of cavernous nerve injury and nitrergic nerve apoptosis | [42,43] |
| Impairment of erectile tissue physiology | [42] | |
| Regulation of corporal smooth muscle function | [43] | |
| Obesity-related | Increase in TNF-α expression in the corpus cavernosum | [55,56] |
| Stimulation of inflammatory status in penile tissues | [56] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyata, Y.; Matsuo, T.; Nakamura, Y.; Mitsunari, K.; Ohba, K.; Sakai, H. Pathological Significance of Macrophages in Erectile Dysfunction Including Peyronie’s Disease. Biomedicines 2021, 9, 1658. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9111658
Miyata Y, Matsuo T, Nakamura Y, Mitsunari K, Ohba K, Sakai H. Pathological Significance of Macrophages in Erectile Dysfunction Including Peyronie’s Disease. Biomedicines. 2021; 9(11):1658. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9111658
Chicago/Turabian StyleMiyata, Yasuyoshi, Tomohiro Matsuo, Yuichiro Nakamura, Kensuke Mitsunari, Kojiro Ohba, and Hideki Sakai. 2021. "Pathological Significance of Macrophages in Erectile Dysfunction Including Peyronie’s Disease" Biomedicines 9, no. 11: 1658. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9111658