
Evaluation of Pulp Repair after BiodentineTM Full Pulpotomy in a Rat Molar Model of Pulpitis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Induction of Pulpitis
2.3. Pulpotomy Procedure
2.4. Enzyme-Linked Immunosorbent Assay
2.5. Sample Preparation for Histology
2.6. Histological Analysis
2.7. Immunohistochemistry
2.8. Micro-CT Follow-Up
2.9. Statistical Analysis
3. Results
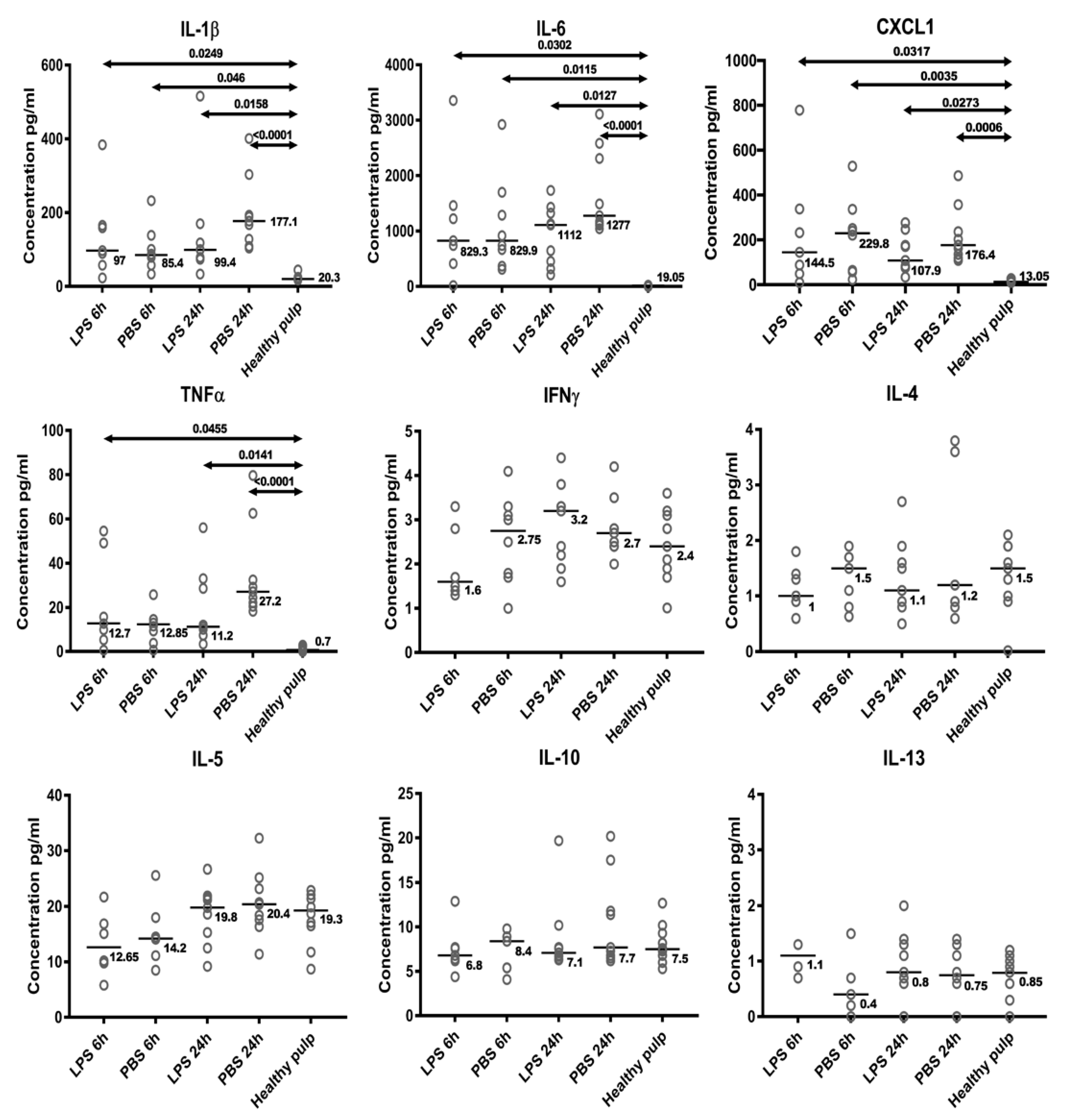
3.1. Cytokine Profile in the Inflamed Coronal Pulp Chamber
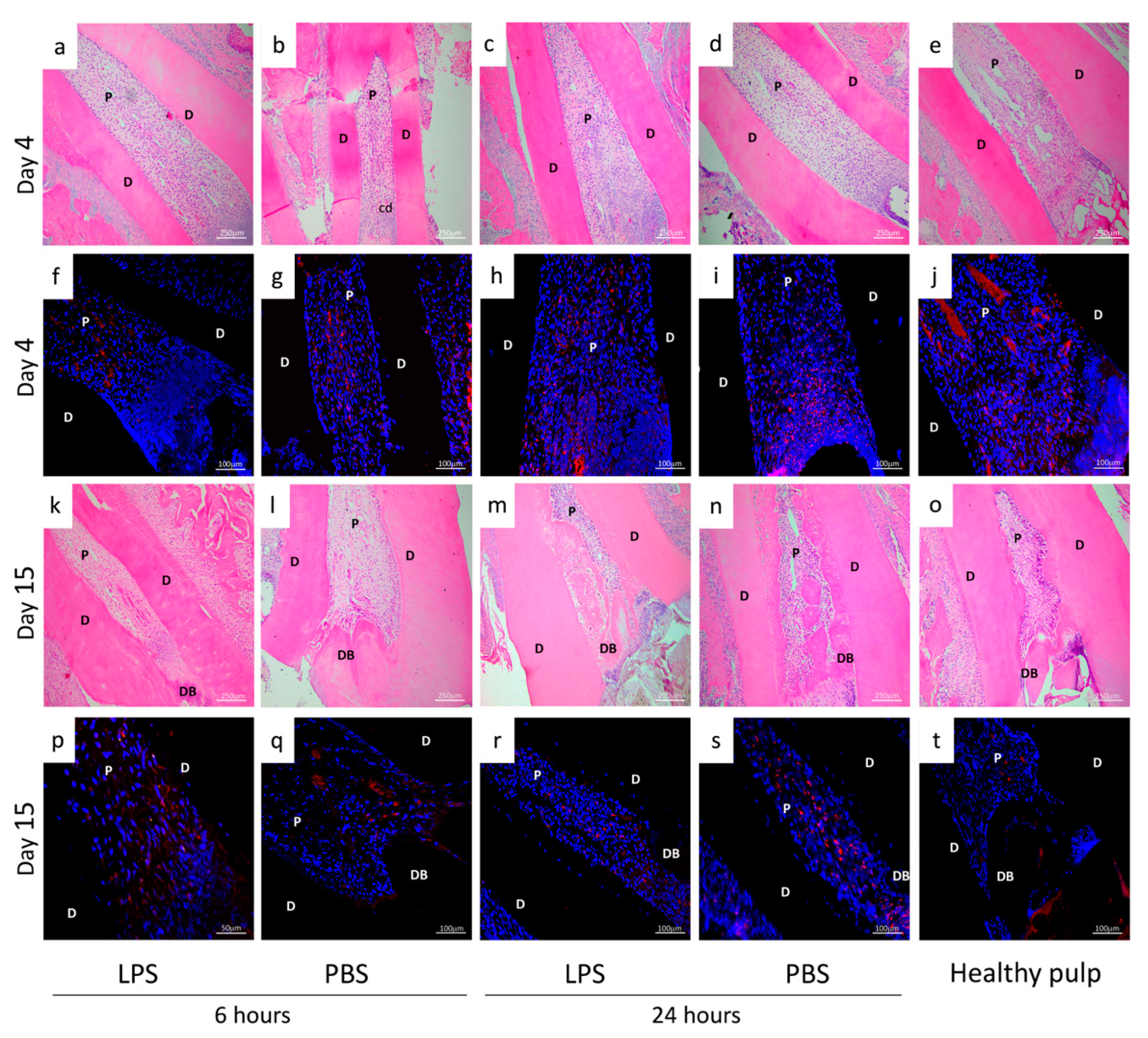
3.2. Residual Pulp Inflammation after Pulpotomy at D4 and D15

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score |
|---|
Inflammatory reaction
|
| Inflammatory Condition Groups | Product Injected | Inflammatory Reaction | General State of the Pulp | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | ||
| Control | 25% | 50% | 25% | 0% | 50% | 25% | 25% | 0% | |
| 6 h | PBS | 42.85% * | 28.57% * | 0% | 28.57% | 28.57% * | 57.14% * | 14.28% * | 0% |
| pulpitis induction | LPS | 33.33% * | 33.33% * | 33.33% | 0% | 33.33% * | 66.66% * | 16.66% * | 0% |
| 24 h | PBS | 27.27% | 45.45% | 27% | 0% | 18.18% | 72.72% | 9.09% | 0% |
| pulpitis induction | LPS | 22.22% | 55.55% | 22.22% | 0% | 22.22% | 77.77% | 0% | 0% |
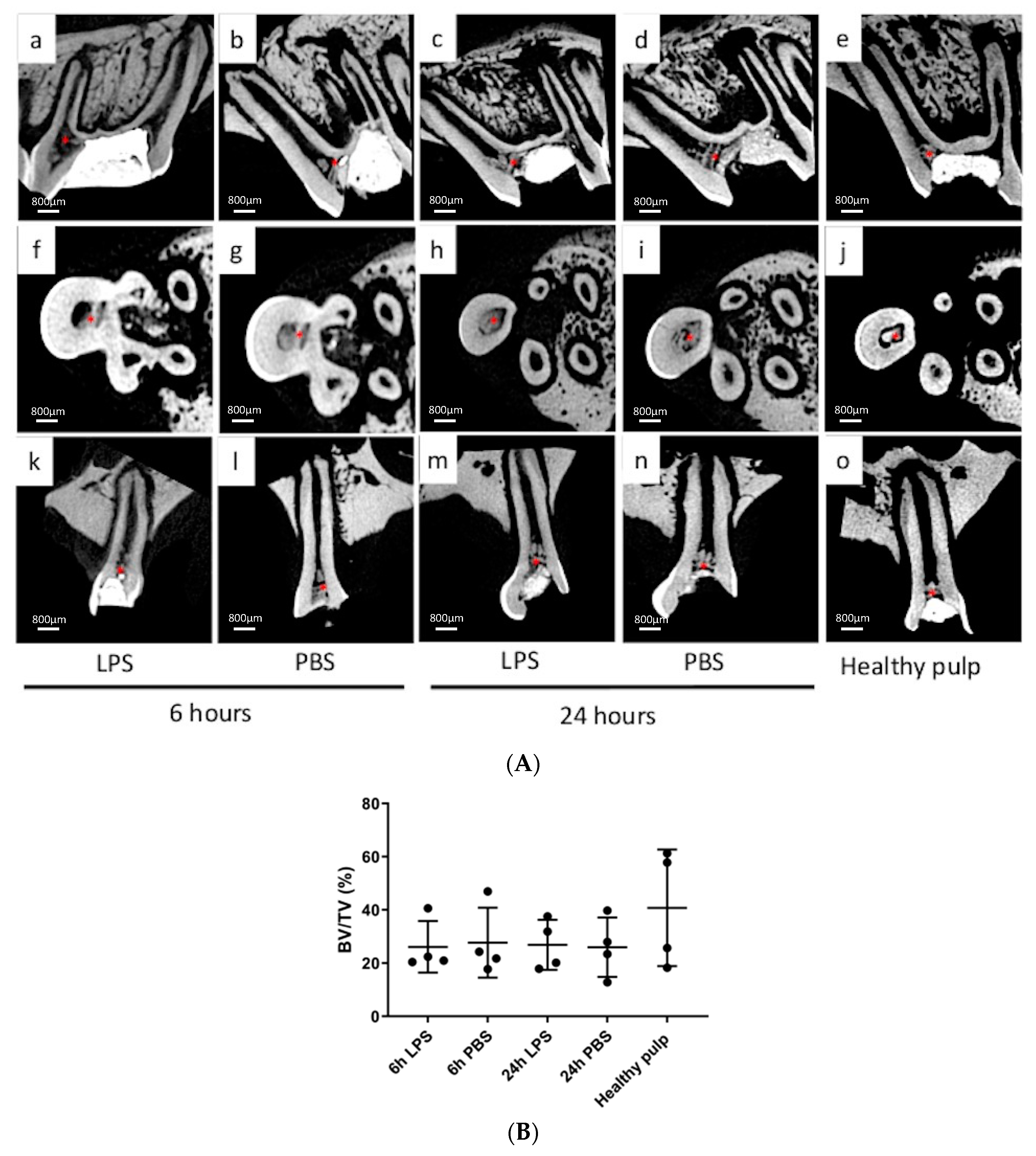
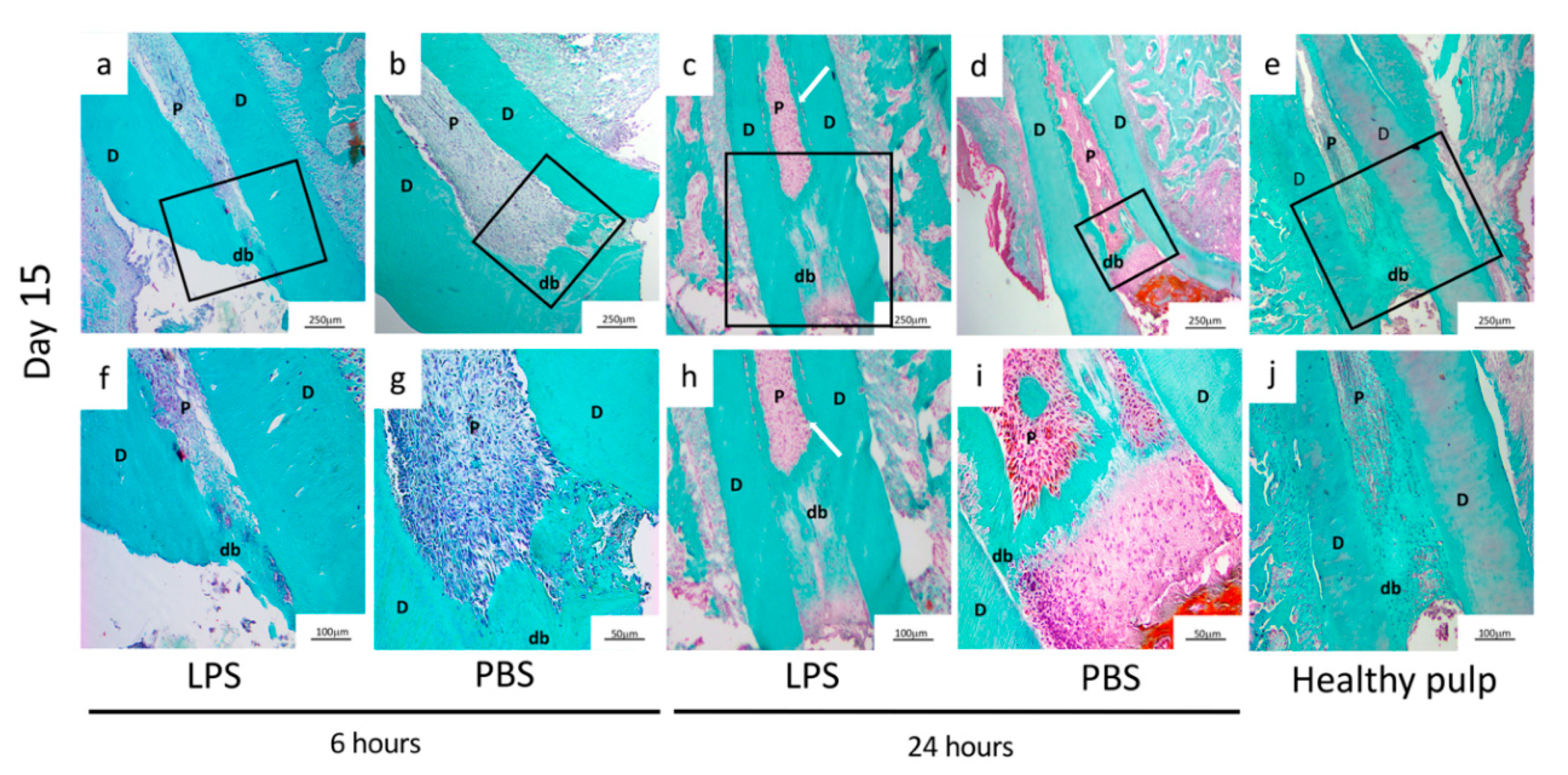
3.3. Characterization of the Mineralized Bridge at D15
| Score | |
|---|---|
| Hard Tissue | |
| 1 | Present |
| 4 | Absent |
| Continuity | |
| 1 | Complete |
| 2 | Little contact of the capping material with dental pulp |
| 3 | Only lateral deposition of hard tissue on radicular pulp |
| 4 | No hard tissue bridge or lateral deposition of hard tissue |
| Morphology | |
| 1 | Dentin or dentin associated with irregular hard tissue |
| 2 | Only irregular hard tissue deposition |
| 3 | Only a thin layer of hard tissue deposition |
| 4 | No hard tissue deposition |
| Localization | |
| 1 | Close to the exposed area without invading the radicular space |
| 2 | Bridge invading pulp space up to 50% of radicular space |
| 3 | Bridge invading more than 50% of radicular space |
| 4 | No bridge or only hard tissue deposition on walls of the exposed cavity |
| Inflammatory Condition Groups | Product Injected | Hard Tissue | Continuity | Morphology | Localization | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | ||
| Control | 75% | 25% | 50% | 0% | 25% | 25% | 0% | 25% | 50% | 25% | 25% | 50% | 0% | 25% | |
| 6 h pulpitis | PBS | 71.40% | 28.60% | 14.28% | 14.28% | 42.85% | 28.57% | 0% * | 42.85% * | 28.57% | 28.57% | 14.28% * | 28.57% | 28.57% * | 28.57% |
| induction | LPS | 83.33% | 16.60% | 33.33% | 33.33% | 16.66% | 16.66% | 16.66% * | 33.33% * | 16.66% | 16.66% | 16.66% * | 50.0% | 0% * | 16.66% |
| 24 h pulpitis | PBS | 73% | 27% | 18.18% | 9.09% | 45.45% | 27.27% | 27.27% | 18.18% | 27% | 27% | 0% | 9.09% | 63.63% | 27.27% |
| induction | LPS | 89% | 11.11% | 55.55% | 0% | 33.33% | 11.11% | 33.33% | 22.22% | 33.33% | 11.11% | 0% | 33.33% | 55.55% | 11.11% |
3.4. Characterization of Cells Involved in DP Repair
4. Discussion
4.1. Development of a New Model of Pulp Inflammation in Rats
4.2. BiodentineTM Induces Pulp-Dentin Complex Regeneration in Inflammatory Conditions
4.3. A new model of Pulp Inflammation Suitable for Pulp Repair Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gaudin, A.; Renard, E.; Hill, M.; Bouchet-Delbos, L.; Bienvenu-Louvet, G.; Farges, J.C.; Cuturi, M.C.; Alliot-Licht, B. Phenotypic analysis of immunocompetent cells in healthy human dental pulp. J. Endod. 2015, 41, 621–627. [Google Scholar] [CrossRef]
- Izumi, T.; Kobayashi, I.; Okamura, K.; Sakai, H. Immunohistochemical study on the immunocompetent cells of the pulp in human non-carious and carious teeth. Arch. Oral. Biol. 1995, 40, 609–614. [Google Scholar] [CrossRef]
- Renard, E.; Gaudin, A.; Bienvenu, G.; Amiaud, J.; Farges, J.C.; Cuturi, M.C.; Moreau, A.; Alliot-Licht, B. Immune Cells and Molecular Networks in Experimentally Induced Pulpitis. J. Dent. Res. 2016, 95, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.R.; Takahashi, Y.; Graham, L.W.; Simon, S.; Imazato, S.; Smith, A.J. Inflammation-regeneration interplay in the dentine-pulp complex. J. Dent. 2010, 38, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.D.; Nedjai, B.; Hurst, T.; Pennington, D.J. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochim. Biophys. Acta 2014, 1843, 2563–2582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, H.F.; Cooper, P.R.; Smith, A.J. Dissecting dentine-pulp injury and wound healing responses: Consequences for regenerative endodontics. Int. Endod. J. 2019, 52, 261–266. [Google Scholar] [CrossRef] [Green Version]
- Cooper, P.R.; Holder, M.J.; Smith, A.J. Inflammation and regeneration in the dentin-pulp complex: A double-edged sword. J. Endod. 2014, 40, S46–S51. [Google Scholar] [CrossRef]
- Wolters, W.J.; Duncan, H.F.; Tomson, P.L.; Karim, I.E.; McKenna, G.; Dorri, M.; Stangvaltaite, L.; van der Sluis, L.W.M. Minimally invasive endodontics: A new diagnostic system for assessing pulpitis and subsequent treatment needs. Int. Endod. J. 2017, 50, 825–829. [Google Scholar] [CrossRef]
- Mejare, I.A.; Axelsson, S.; Davidson, T.; Frisk, F.; Hakeberg, M.; Kvist, T.; Norlund, A.; Petersson, A.; Portenier, I.; Sandberg, H.; et al. Diagnosis of the condition of the dental pulp: A systematic review. Int. Endod. J. 2012, 45, 597–613. [Google Scholar] [CrossRef]
- Elsalhy, M.; Azizieh, F.; Raghupathy, R. Cytokines as diagnostic markers of pulpal inflammation. Int. Endod. J. 2013, 46, 573–580. [Google Scholar] [CrossRef]
- Rechenberg, D.K.; Galicia, J.C.; Peters, O.A. Biological Markers for Pulpal Inflammation: A Systematic Review. PLoS ONE 2016, 11, e0167289. [Google Scholar] [CrossRef] [Green Version]
- Zehnder, M.; Wegehaupt, F.J.; Attin, T. A first study on the usefulness of matrix metalloproteinase 9 from dentinal fluid to indicate pulp inflammation. J. Endod. 2011, 37, 17–20. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef]
- Arias-Moliz, M.T.; Farrugia, C.; Lung, C.Y.K.; Wismayer, P.S.; Camilleri, J. Antimicrobial and biological activity of leachate from light curable pulp capping materials. J. Dent. 2017, 64, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ballal, N.V.; Shavi, G.V.; Kumar, R.; Kundabala, M.; Bhat, K.S. In vitro sustained release of calcium ions and pH maintenance from different vehicles containing calcium hydroxide. J. Endod. 2010, 36, 862–866. [Google Scholar] [CrossRef] [PubMed]
- Pentek, A.; Paszty, K.; Apati, A. Analysis of Intracellular Calcium Signaling in Human Embryonic Stem Cells. Methods Mol. Biol. 2016, 1307, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Petrou, T.; Olsen, H.L.; Thrasivoulou, C.; Masters, J.R.; Ashmore, J.F.; Ahmed, A. Intracellular Calcium Mobilization in Response to Ion Channel Regulators via a Calcium-Induced Calcium Release Mechanism. J. Pharmacol. Exp. Ther. 2017, 360, 378–387. [Google Scholar] [CrossRef]
- Nam, O.H.; Lee, H.S.; Kim, J.H.; Chae, Y.K.; Hong, S.J.; Kang, S.W.; Lee, H.S.; Choi, S.C.; Kim, Y. Differential Gene Expression Changes in Human Primary Dental Pulp Cells Treated with Biodentine and TheraCal LC Compared to MTA. Biomedicines 2020, 8, 445. [Google Scholar] [CrossRef] [PubMed]
- Rathinam, E.; Govindarajan, S.; Rajasekharan, S.; Declercq, H.; Elewaut, D.; De Coster, P.; Martens, L.; Leybaert, L. The calcium dynamics of human dental pulp stem cells stimulated with tricalcium silicate-based cements determine their differentiation and mineralization outcome. Sci. Rep. 2021, 11, 645. [Google Scholar] [CrossRef] [PubMed]
- Bjorndal, L.; Simon, S.; Tomson, P.L.; Duncan, H.F. Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 949–973. [Google Scholar] [CrossRef]
- Kang, C.M.; Sun, Y.; Song, J.S.; Pang, N.S.; Roh, B.D.; Lee, C.Y.; Shin, Y. A randomized controlled trial of various MTA materials for partial pulpotomy in permanent teeth. J. Dent. 2017, 60, 8–13. [Google Scholar] [CrossRef]
- Kundzina, R.; Stangvaltaite, L.; Eriksen, H.M.; Kerosuo, E. Capping carious exposures in adults: A randomized controlled trial investigating mineral trioxide aggregate versus calcium hydroxide. Int. Endod. J. 2017, 50, 924–932. [Google Scholar] [CrossRef]
- Gala-Garcia, A.; Carneiro, M.B.; Silva, G.A.; Ferreira, L.S.; Vieira, L.Q.; Marques, M.M.; Sinisterra, R.D.; Cortes, M.E. In vitro and in vivo evaluation of the biocompatibility of a calcium phosphate/poly(lactic-co-glycolic acid) composite. J. Mater. Sci. Mater. Med. 2012, 23, 1785–1796. [Google Scholar] [CrossRef]
- Liu, S.; Wang, S.; Dong, Y. Evaluation of a bioceramic as a pulp capping agent in vitro and in vivo. J. Endod. 2015, 41, 652–657. [Google Scholar] [CrossRef]
- Ohkura, N.; Edanami, N.; Takeuchi, R.; Tohma, A.; Ohkura, M.; Yoshiba, N.; Yoshiba, K.; Ida-Yonemochi, H.; Ohshima, H.; Okiji, T.; et al. Effects of pulpotomy using mineral trioxide aggregate on prostaglandin transporter and receptors in rat molars. Sci. Rep. 2017, 7, 6870. [Google Scholar] [CrossRef] [Green Version]
- Kawashima, N.; Nakano-Kawanishi, H.; Suzuki, N.; Takagi, M.; Suda, H. Effect of NOS inhibitor on cytokine and COX2 expression in rat pulpitis. J. Dent. Res. 2005, 84, 762–767. [Google Scholar] [CrossRef]
- Kermeoglu, F.; Aksoy, U.; Sebai, A.; Savtekin, G.; Ozkayalar, H.; Sayiner, S.; Sehirli, A.O. Anti-Inflammatory Effects of Melatonin and 5-Methoxytryptophol on Lipopolysaccharide-Induced Acute Pulpitis in Rats. Biomed. Res. Int. 2021, 2021, 8884041. [Google Scholar] [CrossRef] [PubMed]
- Rupf, S.; Kannengiesser, S.; Merte, K.; Pfister, W.; Sigusch, B.; Eschrich, K. Comparison of profiles of key periodontal pathogens in periodontium and endodontium. Endod. Dent. Traumatol. 2000, 16, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Hoebe, K.; Janssen, E.; Beutler, B. The interface between innate and adaptive immunity. Nat. Immunol. 2004, 5, 971–974. [Google Scholar] [CrossRef]
- Mutoh, N.; Tani-Ishii, N.; Tsukinoki, K.; Chieda, K.; Watanabe, K. Expression of toll-like receptor 2 and 4 in dental pulp. J. Endod. 2007, 33, 1183–1186. [Google Scholar] [CrossRef] [PubMed]
- Aubeux, D.; Renard, E.; Pérez, F.; Tessier, S.; Geoffroy, V.; Gaudin, A. Review of Animal Models to Study Pulp Inflammation. Front. Dent. Med. 2021, 2, 21. [Google Scholar] [CrossRef]
- Chung, M.K.; Lee, J.; Duraes, G.; Ro, J.Y. Lipopolysaccharide-induced pulpitis up-regulates TRPV1 in trigeminal ganglia. J. Dent. Res. 2011, 90, 1103–1107. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.A.; Lim, S.S. T lymphocyte subpopulations and interleukin-2, interferon-gamma, and interleukin-4 in rat pulpitis experimentally induced by specific bacteria. J. Endod. 2002, 28, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Qiao, W.; Huang, Y.; Bian, Z.; Sun, X.; Wang, X.; Gao, Q.; Peng, Y.; Meng, L. Lipopolysaccharide-induced DNA damage response activates nuclear factor kappaB signalling pathway via GATA4 in dental pulp cells. Int. Endod. J. 2019, 52, 1704–1715. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Wang, S.C.; Tong, J.; Hu, Y.; Zhang, Y.Q.; Yu, Q. Activation and dynamic expression of Notch signalling in dental pulp cells after injury in vitro and in vivo. Int. Endod. J. 2016, 49, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Maeda, M.; Yamakita, J.; Nakamura, Y. Effects of zinc oxide-eugenol on leucocyte number and lipoxygenase products in artificially inflamed rat dental pulp. Arch. Oral. Biol. 1990, 35, 87–93. [Google Scholar] [CrossRef]
- Renard, E.; Amiaud, J.; Delbos, L.; Charrier, C.; Montembault, A.; Ducret, M.; Farges, J.C.; David, L.; Alliot-Licht, B.; Gaudin, A. Dental pulp inflammatory/immune response to a chitosan-enriched fibrin hydrogel in the pulpotomised rat incisor. Eur. Cell Mater. 2020, 40, 74–87. [Google Scholar] [CrossRef]
- Jontell, M.; Okiji, T.; Dahlgren, U.; Bergenholtz, G. Immune defense mechanisms of the dental pulp. Crit. Rev. Oral Biol. Med. 1998, 9, 179–200. [Google Scholar] [CrossRef] [Green Version]
- Kamal, A.M.; Okiji, T.; Kawashima, N.; Suda, H. Defense responses of dentin/pulp complex to experimentally induced caries in rat molars: An immunohistochemical study on kinetics of pulpal Ia antigen-expressing cells and macrophages. J. Endod. 1997, 23, 115–120. [Google Scholar] [CrossRef]
- Tran, X.V.; Salehi, H.; Truong, M.T.; Sandra, M.; Sadoine, J.; Jacquot, B.; Cuisinier, F.; Chaussain, C.; Boukpessi, T. Reparative Mineralized Tissue Characterization after Direct Pulp Capping with Calcium-Silicate-Based Cements. Materials 2019, 12, 2102. [Google Scholar] [CrossRef] [Green Version]
- Nowicka, A.; Lipski, M.; Parafiniuk, M.; Sporniak-Tutak, K.; Lichota, D.; Kosierkiewicz, A.; Kaczmarek, W.; Buczkowska-Radlinska, J. Response of human dental pulp capped with biodentine and mineral trioxide aggregate. J. Endod. 2013, 39, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Giraud, T.; Jeanneau, C.; Bergmann, M.; Laurent, P.; About, I. Tricalcium Silicate Capping Materials Modulate Pulp Healing and Inflammatory Activity In Vitro. J. Endod. 2018, 44, 1686–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cushley, S.; Duncan, H.F.; Lappin, M.J.; Tomson, P.L.; Lundy, F.T.; Cooper, P.; Clarke, M.; El Karim, I.A. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: A systematic review. J. Dent. 2019, 88, 103158. [Google Scholar] [CrossRef]
- Taha, N.A.; Abdelkhader, S.Z. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int. Endod. J. 2018, 51, 819–828. [Google Scholar] [CrossRef]
- Camilleri, J. Hydration characteristics of Biodentine and Theracal used as pulp capping materials. Dent. Mater. 2014, 30, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J.; Sorrentino, F.; Damidot, D. Investigation of the hydration and bioactivity of radiopacified tricalcium silicate cement, Biodentine and MTA Angelus. Dent. Mater. 2013, 29, 580–593. [Google Scholar] [CrossRef] [PubMed]
- Tecles, O.; Laurent, P.; Aubut, V.; About, I. Human tooth culture: A study model for reparative dentinogenesis and direct pulp capping materials biocompatibility. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 85, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Tran, X.V.; Gorin, C.; Willig, C.; Baroukh, B.; Pellat, B.; Decup, F.; Opsahl Vital, S.; Chaussain, C.; Boukpessi, T. Effect of a calcium-silicate-based restorative cement on pulp repair. J. Dent. Res. 2012, 91, 1166–1171. [Google Scholar] [CrossRef]
- Schroder, U. Effects of calcium hydroxide-containing pulp-capping agents on pulp cell migration, proliferation, and differentiation. J. Dent. Res. 1985, 64, 541–548. [Google Scholar] [CrossRef]
- Torabinejad, M.; Hong, C.U.; Pitt Ford, T.R.; Kettering, J.D. Antibacterial effects of some root end filling materials. J. Endod. 1995, 21, 403–406. [Google Scholar] [CrossRef]
- An, S.; Gao, Y.; Ling, J.; Wei, X.; Xiao, Y. Calcium ions promote osteogenic differentiation and mineralization of human dental pulp cells: Implications for pulp capping materials. J. Mater. Sci. Mater. Med. 2012, 23, 789–795. [Google Scholar] [CrossRef]
- Camilleri, J.; Laurent, P.; About, I. Hydration of Biodentine, Theracal LC, and a prototype tricalcium silicate-based dentin replacement material after pulp capping in entire tooth cultures. J. Endod. 2014, 40, 1846–1854. [Google Scholar] [CrossRef]
- Dominguez, M.S.; Witherspoon, D.E.; Gutmann, J.L.; Opperman, L.A. Histological and scanning electron microscopy assessment of various vital pulp-therapy materials. J. Endod. 2003, 29, 324–333. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Goncalves, L.S.; Rocas, I.N.; Siqueira, J.F., Jr. Histobacteriologic Conditions of the Apical Root Canal System and Periapical Tissues in Teeth Associated with Sinus Tracts. J. Endod. 2018, 44, 405–413. [Google Scholar] [CrossRef]
- D’Souza, R.N.; Bachman, T.; Baumgardner, K.R.; Butler, W.T.; Litz, M. Characterization of cellular responses involved in reparative dentinogenesis in rat molars. J. Dent. Res. 1995, 74, 702–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couve, E. Ultrastructural changes during the life cycle of human odontoblasts. Arch. Oral Biol. 1986, 31, 643–651. [Google Scholar] [CrossRef]
- Vijaykumar, A.; Dyrkacz, P.; Vidovic-Zdrilic, I.; Maye, P.; Mina, M. Expression of BSP-GFPtpz Transgene during Osteogenesis and Reparative Dentinogenesis. J. Dent. Res. 2020, 99, 89–97. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minic, S.; Florimond, M.; Sadoine, J.; Valot-Salengro, A.; Chaussain, C.; Renard, E.; Boukpessi, T. Evaluation of Pulp Repair after BiodentineTM Full Pulpotomy in a Rat Molar Model of Pulpitis. Biomedicines 2021, 9, 784. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9070784
Minic S, Florimond M, Sadoine J, Valot-Salengro A, Chaussain C, Renard E, Boukpessi T. Evaluation of Pulp Repair after BiodentineTM Full Pulpotomy in a Rat Molar Model of Pulpitis. Biomedicines. 2021; 9(7):784. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9070784
Chicago/Turabian StyleMinic, Sandra, Marion Florimond, Jérémy Sadoine, Anne Valot-Salengro, Catherine Chaussain, Emmanuelle Renard, and Tchilalo Boukpessi. 2021. "Evaluation of Pulp Repair after BiodentineTM Full Pulpotomy in a Rat Molar Model of Pulpitis" Biomedicines 9, no. 7: 784. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9070784