
Endothelial Progenitor Cells: Relevant Players in the Vasculopathy and Lung Fibrosis Associated with the Presence of Interstitial Lung Disease in Systemic Sclerosis Patients

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. EPC Quantification by Flow Cytometry
2.3. Statistical Analyses
3. Results
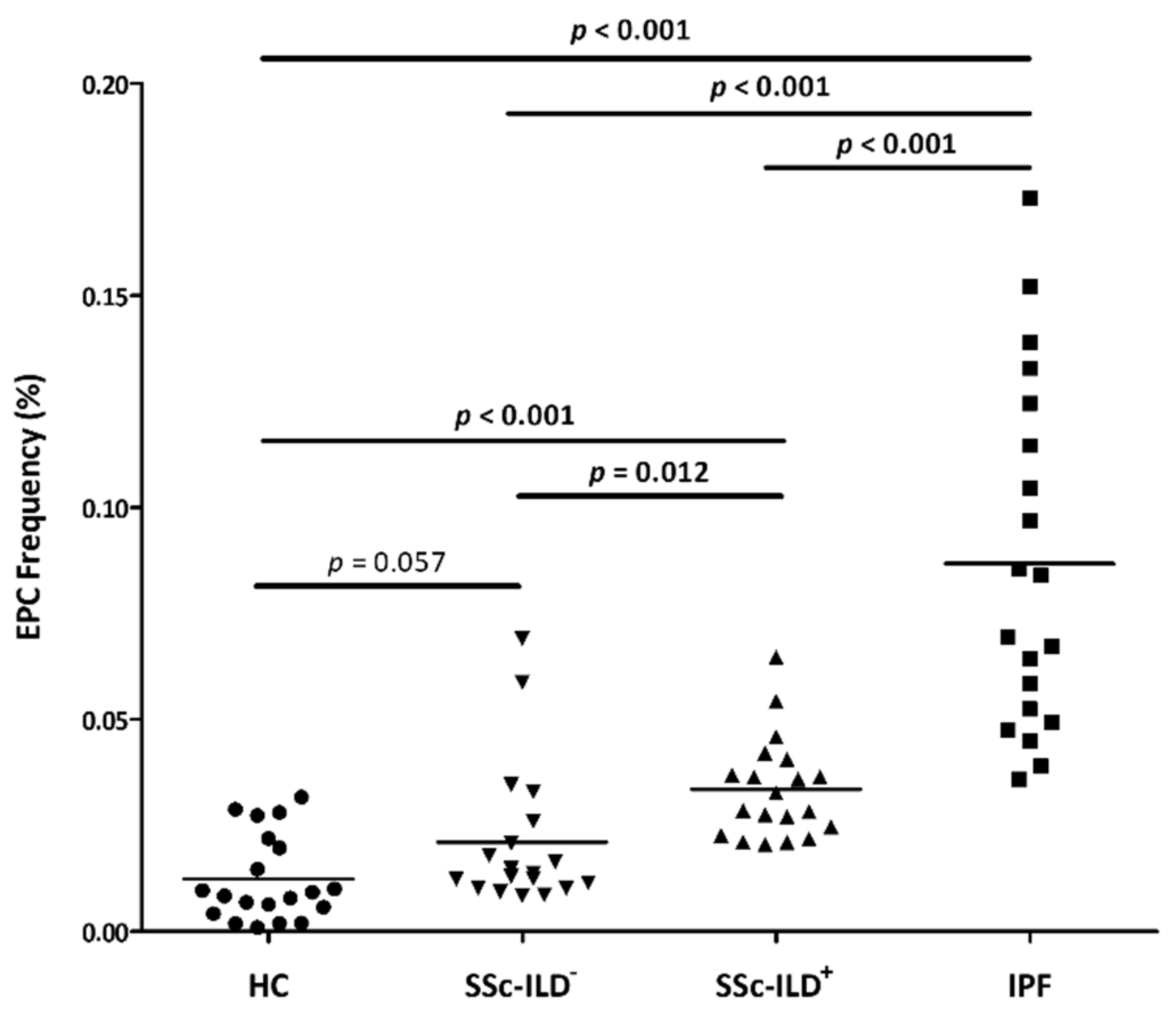
3.1. Differences in EPC Frequency between SSc-ILD+ Patients and the Comparative Groups
3.2. Relationship of EPC Frequency with Demographic and Clinical Features
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asahara, T.; Toyoaki, M.; Sullivan, A.; Silver, M.; Van der Zee, R.; Li, T.; Witzenbichler, B.; Schatteman, G.; Isner, J.M. Isolation of Putative Progenitor Endothelial Cells for Angiogenesis. Sci. New Ser. 1997, 275, 964–967. [Google Scholar] [CrossRef] [PubMed]
- Khakoo, A.Y.; Finkel, T. Endothelial Progenitor Cells. Annu. Rev. Med. 2005, 56, 79–101. [Google Scholar] [CrossRef]
- Fadini, G.P.; Baesso, I.; Albiero, M.; Sartore, S.; Agostini, C.; Avogaro, A. Technical notes on endothelial progenitor cells: Ways to escape from the knowledge plateau. Atherosclerosis 2008, 197, 496–503. [Google Scholar] [CrossRef]
- Ferrante, A.; Guggino, G.; Di Liberto, D.; Ciccia, F.; Cipriani, P.; Balistreri, C.R.; Sireci, G.; Giacomelli, R.; Triolo, G. Endothelial progenitor cells: Are they displaying a function in autoimmune disorders? Mech. Ageing Dev. 2016, 159, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Distler, H.W.; Beyer, C.; Schett, G.; Luscher, T.F.; Gay, S.; Distler, O. Endothelial Progenitor Cells Novel Players in the Pathogenesis of Rheumatic Diseases. Arthritis Rheum. 2009, 60, 3168–3179. [Google Scholar] [CrossRef] [Green Version]
- De Biasi, S.; Cerri, S.; Bianchini, E.; Gibellini, L.; Persiani, E.; Montanari, G.; Luppi, F.; Carbonelli, C.M.; Zucchi, L.; Bocchino, M.; et al. Levels of circulating endothelial cells are low in idiopathic pulmonary fibrosis and are further reduced by anti-fibrotic treatments. BMC Med. 2015, 13, 277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulito-Cueto, V.; Remuzgo-Martínez, S.; Genre, F.; Mora-Cuesta, V.M.; Iturbe-Fernández, D.; Fernández-Rozas, S.; Atienza-Mateo, B.; Lera-Gómez, L.; Alonso-Lecue, P.; Rodríguez-Carrio, J.; et al. Endothelial Progenitor Cells as a Potential Biomarker in Interstitial Lung Disease Associated with Rheumatoid Arthritis. J. Clin. Med. 2020, 9, 4098. [Google Scholar] [CrossRef]
- Arias-Nuñez, M.C.; Llorca, J.; Vazquez-Rodriguez, T.R.; Gomez-Acebo, I.; Miranda-Filloy, J.A.; Martin, J.; Gonzalez-Juanatey, C.; Gonzalez-Gay, M.A. Systemic sclerosis in northwestern Spain: A 19-year epidemiologic study. Medicine 2008, 87, 272–280. [Google Scholar] [CrossRef]
- Khanna, D.; Tashkin, D.P.; Denton, C.P.; Renzoni, E.A.; Desai, S.R.; Varga, J. Etiology, Risk Factors, and Biomarkers in Systemic Sclerosis with Interstitial Lung Disease. Am. J. Respir. Crit. Care Med. 2020, 201, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Distler, O.; Assassi, S.; Cottin, V.; Cutolo, M.; Danoff, S.K.; Denton, C.P.; Distler, J.H.W.; Hoffmann-Vold, A.; Johnson, S.R.; Ladner, U.M.; et al. Predictors of progression in systemic sclerosis patients with interstitial lung disease. Eur. Respir. J. 2020, 55, 1902026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottin, V.; Brown, K.K. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respir. Res. 2019, 20, 13. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Patel, N.M.; Volkmann, E.R. Interstitial Lung Disease in Systemic Sclerosis: Focus on Early Detection and Intervention. Open Access Rheumatol. 2019, 11, 283–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwana, M.; Okazaki, Y.; Yasuoka, H.; Kawakami, Y.; Ikeda, Y. Defective vasculogenesis in systemic sclerosis. Lancet 2004, 364, 603–610. [Google Scholar] [CrossRef]
- Allanore, Y.; Batteux, F.; Avouac, J.; Assous, N.; Weill, B.; Kahan, A. Levels of circulating endothelial progenitor cells in systemic sclerosis. Clin. Exp. Rheumatol. 2007, 25, 60–66. [Google Scholar] [PubMed]
- Benyamine, A.; Magalon, J.; Cointe, S.; Lacroix, R.; Arnaud, L.; Bardin, N.; Rossi, P.; Francès, Y.; Bernard-Guervilly, F.; Kaplanski, G.; et al. Increased serum levels of fractalkine and progenitor cells in systemic sclerosis. Arthritis Res. Ther. 2017, 19, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunasso, A.M.G.; Massone, C. Update on the pathogenesis of Scleroderma: Focus on circulating progenitor cells. F1000Research 2016, 5, F1000. [Google Scholar] [CrossRef] [Green Version]
- Campioni, D.; Lo Monaco, A.; Lanza, F.; Moretti, S.; Ferrari, L.; Fotinidi, M.; La Corte, R.; Cuneo, A.; Trotta, F. CXCR4 pos circulating progenitor cells coexpressing monocytic and endothelial markers correlating with fibrotic clinical features are present in the peripheral blood of patients affected by systemic sclerosis. Haematologica 2008, 93, 1233–1237. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, Y.; Kuwana, M. Proangiogenic hematopoietic cells of monocytic origin: Roles in vascular regeneration and pathogenic processes of systemic sclerosis. Histol. Histopathol. 2013, 28, 175–183. [Google Scholar] [CrossRef]
- Zhu, S.; Evans, S.; Yan, B.; Povsic, T.J.; Tapson, V.; Goldschmidt-Clermont, P.J.; Dong, C. Transcriptional Regulation of Bim by FOXO3a and Akt Mediates Scleroderma Serum–Induced Apoptosis in endothelial progenitor cells. Circulation 2008, 118, 2156–2165. [Google Scholar] [CrossRef] [Green Version]
- Nevskaya, T.; Bykovskaia, S.; Lyssuk, E.; Shakhov, I.; Zaprjagaeva, M.; Mach, E.; Ananieva, L.; Guseva, N.; Nassonov, E. Circulating endothelial progenitor cells in systemic sclerosis: Relation to impaired angiogenesis and cardiovascular manifestations. Clin. Exp. Rheumatol. 2008, 26, 421–429. [Google Scholar]
- Patschan, S.; Tampe, D.; Müller, C.; Seitz, C.; Herink, C.; Müller, G.A.; Zeisberg, E.; Henze, E.; Patschan, D. Early Endothelial Progenitor Cells (eEPCs) in systemic sclerosis (SSc)-dynamics of cellular regeneration and mesenchymal transdifferentiation. BMC Musculoskelet. Disord. 2016, 12, 339. [Google Scholar] [CrossRef] [Green Version]
- Shirai, Y.; Okazaki, Y.; Inoue, Y.; Tamura, Y.; Yasuoka, H.; Takeuchi, T.; Kuwana, M. Elevated Levels of Pentraxin 3 in Systemic Sclerosis Associations With Vascular Manifestations and Defective Vasculogenesis. Arthritis Rheumatol. 2015, 67, 498–507. [Google Scholar] [CrossRef]
- Kuwana, M.; Okazaki, Y. Quantification of circulating endothelial progenitor cells in systemic sclerosis: A direct comparison of protocols. Ann. Rheum. Dis. 2012, 71, 617–620. [Google Scholar] [CrossRef]
- Andrigueti, F.V.; Arismendi, M.I.; Ebbing, P.C.C.; Kayser, C. Decreased numbers of endothelial progenitor cells in patients in the early stages of systemic sclerosis. Microvasc. Res. 2015, 98, 82–87. [Google Scholar] [CrossRef]
- Mok, M.Y.; Yiu, K.H.; Wong, C.Y.; Qiuwaxi, J.; Lai, W.H.; Wong, W.S.; Tse, H.F.; Lau, C.S. Low circulating level of CD133 + KDR + cells in patients with systemic sclerosis. Clin. Exp. Rheumatol. 2010, 28, S19–S25. [Google Scholar]
- Avouac, J.; Juin, F.; Wipff, J.; Couraud, P.O.; Chiocchia, G.; Kahan, A.; Boileau, C.; Uzan, G.; Allanore, Y. Circulating endothelial progenitor cells in systemic sclerosis: Association with disease severity. Ann. Rheum. Dis. 2008, 67, 1455–1460. [Google Scholar] [CrossRef]
- Del Papa, N.; Quirici, N.; Soligo, D.; Scavullo, C.; Cortiana, M.; Borsotti, C.; Maglione, W.; Comina, D.P.; Vitali, C.; Fraticelli, P. Bone Marrow Endothelial Progenitors Are Defective in Systemic Sclerosis. Arthritis Rheum. 2006, 54, 2605–2615. [Google Scholar] [CrossRef] [Green Version]
- Del Papa, N.; Colombo, G.; Fracchiolla, N.; Moronetti, L.M.; Ingegnoli, F.; Maglione, W.; Comina, D.P.; Vitali, C.; Fantini, F.; Cortelezzi, A. Circulating Endothelial Cells as a Marker of Ongoing Vascular Disease in Systemic Sclerosis. Arthritis Rheum. 2004, 50, 1296–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avouac, J.; Meune, C.; Ruiz, B.; Couraud, P.O.; Uzan, G.; Boileau, C.; Kahan, A.; Chiocchia, G.; Allanore, Y. Angiogenic biomarkers predict the occurrence of digital ulcers in systemic sclerosis. Ann. Rheum. Dis. 2011, 71, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Avouac, J.; Valluci, M.; Smith, V.; Senet, P.; Ruiz, B.; Sulli, A.; Pizzorni, C.; Frances, C.; Chiocchia, G.; Cutolo, M.; et al. Correlations between angiogenic factors and capillaroscopic patterns in systemic sclerosis. Arthritis Res. Ther. 2013, 15, R55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747, Also puplished in Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Update of the International Multidisciplinary Classification of the Idiopathic Interstitial Pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Lynch, D.A.; Sverzellati, N.; Travis, W.D.; Brown, K.K.; Colby, T.V.; Galvin, J.R.; Goldin, J.G.; Hansell, D.M.; Inoue, Y.; Johkoh, T.; et al. Diagnostic criteria for idiopathic pulmonary fibrosis: A Fleischner Society White Paper. Lancet Respir. Med. 2018, 6, 138–153. [Google Scholar] [CrossRef]
- Distler, J.H.W.; Allanore, Y.; Avouac, J.; Giacomelli, R.; Guiducci, S.; Moritz, F.; Akhmetshina, A.; Walker, U.A.; Gabrielli, A.; Müller-Ladner, U.; et al. EULAR Scleroderma Trials and Research group statement and recommendations on endothelial precursor cells EUSTAR statement and recommendations on endothelial precursor cells. Ann. Rheum. Dis. 2009, 68, 163–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt-Lucke, C.; Fichtlscherer, S.; Aicher, A.; Tschöpe, C.; Schultheiss, H.; Zeiher, A.M.; Dimmeler, S. Quantification of Circulating Endothelial Progenitor Cells Using the Modified ISHAGE Protocol. PLoS ONE 2010, 5, e13790. [Google Scholar] [CrossRef]
- Van Craenenbroeck, E.M.; Van Craenenbroeck, A.H.; Van Ierssel, S.; Bruyndonckx, L.; Hoymans, V.Y.; Vrints, C.J.; Conraads, V.M. Quantification of circulating CD34+/KDR+/CD45 dim endothelial progenitor cells: Analytical considerations. Int. J. Cardiol. 2013, 167, 1688–1695. [Google Scholar] [CrossRef]
- Smajda, D.M.; Mauge, L.; Nunes, H.; D’Audigier, C.; Juvin, K.; Borie, R.; Carton, Z.; Bertil, S.; Blanchard, A.; Crestani, B.; et al. Imbalance of circulating endothelial cells and progenitors in idiopathic pulmonary fibrosis. Angiogenesis 2013, 16, 147–157. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SSc-ILD+ Patients n = 21 | SSc-ILD− Patients n = 20 | IPF Patients n = 21 | Healthy Controls n = 21 | |
|---|---|---|---|---|
| Sex (women), n (%) | 13 (61.9) | 18 (90.0) | 7 (33.3) | 7 (33.3) |
| Age at study, mean ± SD, years | 60.3 ± 7.0 | 56.6 ± 15.4 | 69.2 ± 10.0 | 41.2 ± 12.5 |
| Smoking ever, n (%) | 11 (52.4) | 11 (55.0) | 16 (76.2) | 5 (31.3) |
| SSc duration, mean ± SD, years | 10.8 ± 8.3 | 9.6 ± 8.1 | - | - |
| Antibodies status | ||||
| ANA positive, n (%) | 19 (95.0) | 18 (90.0) | - | - |
| ACA positive, n (%) | 1 (5.0) | 9 (45.0) | - | - |
| ATA (anti-Scl70) positive (%) | 10 (50.0) | 4 (20.0) | - | - |
| CRP (mg/dL), mean ± SD | 0.7 ± 1.4 | 0.5 ± 0.5 | - | - |
| ESR (mm/1st hour), mean ± SD | 20.1 ± 15.9 | 17.2 ± 13.4 | - | - |
| Pulmonary function tests | ||||
| FVC (% predicted), mean ± SD | 88.4 ± 27.1 | 106.6 ± 15.9 | 84.9 ± 14.7 | - |
| FEV1 (% predicted), mean ± SD | 87.3 ± 25.6 | 101.9 ± 17.8 | 87.3 ± 19.6 | - |
| FEV1/FVC (% predicted), mean ± SD | 79.7 ± 5.5 | 79.2 ± 9.9 | 79.7 ± 7.8 | - |
| DLCO (% predicted), mean ± SD | 47.5 ± 19.5 | 71.5 ± 15.3 | 43.6 ± 18.4 | - |
| Pulmonary hypertension, n (%) | 3 (15.8) | 0 (0.0) | 4 (26.7) | - |
| HRCT | ||||
| Pulmonary involvement on HRCT | 21 (100.0) | 0 (0.0) | 21 (100.0) | - |
| NSIP pattern, n (%) | 14 (66.7) | - | 0 (0.0) | - |
| Non-NSIP pattern, n (%) | 1 (4.7) | - | 0 (0.0) | - |
| UIP pattern, n (%) | 3 (14.3) | - | 21 (100.0) | - |
| Probable UIP pattern, n (%) | 3 (14.3) | - | 0 (0.0) | - |
| Other SSc clinical manifestations | ||||
| Renal impairment, n (%) | 1 (4.8) | 1 (5.0) | - | - |
| Cardiac involvement, n (%) | 6 (28.6) | 1 (5.0) | - | - |
| Raynaud’s phenomenon, n (%) | 21 (100.0) | 20 (100.0) | - | - |
| Esophageal dysfunction, n (%) | 12 (57.1) | 5 (25.0) | - | - |
| Calcinosis, n (%) | 0 (0.0) | 6 (30.0) | - | - |
| Synovitis, n (%) | 6 (28.6) | 6 (30.0) | - | - |
| SSc-ILD+ Patients | SSc-ILD− Patients | IPF Patients | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Age (years) | −0.33 | 0.14 | −0.34 | 0.14 | 0.02 | 0.94 |
| Duration of SSc disease (years) | −0.45 | 0.04 | −0.10 | 0.69 | - | - |
| CRP (mg/dL) | −0.08 | 0.76 | −0.26 | 0.26 | - | - |
| ESR (mm/1st hour) | −0.25 | 0.33 | −0.01 | 0.96 | - | - |
| FVC (% predicted) | −0.24 | 0.30 | 0.06 | 0.82 | −0.21 | 0.35 |
| FEV1 (% predicted) | −0.19 | 0.40 | 0.04 | 0.89 | −0.19 | 0.40 |
| FEV1/FVC (% predicted) | 0.07 | 0.74 | 0.13 | 0.61 | −0.05 | 0.83 |
| DLCO (% predicted) | −0.01 | 0.99 | −0.06 | 0.84 | −0.23 | 0.40 |
| Variable | Category | SSc-ILD+ Patients | SSc-ILD− Patients | IPF Patients | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | ||
| Sex | Male | 0.045 ± 0.021 | 0.04 | 0.047 ± 0.017 | 0.28 | 0.093 ± 0.047 | 0.70 |
| Female | 0.030 ± 0.007 | 0.024 ± 0.028 | 0.086 ± 0.042 | ||||
| Smoking ever | No | 0.022 ± 0.018 | 0.50 | 0.020 ± 0.019 | 0.40 | 0.092 ± 0.048 | 0.93 |
| Yes | 0.040 ± 0.014 | 0.031 ± 0.033 | 0.091 ± 0.045 | ||||
| ANA | No | 0.025 | 0.46 | 0.022 ± 0.017 | 0.85 | - | |
| Yes | 0.037 ± 0.016 | 0.027 ± 0.029 | |||||
| ACA | No | 0.037 ± 0.016 | 0.33 | 0.024 ± 0.021 | 0.76 | - | |
| Yes | 0.021 | 0.028 ± 0.036 | |||||
| ATA (anti-Scl70) | No | 0.033 ± 0.011 | 0.35 | 0.026 ± 0.030 | 0.93 | - | |
| Yes | 0.040 ± 0.193 | 0.025 ± 0.023 | |||||
| PH | No | 0.033 ± 0.013 | 0.07 | 0.026 ± 0.028 | - | 0.088 ± 0.037 | 0.52 |
| Yes | 0.052 ± 0.028 | - | 0.106 ± 0.066 | ||||
| HRCT pattern | NSIP | 0.032 ± 0.010 | 0.36 | - | - | - | |
| UIP | 0.039 ± 0.023 | 0.091 ± 0.045 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pulito-Cueto, V.; Remuzgo-Martínez, S.; Genre, F.; Atienza-Mateo, B.; Mora-Cuesta, V.M.; Iturbe-Fernández, D.; Lera-Gómez, L.; Pérez-Fernández, R.; Prieto-Peña, D.; Portilla, V.; et al. Endothelial Progenitor Cells: Relevant Players in the Vasculopathy and Lung Fibrosis Associated with the Presence of Interstitial Lung Disease in Systemic Sclerosis Patients. Biomedicines 2021, 9, 847. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9070847
Pulito-Cueto V, Remuzgo-Martínez S, Genre F, Atienza-Mateo B, Mora-Cuesta VM, Iturbe-Fernández D, Lera-Gómez L, Pérez-Fernández R, Prieto-Peña D, Portilla V, et al. Endothelial Progenitor Cells: Relevant Players in the Vasculopathy and Lung Fibrosis Associated with the Presence of Interstitial Lung Disease in Systemic Sclerosis Patients. Biomedicines. 2021; 9(7):847. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9070847
Chicago/Turabian StylePulito-Cueto, Verónica, Sara Remuzgo-Martínez, Fernanda Genre, Belén Atienza-Mateo, Víctor M. Mora-Cuesta, David Iturbe-Fernández, Leticia Lera-Gómez, Raquel Pérez-Fernández, Diana Prieto-Peña, Virginia Portilla, and et al. 2021. "Endothelial Progenitor Cells: Relevant Players in the Vasculopathy and Lung Fibrosis Associated with the Presence of Interstitial Lung Disease in Systemic Sclerosis Patients" Biomedicines 9, no. 7: 847. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9070847