
Circulatory Inflammatory Mediators in the Prediction of Anti-Tuberculous Drug-Induced Liver Injury Using RUCAM for Causality Assessment

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
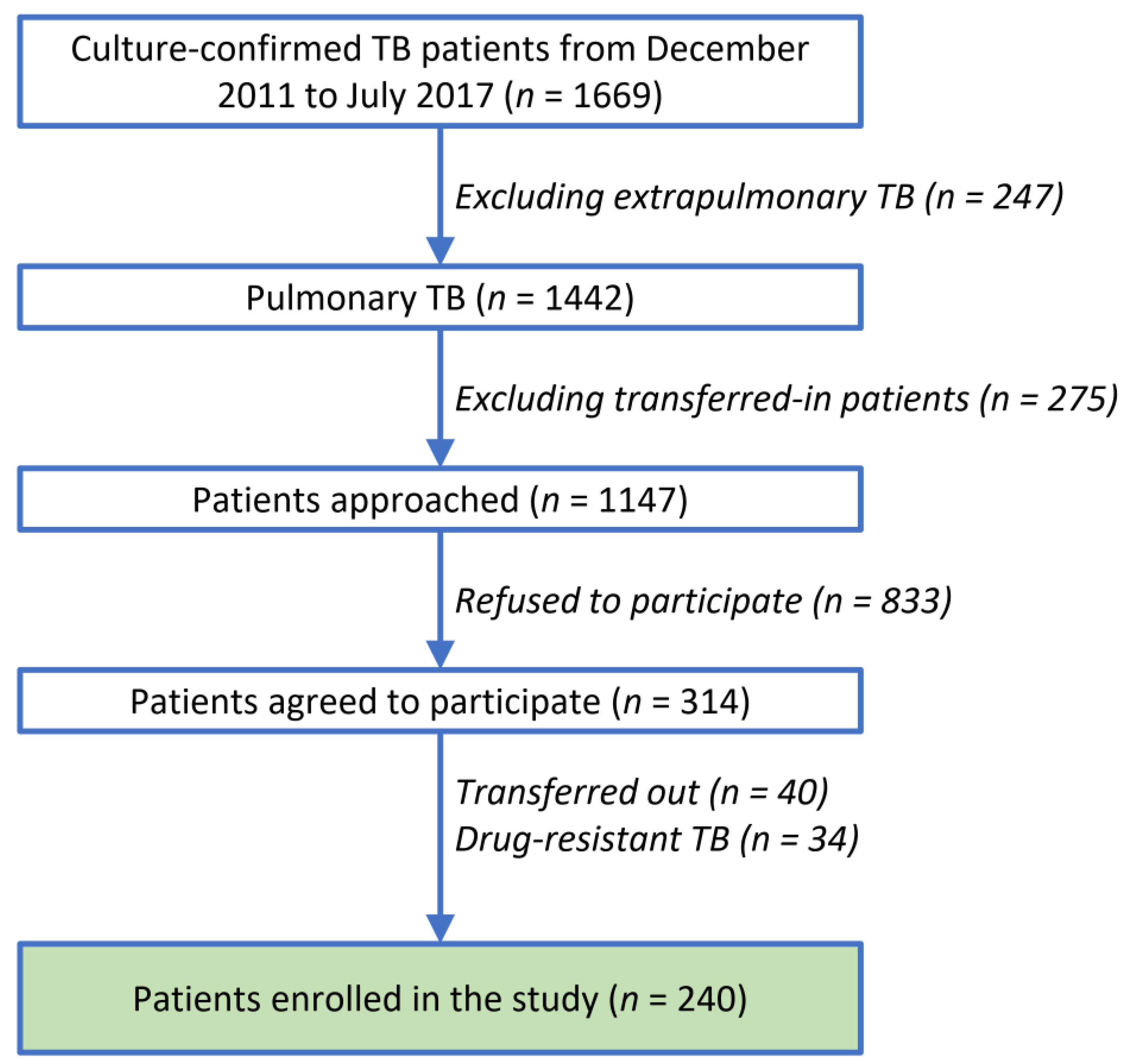
2.1. Patients
2.2. Protocol
2.3. Clinical Parameters
2.4. Outcome Definitions of DILI
2.5. Assays of Plasma Biomarkers
2.6. Statistical Analysis
3. Results
3.1. Demographics, DILI Correlation, and DILI-Free Survival
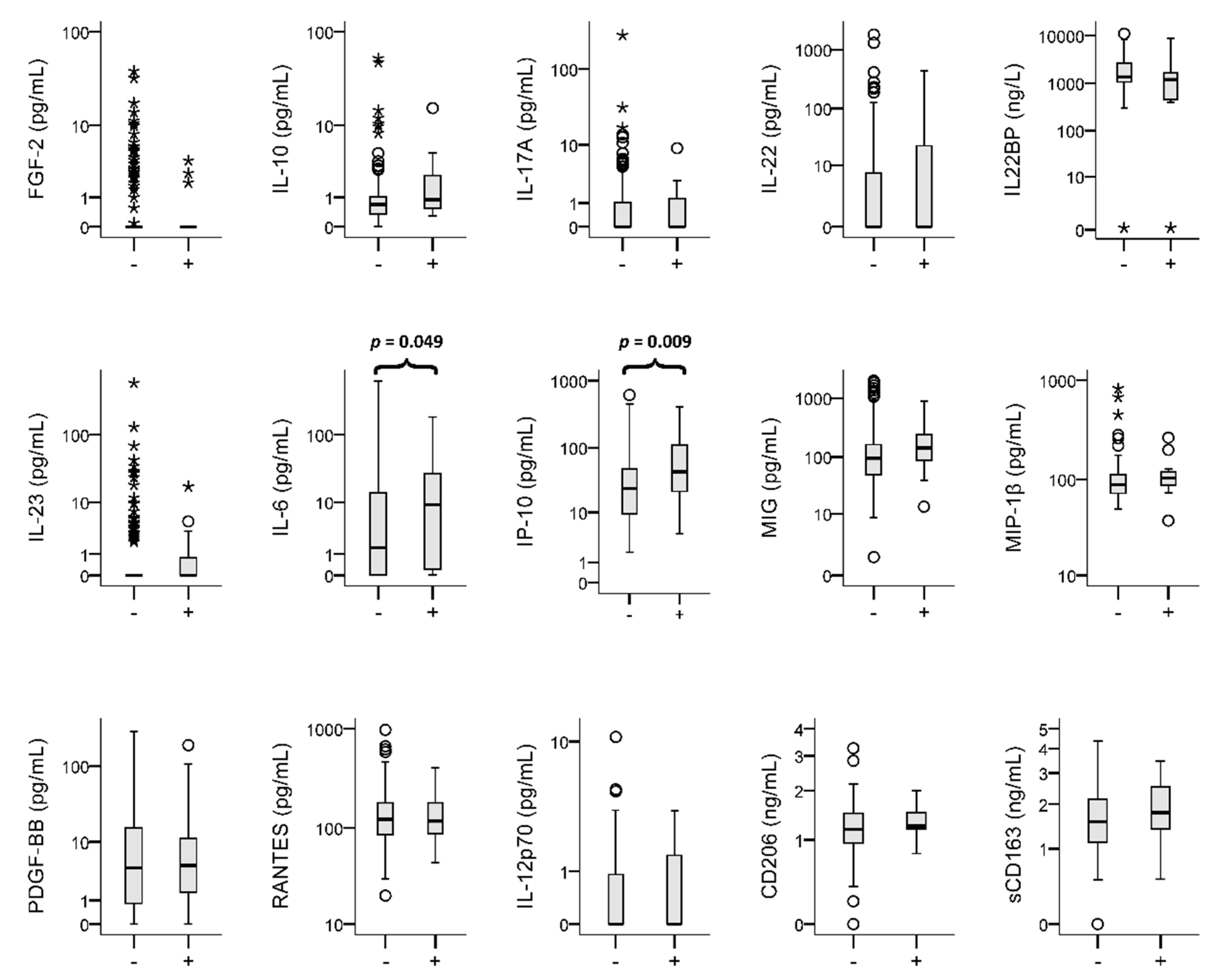
3.2. Plasma Biomarkers and DILI Correlation
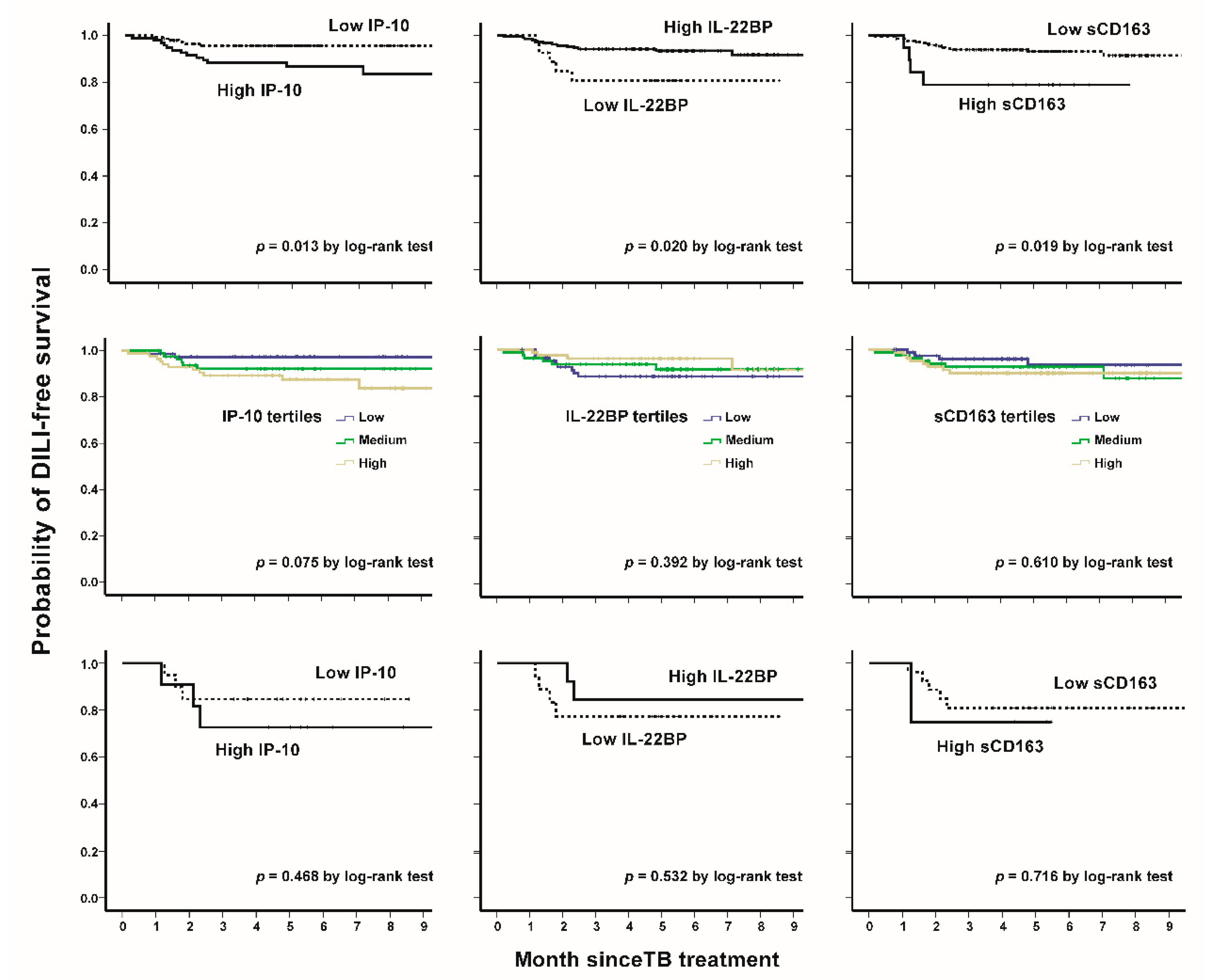
3.3. IP-10, IL22BP, and sCD163: Patient Characteristics, DILI-Free Survivals, and Sensitivity Analysis
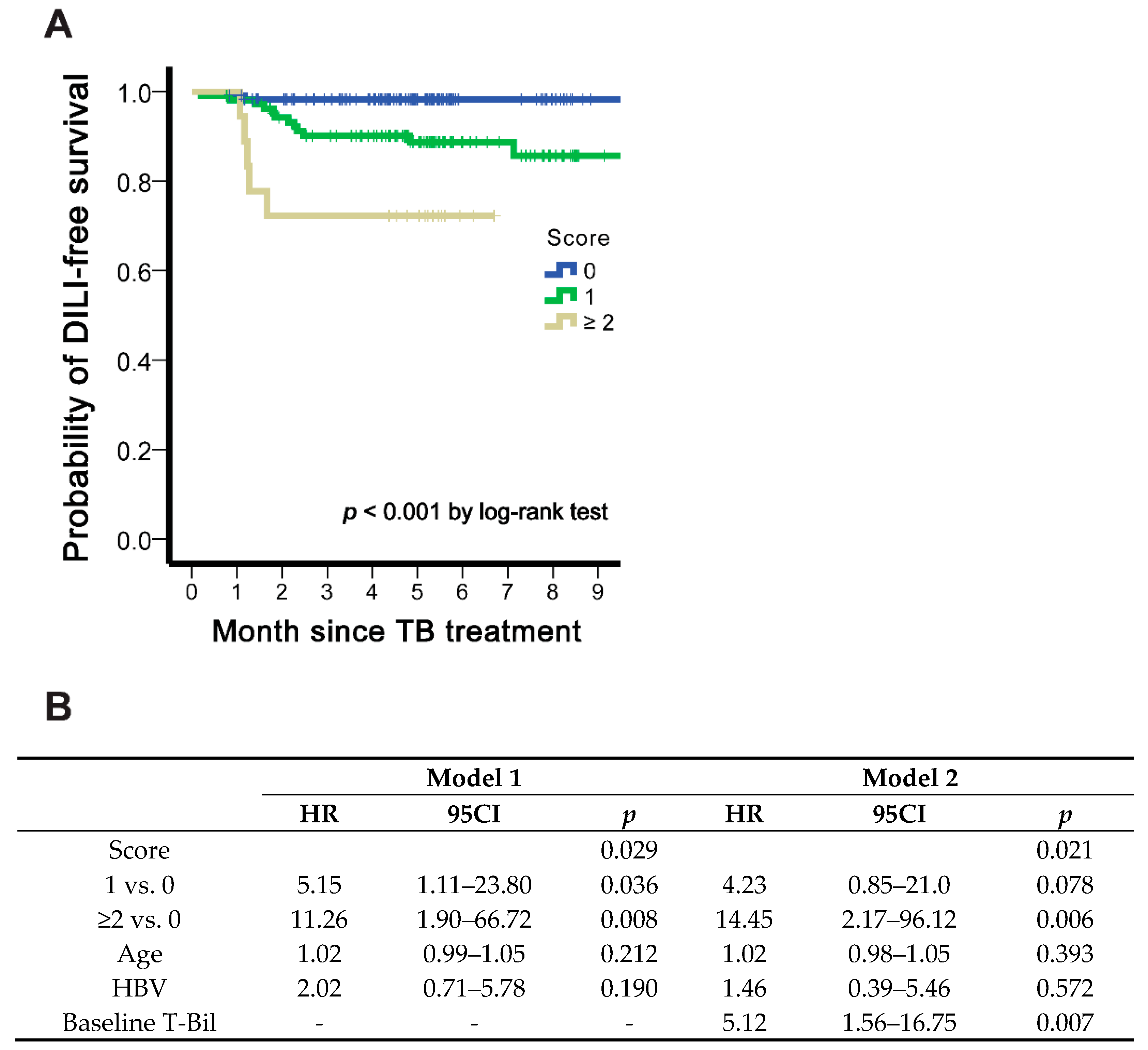
3.4. Scoring Predicting DILI
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Andrade, R.J.; Aithal, G.P.; Björnsson, E.S.; Kaplowitz, N.; Kullak-Ublick, G.A.; Larrey, D.; Karlsen, T.H.; European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Drug-induced liver injury. J. Hepatol. 2019, 70, 1222–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuster, D.; Samet, J. Alcohol use in patients with chronic liver disease. N. Engl. J. Med. 2018, 379, 1251–1261. [Google Scholar] [CrossRef]
- Wen, C.S.; Ho, C.M. Alcohol or not: A review comparing initial mechanisms, contributing factors, and liver transplantation outcomes between alcoholic and nonalcoholic steatohepatitis. Eur. Med. J. 2018, 3, 40–48. [Google Scholar]
- Ho, C.M.; Lee, C.H.; Wang, J.Y.; Lee, P.H.; Lai, H.S.; Hu, R.H. Nationwide longitudinal analysis of acute liver failure in Taiwan. Medicine 2014, 93, e35. [Google Scholar] [CrossRef]
- Wang, J.Y.; Liu, C.H.; Hu, F.C.; Chang, H.C.; Liu, J.L.; Chen, J.M.; Yu, C.J.; Lee, L.N.; Kao, J.H.; Yang, P.C. Risk factors of hepatitis during anti-tuberculous treatment and implications of hepatitis virus load. J. Infect. 2011, 62, 448–455. [Google Scholar] [CrossRef]
- Wang, J.Y.; Lee, L.N.; Yu, C.J.; Chien, Y.J.; Yang, P.C.; Tami Group. Factors influencing time to smear conversion in patients with smear-positive pulmonary tuberculosis. Respirology 2009, 14, 1012–1019. [Google Scholar] [CrossRef]
- Devarbhavi, H.; Aithal, G.; Treeprasertsuk, S.; Takikawa, H.; Mao, Y.; Shasthry, S.M.; Hamid, S.; Tan, S.S.; Philips, C.A.; George, J.; et al. Drug-induced liver injury: Asia Pacific Association of Study of Liver consensus guidelines. Hepatol. Int. 2021, 15, 258–282. [Google Scholar] [CrossRef]
- Tweed, C.D.; Wills, G.H.; Crook, A.M.; Dawson, R.; Diacon, A.H.; Louw, C.E.; McHugh, T.D.; Mendel, C.; Meredith, S.; Mohapi, L.; et al. Liver toxicity associated with tuberculosis chemotherapy in the REMoxTB study. BMC Med. 2018, 16, 46. [Google Scholar] [CrossRef] [Green Version]
- Meunier, L.; Larrey, D. Drug-induced liver injury: Biomarkers, requirements, candidates, and validation. Front. Pharmacol. 2019, 10, 1482. [Google Scholar] [CrossRef]
- Steuerwald, N.M.; Foureau, D.M.; Norton, H.J.; Zhou, J.; Parsons, J.C.; Chalasani, N.; Fontana, R.J.; Watkins, P.B.; Lee, W.M.; Reddy, K.R.; et al. Profiles of serum cytokines in acute drug-induced liver injury and their prognostic significance. PLoS ONE 2013, 8, e81974. [Google Scholar] [CrossRef]
- Chang, S.Y.; Chen, M.L.; Lee, M.R.; Liang, Y.C.; Lu, T.P.; Wang, J.Y.; Yan, B.S. SP110 polymorphisms are genetic markers for vulnerability to latent and active tuberculosis infection in Taiwan. Dis. Markers 2018, 2018, 4687380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, C.Y. Taiwan Guidelines for TB Diagnosis and Treatment, 6th ed.; Centers for Disease Control, R.O.C.: Taipei, Taiwan, 2018. [Google Scholar]
- U.S. Department of Health and Human Services; National Institutes of Health; National Institute of Allergy and Infectious Diseases; Division of AIDS. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events, Corrected Version 2.1. 2017. Available online: https://rsc.niaid.nih.gov/clinical-research-sites/daids-adverse-event-grading-tables (accessed on 6 June 2020).
- Danan, G.; Teschke, R. RUCAM in drug and herb induced liver injury: The update. Int. J. Mol. Sci. 2016, 17, 14. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [Green Version]
- Rathi, C.; Pipaliya, N.; Patel, R.; Ingle, M.; Phadke, A.; Sawant, P. Drug induced liver injury at a tertiary hospital in india: Etiology, clinical features and predictors of mortality. Ann. Hepatol. 2017, 16, 442–450. [Google Scholar] [CrossRef]
- Teschke, R.; Danan, G. Worldwide use of RUCAM for causality assessment in 81,856 idiosyncratic DILI and 14,029 HILI cases published 1993-mid 2020: A comprehensive analysis. Medicines 2020, 7, 62. [Google Scholar] [CrossRef]
- Danan, G.; Teschke, R. Roussel Uclaf Causality Assessment Method for drug-induced liver injury: Present and future. Front. Pharmacol. 2019, 10, 853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teschke, R.; Danan, G. Prospective Indian study of DILI with confirmed causality using the Roussel Uclaf Causality Assessment Method (RUCAM): A report of excellence. Ann. Hepatol. 2017, 16, 324–325. [Google Scholar] [CrossRef]
- Luster, A.D.; Unkeless, J.C.; Ravetch, J.V. Gamma-interferon transcriptionally regulates an early-response gene containing homology to platelet proteins. Nature 1985, 315, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Cornberg, M.; Wiegand, S.B. Importance of IP-10 in hepatitis B. Antivir. Ther. 2016, 21, 93–96. [Google Scholar] [CrossRef]
- Romero, A.I.; Lagging, M.; Westin, J.; Dhillon, A.P.; Dustin, L.B.; Pawlotsky, J.M.; Neumann, A.U.; Ferrari, C.; Missale, G.; Haagmans, B.L.; et al. Interferon (IFN)-gamma-inducible protein-10: Association with histological results, viral kinetics, and outcome during treatment with pegylated IFN-alpha 2a and ribavirin for chronic hepatitis C virus infection. J. Infect. Dis. 2006, 194, 895–903. [Google Scholar] [CrossRef] [Green Version]
- You, E.; Kim, M.H.; Lee, W.I.; Kang, S.Y. Evaluation of IL-2, IL-10, IL-17 and IP-10 as potent discriminative markers for active tuberculosis among pulmonary tuberculosis suspects. Tuberculosis 2016, 99, 100–108. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Corrado, A.; Ferrannini, E.; Fallahi, P. CXCR3, CXCL10 and type 1 diabetes. Cytokine Growth Factor Rev. 2014, 25, 57–65. [Google Scholar] [CrossRef]
- Singh, U.P.; Singh, N.P.; Guan, H.; Hegde, V.L.; Price, R.L.; Taub, D.D.; Mishra, M.K.; Nagarkatti, M.; Nagarkatti, P.S. The severity of experimental autoimmune cystitis can be ameliorated by anti-CXCL10 Ab treatment. PLoS ONE 2013, 8, e79751. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.Y.; Chen, E.M.; Ouyang, X.X.; Xu, X.; Ma, S.; Ji, F.; Wu, D.; Zhang, S.; Zhao, Y.; Li, L. Metabolomics and cytokine analysis for identification of severe drug-induced liver injury. J. Proteome Res. 2019, 18, 2514–2524. [Google Scholar] [CrossRef]
- Dai, S.; Liu, F.; Qin, Z.; Zhang, J.; Chen, J.; Ding, W.X.; Feng, D.; Ji, Y.; Qin, X. Kupffer cells promote T-cell hepatitis by producing CXCL10 and limiting liver sinusoidal endothelial cell permeability. Theranostics 2020, 10, 7163–7177. [Google Scholar] [CrossRef]
- Etzerodt, A.; Berg, R.M.; Plovsing, R.R.; Andersen, M.N.; Bebien, M.; Habbeddine, M.; Lawrence, T.; Møller, H.J.; Moestrup, S.K. Soluble ectodomain CD163 and extracellular vesicle-associated CD163 are two differently regulated forms of ’soluble CD163’ in plasma. Sci. Rep. 2017, 7, 40286. [Google Scholar] [CrossRef]
- Högger, P.; Sorg, C. Soluble CD163 inhibits phorbol ester-induced lymphocyte proliferation. Biochem. Biophys. Res. Commun. 2001, 288, 841–843. [Google Scholar] [CrossRef]
- Kneidl, J.; Löffler, B.; Erat, M.C.; Kalinka, J.; Peters, G.; Roth, J.; Barczyk, K. Soluble CD163 promotes recognition, phagocytosis and killing of Staphylococcus aureus via binding of specific fibronectin peptides. Cell Microbiol. 2012, 14, 914–936. [Google Scholar] [CrossRef]
- Parkner, T.; Sorensen, L.P.; Nielsen, A.R.; Fischer, C.P.; Bibby, B.M.; Nielsen, S.; Pedersen, B.K.; Møller, H.J. Soluble CD163: A biomarker linking macrophages and insulin resistance. Diabetologia 2012, 55, 1856–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanni, M.V.; Burdo, T.H.; Makimura, H.; Williams, K.C.; Grinspoon, S.K. Relationship between monocyte/macrophage activation marker soluble CD163 and insulin resistance in obese and normal-weight subjects. Clin. Endocrinol 2012, 77, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Gronbaek, H.; Sandahl, T.D.; Mortensen, C.; Vilstrup, H.; Møller, H.J.; Møller, S. Soluble CD163, a marker of Kupffer cell activation, is related to portal hypertension in patients with liver cirrhosis. Aliment. Pharmacol. Ther. 2012, 36, 173–180. [Google Scholar] [CrossRef]
- Hong, J.Y.; Lee, H.J.; Kim, S.Y.; Chung, K.S.; Kim, E.Y.; Jung, J.Y.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; et al. Efficacy of IP-10 as a biomarker for monitoring tuberculosis treatment. J. Infect. 2014, 68, 252–258. [Google Scholar] [CrossRef]
- Aristoteli, L.P.; Møller, H.J.; Bailey, B.; Moestrup, S.K.; Kritharides, L. The monocytic lineage specific soluble CD163 is a plasma marker of coronary atherosclerosis. Atherosclerosis 2006, 184, 342–347. [Google Scholar] [CrossRef]
- Kazankov, K.; Barrera, F.; Møller, H.J.; Bibby, B.M.; Vilstrup, H.; George, J.; Grønbaek, H. Soluble CD163, a macrophage activation marker, is independently associated with fibrosis in patients with chronic viral hepatitis B and C. Hepatology 2014, 60, 521–530. [Google Scholar] [CrossRef]
- Møller, H.J.; Grønbaek, H.; Schiødt, F.V.; Holland-Fischer, P.; Schilsky, M.; Munoz, S.; Hassanein, T.; Lee, W.M.; U.S. Acute Liver Failure Study Group. Soluble CD163 from activated macrophages predicts mortality in acute liver failure. J. Hepatol. 2007, 47, 671–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, M.C.; Hvidbjerg Gantzel, R.; Trebicka, J.; Møller, H.J.; Grønbæk, H. Macrophage activation markers, CD163 and CD206, in acute-on-chronic liver failure. Cells 2020, 9, 1175. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Bériou, G.; Heslan, M.; Chauvin, C.; Utriainen, L.; Aumeunier, A.; Scott, C.L.; Mowat, A.; Cerovic, V.; Houston, S.A.; et al. Interleukin-22 binding protein (IL-22BP) is constitutively expressed by a subset of conventional dendritic cells and is strongly induced by retinoic acid. Mucosal Immunol. 2014, 7, 101–113. [Google Scholar] [CrossRef]
- Zheng, Y.; Valdez, P.A.; Danilenko, D.M.; Hu, Y.; Sa, S.M.; Gong, Q.; Abbas, A.R.; Modrusan, Z.; Ghilardi, N.; de Sauvage, F.J.; et al. Interleukin-22 mediates early host defense against attaching and effacing bacterial pathogens. Nat. Med. 2008, 14, 282–289. [Google Scholar] [CrossRef]
- Aujla, S.J.; Chan, Y.R.; Zheng, M.; Fei, M.; Askew, D.J.; Pociask, D.A.; Reinhart, T.A.; McAllister, F.; Edeal, J.; Gaus, K.; et al. IL-22 mediates mucosal host defense against Gram-negative bacterial pneumonia. Nat. Med. 2008, 14, 275–281. [Google Scholar] [CrossRef]
- Eyerich, S.; Eyerich, K.; Cavani, A.; Schmidt-Weber, C. IL-17 and IL-22: Siblings, not twins. Trends Immunol. 2010, 31, 354–361. [Google Scholar] [CrossRef]
- Alabbas, S.Y.; Begun, J.; Florin, T.H.; Oancea, I. The role of IL-22 in the resolution of sterile and nonsterile inflammation. Clin. Transl. Immunol. 2018, 7, e1017. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.; Venkatasubramanian, S.; Paidipally, P.; Barnes, P.F.; Tvinnereim, A.; Vankayalapati, R. Interleukin 22 inhibits intracellular growth of Mycobacterium tuberculosis by enhancing calgranulin A expression. J. Infect. Dis 2014, 209, 578–587. [Google Scholar] [CrossRef] [Green Version]
- Feng, D.; Wang, Y.; Wang, H.; Weng, H.; Kong, X.; Martin-Murphy, B.V.; Li, Y.; Park, O.; Dooley, S.; Ju, C.; et al. Acute and chronic effects of IL-22 on acetaminophen-induced liver injury. J. Immunol. 2014, 193, 2512–2518. [Google Scholar] [CrossRef]
- Xiang, X.; Feng, D.; Hwang, S.; Ren, T.; Wang, X.; Trojnar, E.; Matyas, C.; Mo, R.; Shang, D.; He, Y.; et al. Interleukin-22 ameliorates acute-on-chronic liver failure by reprogramming impaired regeneration pathways in mice. J. Hepatol. 2020, 72, 736–745. [Google Scholar] [CrossRef]
- Schwarzkopf, K.; Rüschenbaum, S.; Barat, S.; Cai, C.; Mücke, M.M.; Fitting, D.; Weigert, A.; Brüne, B.; Zeuzem, S.; Welsch, C.; et al. IL-22 and IL-22-binding protein are associated with development of and mortality from acute-on-chronic liver failure. Hepatol. Commun. 2019, 3, 392–405. [Google Scholar] [CrossRef] [Green Version]
- Laverty, H.G.; Antoine, D.J.; Benson, C.; Chaponda, M.; Williams, D.; Kevin Park, B. The potential of cytokines as safety biomarkers for drug-induced liver injury. Eur. J. Clin. Pharmacol. 2010, 66, 961–976. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 240) | DILI (n = 19) | Non-DILI (n = 221) | p | |
|---|---|---|---|---|
| Age (years) | 55.8 ± 17.7 | 63.9 ± 14.4 | 55.1 ± 17.8 | 0.021 |
| Male sex (%) | 143 (59.6) | 12 (63.2) | 131 (59.3) | 0.812 |
| BMI (kg/m2) | 21.8 ± 3.3 | 21.7 ± 2.3 | 21.8 ± 3.4 | 0.798 |
| Active smoking | 39 (16.3) | 6 (31.6) | 33 (14.9) | 0.099 |
| Diabetes mellitus | 38 (15.8) | 3 (15.8) | 35 (15.8) | 1.000 |
| Hypertension | 34 (14.2) | 2 (10.5) | 32 (14.5) | 1.000 |
| Presence of cancer history | 42 (17.5) | 4 (21.1) | 38 (17.2) | 0.752 |
| Hepatitis B virus | 31 (12.9) | 6 (31.6) | 25 (11.3) | 0.023 |
| Hepatitis C virus | 4 (1.7) | 1 (5.3) | 3 (1.4) | 0.283 |
| Haemodialysis | 3 (1.3) | 1 (5.3) | 2 (0.9) | 0.220 |
| Autoimmune disease | 10 (4.2) | 1 (5.3) | 9 (4.1) | 0.569 |
| Baseline AST (U/L) | 26.5 ± 25.1 | 41.8 ± 46.7 | 25.1 ± 22.1 | 0.178 |
| Baseline ALT (U/L) | 22.4 ± 26.4 | 40.0 ± 52.0 | 20.9 ± 22.7 | 0.141 |
| Baseline T-Bil (mg/dL) | 0.6 ± 0.4 | 1.2 ± 1.1 | 0.6 ± 0.3 | 0.047 |
| Abnormal baseline LFT | 7 (2.9) | 2 (10.5) | 5 (2.3) | 0.098 |
| Case | Initial Data | Time to Peak (Days) | Peak Data | DILI Type | RUCAM Score | Probability of DILI | ||
|---|---|---|---|---|---|---|---|---|
| ALT ≥ 2 ULN | Bil-T ≥ 2 mg/dL | ALT (ULN) | Bil-T (mg/dL) | |||||
| 92.6/F | 0 | 0 | 33 | 8.8 | 1.2 | hepatocellular | 6 | probable |
| 47.8/M | 0 | 0 | 32 | 18.3 | 1.0 | hepatocellular | 7 | probable |
| 65.1/M | 0 | 0 | 37 | 20.8 | 0.9 | hepatocellular | 8 | probable |
| 48.7/F * | 0 | 0 | 38 | 10.9 | 0.5 | hepatocellular | 6 | probable |
| 72.4/F | 0 | 0 | 50 | 8.6 | 0.6 | hepatocellular | 7 | probable |
| 60.4/F | 0 | 0 | 24 | 5.6 | 0.3 | hepatocellular | 8 | probable |
| 65.5/F * | 0 | 0 | 54 | 15.1 | 1.3 | hepatocellular | 8 | probable |
| 47.7/F | 0 | 0 | 42 | 13.7 | 2.1 | hepatocellular | 8 | probable |
| 52.9/M * | 0 | 0 | 35 | 7.0 | 0.9 | hepatocellular | 8 | probable |
| 66.3/M * | 0 | 1 | 64 | 3.6 | 4.4 | cholestatic | 7 | probable |
| 60.1/M | 1 | 0 | 55 | 7.3 | 1.3 | hepatocellular | 10 | highly probable |
| 64.1/M | 0 | 0 | 55 | 5.4 | 0.5 | hepatocellular | 6 | probable |
| 91.0/M | 0 | 0 | 25 | 1.8 | 5.0 | mixed | 8 | probable |
| 38.8/M * | 0 | 0 | 48 | 6.3 | 0.7 | hepatocellular | 6 | probable |
| 85.5/M | 1 | 1 | 6 | 55.8 | 4.1 | hepatocellular | 9 | highly probable |
| 58.5/M * | 0 | 0 | 70 | 21.8 | 0.7 | hepatocellular | 6 | probable |
| 59.5/M | 0 | 0 | 68 | 8.0 | 0.8 | hepatocellular | 6 | probable |
| 70.0/F | 0 | 0 | 74 | 9.8 | 0.7 | hepatocellular | 12 | highly probable |
| 66.6/M | 0 | 0 | 35 | 25.1 | 0.8 | hepatocellular | 8 | probable |
| Univariable | Multivariable Backward Selection | |||||
|---|---|---|---|---|---|---|
| HR | 95CI | p | HR | 95% CI | p | |
| IL-10 | 6.32 | (0.84–47.5) | 0.073 | |||
| IL-17A | 1.22 | (0.47–3.22) | 0.683 | |||
| IL-22 | 1.68 | (0.67–4.17) | 0.267 | |||
| IL-22BP | 0.32 | (0.11–0.88) | 0.027 | 0.20 | (0.07–0.58) | 0.003 |
| IL-23 | 1.40 | (0.51–3.90) | 0.515 | |||
| IL-6 | 2.49 | (1.00–6.20) | 0.049 | |||
| IP-10 | 3.21 | (1.22–8.44) | 0.018 | 3.71 | (1.35–10.21) | 0.011 |
| MIG | 1.82 | (0.53–6.25) | 0.342 | |||
| MIP-1b | 5.43 | (0.73–40.7) | 0.100 | 6.81 | (0.87–53.47) | 0.068 |
| PDGF-BB | 1.62 | (0.47–5.57) | 0.443 | |||
| RANTES | 0.61 | (0.08–4.54) | 0.626 | |||
| IL-12p70 | 2.12 | (0.83–5.38) | 0.115 | |||
| CD206 | 4.02 | (1.17–13.8) | 0.027 | |||
| sCD163 | 3.47 | (1.15–10.5) | 0.028 | 3.28 | (1.07–10.06) | 0.038 |
| High IP-10 (n = 96) | Low IP-10 (n = 144) | p | High IL-22 BP (n = 213) | Low IL-22 BP (n = 27) | p | High sCD163 (n = 19) | Low sCD163 (n = 221) | p | |
|---|---|---|---|---|---|---|---|---|---|
| Average age (years, SD) | 60.8 ± 17.7 | 52.5 ± 16.9 | <0.001 | 55.8 ± 18.2 | 56.2 ± 13.8 | 0.912 | 67.8 ± 12.6 | 54.8 ± 17.7 | 0.002 |
| Male sex | 61 (63.5) | 82 (56.9) | 0.348 | 122 (57.3) | 21 (77.8) | 0.059 | 11 (57.9) | 132 (59.7) | >0.999 |
| BMI, kg/m2 (mean, SD) | 21.3 ± 3.3 | 22.1 ± 3.4 | 0.059 | 21.8 ± 3.4 | 22.2 ± 2.5 | 0.499 | 22.8 ± 2.9 | 21.7 ± 3.4 | 0.194 |
| Active smoking | 19 (20.4) | 20 (14.0) | 0.212 | 33 (15.8) | 6 (22.2) | 0.411 | 1 (5.6) | 38 (17.4) | 0.321 |
| Diabetes mellitus | 20 (20.8) | 18 (12.5) | 0.104 | 34 (16.0) | 4 (14.8) | >0.999 | 4 (21.1) | 34 (15.4) | 0.514 |
| Hypertension | 21 (21.9) | 13 (9.0) | 0.008 | 34 (16.0) | 0 | 0.018 | 5 (26.3) | 29 (13.1) | 0.160 |
| Cancer status | 19 (19.8) | 23 (16.0) | 0.490 | 38 (17.8) | 4 (14.8) | >0.999 | 3 (15.8) | 39 (17.6) | >0.999 |
| Hepatitis B virus | 11 (11.5) | 20 (13.9) | 0.696 | 13 (6.1) | 18 (66.7) | <0.001 | 4 (21.1) | 27 (12.2) | 0.282 |
| Hepatitis C virus | 4 (4.2) | 0 | 0.025 | 4 (1.9) | 0 | >0.999 | 0 | 4 (1.8) | >0.999 |
| Haemodialysis | 3 (3.1) | 0 | 0.063 | 2 (0.9) | 1 (3.7) | 0.302 | 0 | 3 (1.4) | >0.999 |
| Autoimmune disease | 7 (7.3) | 3 (2.1) | 0.094 | 9 (4.2) | 1 (3.7) | >0.999 | 0 | 10 (4.5) | >0.999 |
| Baseline AST (U/L) | 34.2 ± 37.6 | 21.9 ± 11.2 | 0.008 | 25.7 ± 25.5 | 32.1 ± 22.2 | 0.240 | 26.9 ± 14.6 | 26.4 ± 25.9 | 0.945 |
| Baseline ALT (U/L) | 27.4 ± 34.6 | 19.2 ± 18.8 | 0.039 | 21.4 ± 24.8 | 30.7 ± 36.3 | 0.092 | 24.9 ± 20.3 | 22.2 ± 26.9 | 0.664 |
| Baseline T-Bil (mg/dL) | 0.7 ± 0.6 | 0.6 ± 0.2 | 0.032 | 0.6 ± 0.5 | 0.7 ± 0.3 | 0.506 | 0.6 ± 0.3 | 0.6 ± 0.4 | 0.648 |
| Abnormal baseline LFT | 5 (5.2) | 2 (1.4) | 0.119 | 5 (2.3) | 2 (7.4) | 0.180 | 1 (5.3) | 6 (2.7) | 0.443 |
| Drug-induced liver injury | 13 (13.5) | 6 (4.2) | 0.013 | 14 (6.6) | 5 (18.5) | 0.047 | 4 (21.1) | 15 (6.8) | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-M.; Chen, C.-L.; Chang, C.-H.; Lee, M.-R.; Wang, J.-Y.; Hu, R.-H.; Lee, P.-H. Circulatory Inflammatory Mediators in the Prediction of Anti-Tuberculous Drug-Induced Liver Injury Using RUCAM for Causality Assessment. Biomedicines 2021, 9, 891. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9080891
Ho C-M, Chen C-L, Chang C-H, Lee M-R, Wang J-Y, Hu R-H, Lee P-H. Circulatory Inflammatory Mediators in the Prediction of Anti-Tuberculous Drug-Induced Liver Injury Using RUCAM for Causality Assessment. Biomedicines. 2021; 9(8):891. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9080891
Chicago/Turabian StyleHo, Cheng-Maw, Chi-Ling Chen, Chia-Hao Chang, Meng-Rui Lee, Jann-Yuan Wang, Rey-Heng Hu, and Po-Huang Lee. 2021. "Circulatory Inflammatory Mediators in the Prediction of Anti-Tuberculous Drug-Induced Liver Injury Using RUCAM for Causality Assessment" Biomedicines 9, no. 8: 891. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9080891