Parent, partner, co-parent or partnership? The need for clarity as family systems thinking takes hold in the quest to motivate behavioural change


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Research on Childhood Obesity Research Skewed towards Maternal Participation
3. Family Systems and Behaviour Change
4. The Importance of Parenting Partnerships
5. Parenting Partnerships and PSE
6. Partnership-Inclusive Practice
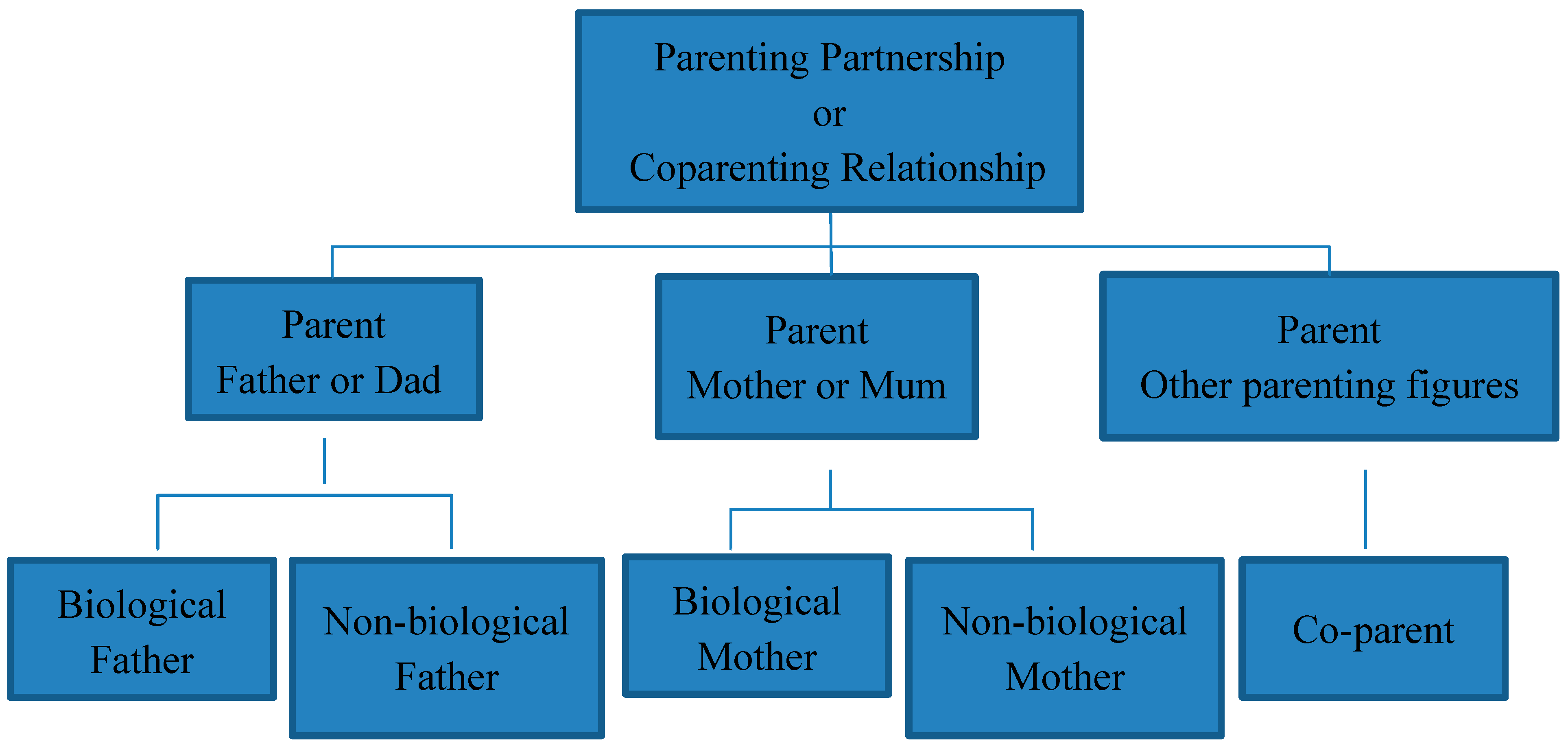
7. Recommendations for the Terminology Used to Describe Parents
8. Conclusions
Conflicts of Interest
References
- Van Der Kruk, J.J.; Kortekaas, F.; Lucas, C.; Jager-Wittenaar, H. Obesity: A systematic review on parental involvement in long-term European childhood weight control interventions with a nutritional focus. Obes. Rev. 2013, 14, 745–760. [Google Scholar] [CrossRef] [PubMed]
- Walsh, B.; Cullinan, J. Decomposing socioeconomic inequalities in childhood obesity: Evidence from Ireland. Econ. Hum. Biol. 2015, 16, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Paluch, R.A.; Roemmich, J.N.; Beecher, M.D. Family-Based Obesity Treatment, Then and Now: Twenty-Five Years of Pediatric Obesity Treatment. Health psychology: Official journal of the Division of Health Psychology, American Psychological Association. Health Psychol. 2007, 26, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Oude Luttikhuis, H.; Baur, L.; Jansen, H.; Shrewsbury, V.A.; O’Malley, C.; Stolk, R.P.; Summerbell, C.D. Interventions for treating obesity in children. Cochrane Database Syst. Rev. 2009, 1, CD001872. [Google Scholar]
- Loveman, E.; Al-Khudairy, L.; Johnson, R.E.; Robertson, W.; Colquitt, J.L.; Mead, E.L.; Rees, K. Parent-only interventions for childhood overweight or obesity in children aged 5 to 11 years. Cochrane Database Syst. Rev. 2015, 12, CD012008. [Google Scholar]
- Ewald, H.; Kirby, J.; Rees, K.; Robertson, W. Parent-only interventions in the treatment of childhood obesity: A systematic review of randomized controlled trials. J. Public Health 2014, 36, 476–489. [Google Scholar] [CrossRef] [PubMed]
- Jang, M.; Chao, A.; Whittemore, R. Evaluating Intervention Programs Targeting Parents to Manage Childhood Overweight and Obesity: A Systematic Review Using the RE-AIM Framework. J. Pediatr. Nurs. 2015, 30, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Berlyn, C.; Wise, S.; Soriano, G. Engaging Fathers in Child and Family Services: Participation, perceptions and good practice. Fam. Matters 2008, 80, 37. [Google Scholar]
- Fletcher, R.; May, C.; St George, J.; Stoker, L.; Oshan, M. Engaging Fathers: Evidence Review; Australian Research Alliance for Children and Youth (ARACY): Canberra, Australia, 2014. [Google Scholar]
- Gicevic, S.; Aftosmes-Tobio, A.; Manganello, J.A.; Ganter, C.; Simon, C.L.; Newlan, S.; Davison, K.K. Parenting and childhood obesity research: A quantitative content analysis of published research 2009–2015. Obes. Rev. 2016, 17, 724–734. [Google Scholar] [CrossRef] [PubMed]
- McAllister, F.; Burgess, A.; Kato, J.; Barker, G. Fatherhood: Parenting Programmes and Policy—A Critical Review of Best Practice; Fatherhood Institute/Promundo/MenCare: Washington, DC, USA, 2012; Available online: http://www.fatherhoodinstitute.org/wp-content/uploads/2012/07/Parenting-Programmes-and-Policy-Critical-Review-Full-Report.pdf (accessed on 19 April 2017).
- Bronfenbrenner, U. Ecology of the Family as a Context for Human Development: Research Perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Lloyd, A.B.; Wang, M.L.; Eather, N.; Miller, A.; Pagoto, S.L. Involvement of Fathers in Pediatric Obesity Treatment and Prevention Trials: A Systematic Review. Pediatrics 2017, 139, e20162635. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Gicevic, S.; Aftosmes-Tobio, A.; Ganter, C.; Simon, C.L.; Newlan, S.; Manganello, J.A. Fathers’ Representation in Observational Studies on Parenting and Childhood Obesity: A Systematic Review and Content Analysis. Am. J. Public Health 2016, 106, e14–e21. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.; Fletcher, R.; Collins, C.E.; Morgan, P.J.; Burrows, T.; Callister, R. Preventing and treating childhood obesity: Time to target fathers. Int. J. Obes. 2012, 36, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Lubans, D.R.; Callister, R.; Okely, A.D.; Burrows, T.L.; Fletcher, R.; Collins, C.E. The ‘Healthy Dads, Healthy Kids’ randomized controlled trial: Efficacy of a healthy lifestyle program for overweight fathers and their children. Int. J. Obes. 2011, 35, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Coleman, P.K.; Karraker, K.H. Parenting Self-Efficacy Among Mothers of School-Age Children: Conceptualization, Measurement, and Correlates*. Fam. Rel. 2000, 49, 13–24. [Google Scholar] [CrossRef]
- Sevigny, P.R.; Loutzenhiser, L. Predictors of parenting self-efficacy in mothers and fathers of toddlers. Child Care Health Dev. 2010, 36, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Spielman, V.; Taubman-Ben-Ari, O. Parental self-efficacy and stress-related growth in the transition to parenthood: A comparison between parents of pre- and full-term babies. Health Soc. Work 2009, 34, 201–212. [Google Scholar]
- Bandura, A. Self Efficacy: The Exercise of Control; W.H. Freeman and Company: New York, NY, USA, 1997. [Google Scholar]
- Duncanson, K.; Burrows, T.; Collins, C. Effect of a low-intensity parent-focused nutrition intervention on dietary intake of 2- to 5-year olds. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Okely, A.D.; Morgan, P.J.; Jones, R.A.; Burrows, T.L.; Cliff, D.P.; Baur, L.A. Parent diet modification, child activity, or both in obese children: An RCT. Pediatrics 2011, 127, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Crabb, A. The Wife Drought; Random House: Sydney, Australia, 2015. [Google Scholar]
- Duncanson, K.; Burrows, T.; Holman, B.; Collins, C. Parents’ perceptions of child feeding: A qualitative study based on the theory of planned behavior. J. Dev. Behav. Pediatr. 2013, 34, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Spinney, L. Venus and Mars collide. New Sci. 2011, 209, 43–45. [Google Scholar]
- Frascarolo, F.; Feinberg, M.; Albert Sznitman, G.; Favez, N. Professional gatekeeping toward fathers: A powerful influence on family and child development. Perspectives in Infant Mental Health [Internet]. 2016. (Summer 2016): [pp. 1–7]. Available online: http://www.waimh.org/files/Perspectives%20in%20IMH/2016_3/4-7_Frascaroloetal_2016_3_Perspectives_IMH.pdf7_Frascaroloetal_2016_3_Perspectives_IMH.pdf (accessed on 19 April 2017).
- Sayer, L.C.; Bianchi, S.M.; Robinson, J. Are Parents Investing Less in Children? Trends in Mothers’ and Fathers’ Time with Children. Am. J. Sociol. 2004, 110, 1–43. [Google Scholar] [CrossRef]
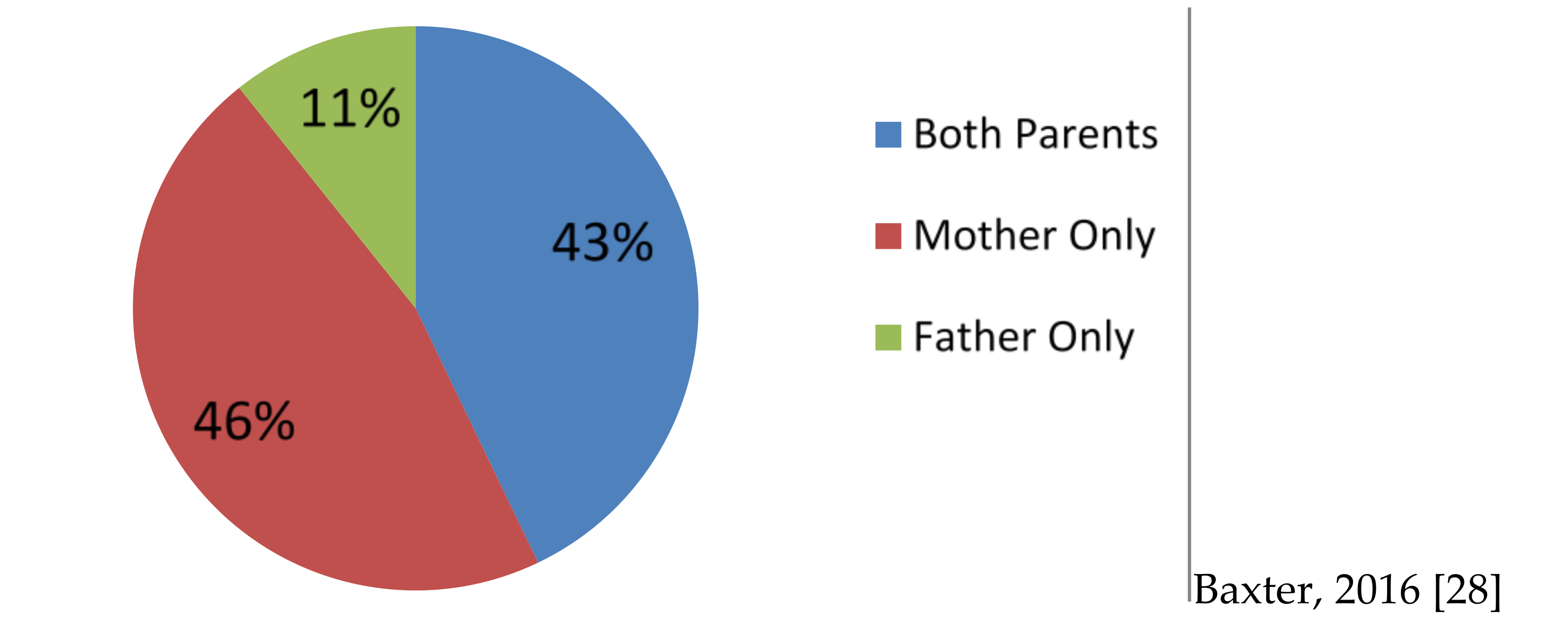
- Baxter, A. Australian Institute of Family Studies. Presented at Fathering Research Symposium, University of Newcastle, Newcastle, NSW, Australia, September 2016. [Google Scholar]
- Belsky, J. The Determinants of Parenting: A Process Model. Child Dev. 1984, 55, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Flouri, E.; Buchanan, A. Early father’s and mother’s involvement and child’s later educational outcomes. Br. J. Educ. Psychol. 2004, 74, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, M.E. The Internal Structure and Ecological Context of Co-parenting: A Framework for Research and Intervention. Parent. Sci. Pract. 2003, 3, 95–131. [Google Scholar] [CrossRef] [PubMed]
- McHale, J.P.; Kuersten-Hogan, R. Introduction: The Dynamics of Raising Children Together. J. Adult Dev. 2004, 11, 163–164. [Google Scholar] [CrossRef]
- Van Egeren, L.A.; Hawkins, D.P. Coming to Terms with Co-parenting: Implications of Definition and Measurement. J. Adult Dev. 2004, 11, 165–178. [Google Scholar] [CrossRef]
- Feinberg, M.E.; Brown, L.D.; Kan, M.L. A Multi-Domain Self-Report Measure of Co-parenting. Parent. Sci. Pract. 2012, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Morrill, M.I.; Hines, D.A.; Mahmood, S.; Cordova, J.V. Pathways between marriage and parenting for wives and husbands: The role of co-parenting. Fam. Process 2010, 49, 59–73. [Google Scholar] [CrossRef] [PubMed]
- McHale, J.P.; Kuersten-Hogan, R.; Rao, N. Growing Points for Co-parenting Theory and Research. J. Adult Dev. 2004, 11, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, M.E.; Jones, D.E.; Kan, M.L.; Goslin, M.C. Effects of family foundations on parents and children: 3.5 years after baseline. J. Fam. Psychol. 2010, 24, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Schoppe, S.J.; Mangelsdorf, S.C.; Frosch, C.A. Co-parenting, family process, and family structure: Implications for preschoolers’ externalizing behavior problems. J. Fam. Psychol. 2001, 15, 526–545. [Google Scholar] [CrossRef] [PubMed]
- Teubert, D.; Pinquart, M. The association between co-parenting and child adjustment: A meta-analysis. Parent.: Sci. Pract. 2010, 10, 286–307. [Google Scholar] [CrossRef]
- Jones, T.L.; Prinz, R.J. Potential roles of parental self-efficacy in parent and child adjustment: A review. Clin. Psychol. Rev. 2005, 25, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Leerkes, E.M.; Burney, R.V. The Development of Parenting Efficacy Among New Mothers and Fathers. Infancy 2007, 12, 45–67. [Google Scholar] [CrossRef]
- Yu, M. Family Relationships Quarterly No. 19: Australian Institute of Family Studies. 2011 [updated 2011 Aug. Available online: https://aifs.gov.au/cfca/publications/family-relationships-quarterly-no-19/parenting-efficacy-how-can-service-providers-help. (accessed on 6 December 2016).
- May, C.D. The importance of co-parenting quality when parenting a child with an Autism Spectrum Disorder: A mixed method investigation 2014. Available online: http://nova.newcastle.edu.au/vital/access/manager/Repository/uon:15001 (accessed on 6 December 2016).
- Davison, K.K.; Jurkowski, J.M.; Li, K.; Kranz, S.; Lawson, H.A. A childhood obesity intervention developed by families for families: Results from a pilot study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.S.; Vaughn, A.E.; Bangdiwala, K.I.; Campbell, M.; Jones, D.J.; Panter, A.T.; Stevens, J. Integrating a family-focused approach into child obesity prevention: Rationale and design for the My Parenting SOS study randomized control trial. BMC Public Health. 2011, 11, 431. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Collins, C.E.; Plotnikoff, R.C.; Callister, R.; Burrows, T.; Fletcher, R.; Cook, A.T. The ‘Healthy Dads, Healthy Kids’ community randomized controlled trial: A community-based healthy lifestyle program for fathers and their children. Prev. Med. 2014, 61, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Eapen, Z.J.; Peterson, E.D. Can Mobile Health Applications Facilitate Meaningful Behavior Change? Time Answ. JAMA 2015, 314, 1236–1237. [Google Scholar] [CrossRef] [PubMed]
- May, C.; Fletcher, R. The Development and Application of A Protocol for Writing, Assessing and Validating A Corpus of Relationship-Focused Text Messages for New and Expecting Fathers. Health Informatics, in press.
- Whittaker, R.; Matoff-Stepp, S.; Meehan, J.; Kendrick, J.; Jordan, E.; Stange, P.; Ratzan, S. Text4baby: Development and Implementation of a National Text Messaging Health Information Service. Am. J. Public Health 2012, 102, 2207–2213. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, N.J.; Fitzgerald, H.E.; Bradley, R.H.; Roggman, L. The Ecology of Father-Child Relationships: An Expanded Model. J. Fam. Theory Rev. 2014, 6, 336–354. [Google Scholar]
- Favez, N.; Widmer, E.D.; Doan, M.-T.; Tissot, H. Co-parenting in Stepfamilies: Maternal Promotion of Family Cohesiveness with Partner and with Father. J. Child Fam. Stud. 2015, 24, 3268–3278. [Google Scholar] [CrossRef]
- Merriam-Webster. Dictionary: Co-parent [Internet]. 2016. Available online: https://www.merriam-webster.com/dictionary/co-parent. (accessed on 15 Decemeber 2016).
- Secretariat of National Aboriginal and Islander Child Care. Child Rearing Practices 2016. Available online: http://www.supportingcarers.snaicc.org.au/caring-for-kids/child-rearing-practices/ (accessed on 19 December 2016).



© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
May, C.; Chai, L.K.; Burrows, T. Parent, partner, co-parent or partnership? The need for clarity as family systems thinking takes hold in the quest to motivate behavioural change. Children 2017, 4, 29. https://0-doi-org.brum.beds.ac.uk/10.3390/children4040029
May C, Chai LK, Burrows T. Parent, partner, co-parent or partnership? The need for clarity as family systems thinking takes hold in the quest to motivate behavioural change. Children. 2017; 4(4):29. https://0-doi-org.brum.beds.ac.uk/10.3390/children4040029
Chicago/Turabian StyleMay, Chris, Li Kheng Chai, and Tracy Burrows. 2017. "Parent, partner, co-parent or partnership? The need for clarity as family systems thinking takes hold in the quest to motivate behavioural change" Children 4, no. 4: 29. https://0-doi-org.brum.beds.ac.uk/10.3390/children4040029