The Many Roles of the Rock: A Qualitative Inquiry into the Roles and Responsibilities of Fathers of Children with Brain Tumors


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Description
2.2. Study Procedures
2.3. Data Analysis
3. Results
3.1. Paternal Knowledge Content and Format Preferences
3.2. Self-Definition of Paternal Role in Caring for a Child with a Neuro-Oncological Diagnosis
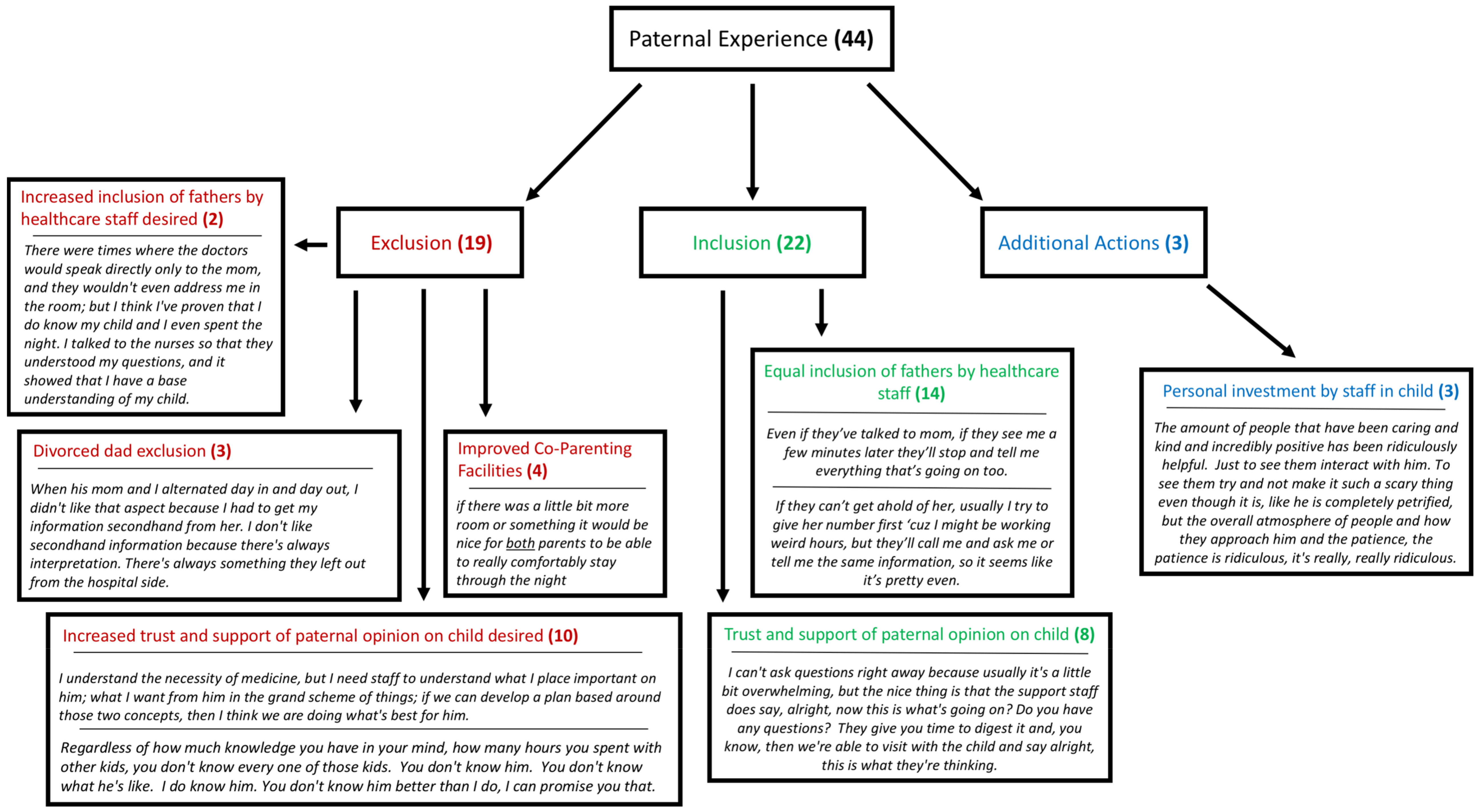
3.3. Hospital Actions of Paternal Inclusion and Exclusion
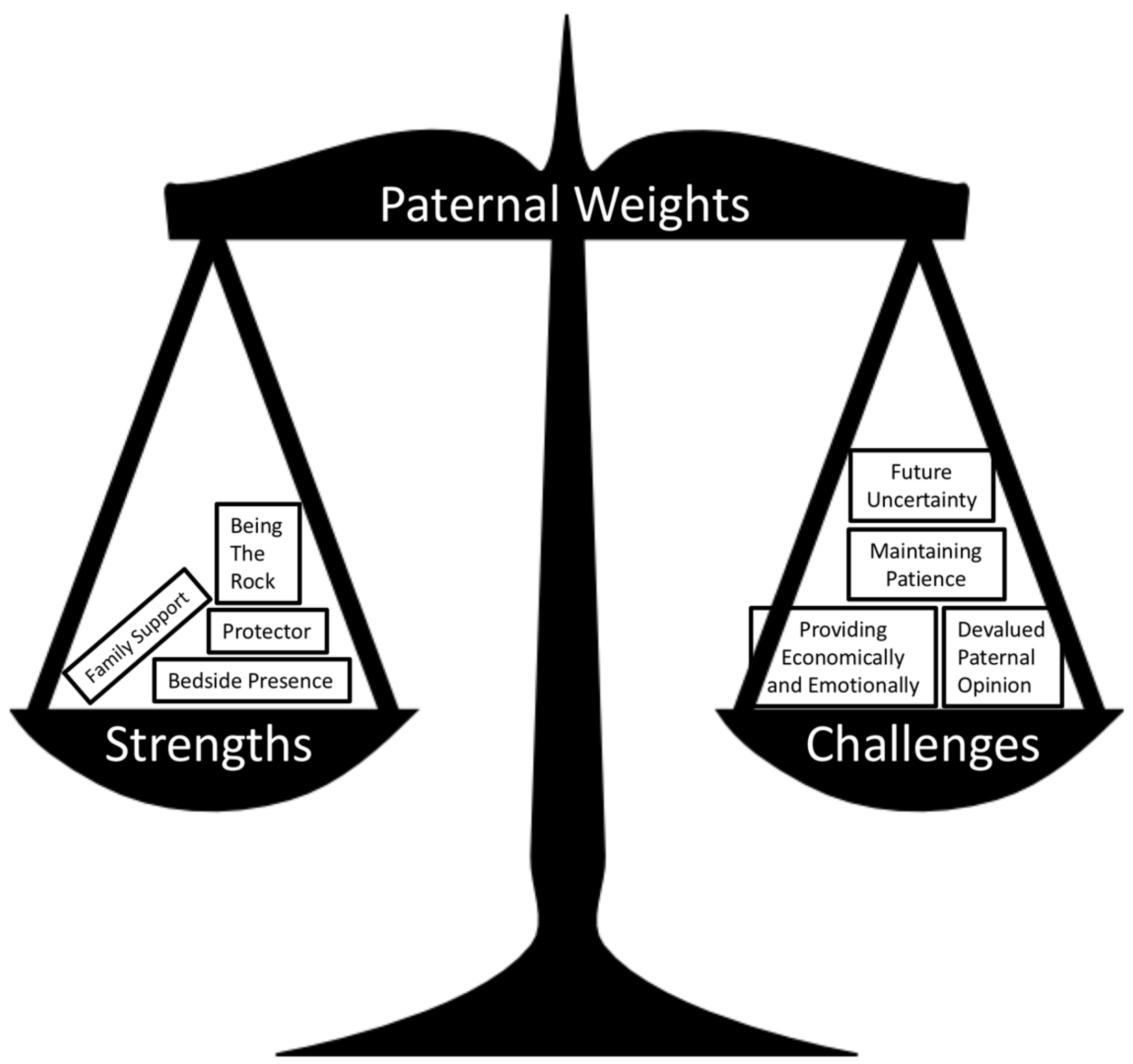
3.4. Unique Paternal Strengths and Challenges
3.5. Personal Growth
3.6. Advice for Other Fathers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Woodgate, R.L.; Tailor, K.; Yanofsky, R.; Vanan, M.I.; Information, P.E.K.F.C. Childhood brain cancer and its psychosocial impact on survivors and their parents: A qualitative thematic synthesis. Eur. J. Oncol. Nurs. 2016, 20, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Bennett, E.; English, M.W.; Rennoldson, M.; Starza-Smith, A. Predicting parenting stress in caregivers of children with brain tumours. Psycho-Oncology 2013, 22, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.M.; Holm, K.E.; Gurney, J.G. The impact of childhood cancer on the family: A qualitative analysis of strains, resources, and coping behaviors. Psycho-Oncology 2004, 13, 390–407. [Google Scholar] [CrossRef] [PubMed]
- Rocque, B.G.; Cutillo, A.; Zimmerman, K.; Arynchyna, A.; Davies, S.; Landier, W.; Madan-Swain, A. Distress and psychosocial risk in families with newly diagnosed pediatric brain tumors. J. Neurosurg. Pediatr. 2018, 23, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Boydell, K.M.; Stasiulis, E.; Greenberg, M.; Greenberg, C.; Spiegler, B. I’ll Show Them: The Social Construction of (In)Competence in Survivors of Childhood Brain Tumors. J. Pediatr. Oncol. Nurs. 2008, 25, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.M.; Chen, Y.C.; Haase, J.E. Games of lives in surviving childhood brain tumors. West J. Nurs. Res. 2008, 30, 435–457. [Google Scholar] [CrossRef]
- Barrera, M.; Atenafu, E.G.; Schulte, F.; Bartels, U.; Sung, L.; Janzen, L.; Chung, J.; Cataudella, D.; Hancock, K.; Saleh, A.; et al. Determinants of quality of life outcomes for survivors of pediatric brain tumors. Pediatr. Blood Cancer 2017, 64, e26481. [Google Scholar] [CrossRef]
- Beek, L.; Schappin, R.; Gooskens, R.; Huisman, J.; Jongmans, M. Surviving a brain tumor in childhood: Impact on family functioning in adolescence. Psychooncology 2015, 24, 89–94. [Google Scholar] [CrossRef]
- Kearney, J.A.; Salley, C.G.; Muriel, A.C. Standards of Psychosocial Care for Parents of Children With Cancer. Pediatr. Blood Cancer 2015, 62, S632–S683. [Google Scholar] [CrossRef] [Green Version]
- Shortman, R.I.; Beringer, A.; Penn, A.; Malson, H.; Lowis, S.P.; Sharples, P.M. The experience of mothers caring for a child with a brain tumour. Child Care, Health Dev. 2013, 39, 743–749. [Google Scholar] [CrossRef]
- Lou, H.-L.; Mu, P.-F.; Wong, T.-T.; Mao, H.-C. A Retrospective Study of Mothers’ Perspectives of the Lived Experience of Anticipatory Loss of a Child from a Terminal Brain Tumor. Cancer Nurs. 2015, 38, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Feudtner, C.; Walter, J.K.; Faerber, J.A.; Hill, D.L.; Carroll, K.W.; Mollen, C.J.; Miller, V.A.; Morrison, W.E.; Munson, D.; Kang, T.I.; et al. Good-parent beliefs of parents of seriously ill children. JAMA Pediatr. 2015, 169, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.C.; Enderby, K.; O’Toole, M.; Thomas, S.A.; Ashley, D.; Rosenfeld, J.V.; Simos, E.; Tokatlian, N.; Gedye, R. The Role of Social Support in Families Coping with Childhood Brain Tumor. J. Psychosoc. Oncol. 2009, 27, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.L.; Pelletier, W.; Decker, C.; Barczyk, A.; Dungan, S.S. Fathers of Children with Cancer: A Descriptive Synthesis of the Literature. Soc. Work. Heal. Care 2010, 49, 458–493. [Google Scholar] [CrossRef]
- Willis, G.B.; Artino, A.R., Jr. What do our respondents think we’re asking? Using cognitive interviewing to improve medical education surveys. J. Grad. Med. Educ. 2013, 5, 353–356. [Google Scholar] [CrossRef]
- Mays, N.; Pope, C. Qualitative research in health care. Assessing quality in qualitative research. BMJ 2000, 320, 50–52. [Google Scholar]
- Pope, C.; Ziebland, S.; Mays, N. Qualitative research in health care. Analysing qualitative data. BMJ 2000, 320, 114–116. [Google Scholar] [CrossRef]
- Wakefield, C.E.; Drew, D.; Ellis, S.J.; Doolan, E.L.; McLoone, J.K.; Cohn, R.J. ‘What they’re not telling you’: A new scale to measure grandparents’ information needs when their grandchild has cancer. Patient Educ. Couns. 2014, 94, 351–355. [Google Scholar] [CrossRef]
- Tran, L.N.; Back, A.L.; Creutzfeldt, C.J. Palliative Care Consultations in the Neuro-ICU: A Qualitative Study. Neurocritical Care 2016, 25, 266–272. [Google Scholar] [CrossRef]
- Björk, M.; Wiebe, T.; Hallström, I.K. Striving to Survive: Families’ Lived Experiences When a Child Is Diagnosed With Cancer. J. Pediatr. Oncol. Nurs. 2005, 22, 265–275. [Google Scholar] [CrossRef]
- Neil-Urban, S.; Jones, J.B. Father-to-father support: Fathers of children with cancer share their experience. J. Pediatr. Oncol. Nurs. 2002, 19, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Alderfer, M.A.; Mougianis, I.; Barakat, L.P.; Beele, D.; DiTaranto, S.; Hwang, W.T.; Reilly, A.T.; Kazak, A.E. Family psychosocial risk, distress, and service utilization in pediatric cancer: Predictive validity of the psychosocial assessment tool. Cancer 2009, 115, 4339–4349. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.; Newman, S.; Souhami, R. Anxiety and depression in adolescent cancer: Findings in patients and parents at the time of diagnosis. Eur. J. Cancer 1997, 33, 1250–1255. [Google Scholar] [CrossRef]
- Davies, B.; Gudmundsdottir, M.; Worden, B.; Orloff, S.; Sumner, L.; Brenner, P. “Living in the dragon’s shadow” fathers’ experiences of a child’s life-limiting illness. Death Stud. 2004, 28, 111–135. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, D.B.; Beaune, L.; Barrera, M.; Blumberg, J.; Belletrutti, M. Examining the Experiences of Fathers of Children with a Life-Limiting Illness. J. Soc. Work. End-Of-Life Palliat. Care 2016, 12, 126–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett Murphy, L.M.; Flowers, S.; McNamara, K.A.; Young-Saleme, T. Fathers of children with cancer: Involvement, coping, and adjustment. J. Pediatr. Health Care 2008, 22, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, D.B.; Gearing, R.E.; McNeill, T.; Fung, K.; Lucchetta, S.; Selkirk, E.K. Experiences and Resistance Strategies Utilized by Fathers of Children with Cancer. Soc. Work. Heal. Care 2009, 48, 260–275. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.C.; Stewart, H.; O’Toole, M.; Tokatlian, N.; Enderby, K.; Miller, J.; Ashley, D. Pediatric Brain Tumor Patients: Their Parents’ Perceptions of the Hospital Experience. J. Pediatr. Oncol. Nurs. 2007, 24, 95–105. [Google Scholar] [CrossRef] [PubMed]
- McGrath, P.; Chesler, M. Fathers’ perspectives on the treatment for pediatric hematology: Extending the findings. Issues Compr. Pediatr. Nurs. 2004, 27, 39–61. [Google Scholar] [CrossRef] [PubMed]
- Stavinoha, P.L.; Askins, M.A.; Powell, S.K.; Pillay Smiley, N.; Robert, R.S. Neurocognitive and psychosocial outcomes in pediatric brain tumor survivors. Bioengineering 2018, 5, 73. [Google Scholar] [CrossRef]
- Hocking, M.C.; Quast, L.F.; Brodsky, C.; Deatrick, J.A. Caregiver perspectives on the social competence of pediatric brain tumor survivors. Support. Care Cancer 2017, 25, 3749–3757. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, P.; Given, B.; Given, C.; Schiffman, R.; Murman, D.; Lovely, M. Caregivers of persons with a brain tumor: a conceptual model. Nurs. Inq. 2004, 11, 43–53. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n = ____ (%) | |
|---|---|---|
| Child’s Gender | Male | 2 (20) |
| Female | 2 (20) | |
| Child’s Age | Mean/Range (years) | 9.25/5–14 |
| Child’s Time Since Diagnosis | Mean/Range (months) | 47.8/3–168 |
| Child’s Location at Time of Interview | Hospital | 3 (75) |
| Outpatient | 1 (25) | |
| Father’s Ethnicity | Caucasian | 4 (100) |
| Father’s Home Locale | Rural | 1 (25) |
| Urban | 3 (75) | |
| Distance Home to Hospital | Mean/Range (miles) | 31.5/10–90 |
| Does the Child Reside Within the Home? | Yes | 4 (100) |
| Number of Other Children Living in the Home | Mean/Range (children) | 3.33/0–5 |
| Parental Marital Status | Married | 3 (75) |
| Separated | 1 (25) | |
| Parent Highest Level of Formal Education | Some College | 2 (50) |
| College Completion | 2 (50) | |
| Parent Employment Type | Manual Labor | 2 (50) |
| Office Work | 2 (50) | |
| Primary Caregiver of Child | Both | 2 (50) |
| Father | 1 (25) | |
| Mother | 1 (25) |
| Themes (n = 4) | Definition | Codes, n = __/ 27 (%) Participants, n = __/ 4 (%) | Exemplary Quotes |
|---|---|---|---|
| Teacher | A “good dad” is a willing teacher for his child. He teaches them values and lessons, and he provides the opportunity for them to achieve their life aspirations. | 4 (14.8%), 2 (50.0%) | “If you want to be an astronaut on Mars, go for it. It is going to take work. That is my job as a father to give them those, give them access to those avenues.” “Try to teach them as much as I can.” |
| Fulfiller of Life | A “good dad” provides a wide array of life experiences for their child. He helps them achieve their goals, and he helps them enjoy life through fun adventures and happy moments. | 11 (40.7%), 3 (75.0%) | “Giving them 100% access to the things that make them, allow them to figure out who they are.” “You know, like take them camping, fishing, and let them see everything.” “Making sure she gets as many experiences as possible and having a full life.” “(Providing) life, like trying different foods.” |
| Puts Child First | A “good dad” is unselfish. He puts his needs behind the needs of his child and his family, and he is present and involved with them for their entire life. | 10 (37.0%), 2 (50.0%) | “Somebody who puts the needs of the family above their needs and their wants.” “I just think that it just takes time and you have to be involved and you have to be willing to, you know, takes days off of work. You have to be willing to put what you can from your career off to the side.” |
| Rises to the Occasion | A “good dad” rises to the occasion of supporting their child by doing everything they may need to and by being strong, by “being a man.” | 2 (7.4%), 2 (50.0%) | “(Help them) with everything.” “That is the role of being a man.” |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, J.E.; Huskey, D.; Schwartz, J.; Weaver, M.S. The Many Roles of the Rock: A Qualitative Inquiry into the Roles and Responsibilities of Fathers of Children with Brain Tumors. Children 2019, 6, 113. https://0-doi-org.brum.beds.ac.uk/10.3390/children6100113
Robinson JE, Huskey D, Schwartz J, Weaver MS. The Many Roles of the Rock: A Qualitative Inquiry into the Roles and Responsibilities of Fathers of Children with Brain Tumors. Children. 2019; 6(10):113. https://0-doi-org.brum.beds.ac.uk/10.3390/children6100113
Chicago/Turabian StyleRobinson, Jacob E., David Huskey, Jonathan Schwartz, and Meaghann S. Weaver. 2019. "The Many Roles of the Rock: A Qualitative Inquiry into the Roles and Responsibilities of Fathers of Children with Brain Tumors" Children 6, no. 10: 113. https://0-doi-org.brum.beds.ac.uk/10.3390/children6100113