The Influence of Caregiver Distress and Child Anxiety in Predicting Child Somatization in Youth with Functional Abdominal Pain Disorders


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Questionnaires
Background and Demographics
Caregiver Distress Measure
Child FAPD and Associated Symptoms Measures
2.2.2. Data Analytic Plan
Missing Data Handling
Data Analytic Plan
3. Results
3.1. Participant Characteristics
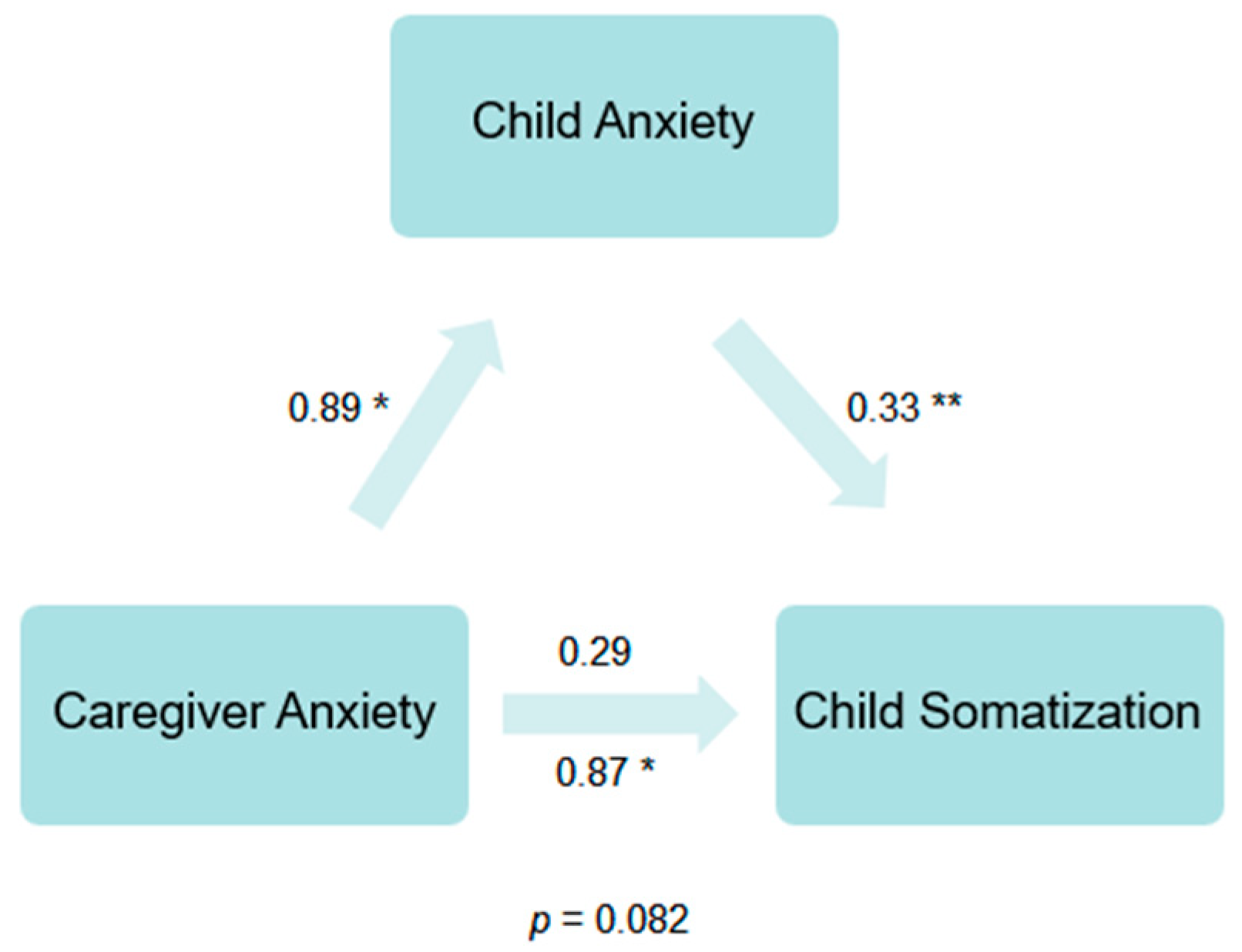
3.2. Primary Analyses
4. Discussion
Future Research and Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; MacDonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef]
- van der Veek, S.M.; Derkx, H.H.F.; de Haan, E.; Benninga, M.A.; Boer, F. Abdominal pain in Dutch schoolchildren: Relations with physical and psychological comorbid complaints in children and their parents. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 481–487. [Google Scholar] [CrossRef]
- Campo, J.V.; Comer, D.M.; Jansen-McWilliams, L.; Gardner, W.; Kelleher, K.J. Recurrent pain, emotional distress, and health service use in childhood. J. Pediatr. 2002, 141, 76–83. [Google Scholar] [CrossRef]
- Astrada, C.A.; Licamele, W.L.; Walsh, T.L.; Kessler, E.S. Recurrent abdominal pain in children and associated DSM-III diagnoses. Am. J. Psychiatry 1981, 138, 687–688. [Google Scholar]
- Gulewitsch, M.D.; Enck, P.; Schwille-Kiuntke, J.; Weimer, K.; Schlarb, A.A. Rome III criteria in parents’ hands: Pain-related functional gastrointestinal disorders in community children and associations with somatic complaints and mental health. Eur. J. Gastroenterol. Hepatol. 2013, 25, 1223–1229. [Google Scholar] [CrossRef]
- Horst, S.; Shelby, G.; Anderson, J.; Acra, S.; Polk, D.B.; Saville, B.R.; Garber, J.; Walker, L.S. Predicting persistence of functional abdominal pain from childhood into young adulthood. Clin. Gastroenterol. Hepatol. 2014, 12, 2026–2032. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.E.; Heitkemper, M.; Self, M.M.; Czyzewski, D.I.; Shulman, R.J. Endogenous inhibition of somatic pain is impaired in girls with irritable bowel syndrome compared with healthy girls. J. Pain 2013, 14, 921–930. [Google Scholar] [CrossRef] [Green Version]
- Yacob, D.; Di Lorenzo, C.; Bridge, J.A.; Rosenstein, P.F.; Onorato, M.; Bravender, T.; Campo, J.V. Prevalence of pain-predominant functional gastrointestinal disorders and somatic symptoms in patients with anxiety or depressive disorders. J. Pediatr. 2013, 163, 767–770. [Google Scholar] [CrossRef]
- Machnes-Maayan, D.; Elazar, M.; Apter, A.; Zeharia, A.; Krispin, O.; Eidlitz-Markus, T. Screening for psychiatric comorbidity in children with recurrent headache or recurrent abdominal pain. Pediatr. Neurol. 2014, 50, 49–56. [Google Scholar] [CrossRef]
- Eccleston, C.; Crombez, G.; Scotford, A.; Clinch, J.; Connell, H. Adolescent chronic pain: Patterns and predictors of emotional distress in adolescents with chronic pain and their parents. Pain 2004, 108, 221–229. [Google Scholar] [CrossRef]
- Ramchandani, P.G.; Stein, A.; Hotopf, M.; Wiles, N.J.; ALSPAC Study Team. Early parental and child predictors of recurrent abdominal pain at school age: Results of a large population-based study. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 729–736. [Google Scholar] [CrossRef]
- Campo, J.V.; Jansen-McWilliams, L.; Comer, D.M.; Kelleher, K.J. Somatization in pediatric primary care: Association with psychopathology, functional impairment, and use of services. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1093–1101. [Google Scholar] [CrossRef]
- Williams, A.E.; Czyzewski, D.I.; Self, M.M.; Shulman, R.J. Are child anxiety and somatization associated with pain in pain-related functional gastrointestinal disorders? J. Health Psychol. 2015, 20, 369–379. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Li, D.; Cheng, G.; Fan, J.; Lu, H. An epidemiologic study of irritable bowel syndrome in adolescents and children in South China: A school-based study. Child Care Health Dev. 2010, 36, 781–786. [Google Scholar] [CrossRef]
- Walker, L.S.; Garber, J.; Van Slyke, D.; Greene, J.W. Long-term health outcomes in patients with recurrent abdominal pain. J. Pediatr. Psychol. 1995, 20, 233–245. [Google Scholar] [CrossRef]
- Campo, J.V.; Bridge, J.; Ehmann, M.; Altman, S.; Lucas, A.; Birmaher, B.; Lorenzo, C.D.; Iyengar, S.; Brent, D.A. Recurrent abdominal pain, anxiety, and depression in primary care. Pediatrics 2004, 113, 817–824. [Google Scholar] [CrossRef] [Green Version]
- Dorn, L.D.; Campo, J.C.; Thato, S.; Dahl, R.E.; Lewin, D.; Chandra, R.; Di Lorenzo, C. Psychological comorbidity and stress reactivity in children and adolescents with recurrent abdominal pain and anxiety disorders. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 66–75. [Google Scholar] [CrossRef]
- Mulvaney, S.; Lambert, E.W.; Garber, J.; Walker, L.S. Trajectories of symptoms and impairment for pediatric patients with functional abdominal pain: A 5-year longitudinal study. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 737–744. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, N.R.; Lynch-Jordan, A.; Barnett, K.; Peugh, J.; Sil, S.; Goldschneider, K.; Kashikar-Zuck, S. Child pain catastrophizing mediates the relationship between parent responses to pain and disability in youth with functional abdominal pain. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 732. [Google Scholar] [CrossRef] [Green Version]
- Langer, S.L.; Romano, J.M.; Levy, R.L.; Walker, L.S.; Whitehead, W.E. Catastrophizing and parental response to child symptom complaints. Children Health Care 2009, 38, 169–184. [Google Scholar] [CrossRef] [Green Version]
- Simons, L.E.; Kaczynski, K.J. The Fear Avoidance model of chronic pain: Examination for pediatric application. Pain 2012, 13, 827–835. [Google Scholar] [CrossRef] [Green Version]
- Walker, L.S.; Levy, R.L.; Whitehead, W.E. Validation of a measure of protective parent responses to children’s pain. Clin. J. Pain 2006, 22, 712–716. [Google Scholar] [CrossRef] [Green Version]
- Hodges, K.; Kline, J.J.; Barbero, G.; Woodruff, C. Anxiety in children with recurrent abdominal pain and their parents. Psychosomatics 1985, 26, 859–866. [Google Scholar] [CrossRef]
- Logan, D.E.; Scharff, L. Relationships between family and parent characteristics and functional abilities in children with recurrent pain syndromes: An investigation of moderating effects on the pathway from pain to disability. J. Pediatr. Psychol. 2005, 30, 698–707. [Google Scholar] [CrossRef] [Green Version]
- Hodges, K.; Kline, J.J.; Barbero, G.; Flanery, R. Depressive symptoms in children with recurrent abdominal pain and in their families. J. Pediatr. 1985, 107, 622–626. [Google Scholar] [CrossRef]
- van Tilburg, M.A.; Levy, R.L.; Walker, L.S.; Von Korff, M.; Feld, L.D.; Garner, M.D.; Feld, A.; Whitehead, W.E. Psychosocial mechanisms for the transmission of somatic symptoms from parents to children. World J. Gastroenterol. 2015, 21, 5532–5541. [Google Scholar] [CrossRef]
- Cunningham, N.R.; Lynch-Jordan, A.; Mezoff, A.G.; Farrell, M.K.; Cohen, M.B.; Kashikar-Zuck, S. Importance of addressing anxiety in youth with functional abdominal pain: Suggested guidelines for physicians. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 469. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, N.R.; Jagpal, A.; Peugh, J.; Farrell, M.K.; Cohen, M.B.; Mezoff, A.G.; Lynch-Jordan, A.; Kashikar-Zuck, S. Risk categorization predicts disability in pain-associated functional gastrointestinal disorders (FGIDs) after 6 months. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 685–690. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, N.R.; Cohen, M.B.; Farrell, M.K.; Mezoff, A.G.; Lynch-Jordan, A.; Kashikar-Zuck, S. Concordant parent-child reports of anxiety predict impairment in youth with functional abdominal pain. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 312–317. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, N.R.; Jagpal, A.; Tran, S.T.; Kashikar-Zuck, S.; Goldschneider, K.; Coghill, R.C.; Lynch-Jordan, A.M. Anxiety adversely impacts response to cognitive behavioral therapy in children with chronic pain. J. Pediatr. 2016, 171, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Drossman, D.A. Functional gastrointestinal disorders: History, pathophysiology, clinical features, and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef] [Green Version]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21). Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef]
- Cunningham, N.R.; Jagpal, A.; Nelson, S.; Jastrowski Mano, K.E.; Tran, S.T.; Lynch-Jordan, A.M.; Hainsworth, K.; Peugh, J.; Mara, C.A.; Kashikar-Zuck, S. Clinical reference points for the screen for child anxiety–related disorders in 2 investigations of youth with chronic pain. Clin. J. Pain 2019, 35, 238–246. [Google Scholar] [CrossRef]
- Jastrowski Mano, K.E.; Evans, J.R.; Tran, S.T.; Anderson Khan, K.; Weisman, S.J.; Hainsworth, K.R. The psychometric properties of the screen for child anxiety related emotional disorders in pediatric chronic pain. J. Pediatr. Psychol. 2012, 37, 999–1011. [Google Scholar] [CrossRef] [Green Version]
- Claar, R.L.; Walker, L.S. Functional assessment of pediatric pain patients: Psychometric properties of the functional disability inventory. Pain 2006, 121, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Kashikar-Zuck, S.; Flowers, S.R.; Claar, R.L.; Guite, J.W.; Logan, D.E.; Lynch-Jordan, A.M.; Palermo, T.M.; Wilson, A.C. Clinical utility and validity of the Functional Disability Inventory among a multicenter sample of youth with chronic pain. Pain 2011, 152, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.; Huskisson, E.C. Vertical or horizontal visual analogue scales. Ann. Rheum. Dis. 1979, 38, 560. [Google Scholar] [CrossRef]
- Wendland, M.; Jackson, Y.; Stokes, L.D. Functional disability in paediatric patients with recurrent abdominal pain. Child Care Health Dev. 2010, 36, 516–523. [Google Scholar] [CrossRef]
- Brown, T.A.; Chorpita, B.F.; Korotitsch, W.; Barlow, D.H. Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behav. Res. Ther. 1997, 35, 79–89. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Cunningham, N.R.; Nelson, S.; Jagpal, A.; Moorman, E.; Farrell, M.; Pentiuk, S.; Kashikar-Zuck, S. Development of the Aim to Decrease Anxiety and Pain Treatment for Pediatric Functional Abdominal Pain Disorders. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 16–20. [Google Scholar] [CrossRef]
- Kendall, P.C. Treating anxiety disorders in children: Results of a randomized clinical trial. J. Consult. Clin. Psychol. 1994, 62, 100–110. [Google Scholar] [CrossRef]
- Walker, L.S.; Sherman, A.L.; Bruehl, S.; Garber, J.; Smith, C.A. Functional abdominal pain patient subtypes in childhood predict functional gastrointestinal disorders with chronic pain and psychiatric comorbidities in adolescence and adulthood. Pain 2012, 153, 1798–1806. [Google Scholar] [CrossRef] [Green Version]
- Lavigne, J.V.; Saps, M.; Bryant, F.B. Models of Anxiety, Depression, Somatization, and Coping as Predictors of Abdominal Pain in a Community Sample of School-Age Children. J. Pediatr. Psychol. 2013, 39, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Hollier, J.M.; van Tilburg, M.; Liu, Y.; Czyzewski, D.I.; Self, M.M.; Weidler, E.M.; Heitkemper, M.; Shulman, R.J. Multiple psychological factors predict abdominal pain severity in children with irritable bowel syndrome. Neurogastroenterol. Motil. 2019, 31, e13509. [Google Scholar] [CrossRef]
- Newton, E.; Schosheim, A.; Patel, S.; Chitkara, D.K.; van Tilburg, M.A.L. The role of psychological factors in pediatric functional abdominal pain disorders. Neurogastroenterol. Motil. 2019, 31, e13538. [Google Scholar] [CrossRef]


{kind=link}
| Race/Ethnicity Percentage | |
|---|---|
| Race | |
| Caucasian | 89% |
| African-American | 4.4% |
| Biracial | 3.3% |
| American Indian/Alaskan Native | 2.2% |
| Other | 1.1% |
| Ethnicity | |
| Latino/Hispanic | 3.3% |
| Range | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. VAS | 0–10 | 3.8 | 16.2 | - | 0.19 | 0.27 * | −0.01 | −0.01 | −0.07 | 0.19 | 0.12 |
| 2. CSI | 0–140 | 32.7 | 16.2 | 0.19 | - | 0.04 | 0.09 | 0.22* | 0.13 | 0.36 ** | 0.09 |
| 3. FDI | 0–60 | 18.2 | 8.5 | 0.27 * | 0.04 | - | 0.12 | 0.15 | 0.18 | 0.21 * | 0.21 * |
| 4. DASS Dep | 0–14+ | 3.3 | 3.8 | −0.01 | 0.09 | 0.12 | - | 0.70 ** | 0.61 ** | 0.13 | 0.26 * |
| 5. DASS Anx | 0–10+ | 3.4 | 4.1 | −0.01 | 0.22 * | 0.15 | 0.70 ** | - | 0.67 ** | 0.25 * | 0.19 |
| 6. DASS Stress | 0–17+ | 6.6 | 4.4 | −0.07 | 0.13 | 0.18 | 0.61 ** | 0.67 ** | - | 0.17 | 0.13 |
| 7. SCARED | 0–82 | 34.6 | 16.8 | 0.19 | 0.36 ** | 0.21 * | 0.13 | 0.25 * | 0.17 | - | 0.04 |
| 8. Age | 9–14 | 11.6 | 1.74 | 0.12 | 0.09 | 0.21 * | 0.26 * | 0.19 | 0.13 | 0.04 | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Love, S.C.; Mara, C.A.; Kalomiris, A.E.; Cunningham, N.R. The Influence of Caregiver Distress and Child Anxiety in Predicting Child Somatization in Youth with Functional Abdominal Pain Disorders. Children 2019, 6, 134. https://0-doi-org.brum.beds.ac.uk/10.3390/children6120134
Love SC, Mara CA, Kalomiris AE, Cunningham NR. The Influence of Caregiver Distress and Child Anxiety in Predicting Child Somatization in Youth with Functional Abdominal Pain Disorders. Children. 2019; 6(12):134. https://0-doi-org.brum.beds.ac.uk/10.3390/children6120134
Chicago/Turabian StyleLove, Sarah C., Constance A. Mara, Anne E. Kalomiris, and Natoshia R. Cunningham. 2019. "The Influence of Caregiver Distress and Child Anxiety in Predicting Child Somatization in Youth with Functional Abdominal Pain Disorders" Children 6, no. 12: 134. https://0-doi-org.brum.beds.ac.uk/10.3390/children6120134