Optimal Inspired Fraction of Oxygen in the Delivery Room for Preterm Infants
by
 ,
,
Inmaculada Lara-Cantón
1, 
Alvaro Solaz
1,
Anna Parra-Llorca
1,
Ana García-Robles
1 and
Máximo Vento
1,2,* 1
Neonatal Research Group, Health Research Institute La Fe, Avenida Fernando Abril Martorell 106, 46026 Valencia, Spain
2
Division of Neonatology, University and Polytechnic Hospital La Fe, Avenida Fernando Abril Martorell 106, 46026 Valencia, Spain
*
Author to whom correspondence should be addressed.
Children 2019, 6(2), 29; https://0-doi-org.brum.beds.ac.uk/10.3390/children6020029
Submission received: 29 January 2019
/
Revised: 13 February 2019
/
Accepted: 18 February 2019
/
Published: 19 February 2019
(This article belongs to the Special Issue Emerging Concepts in Neonatal Resuscitation)
Abstract
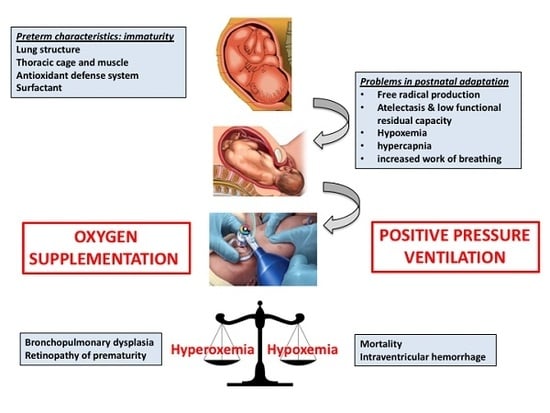
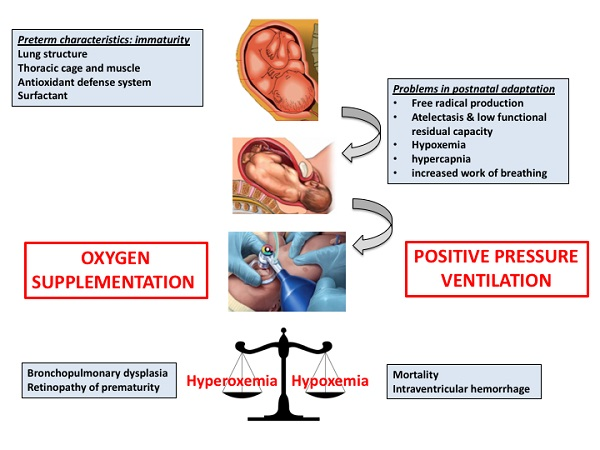
:Postnatal adaptation of preterm infants entails a series of difficulties among which the immaturity of the respiratory system is the most vital. To overcome respiratory insufficiency, caregivers attending in the delivery room use positive pressure ventilation and oxygen. A body of evidence in relation of oxygen management in the delivery room has been accumulated in recent years; however, the optimal initial inspired fraction of oxygen, the time to achieve specific oxygen saturation targets, and oxygen titration have not been yet clearly established. The aim of this review is to update the reader by critically analyzing the most relevant literature.
1. Introduction
Lung cytoarchitecture, thoracic cage structure, and muscular strength only mature late in gestation [1]. Moreover, metabolic components that essentially contribute to an effective respiration, such as surfactant and antioxidant enzymatic and non-enzymatic defenses, are not produced in sufficient quantity until the last weeks of gestation [2]. Consequently, preterm infants, and especially very preterm infants with gestational ages below 32 weeks, frequently undergo respiratory difficulties immediately after birth. Generalized atelectasis, inability to establish a functional residual capacity, hypoxemia, hypercapnia, and increased work of breathing are the clinical characteristics that describe the respiratory failure of preterm infants when initiating air breathing. Under these circumstances, prenatal interventions such as the administration to the mother of antenatal steroids, and postnatal ventilation and oxygen supplementation to the newborn preterm infants render essential to overcome this dramatic situation [3]. The benefits of antenatal steroids and postnatal non-invasive ventilation in the delivery room (DR) have been widely acknowledged. Nonetheless, despite the generalized acceptance of oxygen as the most important drug for preterm resuscitation, there are still relevant aspects in the management of oxygen that are yet to be answered. Hence, the preferred initial inspired fraction of oxygen (FiO2), the oxygen saturation (SpO2) target ranges along the first minutes after birth, and how to perform the adjustments to increase or decrease FiO2 along stabilization still require further evidence. There is an inherent risk to using inappropriate oxygen concentrations in very preterm infants. Oxygen in excess causing hyperoxemia leads to an enhanced production of oxygen free radicals, oxidative stress, and tissue damage in preterm babies with an immature antioxidant defense system [2]. On the contrary, hypoxemia especially when combined with bradycardia significantly enhances the risk for intraventricular hemorrhage (IVH) and death. Both these situations increase mortality and/or short-long term morbidities in survivors [4].
The aim in the present review article is to critically analyze the most relevant and recent literature concerning the use of oxygen in the DR to help neonatologists improving the management of preterm infants during postnatal stabilization.
2. Oxygen in the Fetal to Neonatal Transition
Fetal life elapses in a low oxygen environment as compared to the extrauterine environment. The arterial partial pressure of oxygen in utero is about 25–30 mmHg as compared to 80–90 mmHg in the mother [5]. Of note, the most oxygenated fetal blood is directed through circulatory shunts to the brain and myocardium which are the two most oxygen demanding tissues [6]. Initiation of breathing immediately after birth triggers profound cardiorespiratory and metabolic changes. Lung expansion with the initial inspiratory movements and extrusion of lung fluid from the respiratory airways and alveoli to the interstitium contributes to dilatation of the lung vasculature, drop of the vascular resistance, closure of the intra-and-extra-cardiac shunting, and redirecting of the ventricular output to the lungs, where it gets oxygenated [7]. PaO2 rises abruptly to 70–80 mmHg in the first 5–10 min after birth. Arterial oxygen saturation (SpO2) reflects the percentage of hemoglobin that is saturated with oxygen. Under physiologic circumstances SpO2 range oscillates between 95% and 100% in newborn infants [7].
What is the timing for postnatal SpO2 stabilization? Dawson et al. merged three different data bases from term and preterm newborn infants who did not need resuscitation or oxygen supplementation upon stabilization. With these data they assembled an oxygen saturation range graph with centiles for term and preterm babies for the first 10 min after birth [8]. Reference ranges for term infants have been adopted by international guidelines to establish target SpO2 recommendations minute by minute. Thus, recommended range for SpO2 at 1 min 60–65%, 2 min 65–70%, 3 min 70–75%, 4 min 75–80%, 5 min 80–85% and 10 min 85–95% [9]. However, the reference ranges for preterm infants were based on a population mainly composed by late preterm infant (33+6 to 36+6 weeks gestation) with very little representation of very preterm infants [10]. Interestingly, very preterm infants using positive pressure ventilation with air achieved significantly earlier Dawson’s nomogram SpO2 targets introducing an additional confounder for the clinician [11].
Oei et al. launched an international survey to determine current clinical practice and opinions regarding FiO2 and SpO2 targets for DR resuscitation of very preterm infants [12]. The majority of neonatologists (77%) who participated in the survey would target SpO2 between the 10th and 50th percentiles of the reference range for full-term infants [8], and would choose to start with an initial FiO2 0.3; however, most of the interviewed neonatologists acknowledged that evidence was lacking and further research is needed [12].
3. Initial FiO2 in the Delivery Room
In 2015, the International Liaison Committee on Resuscitation [15], American Heart Association (AHA) [9], and the European Resuscitation Council (ERC) [16], strongly recommended to initiate resuscitation of preterm infants with an FiO2 between 0.21 and 0.30, although evidence showed that no differences in clinical outcomes were present when initiating resuscitation either with lower (<0.3) or higher (>0.6) initial FiO2. However, criticism arose as neither of the recommendations included relevant studies that reported an increased mortality and morbidity, especially in extremely preterm infants (≤28 weeks’ gestation), when stabilization was initiated with air [17]. Hence, while a meta-analysis published in 2014 by Saugstad et al. [18], had shown that preterm babies ≤32 weeks’ gestation resuscitated with lower (0.21–0.3) versus higher (0.6–1.0) initial FiO2 showed no differences in morbidity but exhibited an almost significant trend towards reduced mortality [18], both the TORPIDO trial from Australia/New Zealand/Malaysia [19] and the Neonatal Network in Canada [20] reported increased mortality in very preterm babies initially stabilized with air. The results of the TORPIDO trial [19] showed in 289 preterm infants <32 weeks’ gestation that the mortality in a subgroup of babies <29 weeks’ gestation (16.2%) was significantly increased as compared with the mortality (6%) in the pure oxygen group (p = 0.013). Rabi et al. [20], in a retrospective study, compared the results of babies ≤27 weeks’ gestation from the Canadian Neonatal Network before and after 2006 when the initial FiO2 was changed from 1.0 to <1.0 with the primary outcome being severe neurologic injury or death. Adjusted odds ratio for the primary outcome was significantly higher in the lower oxygen group (AOR 1.36; 95% CI 1.11–1.66) and in those resuscitated with RA (AOR 1.33; 95% CI 1.04–1.69), when compared with 100% oxygen [20]. These studies [19,20] underpinned the necessity of performing in depth analysis of the available information and the stringent necessity to launch adequately designed and powered studies to overcome the uncertainty about the use of oxygen in the DR in these very vulnerable infants.
Welsford et al. recently published a systematic review and meta-analysis summarizing the available evidence for the FiO2 used to initiate resuscitation of preterm infants who require positive pressure ventilation in the DR [21]. Data pertained to 10 randomized/quasi randomized controlled and 4 retrospective observational cohort studies—including a total of 5697 preterm infants <35 weeks’ gestation. The use of higher (≥0.5) or lower (<0.5) initial FiO2 did not report benefit or harm in the primary outcome of short-term mortality (risk ratio (RR) 0.83, 95% confidence interval (CI) 0.50–1.37), long-term mortality, neurodevelopmental impairment, or other morbidities [21]. The results of this study should be interpreted cautiously. The study encompasses from 1980 to 2018 and includes a wide range of different designs and gestational ages. Finally, it also has included studies performed with enormous differences in the technology employed in the DR, especially pulse oximetry and air/oxygen blender. The authors confirmed that the study has important limitations especially due to the risk of bias and imprecision and conclude that the ideal initial FiO2 for preterm infants it yet unknown despite the fact that many of these infants will require oxygen supplementation upon stabilization in the DR [21].
Almost simultaneously, a Cochrane systematic review has analyzed lower (<0.4) vs. higher (≥0.4) initial FiO2 titrated to target oxygen saturations during resuscitation of preterm infants [22]. The search included only randomized controlled trials and the study period was also shorter (2008–2016). Interestingly, in each of these studies SpO2 and heart rate were monitored and FiO2 titrated according to targeted saturations. No differences in mortality between both groups could be assessed (RR 1.05, 95% CI 0.68–1.63). However, the quality of evidence was graded as low due to risk of bias and imprecision [22]. No differences were shown in other relevant outcomes such as ROP, PVL, IVH, NEC, BPD or PAD. The authors concluded that there is uncertainty as to whether the use of higher or lower initial FiO2 affects short or long-term outcomes in preterm infants [22]. Clinical studies have shown that very preterm infants have difficulty achieving adequate oxygenation in the first minutes after birth when supplemented with room air. In a preterm lamb model of asphyxia/resuscitation using FiO2, 0.21 did not reduce pulmonary vascular resistance as compared to FiO2 of 1.0 [23]. On the contrary, the use of 100% oxygen caused hyperoxemia detected in the carotid arteries but did not cause cerebral vasoconstriction; however, cerebral oxygen extraction did not differ between groups [23]. Very preterm infants need higher FiO2 than term infants to dilate the pulmonary vessels and avoid hypoxemia and/or bradycardia; notwithstanding, the risk of cerebral hyperoxia and subsequent brain damage should be avoided using intermediate inspired fractions of oxygen, closely titrating SpO2 [23]. The use of near infrared spectroscopy (NIRS) in the delivery room allows to monitor evolving cerebral regional oxygen saturation and fraction of oxygen extraction rapidly and accurately after birth. Brain oxygenation measured by NIRS reaches a plateau much faster than arterial oxygen saturation. Cerebral tissue oxygenation relies not only in arterial oxygen saturation but also in cerebral blood flow, hemoglobin content and oxygen consumption. Thus, with the information provided by NIRS oxygen targeting especially in the first minutes after birth can be more accurately achieved and cerebral hyper-or-hypoxia more easily avoided [24,25].
4. Target Oxygen Saturation during Stabilization
AHA 2015 guidelines recommend that FiO2 should be titrated according to pre-established saturation targets from spontaneously breathing, full-term infants [9]. Despite this recommendation, SpO2 is not routinely registered as complementary information to the Apgar score. A prospective observational study, however, showed that reflecting objective information during postnatal stabilization, the so-called expanded Apgar score, would not only better reflect the process of adaptation but also it would better predict early and late clinical outcomes [26]. In individual patient data from 768 infants <32 weeks’ gestation enrolled in 8 RCTs, infants who did not reach a SpO2 80% by 5 min were more likely to develop a severe intraventricular hemorrhage (OR 2.04, 95% CI 1.01–4.11) and die (OR 4,.57, 95% CI 1.62–13.98) compared to infants with SpO2 >80% [27]. Infants were also less likely to reach SpO2 80% if resuscitation was commenced with lower (≤0.3) FiO2 instead of higher (>0.6) FiO2 (OR 2.63, 95% CI 1.21–5.74) were more premature and had lower birth weight [27]. Similarly, Thamrin et al. [28] reported the results of a follow up study at 2–3 years corrected age of preterm babies born at <32 weeks’ gestation and resuscitated with FiO2 or either 0.21 or 1.0. They found no differences in Bayley Scales independently of the initial FiO2 employed. Interestingly, in a post hoc exploratory analysis of the entire cohort, babies who did not reach SpO2 80% at five minutes after birth were more likely to die or have neurodevelopmental impairment (OR, 1.85; 95% CI 1.07–3.2; P = 0.03). From the results of these studies [27,28], it may be deduced that more than starting with a specific FiO2, performing an adequate ventilation and oxygen titration that allows the patient reaching a specific SpO2 at a given time point after birth has a notable influence on major outcomes. Inability to do so could be informing about prenatal complications in utero or inadequate resuscitation. Thus, SpO2 at 5 min after birth should be registered together with the 5 min Apgar score. Moreover, it should have an influence on the pace of FiO2 adjustments to reach the SpO2 target. Babies who do not reach 80–85% saturation around 5 min should be considered at high risk of severe complications and must be closely monitored.
5. Heart Rate
Myocardial function is indispensable for an adequate tissue perfusion and oxygenation. Cardiac output is the result of stroke volume and heart rate. Cardiac function is highly dependent on aerobic metabolism. Coronary blood flow is regulated by arterial blood oxygen content. Therefore, under hypoxemic conditions myocardium suffers hypoperfusion and energy exhaustion which lead to bradycardia and generalized hypoperfusion and hypoxemia [29]. Heart rate is therefore the most critical sign for an adequate response to resuscitation maneuvers. Monitoring heart rate (HR) even if SpO2 monitoring is not available may be highly informative. The Bradyprem study [30] is a multicenter retrospective study that retrieved data from 596 infants <32 weeks’ gestation from 8 RCT of higher (>0.6) vs. lower (≤0.3) FiO2. The study aimed to determine if there was an association between bradycardia and neonatal morbidity and mortality during stabilization in preterm infants during the first 10 min after birth. In addition, the study also aimed to conclude if there was an interaction between prolonged bradycardia and low SpO2 during resuscitation [30]. The primary outcome was in-hospital mortality and secondary outcomes were intraventricular hemorrhage (IVH, ≥grade 3), bronchopulmonary dysplasia (BPD) and retinopathy of prematurity (ROP, ≥grade 3). Results showed that 38% of babies in the DR experienced prolonged bradycardia (HR <100 bpm for >2 minutes). These babies were more likely to have 5 min SpO2 <80%, and more likely to die and/or to have IVH. Duration of bradycardia was associated with higher mortality even after adjusting for confounders such as gestational age, birth weight, gender, antenatal steroids, SpO2 at 5 min <80% and individual study variability. An accurate and continuous measurement of HR during neonatal resuscitation is critical and evaluation of long-term outcomes of patients who experienced prolonged bradycardia in the first 10 min after birth are paramount [30].
6. Follow-Up
The long-term consequences of hypoxia and/or hyperoxia during postnatal stabilization have only been recently studied. As shown in recent meta-analyses [21,22] follow-up studies of babies resuscitated with different initial FiO2 rates are relatively scarce. However, it is well-known that both hypoxia and hyperoxia can directly cause neuronal necrosis and/or activate pro-inflammatory and pro-apoptotic pathways causing deleterious effects on the developing brain [31]. Soraisham et al. [32] performed a retrospective cohort study that included 1509 preterm infants <29 weeks’ gestation resuscitated either with room air, intermediate oxygen concentration or 100% oxygen with the primary outcome being death or neurodevelopmental impairment (NDI). The results showed no differences for the composite outcome of death or severe NDI between the groups. However, the odds of severe NDI among survivors were significantly higher in infants that received 100% oxygen as compared to room air (aOR 1.57, 95% CI 1.05, 2.35) indicating that the use of pure oxygen could be damaging for the central nervous system in those babies who survived the neonatal period [32]. Similarly, Kapadia et al. [33], in a retrospective observational study, compared the impact of changing FiO2 from 1.0 to 0.21 introduced in 2011 in the Neonatal Resuscitation Program of his institution upon neonatal morbidities, mortality and neurodevelopmental outcomes in preterm infants. The results showed that babies resuscitated with a low oxygen approach had lower oxygen exposure, spent fewer days on oxygen, and had lower odds of developing BPD. Mortality was no different between groups; however, survivors of the air group had greater motor composites scores on Bayley III Scales [33] confirming results obtained in Canada by Shoraisham et al. [32]. Finally, Boronat et al. [34] included a total of 253 surviving preterm infants <32 weeks’ gestation from two randomized, double blinded, international, multicenter clinical trials in which patients were assigned to higher (0.6 or 0.65) or lower (0.3) initial FiO2 in the DR. A total of 206 (81.4%) completed follow up at 24 months that included Bayley III Scales comprehensive scoring, visual acuity, neurosensory deafness, and language skills. No differences in survival or NDI were found between both groups [34]. Results from follow up studies show that using an initial FiO2 of 1.0 increases the chance of NDI in survivors. However, when using initial FiO2 of 0.6–0.65 as shown in Boronat’s paper [34] no differences in neurocognitive or sensorial outcomes were present.
From the results shown in the follow up studies it may be deduced that the oxygen load defined as the amount of pure oxygen expressed in mL/kg body weight supplied to preterm infants during resuscitation causes a long-term impact on NDI. Oxygen load is highly dependent on gestational age, type of birth and gender and especially on initial FiO2 and titration protocols [35]. Moreover, the amount of oxygen provided immediately after birth significantly influenced DNA methylation causing hypomethylation of a significant number of genes related with cell cycle progression, DNA repair, and oxidative stress [36]. We can only speculate if oxygen load is responsible at least partially for long-term clinical outcomes.
7. Clinical Practice
Evidence based knowledge and clinical practice do not always run in parallel. While the scientific approach has not yet determined the optimal oxygen inspired fraction and the ideal procedure to titrate oxygen in the DR, the clinical practice has highly inclined the plate towards a lower initial FiO2 during postnatal stabilization. Avoiding hyperoxia-derived oxidative stress and its consequences has had a higher impact than hypoxemia during the first minutes after birth which seems to be a transitory physiological status especially for very preterm infants especially if the baby keeps a HR >100 bpm after two minutes after birth. Thereafter, titrating FiO2 always avoiding SpO2 >96% is the experts’ recommendation to avoid damage caused by hyperoxia [37]. In a survey performed among 630 clinicians from 25 countries the majority (77%) would target SpO2 between the 10th and 50th percentiles values for term infants as shown in the AHA 2015 guidelines [9] and expressed their preference for the use of 0.3–0.4 or even lower initial FiO2 (0.21) for preterm infants in the DR. Of note, a substantial number of responders agreed that there was a gap of knowledge and further studies would need to be performed [12]. More recently, a review of the guidelines for oxygen use in the DR in 45 different countries showed a great variability regarding gestational ages, initial FiO2 and SpO2 targets [38]. Initial FiO2 recommendations ranged from 0.21–1.0; however, the most frequently recommended were 0.21–0.3 (38%), 0.3 (20%) and 0.21 (18%). Differences in target SpO2 at five minutes were notably different between countries. Therefore, while Scandinavian countries recommended 70%, other countries such as New Zealand or Australia recommended 90% and some countries did not make any recommendation [38]. Another relevant question is around the adherence to guidelines. As expressed by Farquhar et al., although clinicians rely on guidelines as a good educational tool they considered them too rigid for a specific patient and limit physician’s own clinical choice [39]. In addition, the permeation of national guidelines is also highly dependent on the clinical level of the hospital. Thus, care givers in smaller countryside hospitals tend to substantially delay the application of new standards of care especially if they imply the use of novel technical devices, such as air/oxygen blenders, pulse oximeters or T-piece resuscitators. Hence, countryside hospitals significantly delayed the use of oxygen blenders for FiO2 titration and the systematic use of pulse oximeters when attending preterm infants in the DR as compared with level III reference regional centers as shown in the survey performed in Spain by Iriondo et al. [40].
8. Seeking an Answer: Forthcoming Trials
Meta-analyses and systematic reviews performed in the last few years, as shown in Section 3 and Section 4, have not been able to shed light on the optimal use of oxygen in preterm infants in the delivery room. Striking differences in favor of initiating resuscitation with higher (even 100%) oxygen, intermediate (60%) or lower (21–30%) have been concluded. The small size, differences in gestational ages, and varied designs and primary objectives, among other things, have led to different conclusions generating confusion among clinicians. To overcome this conundrum, large multicenter trials of sufficient sample size powered to look at safety outcomes such as mortality and/or major neurodevelopmental impairment are needed. The HiLo trial (NCT03825835) aims to answer if higher (60%) or lower (30%) initial oxygen concentration has an impact on patient relevant outcomes in preterm infants of 230 to 28+6 weeks’ gestation. The null hypothesis is that neither mortality or NDI at 18–24 months corrected age will be different independently of the initial FiO2 employed. The study has a cluster crossover design, unmasked randomized controlled trial comparing two oxygen concentration at initiation of resuscitation. Hence, NICUs instead of infants will be randomized to an initial FiO2’s (e.g., higher) until several babies are recruited, and then switched to the other FiO2 (i.e., lower). The analysis will be conducted using an “intention-to-treat” approach. Interestingly, SpO2 will be controlled at 3 min after birth and according to the oxygen saturation increased or decreased by 20% every 60 seconds to achieve ≥85% between 5–10 min of age. A second study, the Torpido 30/60 (ACTRN12618000879268) trial, compares initial FiO2 of 0.3 vs. 0.6. This is a phase III, randomized, 2 parallel arms, non-blinded trial in preterm infants 23+0 to 28+6 weeks’ gestation. The aim of this study is to compare short-and-long term outcomes being the primary outcome survival free of major brain injury at 36 weeks, and secondary outcomes mortality and major brain injury. Eligible babies will be randomized to FiO2 of 0.3 or 0.6 before birth. Importantly, target SpO2 at five minutes should be 80–85% and at 10 min and after 85–95%. Both, the HiLo and Torpido 30/60 have been powered to detect an absolute risk difference around 10% in the primary endpoint. Both these ongoing trials seek answering many of the question’s neonatologists have to face when confronted with the resuscitation of very preterm infants.
9. Conclusions
A body of evidence for the field of newborn oxygenation has been accumulated. However, there is increasing awareness that more reliable data are needed. The tendency towards a reduction in the amount of oxygen given to newborn infants, especially very preterm, upon stabilization in the delivery room is an inarguable fact. The benefit of this clinical tendency is still under debate. The need of very preterm infants for some amount of oxygen and the risk of not overcoming bradycardia and hypoxemia and blunt the stimulation of the respiratory center to open the glottis with deleterious consequences upon the myocardium and central nervous system should be a matter of great concern. Published data reveal that very preterm infants but especially <28 weeks’ gestation will need supplemental oxygen in the first minutes after birth to overcome the tendency towards hypoxemia. Strict control of heart rate is mandatory because persistence of bradycardia is an ominous sign and highly predictive of death or major morbidities. Saturation at five minutes should be included together with the 5-minute Apgar score in the electronic registry of every baby. In addition, follow up is recommended for babies who had prolonged bradycardia and desaturation during postnatal adaptation independently of gestational age. Finally, suggestions for the use of oxygen in the delivery room in the first ten minutes after birth as an adaptation of a recent review publication of experts in the field [31] is shown in Table 1.
Author contributions
I.L.-C. conceptualized the manuscript and wrote the manuscript draft; A.S., A.P.-L. and A.G.-R. updated and critically analyzed the literature; M.V. conceptualized the manuscript, supervised the draft version, and approved the final version of the manuscript.
Funding
M.V. acknowledges FIS PI17/0131 grant from the Instituto de Investigación Sanitaria Carlos III (Ministry of Science, Innovation and Universities; Kingdom of Spain). I.L.-C. acknowledges predoctoral fellowship from the Health Research Institute La Fe. Both A.P.-L. and A.G.-R. acknowledge Rio Hortega grants CM18/0165 and CM16/0174 respectively, from the Instituto de Investigación Sanitaria Carlos III (Ministry of Science, Innovation and Universities; Kingdom of Spain).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Alphonse, R.S.; Rajabali, S.; Thébaud, B. Lung injury in preterm neonates: The role and therapeutic potential of stem cells. Antioxid. Redox Signal. 2012, 17, 1013–1040. [Google Scholar] [CrossRef] [PubMed]
- Vento, M.; Aguar, M.; Escobar, J.; Arduini, A.; Escrig, R.; Brugada, M.; Izquierdo, I.; Asensi, M.A.; Sastre, J.; Saenz, P.; et al. Antenatal steroids and antioxidant enzyme activity in preterm infants: Influence of gender and timing. Antioxid. Redox Signal. 2009, 11, 2945–2955. [Google Scholar] [CrossRef] [PubMed]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Plavka, R.; Saugstad, O.D.; Simeoni, U.; Speer, C.P.; Vento, M.; et al. European consensus guidelines on the management of respiratory distress syndrome—2016 Update. Neonatology 2017, 111, 107–125. [Google Scholar] [CrossRef] [PubMed]
- Torres-Cuevas, I.; Cernada, M.; Nuñez, A.; Escobar, J.; Kuligowski, J.; Chafer-Pericas, C.; Vento, M. Oxygen supplementation to stabilize preterm infants in the fetal to neonatal transition: No satisfactory answer. Front. Pediatr. 2016, 4, 29. [Google Scholar] [CrossRef]
- Vento, M.; Teramo, K. Evaluating the fetus at risk for cardiopulmonary compromise. Semin. Fetal Neonatal Med. 2013, 18, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Vali, P.; Lakshminrusimha, S. The fetus can teach us: Oxygen and the pulmonary vasculature. Children 2017, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Raj, J.U. Regulation of the pulmonary circulation in the fetus and newborn. Physiol. Rev. 2010, 90, 1291–2010. [Google Scholar] [CrossRef]
- Dawson, J.A.; Kamlin, C.O.; Vento, M.; Wong, C.; Cole, T.J.; Donath, S.M.; Davis, P.G.; Morley, C.J. Defining the reference range for oxygen saturation for infants after birth. Pediatrics 2010, 125, e1340–e1347. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Aziz, K.; Escobedo, M.B.; Kapadia, V.S.; Kattwinkel, J.; Perlman, J.M.; Simon, W.M.; Weiner, G.M.; Zaichkin, J.G. Part 13: Neonatal resuscitation: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132, S543–S560, Suppl. 2. [Google Scholar] [CrossRef]
- Vento, M.; Escobar, J.; Cernada, M.; Escrig, R.; Aguar, M. The use and misuse of oxygen during the neonatal period. Clin Perinatol. 2012, 39, 165–176. [Google Scholar] [CrossRef]
- Vento, M.; Cubells, E.; Escobar, J.J.; Escrig, R.; Aguar, M.; Brugada, M.; Cernada, M.; Saénz, P.; Izquierdo, I. Oxygen saturation after birth in preterm infants treated with continuous positive airway pressure and air: Assessment of gender differences and comparison with a published nomogram. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F228–F232. [Google Scholar] [CrossRef] [PubMed]
- Oei, J.L.; Ghadge, A.; Coates, E.; Wright, I.M.; Saugstad, O.D.; Vento, M.; Buonocore, G.; Nagashima, T.; Suzuki, K.; Hosono, S.; et al. Clinicians in 25 countries prefer to use lower levels of oxygen to resuscitate preterm infants at birth. Acta Paediatr. 2016, 105, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Anton, O.; Jordan, H.; Rabe, H. Strategies for implementing placental transfusion at birth: A systematic review. Birth 2018. [Google Scholar] [CrossRef] [PubMed]
- Katheria, A.; Hosono, S.; El-Naggar, W. A new wrinkle: Umbilical cord management (how, when, who). Semin. Fetal Neonatal Med. 2018, 23, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Wyckoff, M.H.; Aziz, K.; Guinsburg, R.; Kim, H.S.; Liley, H.G.; Mildenhall, L.; Simon, W.M.; et al. Part 7: Neonatal resuscitation: 2015 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 2015, 132, S204–S241, Suppl. 1. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, J.; Bruinenberg, J.; Roehr, C.C.; Rüdiger, M.; Trevisanuto, D.; Urlesberger, B. European Resuscitation Council guidelines for resuscitation 2015: Section 7. Resuscitation and support of transition of babies at birth. Resuscitation 2015, 95, 249–263. [Google Scholar] [CrossRef] [PubMed]
- Vento, M.; Schmölzer, G.; Cheung, P.Y.; Finer, N.; Solevåg, A.L.; Oei, J.L.; Saugstad, O.D. What initial oxygen is best for preterm infants in the delivery room?-A response to the 2015 neonatal resuscitation guidelines. Resuscitation 2016, 101, e7–e8. [Google Scholar] [CrossRef]
- Saugstad, O.D.; Aune, D.; Aguar, M.; Kapadia, V.; Finer, N.; Vento, M. Systematic review and meta-analysis of optimal initial fraction of oxygen levels in the delivery room at ≤32 weeks. Acta Paediatr. 2014, 103, 744–751. [Google Scholar] [CrossRef]
- Oei, J.L.; Saugstad, O.D.; Lui, K.; Wright, I.M.; Smyth, J.P.; Craven, P.; Wang, Y.A.; McMullan, R.; Coates, E.; Ward, M.; et al. Targeted oxygen in the resuscitation of preterm infants, a randomized clinical trial. Pediatrics 2017, 139, e20161452. [Google Scholar] [CrossRef]
- Rabi, Y.; Lodha, A.; Soraisham, A.; Singhal, N.; Barrington, K.; Shah, P.S. Outcomes of preterm infants following the introduction of room air resuscitation. Resuscitation 2015, 96, 252–259. [Google Scholar] [CrossRef]
- Welsford, M.; Nishiyama, C.; Shortt, C.; Weiner, G.; Roehr, C.C.; Isayama, T.; Dawson, J.A.; Wyckoff, M.H.; Rabi, Y. International Liaison Committee on Resuscitation Neonatal Life Support Task Force. Initial oxygen use for preterm newborn resuscitation: A systematic review with meta-analysis. Pediatrics 2019, 143, e20181828. [Google Scholar] [CrossRef] [PubMed]
- Lui, K.; Jones, L.J.; Foster, J.P.; Davis, P.G.; Ching, S.K.; Oei, J.L.; Osborn, D.A. Lower versus higher oxygen concentrations titrated to target oxygen saturations during resuscitation of preterm infants at birth. Cochrane Database Syst. Rev. 2018, 5, CD010239. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekharan, P.; Rawat, M.; Gugino, S.F.; Koenigsknecht, C.; Helman, J.; Nair, J.; Vali, P.; Lakshminrusimha, S. Effect of various inspired oxygen concentrations on pulmonary and systemic hemodynamics and oxygenation during resuscitation in a transitioning preterm model. Pediatr. Res. 2018, 84, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Pichler, G.; Urlesberger, B.; Balk, N.; Schwaberger, B.; Binder-Heschl, C.; Avian, A.; Pansy, J.; Cheung, P.Y.; Schmölzer, G.M. Cerebral oxygen saturation to guide oxygen delivery in preterm neonates for the immediate transition after birth: A 2-center randomized controlled pilot feasibility trial. J. Pediatr. 2016, 170, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Pichler, G.; Schmölzer, G.M.; Urlesberger, B. Cerebral tissue oxygenation during immediate neonatal transition and resuscitation. Front. Pediatr. 2017, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Rüdiger, M.; Braun, N.; Aranda, J.; Aguar, M.; Bergert, R.; Bystricka, A.; Dimitriou, G.; El-Atawi, K.; Ifflaender, S.; Jung, P.; et al. Neonatal assessment in the delivery room--Trial to evaluate a specified type of apgar (TEST-Apgar). BMC Pediatr. 2015, 15, 18. [Google Scholar] [CrossRef] [PubMed]
- Oei, J.L.; Finer, N.N.; Saugstad, O.D.; Wright, I.M.; Rabi, Y.; Tarnow-Mordi, W.; Rich, W.; Kapadia, V.; Rook, D.; Smyth, J.P.; et al. Outcomes of oxygen saturation targeting during delivery room stabilisation of preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F446–F454. [Google Scholar] [CrossRef] [PubMed]
- Thamrin, V.; Saugstad, O.D.; Tarnow-Mordi, W.; Wang, Y.A.; Lui, K.; Wright, I.M.; De Waal, K.; Travadi, J.; Smyth, J.O.; Craven, P.; et al. Preterm infant outcomes after randomization to initial resuscitation with FiO2 0.21 or 1.0. J. Pediatr. 2018, 201, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Goodwill, A.G.; Dick, G.M.; Kiel, A.M.; Tune, J.D. Regulation of coronary blood flow. Compr. Physiol. 2017, 7, 321–382. [Google Scholar] [PubMed]
- Kapadia, V.S.; Oei, J.L.; Saugstad, O.D.; Rabi, Y.; Finer, N.N.; Tarnow-Mordi, W.; Rich, W.; Rook, D.; Vermeulen, M.; Smyth, J.; et al. BradyPrem study: Heart rate is the most vital signs during resuscitation of preterms. 2019; Unpublished work. [Google Scholar]
- Saugstad, O.D.; Oei, J.L.; Lakshminrusimha, S.; Vento, M. Oxygen therapy of the newborn from molecular understanding to clinical practice. Pediatr. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Soraisham, A.S.; Rabi, Y.; Shah, P.S.; Singhal, N.; Synnes, A.; Yang, J.; Lee, S.K.; Lodha, A.K. Neurodevelopmental outcomes of preterm infants resuscitated with different oxygen concentration at birth. J. Perinatol. 2017, 37, 1141–1147. [Google Scholar] [CrossRef]
- Kapadia, V.S.; Lal, C.V.; Kakkilaya, V.; Heyne, R.; Savani, R.C.; Wyckoff, M.H. Impact of the neonatal resuscitation program-Recommended low oxygen strategy on outcomes of infants born preterm. J. Pediatr. 2017, 191, 35–41. [Google Scholar] [CrossRef]
- Boronat, N.; Aguar, M.; Rook, D.; Iriondo, M.; Brugada, M.; Cernada, M.; Nuñez, A.; Izquierdo, M.; Cubells, E.; Martinez, M.; et al. Survival and neurodevelopmental outcomes of preterms resuscitated with different oxygen fractions. Pediatrics 2016, 138, e20161405. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, V.S.; Chalak, L.F.; Sparks, J.E.; Allen, J.R.; Savani, R.C.; Wyckoff, M.H. Resuscitation of preterm neonates with limited versus high oxygen strategy. Pediatrics 2013, 132, e1488–e1496. [Google Scholar] [CrossRef] [PubMed]
- Lorente-Pozo, S.; Parra-Llorca, A.; Núñez-Ramiro, A.; Cernada, M.; Hervás, D.; Boronat, N.; Sandoval, J.; Vento, M. The oxygen load supplied during delivery room stabilization of preterm infants modifies the DNA methylation profile. J. Pediatr. 2018, 202, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.A.; Vento, M.; Finer, N.N.; Rich, W.; Saugstad, O.D.; Morley, C.J.; Davis, P.G. Managing oxygen therapy during delivery room stabilization of preterm infants. J. Pediatr. 2012, 160, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.; Vento, M.; Shah, P.S.; Saugstad, O.; Finer, N.; Rich, W.; Morton, R.L.; Rabi, Y.; Tarnow-Mordi, W.; Suzuki, K.; et al. A review of international clinical practice guidelines for the use of oxygen in the delivery room resuscitation of preterm infants. Acta Paediatr. 2018, 107, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, C.M.; Kofa, E.W.; Slutsky, J.R. Clinicians' attitudes to clinical practice guidelines: A systematic review. Med. J. Aust. 2002, 177, 502–506. [Google Scholar]
- Iriondo, M.; Thió, M.; Burón, E.; Salguero, E.; Aguayo, J.; Vento, M. Neonatal Resuscitation Group of the Spanish Neonatal Society. A survey of neonatal resuscitation in Spain: Gaps between guidelines and practice. Acta Paediatr. 2009, 98, 786–791. [Google Scholar] [CrossRef]

{kind=link}
Table 1.
Suggestions on how to supply oxygen in the delivery room to newly born infants.
| Gestational Age | Initial FiO2 | Target SpO2 at 5 min |
|---|---|---|
| <37 weeks | 0.21 | 85–90% |
| 33+0 to 36+6 weeks | 0.21 | 85% |
| 29+0 to 32+6 weeks | 0.21-0.30* | 80–85% |
| ≤28 weeks | 0.3 | 80% |
Abbreviations: FiO2: inspired fraction of oxygen; SpO2: arterial oxygen saturation measure by pulseoximetry. Further suggestions: initial FiO2 should be decided after evaluation of immediate postnatal reactivity by the attending neonatologist. If no reactive choose the higher FiO2; FiO2 adjustments should aim to achieve targeted SpO2 and avoiding bradycardia (heart rate <100 bpm); Hear rate >2 min after birth should be >100 bpm.; Register SpO2 at 5 min together with the 5-minute Apgar score; Modified from Saugstad et al. Pediatr. Res. 2018 [31].
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lara-Cantón, I.; Solaz, A.; Parra-Llorca, A.; García-Robles, A.; Vento, M. Optimal Inspired Fraction of Oxygen in the Delivery Room for Preterm Infants. Children 2019, 6, 29. https://0-doi-org.brum.beds.ac.uk/10.3390/children6020029
AMA Style
Lara-Cantón I, Solaz A, Parra-Llorca A, García-Robles A, Vento M. Optimal Inspired Fraction of Oxygen in the Delivery Room for Preterm Infants. Children. 2019; 6(2):29. https://0-doi-org.brum.beds.ac.uk/10.3390/children6020029
Chicago/Turabian StyleLara-Cantón, Inmaculada, Alvaro Solaz, Anna Parra-Llorca, Ana García-Robles, and Máximo Vento. 2019. "Optimal Inspired Fraction of Oxygen in the Delivery Room for Preterm Infants" Children 6, no. 2: 29. https://0-doi-org.brum.beds.ac.uk/10.3390/children6020029
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.