Quality Improvement Project to Improve Screening for Tobacco Use in Adolescent Inpatients at a Children’s Hospital

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Context
2.2. Interventions
2.3. Study of the Interventions
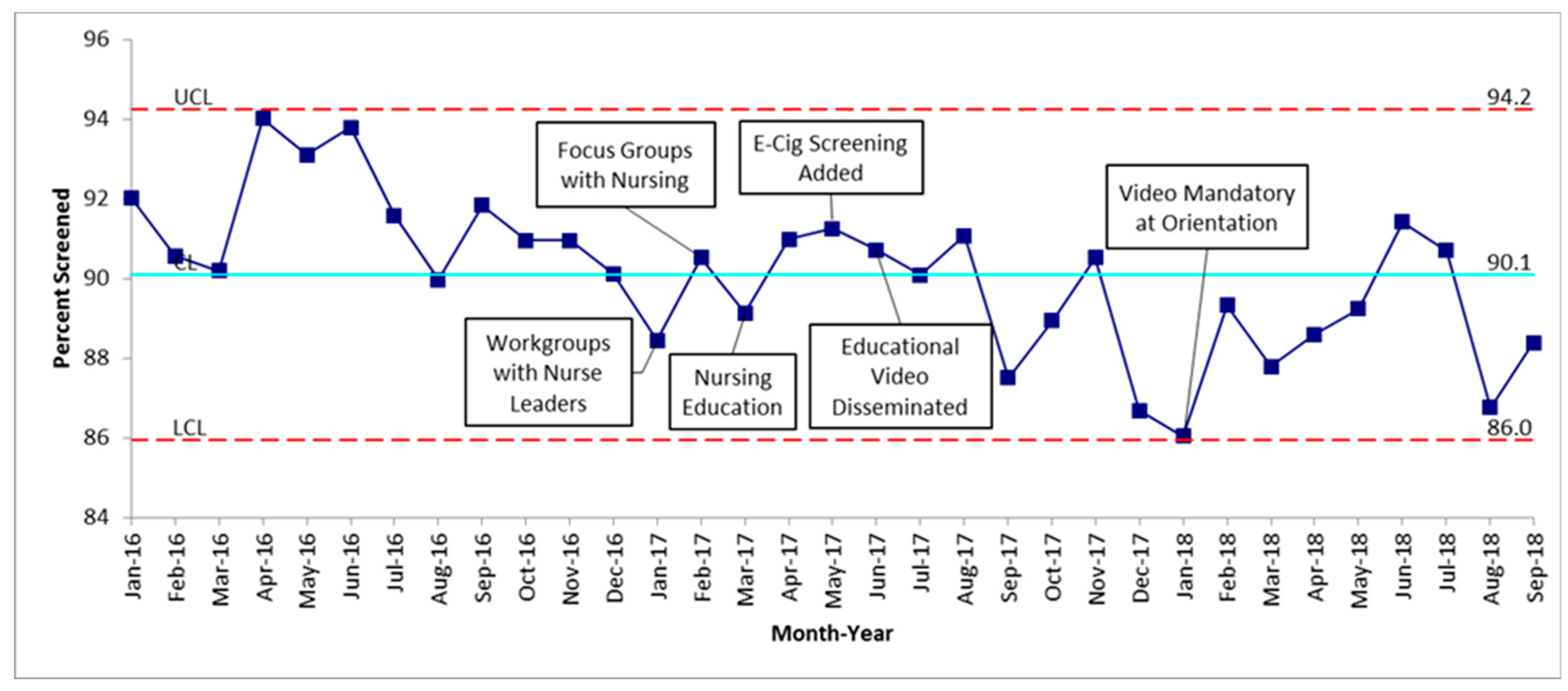
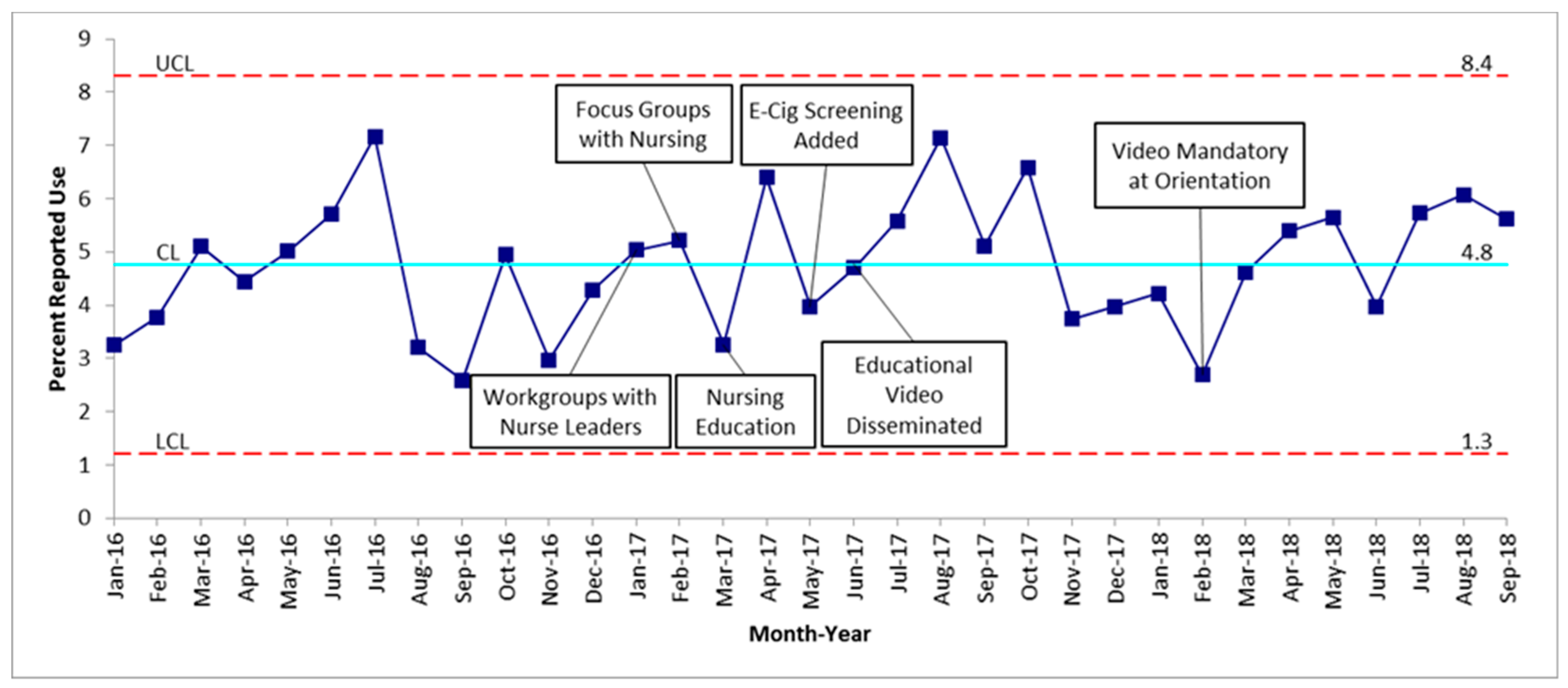
2.4. Measures
2.5. Ethics
3. Results
4. Discussion
4.1. Summary and Interpretation of Findings
4.2. Limitations
4.3. Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress; U.S. Department of Health and Human Services: Rockville, MD, USA, 2014.
- Cullen, K.A.; Ambrose, B.K.; Gentzke, A.S.; Apelberg, B.J.; Jamal, A.; King, B.A. Notes from the Field: Use of Electronic Cigarettes and Any Tobacco Product Among Middle and High School Students—United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1276–1277. [Google Scholar] [CrossRef] [PubMed]
- Tobacco product use among middle and high school students—United States, 2011 and 2012. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 893–897.
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Hawkins, J.; Queen, B.; Lowry, R.; Olsen, E.O.; Chyen, D.; et al. Youth Risk Behavior Surveillance—United States, 2015. Morb. Mortal. Wkly. Rep. Surveill. Summ. (Wash. DC 2002) 2016, 65, 1–174. [Google Scholar] [CrossRef]
- The Centers for Disease Control and Prevention. Extinguishing the Tobacco Epidemic in Alabama. Available online: https://www.cdc.gov/tobacco/about/osh/state-fact-sheets/alabama/ (accessed on 4 December 2018).
- Moyer, V.A. Primary care interventions to prevent tobacco use in children and adolescents: U.S. preventive services task force recommendation statement. Pediatrics 2013, 132, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.C.; Goplerud, E.; Schroeder, S.A. The Joint Commission’s new tobacco-cessation measures--will hospitals do the right thing? N. Engl. J. Med. 2012, 366, 1172–1174. [Google Scholar] [CrossRef] [PubMed]
- Delbecq, A.L.; Van de Ven, A.H. A Group Process Model for Problem Identification and Program Planning. J. Appl. Behav. Sci. 1971, 7, 466–492. [Google Scholar] [CrossRef]
- Berwick, D.M. Improvement, trust, and the healthcare workforce. Qual. Saf. Health Care 2003, 12, 448–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provost, L.P.; Murray, S. M20: Beyond Statistical Process Control: Advanced Charts for Healthcare. Available online: http://app.ihi.org/FacultyDocuments/Events/Event-2206/Presentation-7244/Document-5737/M20_Presentation.pdf (accessed on 16 December 2018).
- Wang, T.W.; Gentzke, A.; Sharapova, S.; Cullen, K.A.; Ambrose, B.K.; Jamal, A. Tobacco Product Use Among Middle and High School Students—United States, 2011–2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Dutra, L.M.; Glantz, S.A. Electronic cigarettes and conventional cigarette use among U.S. adolescents: A cross-sectional study. JAMA Pediatr. 2014, 168, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Yeo, M.S.; Bond, L.M.; Sawyer, S.M. Health risk screening in adolescents: Room for improvement in a tertiary inpatient setting. Med. J. Aust. 2005, 183, 427–429. [Google Scholar] [PubMed]
- Minami, H.; Bloom, E.L.; Brinkman, H.R.; Abrantes, A.M.; Young, C.C.; Brown, R.A. Factors related to cigarette smoking and intent to quit among adolescent inpatients with psychiatric and substance use disorders. Drug Alcohol Depend. 2018, 186, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Ranney, M.L.; Choo, E.K.; Spirito, A.; Mello, M.J. Adolescents’ preference for technology-based emergency department behavioral interventions: Does it depend on risky behaviors? Pediatr. Emerg. Care 2013, 29, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Colby, S.M.; Monti, P.M.; O’Leary Tevyaw, T.; Barnett, N.P.; Spirito, A.; Rohsenow, D.J.; Riggs, S.; Lewander, W. Brief motivational intervention for adolescent smokers in medical settings. Addict. Behav. 2005, 30, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Mahabee-Gittens, E.M.; Ding, L.; Gordon, J.S.; Huang, B. Agreement between parents and youth on measures of anti-smoking socialization. J. Child Adolesc. Subst. Abuse 2010, 19, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Mahabee-Gittens, E.M.; Huang, B.; Slap, G.B.; Gordon, J.S. An Emergency Department Intervention to Increase Parent-Child Tobacco Communication: A Pilot Study. J. Child Adolesc. Subst. Abuse 2008, 17, 71–83. [Google Scholar] [CrossRef]
- Jasm, M.; Chan, P.C.; Ramachandran, R. Health Survey for Adolescents—A brief, Non Obligatory Questionnaire Used as a Screening Tool for the Identification of “At Risk” Adolescents in a Paediatric Inpatient Setting, at a Tertiary Health Care Centre in Singapore. J. Adolesc. Health 2016, 58. [Google Scholar] [CrossRef]
- Mahabee-Gittens, E.; Vaughn, L.; Gordon, J. Youth and Their Parents’ Views on the Acceptability and Design of a Video-Based Tobacco Prevention Intervention. J. Child Adolesc. Subst. Abuse 2010, 19, 391–405. [Google Scholar] [CrossRef] [PubMed]
- NIH. SmokeFreeTeen. Available online: https://teen.smokefree.gov/ (accessed on 25 February 2019).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nursing Focus Groups Prioritized Identified Themes |
|---|
| 1. Parents and caregivers in the room influences honesty of answers |
| 2. Patient feels judged/judgmental questions |
| 3. Not knowing how to follow up with positive response |
| 4. Not a priority |
| 5. Patient severity/cannot ask |
| 6. Time/too busy |
| Measures | Definition |
|---|---|
| Tobacco User | Using cigarettes, cigars, pipes, hookah, or e-cigarette |
| Light Tobacco User | Less than 10 cigarettes or equivalent of cigars/pipes/e-cigs per day |
| Heavy Tobacco User | More than 10 cigarettes or equivalent of cigars/pipes/e-cigs per day |
| Percent screened | Number of patients screened divided by number of all adolescents admitted that month |
| Percent positive | Number of patients reporting tobacco use divided by the total number screened |
| Reported positive | All patients who were screened and reported: tobacco user, current status unknown, former tobacco user, current every day tobacco user, current some day tobacco user, light tobacco user, heavy tobacco user, current chewing tobacco user |
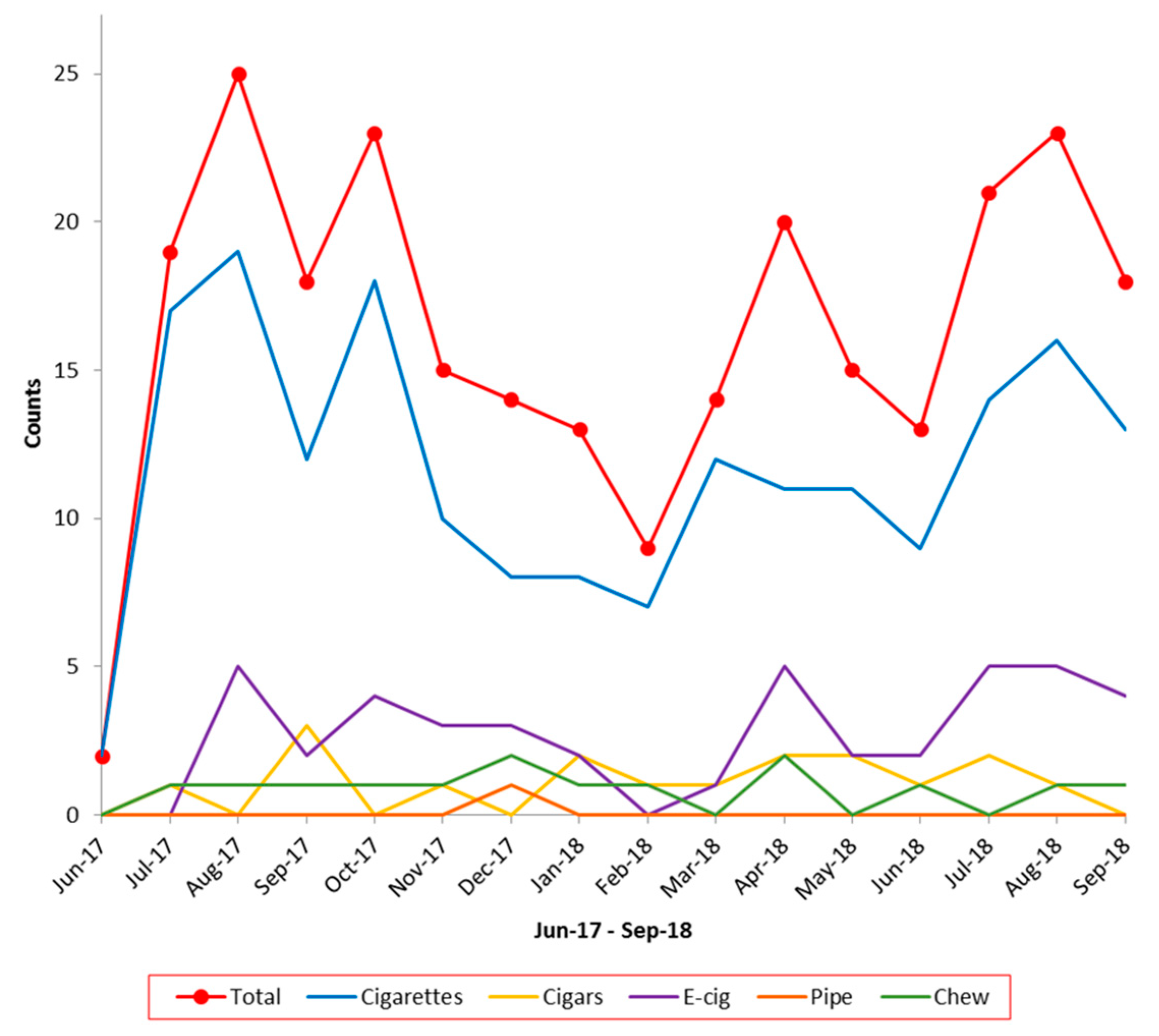
| Absolute number of tobacco products used | Total number of patients who reported use of each type of tobacco product |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, L.A.; Molina, A.L.; Grizzle, K.; Hofto, M.E.; Nassetta, L.B.; Orr, M.M.; Samuy, N.; Schmit, E.O.; Smola, C.; Harrington, K.F.; et al. Quality Improvement Project to Improve Screening for Tobacco Use in Adolescent Inpatients at a Children’s Hospital. Children 2019, 6, 37. https://0-doi-org.brum.beds.ac.uk/10.3390/children6030037
Wagner LA, Molina AL, Grizzle K, Hofto ME, Nassetta LB, Orr MM, Samuy N, Schmit EO, Smola C, Harrington KF, et al. Quality Improvement Project to Improve Screening for Tobacco Use in Adolescent Inpatients at a Children’s Hospital. Children. 2019; 6(3):37. https://0-doi-org.brum.beds.ac.uk/10.3390/children6030037
Chicago/Turabian StyleWagner, Lauren A., Adolfo L. Molina, Karisa Grizzle, Meghan E. Hofto, Lauren B. Nassetta, Mary M. Orr, Nichole Samuy, Erinn O. Schmit, Cassi Smola, Kathleen F. Harrington, and et al. 2019. "Quality Improvement Project to Improve Screening for Tobacco Use in Adolescent Inpatients at a Children’s Hospital" Children 6, no. 3: 37. https://0-doi-org.brum.beds.ac.uk/10.3390/children6030037