Safety and Ergonomic Challenges of Ventilating a Premature Infant During Delayed Cord Clamping


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
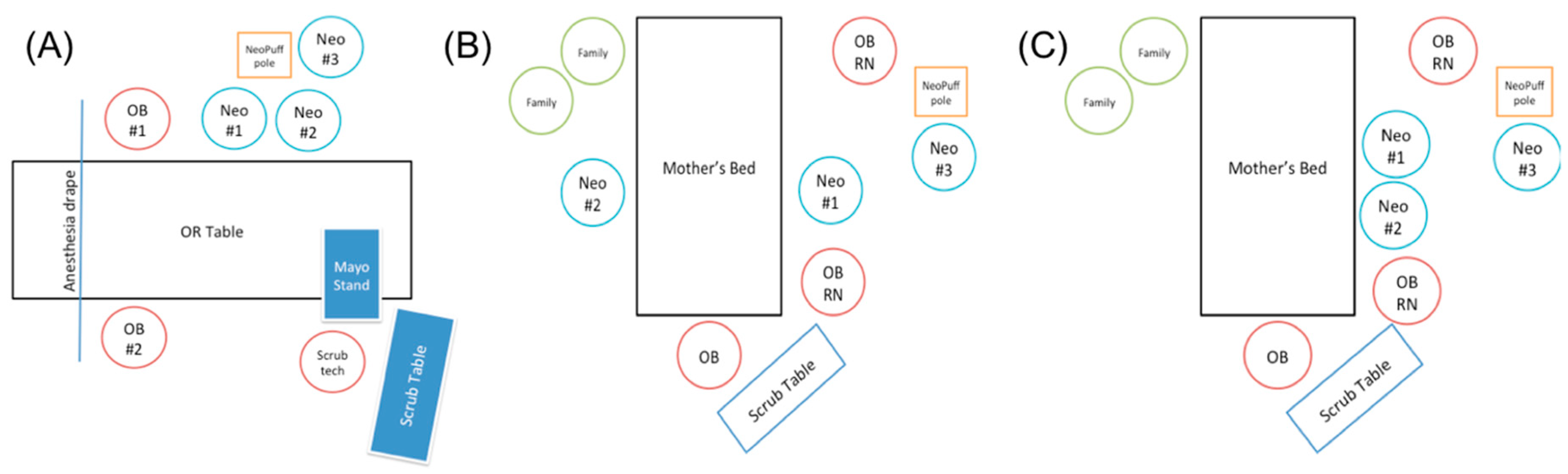
2.2. Setting and Design
3. Results
3.1. Theme 1: Sterility
3.2. Theme 2: Equipment
3.3. Theme 3: Mobility
3.4. Theme 4: Space and Workflow
3.5. Theme 5: Communication
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Katheria, A.C.; Lakshminrusimha, S.; Rabe, H.; McAdams, R.; Mercer, J.S. Placental transfusion: A review. J. Perinatol. Off. J. Calif. Perin. Assoc. 2017, 37, 105–111. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.J.; Middleton, P.; Dowswell, T.; Morris, P.S. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Datab. Syst. Rev. 2013, 7, CD004074. [Google Scholar] [CrossRef] [PubMed]
- Rabe, H.; Diaz-Rossello, J.L.; Duley, L.; Dowswell, T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Datab. Syst. Rev. 2012, 8, CD003248. [Google Scholar] [CrossRef] [PubMed]
- Backes, C.H.; Rivera, B.K.; Haque, U.; Bridge, J.A.; Smith, C.V.; Hutchon, D.J.; Mercer, J.S. Placental transfusion strategies in very preterm neonates: A systematic review and meta-analysis. Obstet. Gynecol. 2014, 124, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, M.; Osborn, D.A.; Askie, L.; Seidler, A.L.; Hunter, K.; Lui, K.; Simes, J.; Tarnow-Mordi, W. Delayed vs early umbilical cord clamping for preterm infants: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2018, 218, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Guidelines on Basic Newborn Resuscitation; World Health Organization: Geneva, Switzerland, 2012.
- World Health Organization. In Guideline: Delayed Umbilical Cord Clamping for Improved Maternal and Infant Health and Nutrition Outcomes; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Wyckoff, M.H.; Aziz, K.; Escobedo, M.B.; Kapadia, V.S.; Kattwinkel, J.; Perlman, J.M.; Simon, W.M.; Weiner, G.M.; Zaichkin, J.G. Part 13: Neonatal resuscitation: 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132, 543–560. [Google Scholar] [CrossRef] [PubMed]
- Weiner, G.M.; Zaichkin, J.; American Academy of Pediatrics and American Heart Association. Textbook of Neonatal Resuscitation (NRP), 7th ed.; Gary, M., Weiner, M., Jeanette Zaichkin, R., Eds.; American Academy of Pediatrics: Itasca, IL, USA, 2016. [Google Scholar]
- Committee on Obstetric Practice. Committee opinion No. 684: Delayed umbilical cord clamping after birth. Obstet. Gynecol. 2017, 129, 5–10. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Intrapartum Care for Healthy Women and Babies; National Institute for Health and Care Excellence: London, UK, 2017. [Google Scholar]
- Delgado Nunes, V.; Gholitabar, M.; Sims, J.M.; Bewley, S. Intrapartum care of healthy women and their babies: Summary of updated NICE guidance. BMJ 2014, 349, g6886. [Google Scholar] [CrossRef]
- American College of Nurse-Midwives. Position Statement: Delayed Cord Clamping. 2014. Available online: http://www.midwife.org/ACNM/files/ACNMLibraryData/UPLOADFILENAME/000000000290/Delayed-Umbilical-Cord-Clamping-May-2014.pdf (accessed on 13 April 2019).
- Leduc, D.; Senikas, V.; Lalonde, A.B. No. 235-Active management of the third stage of labour: Prevention and treatment of postpartum hemorrhage. J. Obstet. Gynaecol. Can. 2018, 40, 841–855. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Alison, B.J.; Wallace, E.M.; Crossley, K.J.; Gill, A.W.; Kluckow, M.; te Pas, A.B.; Morley, C.J.; Polglase, G.R.; Hooper, S.B. Delaying cord clamping until ventilation onset improves cardiovascular function at birth in preterm lambs. J. Physiol. 2013, 591, 2113–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, S.B.; Te Pas, A.B.; Lang, J.; van Vonderen, J.J.; Roehr, C.C.; Kluckow, M.; Gill, A.W.; Wallace, E.M.; Polglase, G.R. Cardiovascular transition at birth: A physiological sequence. Pediatr. Res. 2015, 77, 608. [Google Scholar] [CrossRef] [PubMed]
- Polglase, G.R.; Blank, D.A.; Barton, S.K.; Miller, S.L.; Stojanovska, V.; Kluckow, M.; Gill, A.W.; LaRosa, D.; Te Pas, A.B.; Hooper, S.B. Physiologically based cord clamping stabilises cardiac output and reduces cerebrovascular injury in asphyxiated near-term lambs. Arch. Dis. Child. Fet. Neonat. Ed. 2018, 103, 530–538. [Google Scholar] [CrossRef]
- Nevill, E.; Meyer, M.P. Effect of delayed cord clamping (DCC) on breathing and transition at birth in very preterm infants. Early Hum. Dev. 2015, 91, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.S.; Kaempf, J.; de Klerk, A.; de Klerk, R.; Reilly, M.; Howard, D.; Ferrelli, K.; O’Conor, J.; Soll, R.F.; Vermont Oxford Network DRM Study Group. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics 2011, 128, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Finer, N.N.; Carlo, W.A.; Duara, S.; Fanaroff, A.A.; Donovan, E.F.; Wright, L.L.; Kandefer, S.; Poole, W.K. Delivery room continuous positive airway pressure/positive end-expiratory pressure in extremely low birth weight infants: A feasibility trial. Pediatrics 2004, 114, 651–657. [Google Scholar] [CrossRef]
- Finer, N.N.; Carlo, W.A.; Walsh, M.C.; Rich, W.; Gantz, M.G.; Laptook, A.R.; Yoder, B.A.; Faix, R.G.; Das, A.; Poole, W.K.; et al. Early CPAP versus surfactant in extremely preterm infants. N. Engl. J. Med. 2010, 362, 1970–1979. [Google Scholar] [CrossRef] [PubMed]
- Lapcharoensap, W.; Bennett, M.V.; Powers, R.J.; Finer, N.N.; Halamek, L.P.; Gould, J.B.; Sharek, P.J.; Lee, H.C. Effects of delivery room quality improvement on premature infant outcomes. J. Perinatol. Off. J. Calif. Perin. Assoc. 2016, 37, 349. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Respiratory support in preterm infants at birth. Pediatrics 2014, 133, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Duley, L.; Dorling, J.; Pushpa-Rajah, A.; Oddie, S.J.; Yoxall, C.W.; Schoonakker, B.; Bradshaw, L.; Mitchell, E.J.; Fawke, J.A. Randomised trial of cord clamping and initial stabilisation at very preterm birth. Arch. Dis. Child. Fet. Neonat. Ed. 2018, 103, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.; Kattwinkel, J.; Chisholm, C.; Blackman, A.; Wilson, S.; Fairchild, K. Ventilation of preterm infants during delayed cord clamping (VentFirst): A pilot study of feasibility and safety. Am. J. Perinatol. 2017, 34, 111–116. [Google Scholar] [CrossRef]
- Katheria, A.; Poeltler, D.; Durham, J.; Steen, J.; Rich, W.; Arnell, K.; Maldonado, M.; Cousins, L.; Finer, N. Neonatal Resuscitation with an Intact Cord: A Randomized Clinical Trial. J. Pediatr. 2016, 178, 75–80. [Google Scholar] [CrossRef]
- Pratesi, S.; Montano, S.; Ghirardello, S.; Mosca, F.; Boni, L.; Tofani, L.; Dani, C. Placental circulation intact trial (PCI-T)-resuscitation with the placental circulation intact vs. cord milking for very preterm infants: A feasibility study. Front. Pediatr. 2018, 6, 364. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Committee on Fetus And Newborn. Levels of neonatal care. Pediatrics 2012, 130, 587–597. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Aoki, S.; Oba, M.S.; Seki, K.; Hirahara, F. Relationship between short umbilical cord length and adverse pregnancy outcomes. Fetal Pediatr. Pathol. 2016, 35, 81–87. [Google Scholar] [CrossRef]
- Castrodale, V.; Rinehart, S. The golden hour: Improving the stabilization of the very low birth-weight infant. Adv. Neonat. Care Off. J. Nat. Assoc. Neonat. Nurses 2014, 14, 9–14. [Google Scholar] [CrossRef]
- Oddie, S.; Rhodes, P. Barriers to deferred cord clamping in preterm infants. Arch. Dis. Child. Fetal Neonat. Ed. 2014, 99, 391–394. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Organization | Year | Recommendation |
|---|---|---|
| World Health Organization (WHO) [6,7] | 2006, most recently updated 2017 | “In newly-born term or preterm babies who do not require positive-pressure ventilation, the cord should not be clamped earlier than one minute after birth.” “Delayed umbilical cord clamping (not earlier than 1 min after birth) is recommended for improved maternal and infant health and nutrition outcomes.” |
| International Liaison Committee on Resuscitation (ILCOR) [8] | 2010, updated 2015 | “DCC for longer than 30 s is reasonable for both term and preterm infants who do not require resuscitation at birth” |
| Neonatal Resuscitation Program (NRP) guidelines from the American Academy of Pediatrics (AAP) [9] | 2017 | “Delay in umbilical cord clamping for at least 30–60 s for most vigorous term and preterm infants.” |
| American College of Obstetricians and Gynecologists (ACOG) [10] | 2010, recently updated in 2017 | “Delay in umbilical cord clamping in vigorous term and preterm infants for at least 30–60 s after birth” |
| National Institute for Health and Care Excellence (United Kingdom) [11,12] | 2014, updated 2017 | “Do not clamp the cord earlier than 1 min from the birth of the baby unless there is concern about the integrity of the cord or the baby has a heart rate below 60 beats/minute that is not getting faster.” |
| American College of Nurse–Midwives [13] | 2014 | “For term newborns, delaying the clamping of the cord for 5 min if the newborn is placed skin-to-skin or 2 min with the newborn at or below the level of the introitus ensures the greatest benefit. For preterm newborns, the benefits of delaying cord clamping for 30 to 60 s include a significant reduction in intraventricular hemorrhage and a reduced need for blood transfusion.” |
| Society of Obstetricians and Gynecologists of Canada [14] | 2009, reaffirmed 2018 | “Whenever possible, delaying cord clamping by at least 60 s is preferred to clamping earlier in premature newborns (<37 weeks’ gestation) since there is less intraventricular hemorrhage and less need for transfusion in those with late clamping.” |
| Term Infants |
| Increased hemoglobin levels at birth Increased iron stores in first several months of life |
| Preterm Infants |
| Increased hematocrit levels Reduced need for blood transfusions Reduced incidence of intraventricular hemorrhage Reduced incidence of necrotizing enterocolitis Decreased hospital mortality |
| Topic | Identified Challenges |
|---|---|
| Sterility | ● Current available respiratory equipment (CPAP mask, ventilation tubing) is not sterile, forcing clinicians to use a nonsterile piece of equipment adjacent to a sterile field with the theoretical risk of increasing surgical site infections. ● An ideal surface would provide adequate warmth to the vulnerable preterm infant. Current commercially available thermal mattresses are not sterile and require a workaround. ● Maintaining sterility requires more personnel than community hospitals may be able to staff. |
| Equipment | ● CPAP is ideally performed on a flat surface. However, there are limited options on how to best provide CPAP during DCC. Currently there is not an ideal surface and respiratory setup that allows for all infants to receive CPAP during DCC. ● Providers are often limited by the umbilical cord length to reach any available surfaces. |
| Mobility | ● Following DCC, the infant needs to be moved from the DCC site to a resuscitation bed or the intensive care unit. Concerns raised about the safety of moving a patient vulnerable to intraventricular hemorrhages multiple times in a short period (DCC to resuscitation bed to the ICU bed). An ideal setup would include minimal transportation and lifting of the infant. |
| Space and Workflow | ● In this new arrangement, the workflow was awkward. As there are multiple team members present at the mother’s side in a small space to provide DCC with CPAP, neonatal providers will often start from far away. There needs to be adequate time, space, and communication for the neonatal providers to safely approach the bed. |
| Communication | ● Obstetric providers voiced concerns about safety for the mother during DCC and emphasized the need for clear communication between the multidisciplinary teams. ● Neonatal providers request communication about when they are able to approach the mother safely in order to care for the infant. ● There is a need for protocols on when to discontinue DCC due to the infant or maternal status. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lapcharoensap, W.; Cong, A.; Sherman, J.; Schwandt, D.; Crowe, S.; Daniels, K.; Lee, H.C. Safety and Ergonomic Challenges of Ventilating a Premature Infant During Delayed Cord Clamping. Children 2019, 6, 59. https://0-doi-org.brum.beds.ac.uk/10.3390/children6040059
Lapcharoensap W, Cong A, Sherman J, Schwandt D, Crowe S, Daniels K, Lee HC. Safety and Ergonomic Challenges of Ventilating a Premature Infant During Delayed Cord Clamping. Children. 2019; 6(4):59. https://0-doi-org.brum.beds.ac.uk/10.3390/children6040059
Chicago/Turabian StyleLapcharoensap, Wannasiri, Allison Cong, Jules Sherman, Doug Schwandt, Susan Crowe, Kay Daniels, and Henry C. Lee. 2019. "Safety and Ergonomic Challenges of Ventilating a Premature Infant During Delayed Cord Clamping" Children 6, no. 4: 59. https://0-doi-org.brum.beds.ac.uk/10.3390/children6040059