The Role of Social Support in Adolescent/Young Adults Coping with Cancer Treatment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
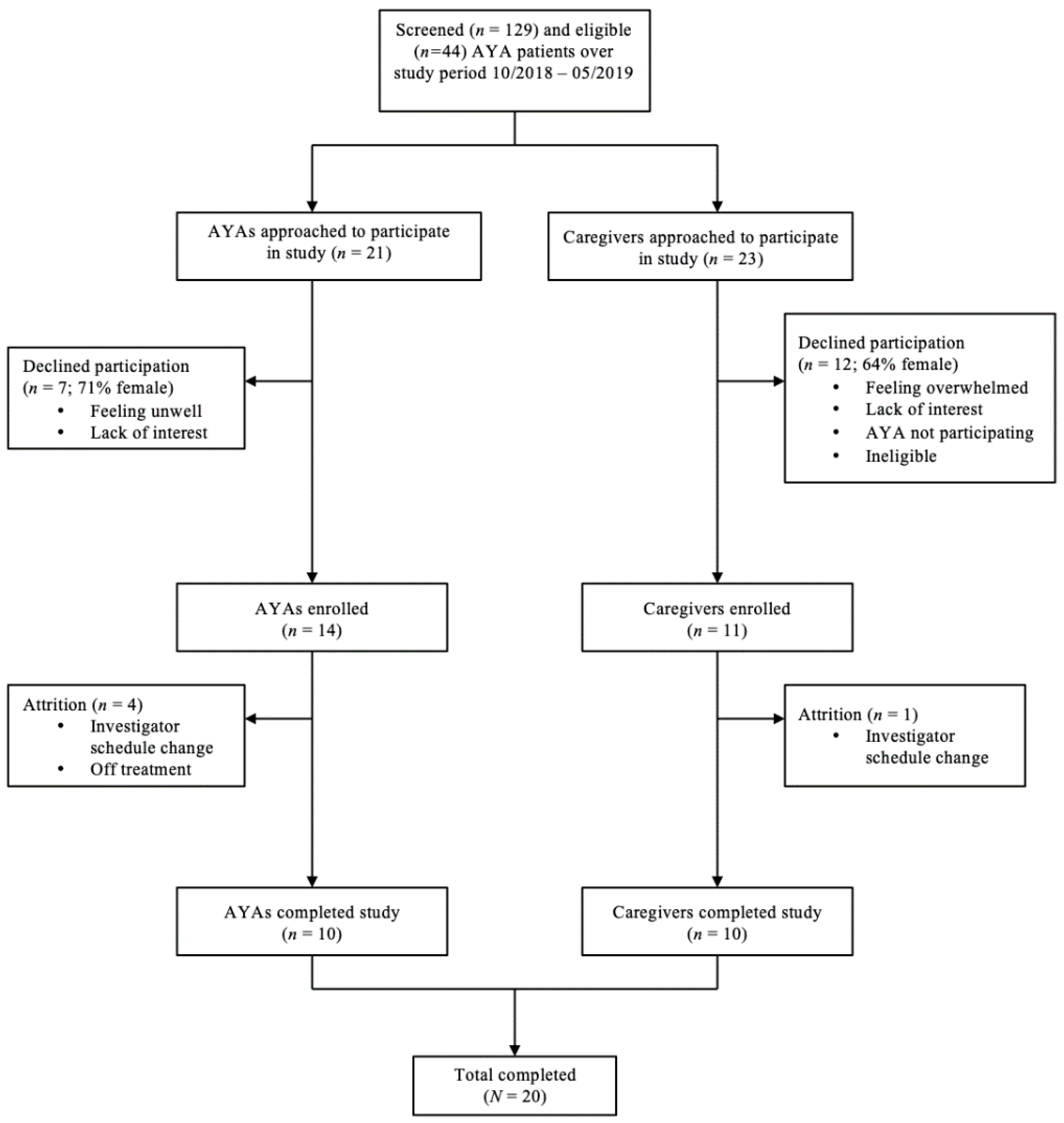
2.2. Participants
2.3. Procedure
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Results from Instruments/Measures
3.2. Results from Qualitative Analysis
3.2.1. Family
3.2.1.1. Presence
3.2.1.2. Everyday Tasks
3.2.1.3. Maintaining Autonomy (Independence, Privacy, and Space)
3.2.1.4. Advocate/Source of Information
3.2.1.5. Positive Attitude
3.2.2. Friends
3.2.2.1. Presence
3.2.2.2. Communication/Contact
3.2.2.3. Distraction
3.2.2.4. Encouragement/Gestures
3.2.3. Other Social Support
3.2.3.1. Peers
3.2.3.2. Medical Staff
3.2.3.3. Spouse/Significant Other
3.2.3.4. School/Work
3.2.3.5. Professional or Collegiate Athletes
3.2.3.6. Organizations
3.2.3.7. Community
3.2.4. Opinions/Advice
3.2.4.1. Not Helpful
3.2.4.2. Advice to Others
4. Discussion
4.1. Social Support and AYA Coping
4.1.2. Family Support
4.1.3. Friend Support
4.1.4. Cancer Peer Support
4.1.5. Medical Staff Support
4.1.6. Other Social Support
4.2. Clinical Implications
4.2.1. Implications for Education
4.2.2. Implications for Screening
4.2.3. Implications for Intervention
4.3. Future Directions
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
A.1. Interview Guide—AYA Form
- Tell me how things have gone for you since you were diagnosed with cancer.
- Has anything happened during this time that has changed things for you? If so, what?
- What kind of things are you doing/have you done to get through this time?
- How did you do that?
- What has been a challenge so far and how did you handle it?
- What have others done?
- Why was it unhelpful/helpful?
- What do you wish they would/would not do?
- (Follow up: How do you think social support is related to your coping?)
- However you think of hope, how is hope related to all of this?
- Tell me about times you did not feel hopeful or you had low hope.
- What do you hope for now?
- How do you plan to get there?
- What else should I know about your experience with cancer that I haven’t asked?
- What is important for us to know?
A.2. Interview Guide—Parent Form
- Tell me how things have gone for your child since their diagnosis.
- What kind of things is/has your child done to get through this time?
- What has been a challenge for them so far and how did they handle it?
- What have you done to help your child through this time?
- What do you think your child wanted you to do/wanted from you?
- How did these match or mismatch?
- What have others done?
- Why was it unhelpful/helpful?
- However you think of hope, how is hope related to all of this?
- What does your child hope for?
- How do you think he or she will get there?
- What else should I know about your child’s experience with cancer that I haven’t asked?
- What is important for us to know?
References
- Coccia, P. Overview of Adolescent and Young Adult Oncology. J. Oncol. Pract. 2019, 15, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.; Drotar, D. Posttraumatic stress and related impairment in survivors of childhood cancer in early adulthood compared to healthy peers. J. Pediatr. Psychol. 2005, 31, 356–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrera, M.; Shaw, A.K.; Speechley, K.N.; Maunsell, E.; Pogany, L. Educational and social late effects of childhood cancer and related clinical, personal, and familial characteristics. Cancer 2005, 104, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Rourke, M.T.; Hobbie, W.L.; Schwartz, L.; Kazak, A.E. Posttrauamatic stress disorder (PTSD) in young adult survivors of childhood cancer. Pediatr. Blood Cancer 2007, 49, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Kazak, A.E.; DeRosa, B.W.; Schwartz, L.A.; Hobbie, W.; Carlson, C.; Ittenbach, R.F.; Mao, J.J.; Ginsberg, J.P. Psychological outcomes and health beliefs in adolescent and young adult survivors of childhood cancer and controls. J. Clin. Oncol. 2010, 28, 2002–2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felder-Puig, R.; Formann, A.K.; Mildner, A.; Bretschneider, W.; Bucher, B.; Windhager, R.; Zoubek, A.; Puig, S.; Topf, R. Quality of life and psychosocial adjustment of young patients after treatment of bone cancer. Cancer 1998, 83, 69–75. [Google Scholar] [CrossRef]
- Abrams, A.N.; Hazen, E.P.; Penson, R.T. Psychosocial issues in adolescents with cancer. Cancer Treat. Rev. 2007, 33, 622–630. [Google Scholar] [CrossRef]
- Langeveld, N.; Stam, H.; Grootenhuis, M.; Last, B. Quality of life in young adult survivors of childhood cancer. Support. Care Cancer 2002, 10, 579–600. [Google Scholar] [CrossRef]
- Kyngäs, H.; Mikkonen, R.; Nousiainen, E.M.; Rytilahti, M.; Seppänen, P.; Vaattovaara, R.; Jämsä, T. Coping with the onset of cancer: Coping strategies and resources of young people with cancer. Eur. J. Cancer Care 2001, 10, 6–11. [Google Scholar] [CrossRef]
- Hokkanen, H.; Eriksson, E.; Ahonen, O.; Salantera, S. Adolescents with cancer: Experience of life and how it could be made easier. Cancer Nurs. 2004, 27, 325–335. [Google Scholar] [CrossRef]
- Ishibashi, A. The needs of children and adolescents with cancer for information and social support. Cancer Nurs. 2001, 24, 61. [Google Scholar] [CrossRef] [PubMed]
- Tillery, R.; Howard Sharp, K.M.; Okado, Y.; Long, A.; Phipps, S. Profiles of resilience and growth in youth with cancer and healthy comparisons. J. Pediatr. Psychol. 2015, 41, 290–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodgate, R.L. The importance of being there: Perspectives of social support by adolescents with cancer. J. Pediatr. Oncol. Nurs. 2006, 23, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Hollingshead, A.B. Four Factor Index of Social Status. Yale J. Sociol. 2011, 8, 21–52. [Google Scholar]
- Snyder, C.R.; Sympson, S.C.; Ybasco, F.C.; Borders, T.F.; Babyak, M.A.; Higgins, R.L. Development and Validation of the State Hope Scale. J. Personal. Soc. Psychol. 1996, 70, 321–335. [Google Scholar] [CrossRef]
- Snyder, C.R.; Harris, C.; Anderson, J.R.; Holleran, S.A.; Irving, L.M.; Sigmon, S.T.; Yoshinobu, L.; Gibb, J.; Langelle, C.; Harney, P. The Will and the Ways: Development and Validation of an Individual-Differences Measure of Hope. J. Personal. Soc. Psychol. 1991, 60, 570–585. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scale, 2nd ed.; The Psychological Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Osman, A.; Wong, J.L.; Bagge, C.L.; Freedenthal, S.; Gutierrez, P.M.; Lozano, G. The depression anxiety stress Scales—21 (DASS-21): Further examination of dimensions, scale reliability, and correlates. J. Clin. Psychol. 2012, 68, 1322–1338. [Google Scholar] [CrossRef]
- Szabó, M. The short version of the Depression Anxiety Stress Scales (DASS-21): Factor structure in a young adolescent sample. J. Adolesc. 2010, 33, 1–8. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Katz, E.R.; Meeske, K.; Dickinson, P. The PedsQL™ in pediatric cancer. Cancer 2002, 94, 2090–2106. [Google Scholar] [CrossRef]
- Ewing, J.E.; King, M.T.; Smith, N.F. Validation of modified forms of the PedsQL generic core scales and cancer module scales for adolescents and young adults (AYA) with cancer or a blood disorder. Qual. Life Res. 2009, 18, 231–244. [Google Scholar] [CrossRef] [Green Version]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldin Pub: Chicago, IL, USA, 1967. [Google Scholar]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Glaser, B.G. The constant comparative method of qualitative analysis. Soc. Probl. 1965, 12, 436–445. [Google Scholar] [CrossRef]
- Morse, J.M. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual. Health Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Decker, C.L. Social support and adolescent cancer survivors: A review of the literature. Psycho Oncol. 2007, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.E.; Doan, B.D.; Shermer, P.; Fitzgerald, A.V.; Bery, M.P.; Jenkin, D.; Doherty, M.A. Psychologic adaptation of survivors of childhood cancer. Cancer 1992, 70, 2713–2721. [Google Scholar] [CrossRef]
- Haluska, H.B.; Jessee, P.O.; Nagy, M.C. Sources of social support: Adolescents with cancer. Oncol. Nurs. Forum 2002, 29, 1317–1324. [Google Scholar] [CrossRef]
- Banner, L.M.; Mackie, E.J.; Hill, J.W. Family relationships in survivors of childhood cancer: Resource or restraint? Patient Educ. Couns. 1996, 28, 191–199. [Google Scholar] [CrossRef]
- Howard Sharp, K.M.; Willard, V.W.; Barnes, S.; Tillery, R.; Long, A.; Phipps, S.; Gerhardt, C.A.; Berg, C.A.; Wiebe, D.J.; Holmbeck, J.N.; et al. (Eds.) Emotion socialization in the context of childhood cancer: Perceptions of parental support promotes posttraumatic growth. J. Pediatr. Psychol. 2016, 42, 95–103. [Google Scholar]
- Rolland, J.S. Chronic illness and the life cycle: A conceptual framework. Fam. Process 1987, 26, 203–221. [Google Scholar] [CrossRef]
- Zebrack, B.; Chesler, M.A.; Kaplan, S. To foster healing among adolescents and young adults with cancer: What helps? What hurts? Support. Care Cancer 2010, 18, 131. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.E.; Gerhardt, C.A.; Vannatta, K.; Noll, R.B. Parent and family factors associated with child adjustment to pediatric cancer. J. Pediatr. Psychol. 2006, 32, 400–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zebrack, B.; Bleyer, A.; Albritton, K.; Medearis, S.; Tang, J. Assessing the health care needs of adolescent and young adult cancer patients and survivors. Cancer 2006, 107, 2915–2923. [Google Scholar] [CrossRef] [PubMed]
- D’agostino, N.M.; Penney, A.; Zebrack, B. Providing developmentally appropriate psychosocial care to adolescent and young adult cancer survivors. Cancer 2011, 117, 2329–2334. [Google Scholar] [CrossRef] [Green Version]
- Treadgold, C.L.; Kuperberg, A. Been there, done that, wrote the blog: The choices and challenges of supporting adolescents and young adults with cancer. J. Clin. Oncol. 2010, 28, 4842–4849. [Google Scholar] [CrossRef]
- Parsons, H.M.; Harlan, L.C.; Schmidt, S.; Keegan, T.H.M.; Lynch, C.F.; Kent, E.E.; Xiao-Cheng, W.; Schwartz, S.M.; Chu, R.L.; Keel, G.; et al. Who Treats Adolescents and Young Adults with Cancer/ A Report from the AYA HOPE Study. J. Adolesc. Young Adult Oncol. 2015, 4, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.K.; Zebrack, B. What do adolescents and young adults want from cancer resources? Insights from a Delphi panel of AYA patients. Support Cancer Care 2017, 25, 119–126. [Google Scholar] [CrossRef]
- Kazak, A.K.; Brier, M.; Alderfer, M.A.; Reilly, A.; Fooks Parker, S.; Rogerwick, S.; Diltaranto, S.; Barakat, L.P. Screening for Psychosocial Risk in Pediatric Cancer. Pediatr. Blood Cancer 2013, 59, 822–827. [Google Scholar] [CrossRef] [Green Version]
- Kazak, A.E.; Schneider, S.; Didonato, S.; Pai, A.L. Family psychosocial risk screening guided by the pediatric psychosocial preventative health model (PPPHM) using the Psychosocial Assessment Tool (PAT). Acta Oncol. 2015, 54, 574–580. [Google Scholar] [CrossRef]
- Hutchinson, J.W.; Stafford, E.M. Changing Parental Opinions About Teen Privacy Through Education. Pediatrics 2005, 116, 966–971. [Google Scholar] [CrossRef]
- Robinson, G.L.; Gilbertson, A.D.; Litwack, L. The effects of a psychiatric patient education to medication program on post-discharge compliance. Psychiatr. Q. 1986, 58, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Avval, F.Z.; Jarahi, L.; Ghazvini, K.; Youssefi, M. Distribution of Handouts in Undergraduate Class to Create More Effective Educational Environment. Int. J. Educ. Res. 2013, 12, 1–6. [Google Scholar]
- Wolfson, J.A.; Sun, C.L.; Wyatt, L.P.; Hurria, A.; Bhatia, S. Impact of care at comprehensive cancer centers on outcome: Results from a population-based study. Cancer 2015, 121, 3885–3893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atieno, O.P. An analysis of the strengths and limitation of qualitative and quantitative research paradigms. Probl. Educ. 21st Century 2009, 13, 13–38. [Google Scholar]
- Choudhury, S. Culturing the adolescent brain: What can neuroscience learn from anthropology? Soc. Cogn. Affect. Neurosci. 2009, 5, 159–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Demographic Variable | Total Sample | AYA | Caregiver | AYA of Caregiver |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n | |
| Age | ||||
| Mean (M) | 32.2 years | 18.9 years | 45.6 years | 16.2 years |
| Standard Deviation (SD) | 13.9 years | 3 years | 4.9 years | 3.9 years |
| 15–17 | 4 (20%) | 4 (40%) | - | 7 |
| 18–23 | 4 (20%) | 4 (40%) | - | 3 |
| 24–29 | 2 (10%) | 2 (20%) | - | - |
| 30–35 | - | - | - | - |
| 36–41 | 2 (10%) | - | 2 (20%) | - |
| 42–47 | 4 (20%) | - | 4 (40%) | - |
| 48 and older | 4 (20%) | - | 4 (40%) | - |
| Sex | ||||
| Male | 9 (45%) | 7 (70%) | 2 (20%) | 6 |
| Female | 11 (55%) | 3 (30%) | 8 (80%) | 4 |
| Race | ||||
| White | 11(55%) | 4 (40%) | 7 (70%) | 7 |
| Black | 7 (35%) | 4 (40%) | 3 (30%) | 3 |
| Asian | 1 (5%) | 1 (10%) | - | - |
| Other | 1 (5%) | 1 (10%) | - | - |
| Ethnicity | ||||
| Hispanic | 5 (25%) | 2 (20%) | 3 (30%) | 3 |
| Non-Hispanic | 15 (75%) | 8 (80%) | 7 (70%) | 7 |
| Insurance 1 | ||||
| Public | 10 (50%) | 3 (30%) | 7 (70%) | 7 |
| Private | 10 (50%) | 7 (70%) | 3 (30%) | 3 |
| Education | ||||
| Partial high school | 6 (30%) | 6 (60%) | - | 8 |
| High school graduate | 4 (20%) | 1 (10%) | 3 (30%) | 2 |
| Partial college | 3 (15%) | 2 (20%) | 1 (10%) | - |
| Standard college graduate | 4 (20%) | 1 (10%) | 3 (30%) | - |
| Graduate professional training | 2 (10%) | - | 2 (20%) | - |
| Marital Status | ||||
| Married | 6 (30%) | 1 (10%) | 5 (50%) | - |
| Single | 11 (55%) | 8 (80%) | 3 (30%) | 10 |
| Separated | 1 (5%) | - | 1 (10%) | - |
| Divorced | 1 (5%) | - | 1 (10%) | - |
| Other | 1 (5%) | 1 (10%) | - | - |
| Employment Status | ||||
| Working full-time | 5 (25%) | 1 (10%) | 4 (40%) | - |
| Working part-time | 2 (10%) | 1 (10%) | 1 (10%) | 1 |
| Homemaker | 3 (15%) | - | 3 (30%) | - |
| Unemployed | 1 (5%) | 1 (10%) | - | 2 |
| Temporarily laid off (FMLA) | 3 (15%) | 2 (20%) | 1 (10%) | - |
| Student | 5 (25%) | 5 (50%) | - | 6 |
| Failed to respond | 1 (5%) | - | 1 (10%) | - |
| Disabled | - | - | - | 1 |
| Measure | AYA | Caregiver | ||
|---|---|---|---|---|
| M | Interpretation | M | Interpretation | |
| AHS (raw) 1 | range = 8–64 | |||
| Total Hope | 58 | high | 56.3 | high |
| Agency | 27.2 | - | 27.2 | - |
| Pathways | 28.6 | - | 28.6 | - |
| DASS-21 (raw) 2 | range = 0–7 | |||
| Depression | 3.8 | normal | - | - |
| Anxiety | 3.9 | mild | - | - |
| Stress | 6.9 | normal | - | - |
| PedsQL-C (SS) 3 | range = 0–100 | |||
| Total | 72.6 | average | 68.7 | average |
| Physical | 59 | average | 64 | average |
| Emotional | 79.6 | average | 72.8 | average |
| Cognitive | 73.3 | average | 71.4 | average |
| Social | 74 | average | 72.9 | average |
| MPSS (raw) 4 | range = 1–7 | |||
| Total | 5.7 | high | - | - |
| Family | 5.9 | high | - | - |
| Friends | 5.5 | high | - | - |
| Significant other | 5.6 | high | - | - |
| General Support | Q1: “I think family is probably the most important thing because, you know, friends come and go, but family are always there for you. And that, I think you really, you pick up on that when you’re going through this and, um, so I think making sure you have family that are, that are close to you and that can be there for you and, um, you know provide emotional support, um, is a really big deal with getting, with getting through this” (2A) 1 |
| Q2: “Just being here for me and making sure that I’m okay mentally and emotionally to the best of their abilities. They really go above and beyond for me to the best they can” (8A) | |
| Presence | Q3: “It really helps knowing that I have her there and mostly all the time so, I know a lot of kids my age, you know, don’t have that. And she also stays in the hospital with me when I’m here and she spends the night, so you know having someone there all the time I think really helps because you do get lonely in the hospital and even when you’re at, when you’re at home, ‘cause I’m not able to go to college or have a job right now so having someone to talk to you about a certain things really helps” (2A) |
| Q4: “She really likes it when we’re here. Just to be here is important for her” (13C) | |
| Everyday Tasks | Q5: “And I’m very happy to do things for him. And I think maybe I shouldn’t do that as much. To let him, you know, do things that he can. I know that there are some things that he just can’t do. A lot of times he’ll ask me to open a jar or something for him because he just, he can’t grip it” (13C) |
| Q6: “She helps me get up and use the restroom. I’m kind of wobbly, so she helps me with that” (6A) | |
| Q7: “Just to kind of help her with the day-to-day things like, you know, if she’s especially when she’s in pain, she likes someone to be there. Um, or to help her with food like ordering the food in the hospital. Um, go to the bathroom. Kind of get changed. Um, Yeah. Just things like that” (12C) | |
| Maintaining Autonomy | Q8: “He needed his space, we needed our space. Like now I’ll say, ‘I’m going to go get my breakfast.’ And he’ll be like, ‘Yeah you don’t have to hurry back.’ I’m like, ‘Okay.’ […] I’m trying to protect his privacy, um, that’s the other thing is protecting his privacy. So we kind of tried to establish our boundaries to start with” (16C) |
| Q9: “That made a huge difference. Having those couple of hours of privacy, for him to connect with his friends and talk silly […] so now, I’m taking the liberty to leave the room. I’m taking the liberty to walk around, uh, the hospital and give him, uh, some, uh, space. And he’ll call me if I’m gone too long, he’ll call me” (20C) | |
| Advocate | Q10: “It’s nice that she’s here so that when the doctors come in and she can listen and ask questions and make sure a double, like we said earlier, a double set of ears” (5A) |
| Q11: “I also contacted the, um, uh, the psychologist here and she came in and talked to him and, um, and I said, ‘use all the tools that are available to you if, you know, if you, if you think she will be better, use her. Um, if you just need somebody to pray for you, you know who to call, and I just want you to have every tool’” (16C) | |
| Q12: “I’m the one who has to say, ‘Oh, well last week when he had the lumbar puncture, he had a few rough days after that.’ And he’s like, ‘Oh yeah I forgot’” (17C) | |
| Positive Attitude | Q13: “‘Cause my dad, gosh, he’s like the silliest person ever. But I feel like he’s the reason why I can keep going because even if things should be sad, he doesn’t make it sad. He really doesn’t make it sad, he’s just, he can never stop joking” (8A) |
| Q14: “So then I had to pick up the slack and I had to encourage him and I had to let him know, ‘hey, you know, we’re gonna, uh, face this. And we’re gonna be good.’ And, uh, ‘so whatever you read on the internet, you know, that’s, that’s their report. But we have a better report. And this is what’s going on, and this is what we’re going to do’” (20C) |
| Category | Quotes |
|---|---|
| Presence | Q15: “I’m kind of limited on what I can do, I can’t like go out and hang out with all my friends like I used to, you know, but when they come and see me I think, I think that’s really helpful ‘cause, you know, it’s gives me time to interact with my friends and someone my age” (2A) |
| Q16: “Sometimes they bring me stuff like food, because they know I get hungry sometimes, you know. And … I don’t know, just keeping me company in general” (8A) | |
| Communication/Contact | Q17: “At the beginning they just messaged me stuff. Just saying how I’m doing and stuff […] It’s kind of like knowing that [they’re] there feels good in a way, yeah. Seeing that you’re not exactly alone in this process” (1A) |
| Q18: “I do I think they helped. Even though they weren’t always here physically or anything, like it, luckily he had his cell phone […] he could text them different things” (11C) | |
| Distraction | Q19: “There was one time, um, this friend of his came over, a young lady. And she brought food and movies to watch. And I mean, he was having a great time. It was really good” (17C) |
| Q20: “They bought sushi […] Um, and so they just came by, ate, watched movies and stuff like that” (18C) | |
| Encouragement/Gestures | Q21: “his friends gave him cards and stuff […] made him realize that he still was important to them I think” (11C) |
| Q22: “His Young Life buddies, there were like 60 of them that all got together and FaceTimed and said, ‘Oh we missed you’ […] and ‘we’re praying for you’ […] and they all signed a big poster board and he was pretty excited about that” (16C) |
| Source | Quotes |
|---|---|
| Peers | Q23: “I met some really nice people that have had, have had the same cancer as I have right now, which is not very many, but meeting people that have been through it and them giving you tips, you know, on how to get through, um, when you get delayed for chemo and, um, get off schedule, and um, you know, when you, when you get, had to go to the ER for a fever at 2 in the morning, you know, things like that. You know, like how did you make it through that without losing, you know, all your frustration or whatever and so they gave me, I guess they gave me more hope that I, that I can make it through this so, uh, they’ve been, they’ve been really helpful” (2A) |
| Q24: “With the little game room area, the teenage game room area, I know he, he met some kids and talked to them and went to a couple those little meetings with them and what have you, and I think that probably helped a lot to know how other kids were dealing with it and how they were going through it” (11C) | |
| Q25: “I want to talk to somebody my age because uh, uh, it’s, so, so I can kind of relate to, to, I can kind of relate instead of like talking to like a younger kid” (3A) | |
| Q26: “I mean it would, it would […] not only it would show her of course she’s not the only one, and people are facing the same thing, the same situation […] it seems like they bond better. Yeah because there’s an understanding, shared experience” (19C) | |
| Medical Staff | Q27: “The medical team seem to know what they’re doing and I trusted them to get it done correctly” (5A) |
| Q28: “So uh [my doctor] was, you know, real with me from the beginning, you know, with not everyone survives cancer and so, you know, you have to know that there’s a chance that, you know, you may die from it or whatever and stuff, um, that, that, that was helpful” (2A) | |
| Q29: “One of the nurses brought in a backpack with a blanket and sleep pants and other comfort things. And it was wonderful” (16C) | |
| Q30: “And the, just the wonderful staff that’s here at Children’s also working with him and us I think helped them get through it” (14C) | |
| Spouse/ Significant Other | Q31: “My fiancé’s been a big part of it. He helps me. He knows a lot more than anybody else, than anybody else, and he doesn’t let me just … He doesn’t go by with me just saying, ‘Oh yeah, I’m just having a bad day.’ He wants to know what’s going on […] and, and I actually tell because he can, he can brave through it. And he’s a very strong person, and he’s helped me so much. And sometimes whenever I just need somebody to give me a hug, help me through the day” (9A) |
| Q32: “I mean she’s had a boyfriend for some time now and you know he’s been around, and she’s actually really close with his family and his mother. Um, I know I know when she’s not, when she’s feeling really bad and not feeling … She’s feeling bad, she likes to go over to his house and will stay the nights there” (12C) | |
| School/Work | Q33: “You know some of [her] colleagues or her work, people from work have, um, put together like fundraisers for donations and stuff like that which has been helpful” (12C) |
| Q34: “His teachers um they well his school in general is like they all you know rooting for him, rallying for him, um, his, the senior class um, uh, his teachers. […] Everybody is really trying to be very accommodating to make sure he graduates with the with the school you know” (13C) | |
| Professional or Collegiate Athletes | Q35: “So we’ve had a lot of, like, professional athletes reach out to me and stuff. And I, like actually last week [a professional football player] came to my house and it was really cool to talk to him and I’ve gotten signed autographs from so many, so many players that I can’t even name. But, uh, yeah the sports, the sports players and teams have been really kind to me and that they’ve all kind of reached out to me and, you know, given me hope and, you know, knowing, telling me that, you know, they’re here for me and praying for me so it’s really nice to know that you have those kind of people supporting you as well as your family”(2A) |
| Q36: “There so many good things that happen, I forgot like a [college football] team came up here one time and visited with him the [professional football team] came by one time. Uh, some of the [professional hockey] folks came through what have you […] College football players that came through […] and things of that nature that was just, uh, that was a, that was that was a wonderful thing for him” (11C) | |
| Organizations | Q37: “But, um, we, we went with [a national organization] helped us a lot too we would go to games and stuff that he’d never been, or I’d never been, I had never been to the [professional basketball] game we went. That stuff helped him a lot. […] Especially when he was, like he was homeschooled so he had, for at least a year, he didn’t get to go anywhere, you know, anywhere unless [the national organization] invited him once a week, twice a week somewhere” (14C) |
| Q38: “Then we met a wonderful group that was up here that was really helpful that was [a hunting organization], and he went and got to shoot around with them” (11C) | |
| Community | Q39: “They, they send me Bible verses and they tell me to be strong and they remind me of times that I’ve had difficulty in the past and I’ve already gotten through it” (5A) |
| Q40: “We met, I mean we met people on Facebook that are, you know, um, that that just want to do things for us like bring food over or um they send us like a shirt or you know just little things and it really means a lot when they do that” (2A) |
| Category | Quotes |
|---|---|
| Not Helpful | Q41: “I mean she doesn’t wanna do anything that reminds her of what’s happening. I mean we ended up still going, and someone like tried to talk to her or give her a shirt or something and she just really didn’t like that. She doesn’t like the fuss and she hates like people kind of giving her all that attention. You know doing that kind of stuff. So. Yeah that’s really not helpful and even in here I think she really just doesn’t want to hear about anything with her treatment or disease” (12C) |
| Q42: “It’s kind of hard watching [my parents] argue over [my treatment], you know, ‘cause I don’t really need that right now” (2A) | |
| Q43: “Like nobody knew how to handle it. So every time they would talk to me, all they would talk about was being sick. It’s like, man. Like I’m still the same guy. We played, I’m still the same guy, we played football together since we was like seven, eight years old. I’m still, you know? I still like sports. I still like talk about other things. You know? We talked about, we, we, we didn’t, we didn’t become friends over being sick. So like how come every time we talk it got to be about that?” (4A) | |
| Q44: “And like, even my mom, first chemo she left me by myself. And she didn’t want my dad around ‘cause she doesn’t like seeing him, so she made my dad leave so she can come visit me. So he went to work ‘cause he thought she was gonna spend the day with me. As soon as they brought my first chemo out, I told them, ‘hey, can I wait for my dad?’ ‘Cause I want my dad to be here. And they said, ‘okay, sure.’ And my dad wasn’t showing up, it turned out the 18-wheeler broke down, ‘cause he drives an 18-wheeler. Um, he was waiting for somebody to come get him so he can come see me. And then so they said, ‘hey, we have to start soon.’ So they started. As soon as they start plugging me in, my mom just leaves”.(8A) | |
| Advice to Others | Q45: “My advice would have to be like, would, would be try to treat that person as normal as possible. You know? There’s a lot more to me than just having cancer. You know? And that’s one thing that I will say. Like, don’t make, don’t make the person feel like they got cancer patient attached to their name” (4A) |
| Q46: “it would be nice to see more resources for his age group. I think they kind of get lost. […] Like I saw a Facebook post for, by [the pediatric clinic]. I, you know, they have a page or group or whatever. And they posted something about the […] organization, and it had all these cool events that looked like he would even enjoy. There was like a [golf] thing, and a gaming thing. And a couple other events. I don’t remember what the other ones were. But they top out at 18…And I’m like, oh, he’s 20. You know? He would still enjoy doing stuff like this” (17C) | |
| Q47: “I wish that [my friends] knew how to help me more […] I wish they knew kind of like how to, how to relate to me more and understand what I’m going through […] I think I guess just being around me more and, um, you know, maybe coming to the hospital, and then seeing all this. I think when you go to the hospital and, you know, you, you see someone, you know, kind of going through this, um, it’s easier, you know, you understand it more, you know? […] and so, um, I guess if they came and saw me in the hospital they, they would probably you know, be like, ‘wow this, that’s, that’s something else’ having to, having to stay you know here all the time and go here, you know, all the time for blood work and stuff” (2A) | |
| Q48: “Um, I think that, um, I don’t know, I would say maybe in the future, um, I mean I know it’s, it’s limited or, you know, the hospital, but I would say like more so putting teens together and then putting little kids together just so maybe she could have talked to somebody else going through the same thing […] or having a you know teen day or something” (15C) | |
| Q49: “Just to, if the person wants to talk about it, like for anybody in general, if the patient wants to talk about it with you then let ‘em. Let ‘em go all out. Don’t really question ‘em while they’re going. If they want you to ask questions, you know, if they pause and they’re looking for the questions then ask as many as you want, but it’s good to just have somebody to listen to. So just sit there and listen and if they don’t wanna talk about it, then don’t pressure ‘em into it because that’s one of the worst things, and it’d be nice to just have a regular conversation and not be seen as somebody that’s, you know, don’t see just the cancer. See me as well” (9A) | |
| Q50: “When things come up, you need to talk to the patient and actually take, especially if they got, you know, take their feelings and their opinions and everything into consideration about what’s going on with them. Like, don’t have somebody speaking for them, for, you know? ‘What’s going on.’ ‘Hey.’ You know. ‘Okay, let’s talk to him.’ ‘Let’s see how he feels about this.’ You know? […] Basically, let’s not make them feel like, you know, they’re just so, let’s leave them, not make them feel helpless, you know?” (4A) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pennant, S.; C. Lee, S.; Holm, S.; Triplett, K.N.; Howe-Martin, L.; Campbell, R.; Germann, J. The Role of Social Support in Adolescent/Young Adults Coping with Cancer Treatment. Children 2020, 7, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/children7010002
Pennant S, C. Lee S, Holm S, Triplett KN, Howe-Martin L, Campbell R, Germann J. The Role of Social Support in Adolescent/Young Adults Coping with Cancer Treatment. Children. 2020; 7(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/children7010002
Chicago/Turabian StylePennant, Sarah, Simon C. Lee, Suzanne Holm, Kelli N. Triplett, Laura Howe-Martin, Ryan Campbell, and Julie Germann. 2020. "The Role of Social Support in Adolescent/Young Adults Coping with Cancer Treatment" Children 7, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/children7010002