Good Subjective Outcomes, Stable Knee and High Return to Sport after Tibial Eminence Avulsion Fracture in Children

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Treatment
2.2. Patients Evaluation
2.3. Statistical Analysis
3. Results
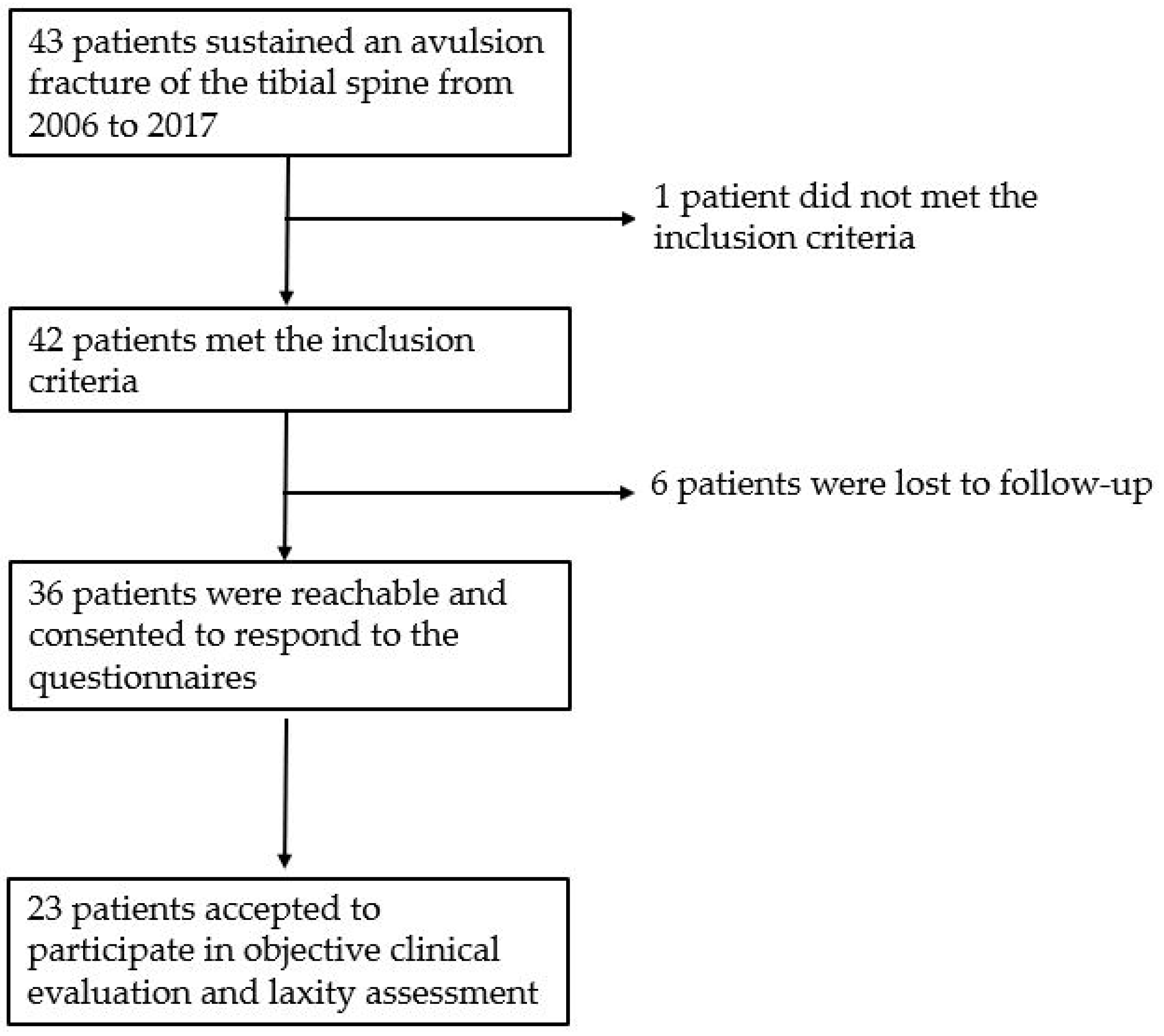
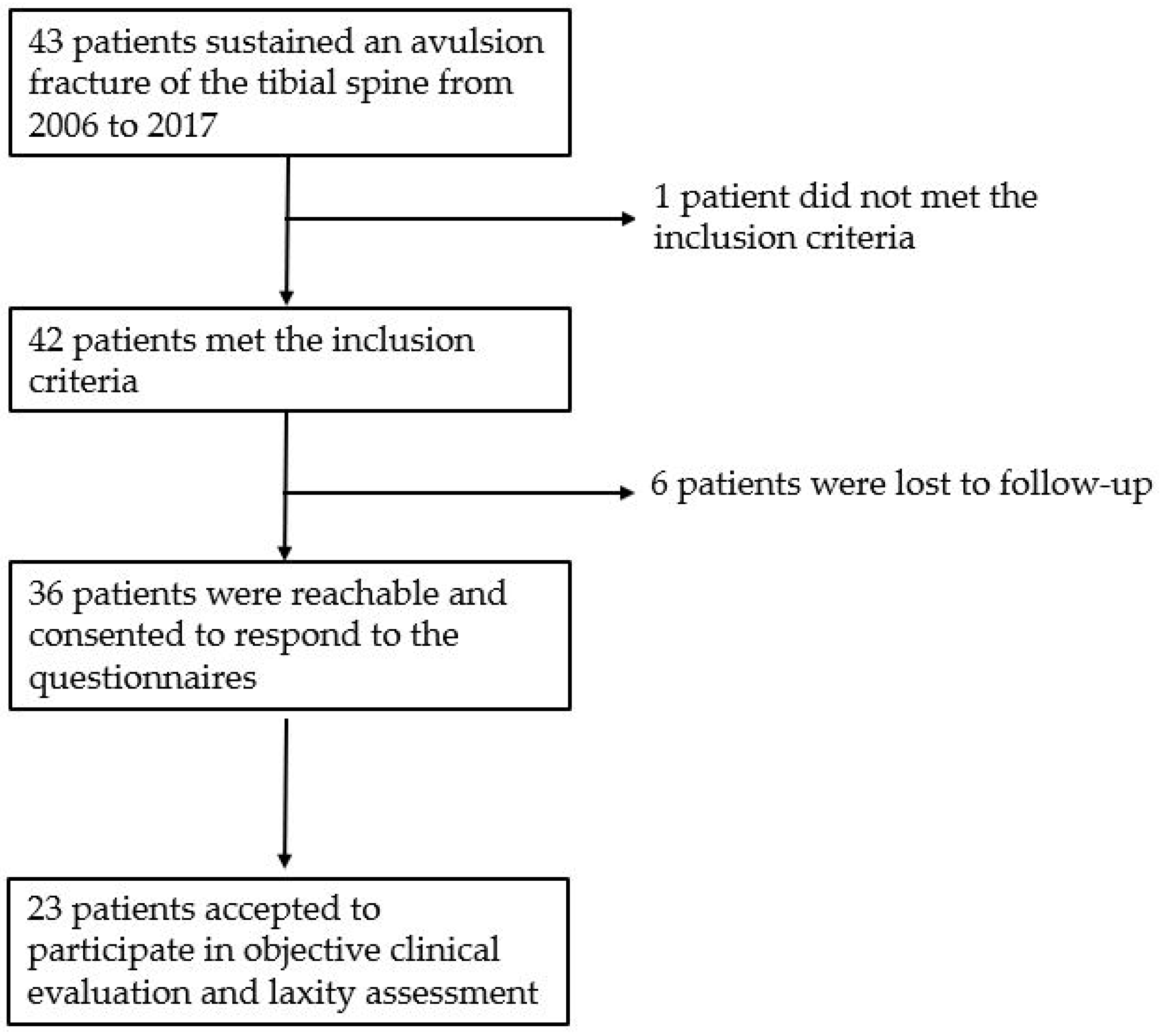
3.1. Patients Population
3.2. Clinical Course, Fracture Healing and Complications
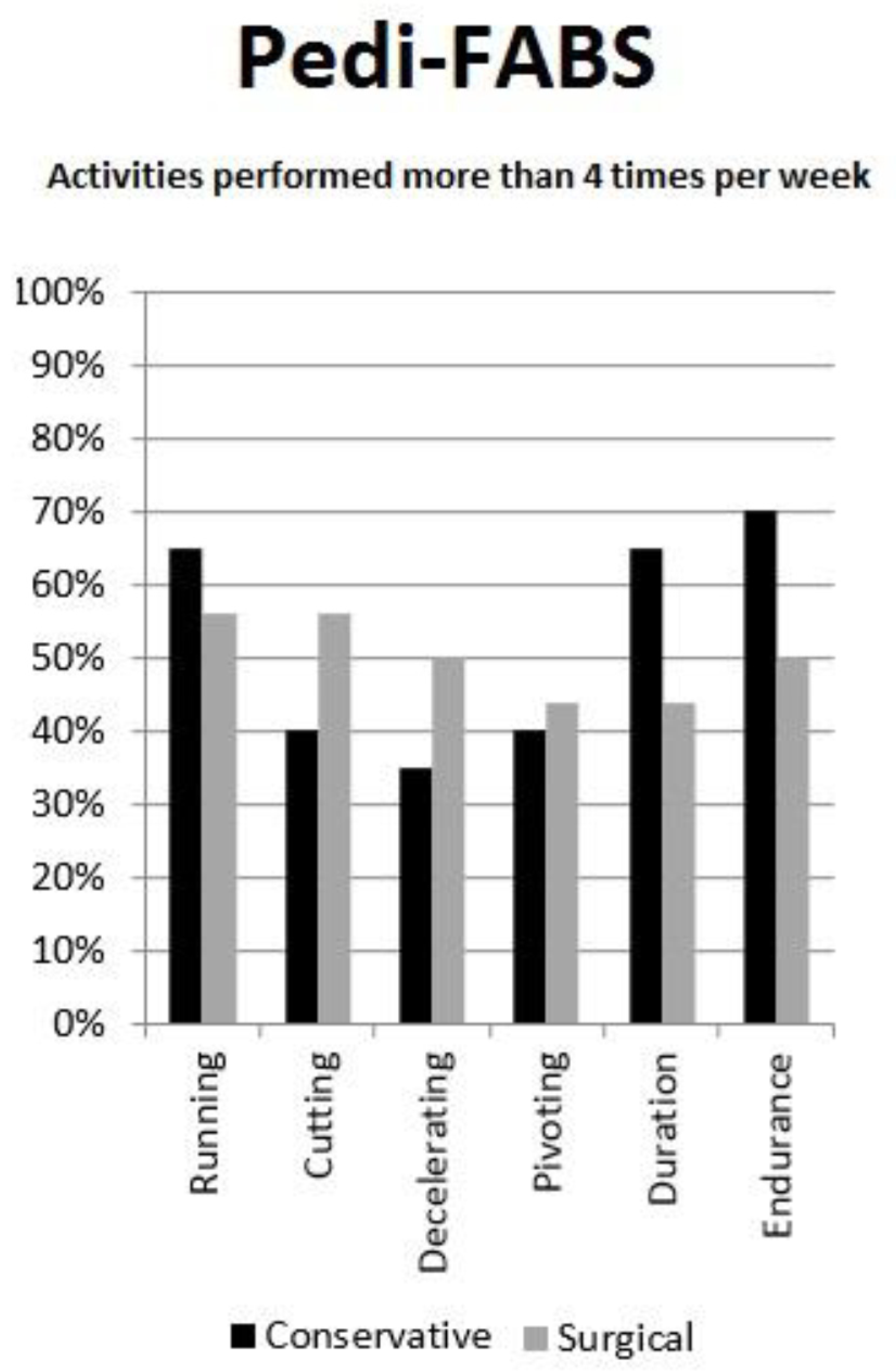
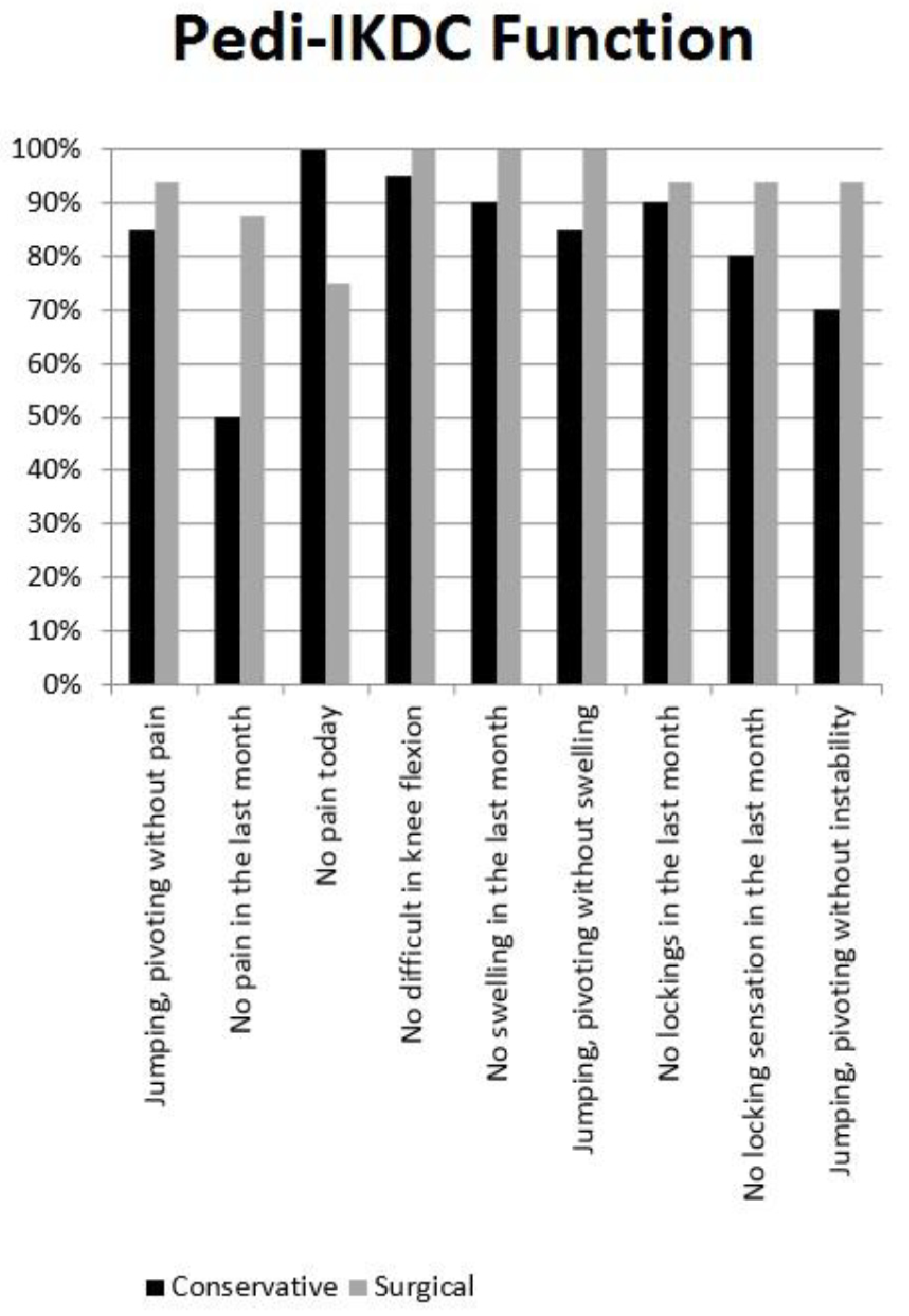
3.3. Subjective Clinical Evaluation and Return to Sport
3.4. Objective Clinical Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ingram, J.G.; Fields, S.K.; Comstock, R.D.; Yard, E.E. Epidemiology of knee injuries among boys and girls in US high school athletics. Am. J. Sports Med. 2008, 36, 1116–1122. [Google Scholar] [CrossRef]
- Bergerault, F.; Le Carrou, T.; De Courtivron, B.; Bonnard, C. Entorses du genou. In Fractures de l’enfant, Monographie du GEOP; Clavert, J.M., Ligier, J.N., Lascombes, P., Metaizeau, J.P., Karger, C., Eds.; Sauramps Médical: Montpellier, France, 2002; pp. 237–245. [Google Scholar]
- Meyers, M.H.; McKeever, F.M. Fracture of the intercondylar eminence of the Tibia. J. Bone Jt. Surg. Am. Vol. 1959, 41, 209–222. [Google Scholar] [CrossRef] [Green Version]
- Zaricznyj, B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J. Bone Jt. Surg. Am. Vol. 1977, 59, 1111–1114. [Google Scholar] [CrossRef]
- Coyle, C.; Jagernauth, S.; Ramachandran, M. Tibial eminence fractures in the paediatric population: A systematic review. J. Child. Orthop. 2014, 8, 149–159. [Google Scholar] [CrossRef] [Green Version]
- Gans, I.; Baldwin, K.D.; Ganley, T.J. Treatment and management outcomes of tibial eminence fractures in pediatric patients: A systematic review. Am. J. Sports Med. 2014, 42, 1743–1750. [Google Scholar] [CrossRef]
- Jackson, T.J.; Storey, E.P.; Ganley, T.J. The surgical management of Tibial spine fractures in children: A survey of the Pediatric Orthopaedic Society of North America (POSNA). J. Pediatr. Orthop. 2019, 39, e572–e577. [Google Scholar] [CrossRef]
- Osti, L.; Buda, M.; Soldati, F.; Del Buono, A.; Osti, R.; Maffulli, N. Arthroscopic treatment of tibial eminence fracture: A systematic review of different fixation methods. Br. Med. Bull. 2016, 118, 73–90. [Google Scholar] [CrossRef] [Green Version]
- Bogunovic, L.; Tarabichi, M.; Harris, D.; Wright, R.W. Treatment of Tibial eminence fractures: A systematic review. J. Knee Surg. 2014, 28, 255–262. [Google Scholar] [CrossRef]
- Callanan, M.; Allen, J.; Flutie, B.; Tepolt, F.; Miller, P.E.; Kramer, D.; Kocher, M.S. Suture versus screw fixation of Tibial spine fractures in children and adolescents: A comparative study. Orthop. J. Sports Med. 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Casalonga, A.; Bourelle, S.; Chalencon, F.; De Oliviera, L.; Gautheron, V.; Cottalorda, J. Tibial intercondylar eminence fractures in children: The long-term perspective. Orthop. Traumatol. Surg. Res. 2010, 96, 525–530. [Google Scholar] [CrossRef] [Green Version]
- Edmonds, E.W.; Fornari, E.D.; Dashe, J.; Roocroft, J.H.; King, M.M.; Pennock, A.T. Results of displaced pediatric Tibial spine fractures: A comparison between open, arthroscopic, and closed management. J. Pediatr. Orthop. 2015, 35, 651–656. [Google Scholar] [CrossRef]
- Tudisco, C.; Giovarruscio, R.; Febo, A.; Savarese, E.; Bisicchia, S. Intercondylar eminence avulsion fracture in children: Long-term follow-up of 14 cases at the end of skeletal growth. J. Pediatr. Orthop. B 2010, 19, 403–408. [Google Scholar] [CrossRef]
- Macchiarola, L.; Grassi, A.; Di Paolo, S.; Pizza, N.; Trisolino, G.; Stallone, S.; Stilli, S.; Zaffagnini, S. The Italian cross-cultural adaptations of the paediatric International Knee Documentation Committee Score and the Hospital for Special Surgery Paediatric Functional Activity Brief Scale are reliable instruments in paediatric population. Knee Surg. Sports Traumatol. Arthrosc. 2020, 1–6. [Google Scholar] [CrossRef]
- Anderson, A.F.; Kocher, M. Paper # 74: Reliability, validity and responsiveness of a modified international knee documentation committee subjective knee form (Pedi-Ikdc) in children with knee disorders. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, e115. [Google Scholar] [CrossRef]
- Jacobsen, J.S.; Knudsen, P.; Fynbo, C.; Rolving, N.; Warming, S. Reproducibility and responsiveness of a D anish P edi-IKDC subjective knee form for children with knee disorders. Scand. J. Med. Sci. Sports 2016, 26, 1408–1414. [Google Scholar] [CrossRef]
- Fabricant, P.D.; Robles, A.; Downey-Zayas, T.; Do, H.T.; Marx, R.G.; Widmann, R.F.; Green, D.W. Development and validation of a pediatric sports activity rating scale: The hospital for special surgery pediatric functional activity brief scale (HSS Pedi-FABS). Am. J. Sports Med. 2013, 41, 2421–2429. [Google Scholar] [CrossRef]
- Van Eck, C.F.; Loopik, M.; Bekerom, M.P.V.D.; Fu, F.H.; Kerkhoffs, G.M.M.J. Methods to diagnose acute anterior cruciate ligament rupture: A meta-analysis of instrumented knee laxity tests. Knee Surg. Sports Traumatol. Arthrosc. 2012, 21, 1989–1997. [Google Scholar] [CrossRef]
- Ganko, A.; Engebretsen, L.; Ozer, H. The Rolimeter: A new arthrometer compared with the KT-1000. Knee Surg. Sports Traumatol. Arthrosc. 2000, 8, 36–39. [Google Scholar] [CrossRef]
- Raggi, F.; Di Sarsina, T.R.; Signorelli, C.; Muccioli, G.M.M.; MacChiarola, L.; Cucurnia, I.; Romagnoli, M.; Grassi, A.; Zaffagnini, S. Triaxial accelerometer can quantify the Lachman test similarly to standard arthrometers. Knee Surg. Sports Traumatol. Arthrosc. 2018, 27, 2698–2703. [Google Scholar] [CrossRef]
- Berruto, M.; Uboldi, F.M.; Gala, L.; Marelli, B.; Albisetti, W. Is triaxial accelerometer reliable in the evaluation and grading of knee pivot-shift phenomenon? Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 981–985. [Google Scholar] [CrossRef]
- Branch, T.; Mayr, H.O.; Browne, J.E.; Campbell, J.C.; Stoehr, A.; Jacobs, C.A. Instrumented examination of anterior cruciate ligament injuries: Minimizing flaws of the manual clinical examination. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 997–1004. [Google Scholar] [CrossRef]
- Hefti, E.; Müller, W.; Jakob, R.P.; Stäubli, H.-U. Evaluation of knee ligament injuries with the IKDC form. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 226–234. [Google Scholar] [CrossRef]
- Muccioli, G.M.M.; Signorelli, C.; Grassi, A.; Di Sarsina, T.R.; Raggi, F.; Carbone, G.; MacChiarola, L.; Vaccari, V.; Zaffagnini, S. In-vivo pivot-shift test measured with inertial sensors correlates with the IKDC grade. J. ISAKOS Jt. Disord. Orthop. Sports Med. 2018, 3, 89–93. [Google Scholar] [CrossRef]
- Zaffagnini, S.; Lopomo, N.F.; Signorelli, C.; Muccioli, G.M.M.; Bonanzinga, T.; Grassi, A.; Visani, A.; Marcacci, M. Innovative technology for knee laxity evaluation: Clinical applicability and reliability of inertial sensors for quantitative analysis of the pivot-shift test. Clin. Sports Med. 2013, 32, 61–70. [Google Scholar] [CrossRef]
- Fabricant, P.D.; Tepolt, F.A.; Kocher, M.S. Range of motion improvement following surgical management of knee Arthrofibrosis in children and adolescents. J. Pediatr. Orthop. 2018, 38, e495–e500. [Google Scholar] [CrossRef]
- Janarv, P.-M.; Westblad, P.; Johansson, C.; Hirsch, G. Long-term follow-up of anterior Tibial spine fractures in children. J. Pediatr. Orthop. 1995, 15, 63–68. [Google Scholar] [CrossRef]
- Perugia, D.; Basiglini, L.; Vadalà, A.; Ferretti, A. Clinical and radiological results of arthroscopically treated tibial spine fractures in childhood. Int. Orthop. 2008, 33, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Iversen, M.D.; Lee, B.; Connell, P.; Andersen, J.; Anderson, A.F.; Kocher, M.S. Validity and comprehensibility of the international knee documentation committee subjective knee evaluation form in children. Scand. J. Med. Sci. Sports 2010, 20, e87–e95. [Google Scholar] [CrossRef]
- Shirazi, C.P.; Israel, H.A.; Kaar, S.G. Is the marx activity scale reliable in patients younger than 18 years? Sports Health A Multidiscip. Approach 2015, 8, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Adams, A.J.; Talathi, N.S.; Gandhi, J.S.; Patel, N.M.; Ganley, T.J. Tibial spine fractures in children: Evaluation, management, and future directions. J. Knee Surg. 2018, 31, 374–381. [Google Scholar] [CrossRef]
- Zhao, C.; Bi, Q.; Bi, M. Management of a type two avulsion fracture of the tibial intercondylar eminence in children: Arthroscopic suture fixation versus conservative immobilization+. Int. Orthop. 2018, 42, 1363–1369. [Google Scholar] [CrossRef]
- Wilfinger, C.; Castellani, C.; Raith, J.; Pilhatsch, A.; Höllwarth, M.; Weinberg, A.M. Nonoperative treatment of Tibial spine fractures in children-38 patients with a minimum follow-up of 1 year. J. Orthop. Trauma 2009, 23, 519–524. [Google Scholar] [CrossRef]
- Willis, R.B.; Blokker, C.; Stoll, T.M.; Paterson, D.C.; Galpin, R.D. Long-term follow-up of anterior Tibial eminence fractures. J. Pediatr. Orthop. 1993, 13, 361–364. [Google Scholar] [CrossRef]
- Doorley, J.D.; Womble, M.N. Psychology of return to play after anterior cruciate ligament injury. In ACL Injuries in Female Athlete, 1st ed.; West, R., Bryant, B., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 95–109. [Google Scholar]
- Zaffagnini, S.; Russo, R.L.; Muccioli, G.M.M.; Marcacci, M. The Videoinsight® method: Improving rehabilitation following anterior cruciate ligament reconstruction—A preliminary study. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 851–858. [Google Scholar] [CrossRef]
- Scrimshire, A.; Gawad, M.; Davies, R.; George, H. Management and outcomes of isolated paediatric tibial spine fractures. Injury 2018, 49, 437–442. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | Type of Trauma | ||
|---|---|---|---|
| 34 | 15 | Ski/Snowboarding | |
| 8 | Motocross | ||
| Sport | 4 | Soccer | |
| 3 | Basket | ||
| 3 | Biking | ||
| 1 | Volleyball | ||
| 3 | Car accident | ||
| 5 | Fall | ||
| Non-Operative | Operative | Total | p | |
|---|---|---|---|---|
| N° of patients | 26 | 16 | 42 | |
| Hospital A/Hospital B Ratio | 17/9 | 5/11 | 22/20 | 0.055 |
| Male/Female | 10/16 | 10/6 | 20/22 | 0.17 |
| Left/Right | 7/19 | 11/5 | 18/24 | 0.01 |
| Meyers and McKeever class. (I/II/IIIA/IIIB/IV) | 13/8/3/1/1 | 0/8/5/3/0 | 13/16/8/4/1 | 0.005 |
| Age at trauma | 10.6 ± 3.6 | 11.3 ± 2.5 | 10.8 ± 3.2 | 0.46 |
| Follow-up (years) | 8.0 ± 3.7 | 5.9 ± 2.6 | 6.9 ± 3.6 | 0.02 |
| Age at last follow-up | 18.4 ± 5.0 | 16.6 ± 4.1 | 17.7 ± 4.8 | 0.24 |
| OUTCOME VARIABLE | Non-Operative | Operative | Total | p Value |
|---|---|---|---|---|
| PROs Questionnaires | ||||
| Number of patients | 20 | 16 | 36 | |
| Pedi-IKDC | 95.4 ± 6.6 | 97.8 ± 4.0 | 96.4 ± 5.7 | 0.58 |
| Pedi FABS | 22.1 ± 5.6 | 22.5 ± 6.8 | 22.2 ± 5.9 | 0.32 |
| Instrumental Knee laxity | ||||
| Number of patients | 13 | 10 | 23 | |
| KT 1000 | 0.15 ± 3.05 | 0.8 ± 1.68 | 0.4 ± 2.46 | 0.16 |
| Rolimeter | 0.46 ± 1.12 | 0.7 ± 1.63 | 0.6 ± 1.32 | 0.45 |
| KiRA | 0.14 ± 0.66 | −0.13 ± 0.89 | 0.05 ± 0.74 | 0.37 |
| Level of Sport | Male | Female | TOT |
|---|---|---|---|
| Elite | Soccer × 2 Motocross × 2 Ski | Athletics Baseball Dance/Ballet | 8 |
| Competitive | Soccer × 2 Basket × 2 Motocross Snowboard Swim | Ski/Snowboard × 3 Dance/Ballet × 2 Horse Riding | 13 |
| Amateur | Soccer Basket | Athletics × 2 Swim × 2 Dance/Ballet | 7 |
| TOT | 14 | 14 | 28 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stallone, S.; Selleri, F.; Trisolino, G.; Grassi, A.; Macchiarola, L.; Magnani, M.; Olivotto, E.; Zaffagnini, S.; Stilli, S.; Catani, F. Good Subjective Outcomes, Stable Knee and High Return to Sport after Tibial Eminence Avulsion Fracture in Children. Children 2020, 7, 173. https://0-doi-org.brum.beds.ac.uk/10.3390/children7100173
Stallone S, Selleri F, Trisolino G, Grassi A, Macchiarola L, Magnani M, Olivotto E, Zaffagnini S, Stilli S, Catani F. Good Subjective Outcomes, Stable Knee and High Return to Sport after Tibial Eminence Avulsion Fracture in Children. Children. 2020; 7(10):173. https://0-doi-org.brum.beds.ac.uk/10.3390/children7100173
Chicago/Turabian StyleStallone, Stefano, Filippo Selleri, Giovanni Trisolino, Alberto Grassi, Luca Macchiarola, Marina Magnani, Eleonora Olivotto, Stefano Zaffagnini, Stefano Stilli, and Fabio Catani. 2020. "Good Subjective Outcomes, Stable Knee and High Return to Sport after Tibial Eminence Avulsion Fracture in Children" Children 7, no. 10: 173. https://0-doi-org.brum.beds.ac.uk/10.3390/children7100173