Dietary Diversity and Nutritional Status of Preschool Children in North West Province, South Africa: A Cross Sectional Study



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Participants
2.4. Sample Size and Sampling Procedure
2.5. Data Collection
2.5.1. Socio-Demographics of Study Participants
2.5.2. Dietary Diversity Score
2.5.3. Anthropometric Measurements and Nutritional Indicators
2.6. Statistical Analysis
2.7. Ethics Statement
3. Results
3.1. Characteristics of Children and Mothers
3.2. Nutritional Status of Children
3.3. Dietary Diversity
3.3.1. Dietary Diversity Scores of the Children by Sex and Age
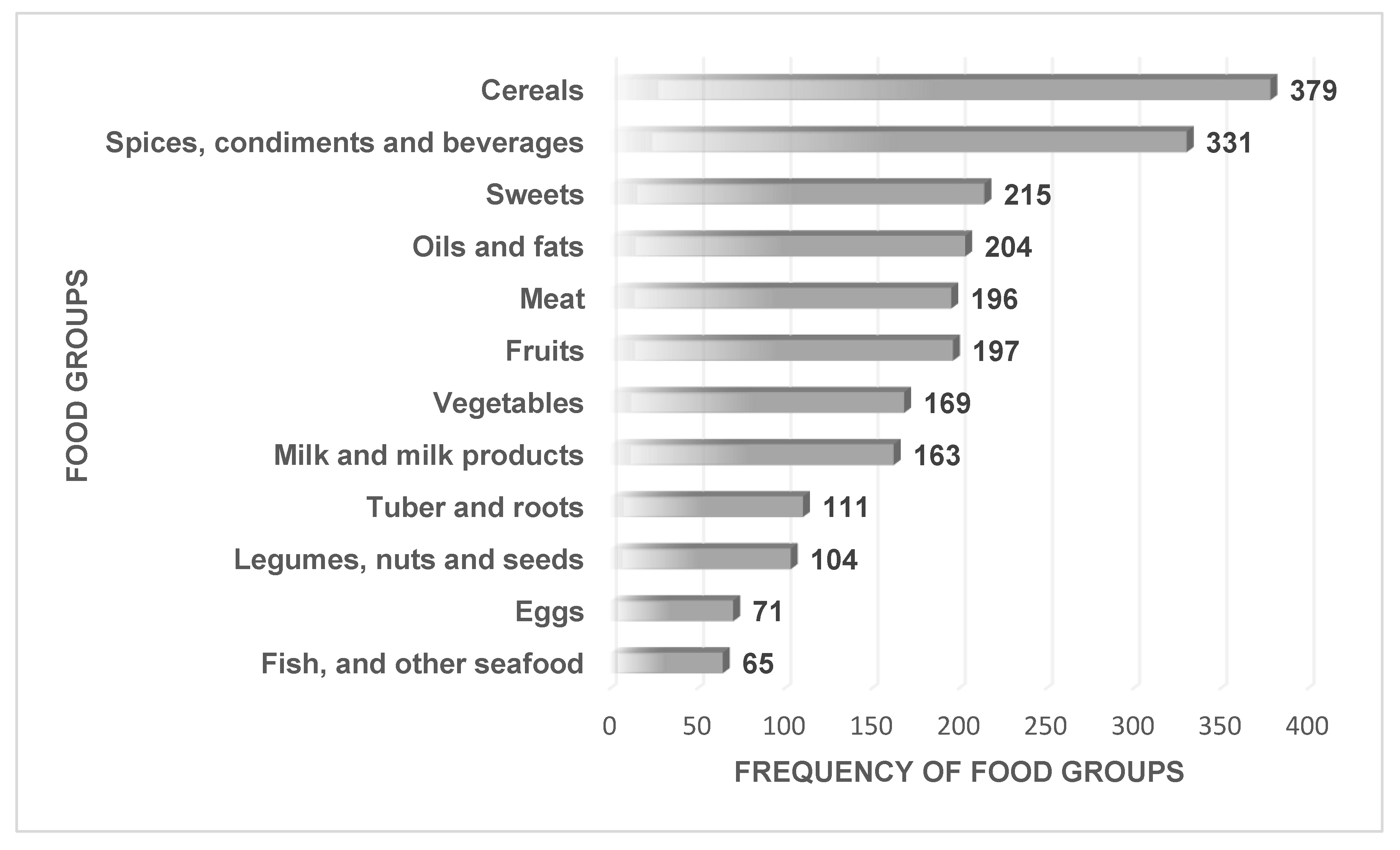
3.3.2. Diversity by Consumption Frequencies of Food Groups
3.4. Association between Dietary Diversity Score and Nutritional Status
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ruel, M.T. Is dietary diversity an indicator of food security or dietary quality? A review of measurement issues and research needs. Food Nutr. Bull. 2003, 24, 231–232. [Google Scholar] [CrossRef]
- Pan American Health Organization (PAHO); World Health Organization (WHO). Guiding Principles for Complemen-Tary Feeding of the Breastfed Child; PAHO: Washington, DC, USA; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Leyna, G.H.; Mmbaga, E.J.; Mnyika, K.S.; Hussain, A.; Klepp, K.-I. Food insecurity is associated with food consumption patterns and anthropometric measures but not serum micronutrient levels in adults in rural Tanzania. Public Health Nutr. 2010, 13, 1438–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Preparation and Use of Food-Based Dietary Guidelines; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Du Plessis, L.M.; Kruger, H.; Sweet, L. Complementary feeding: A critical window of opportunity from six months onwards. S. Afr. J. Clin. Nutr. 2013, 26, S129–S140. [Google Scholar]
- WHO. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1. In Proceedings of the Definitions: Conclusions of a Consensus Meeting, Washington, DC, USA, 6–8 November 2007. [Google Scholar]
- Khamis, A.G.; Mwanri, A.W.; Ntwenya, J.E.; Kreppel, K. The influence of dietary diversity on the nutritional status of children between 6 and 23 months of age in Tanzania. BMC Pediatr. 2019, 19, 518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. The Millennium Development Goals Report; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Chakona, G. Social circumstances and cultural beliefs influence maternal nutrition, breastfeeding and child feeding practices in South Africa. Nutr. J. 2020, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Arimond, M.; Ruel, M.T. Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. J. Nutr. 2004, 134, 2579–2585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nti, C.A. Dietary diversity is associated with nutrient intakes and nutritional status of children in Ghana. Asian J. Med. Sci. 2011, 2, 105–109. [Google Scholar] [CrossRef] [Green Version]
- Caulfield, L.E.; Richard, S.A.; Rivera, J.A.; Musgrove, P.; Black, R.E. Stunting, wasting, and micronutrient deficiency disorders. In Disease Control Priorities in Developing Countries, 2nd ed.; Jamison, D.T., Breman, J.G., Measham, A.R., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2006. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK11761/ (accessed on 24 February 2020).
- De Onis, M.; Onyango, A.W. WHO child growth standards. Lancet 2008, 371, 204. [Google Scholar] [CrossRef] [Green Version]
- Onyango, A.W. Dietary diversity, child nutrition and health in contemporary African communities. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2003, 136, 61–69. [Google Scholar] [CrossRef]
- Labadarios, D.; Steyn, N.; Maunder, E.; Macintryre, U.; Gericke, G.; Swart, R.; Huskisson, J.; Dannhauser, A.; Vorster, H.; Nesmvuni, A. The national food consumption survey (NFCS): South Africa, 1999. Public Health Nutr. 2005, 8, 533–543. [Google Scholar] [CrossRef]
- Modjadji, S.; Alberts, M.; Mamabolo, R. Folate and iron status of South African non-pregnant rural women of childbearing age, before and after fortification of foods. S. Afr. J. Clin. Nutr. 2007, 20, 89–93. [Google Scholar] [CrossRef]
- Papathakis, P.C.; Pearson, K.E. Food fortification improves the intake of all fortified nutrients, but fails to meet the estimated dietary requirements for vitamins A and B 6, riboflavin and zinc, in lactating South African women. Public Health Nutr. 2012, 15, 1810–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faber, M.; Laubscher, R.; Berti, C. Poor dietary diversity and low nutrient density of the complementary diet for 6-to 24-month-old children in urban and rural K wa Z ulu-N atal, S outh A frica. Matern. Child Nutr. 2016, 12, 528–545. [Google Scholar] [CrossRef] [PubMed]
- Labadarios, D.; SteynN, M.E.; Macintyre, U.; Swart, R.; Gericke, G. The National Food Con-sumption Survey (NFCS): Children Aged 1–9 Years, South Africa, 1999; South African Department of Health, Directorate of Nutrition: Pretoria, South Africa, 2000.
- National Department of Health (NDoH); Statistics South Africa (Stats SA); South African Medical Research Council (SA MRC); ICF. South Africa Health and Demographic Survey 2016: Key Indicators; NDoH, Stats SA, SAMRC and ICF: Pretoria, South Africa; Rockville, MD, USA, 2017.
- Nzama, P.; Napier, C. Nutritional adequacy of menus offered to children of 2-5 years in registered childcare facilities in Inanda, KwaZulu-Natal Province, South Africa. S. Afr. J. Child Health 2017, 11, 80–85. [Google Scholar] [CrossRef] [Green Version]
- Early Childhood Education. Available online: https://en.wikipedia.org/wiki/Early_childhood_education (accessed on 15 July 2020).
- Skweyiya, D. Minister of Social Development. In The Guidelines for Early Child Development Services; Department of Social Development: Pretoria, South Africa, 2006. [Google Scholar]
- Sisson, S.; Kiger, A.; Anundson, K.; Rasbold, A.; Krampe, M.; Campbell, J.; De Grace, B.; Hoffman, L. Differences in preschool-age children’s dietary intake between meals consumed at childcare and at home. Prev. Med. Rep. 2017, 6, 33–37. [Google Scholar] [CrossRef]
- Steyn, N.; Nel, J.; Nantel, G.; Kennedy, G.; Labadarios, D. Food Variety and Dietary Diversity Scores in Children: Are they Good Indicators of Dietary Adequacy? Public Health Nutr. 2006, 9, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labadarios, D.; Steyn, N.P.; Nel, J. How diverse is the diet of adult South Africans? Nutr. J. 2011, 10, 33. [Google Scholar] [CrossRef]
- Ogunlade, A.O.; Kruger, H.S.; Jerling, J.C.; Smuts, C.M.; Covic, N.; Hanekom, S.M.; Mamabolo, R.L.; Kvalsvig, J. Point-of-use micronutrient fortification: Lessons learned in implementing a preschool-based pilot trial in South Africa. Int. J. Food Sci. Nutr. 2011, 62, 1–16. [Google Scholar] [CrossRef]
- Mushaphi, L.; Dannhauser, A.; Walsh, C.; Mbhenyane, X.G.; Rooyen, F. Effect of a nutrition education programme on nutritional status of children aged 3–5 years in Limpopo Province, South Africa. S. Afr. J. Child Health 2015, 9, 98. [Google Scholar] [CrossRef] [Green Version]
- Seonandan, P.; McKerrow, N. A review of infant and young child feeding practice in hospital and the home in KwaZulu-Natal Midlands. S. Afr. J. Clin. Nutr. 2016, 29, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Chelule, P.K.; Mokgatle, M.M.; Zungu, L.I.; Chaponda, A. Caregivers’ knowledge and use of fermented foods for infant and young children feeding in a rural community of odi, Gauteng province, South Africa. Health Promot. Perspect. 2014, 4, 54. [Google Scholar] [PubMed] [Green Version]
- Lesiapeto, M.S. Factors Associated with Nutritional Status of Children Aged 0–60 Months Residing in Eastern Cape and KwaZulu-Natal Provinces; North-West University: Potchefstroom, South Africa, 2009. [Google Scholar]
- Mamabolo, R.L.; Alberts, M.; Steyn, N.P.; Delemarre-van de Waal, H.A.; Levitt, N.S. Prevalence and determinants of stunting and overweight in 3-year-old black South African children residing in the Central Region of Limpopo Province, South Africa. Public Health Nutr. 2005, 8, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ertem, G.; Ergun, S. Traditional practices and beliefs regarding nutrition of children in the 0–5 age group in western Turkey: A qualitative study. J. Pak. Med. Assoc. 2013, 63, 173–178. [Google Scholar]
- Modjadji, P.; Madiba, S. Childhood Undernutrition and Its Predictors in a Rural Health and Demographic Surveillance System Site in South Africa. Int. J. Environ. Res. Public Health 2019, 16, 3021. [Google Scholar] [CrossRef] [Green Version]
- Modjadji, P.; Madiba, S. The double burden of malnutrition in a rural health and demographic surveillance system site in South Africa: A study of primary schoolchildren and their mothers. BMC Public Health 2019, 19, 1087. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Strategy for Improved Nutrition of Children and Woman in Developing Counties; UNICEF: New York, NY, USA, 1990. [Google Scholar]
- FAO. Guidelines for Measuring Household and Individual Dietary Diversity. In FAO Nutrition and Consumer Protection Division, with Support from the EC/FAO Food Security Information for Action Programme and the Food and Nutrition Technical Assistance (FANTA) Project; FAO: Rome, Italy, 2007. [Google Scholar]
- FANTA. Nutrition Assessment and cCassification. Nutritional Assessment, Counseling and Support (NACS): A user’s guide. In Food and Nutrition Technical Assistance III Project; Module 2; FANTA: Washington, DC, USA, 2013. [Google Scholar]
- WHO. WHO Global Database on Child Growth and Malnutrition. In Department of Nutrition for Health and Development (NHD); WHO: Geneva, Switzerland, 1997; Available online: http://www.who.int/nutgrowthdb/en/ (accessed on 24 February 2020).
- Sealey-Potts, C.; Potts, A. An Assessment of Dietary Diversity and Nutritional Status of Preschool Children. Austin J. Nutr. Food Sci. 2014, 2, 1040. [Google Scholar]
- Sirasa, F.; Mitchell, L.; Harris, N. Dietary diversity and food intake of urban preschool children in North-Western Sri Lanka. Matern. Child Nutr. 2020, 16, e13006. [Google Scholar] [CrossRef]
- Kennedy, G.L.; Pedro, M.R.; Seghieri, C.; Nantel, G.; Brouwer, I. Dietary diversity score is a useful indicator of micronutrient intake in non-breast-feeding Filipino children. J. Nutr. 2007, 137, 472–477. [Google Scholar] [CrossRef] [Green Version]
- Bandoh, D.A.; Kenu, E. Dietary diversity and nutritional adequacy of under-fives in a fishing community in the central region of Ghana. BMC Nutr. 2017, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Ogechi, U.P.; Chilezie, O.V. Assessment of Dietary Diversity Score, Nutritional Status and Socio-demographic Characteristics of Under-5 Children in Some Rural Areas of Imo State, Nigeria. Malays. J. Nutr. 2017, 23, 425–435. [Google Scholar]
- Bi, J.; Liu, C.; Li, S.; He, Z.; Chen, K.; Luo, R.; Wang, Z.; Yu, Y.; Xu, H. Dietary diversity among preschoolers: A cross-sectional study in poor, rural, and ethnic minority areas of central south china. Nutrients 2019, 11, 558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acham, H.; Oldewage-Theron, W.H.; Egal, A.A. Dietary diversity, micronutrient intake and their variation among black women in informal settlements in South Africa: A cross-sectional study. Int. J. Nutr. Metab. 2012, 4, 24–39. [Google Scholar]
- Drimie, S.; Faber, M.; Vearey, J.; Nunez, L. Dietary diversity of formal and informal residents in Johannesburg, South Africa. BMC Public Health 2013, 13, 911. [Google Scholar] [CrossRef]
- Faber, M.; Schwabe, C.; Drimie, S. Dietary diversity in relation to other household food security indicators. Int. J. Food Saf. Nutr. Public Health 2009, 2, 1–15. [Google Scholar] [CrossRef]
- Labadarios, D.; Mchiza, Z.J.-R.; Steyn, N.P.; Gericke, G.; Maunder, E.M.W.; Davids, Y.D.; Parker, W.-A. Food security in South Africa: A review of national surveys. Bull. World Health Organ. 2011, 89, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Alamu, E.O.; Gondwe, T.; Eyinla, T.E.; Maziya-Dixon, B. Assessment of dietary diversity of mothers and children of 6–24 months from eastern and southern provinces of Zambia. J. Nutr. Metab. 2019, 2019, 1049820. [Google Scholar] [CrossRef]
- Rakotonirainy, N.H.; Razafindratovo, V.; Remonja, C.R.; Rasoloarijaona, R.; Piola, P.; Raharintsoa, C.; Randremanana, R.V. Dietary diversity of 6-to 59-month-old children in rural areas of Moramanga and Morondava districts, Madagascar. PLoS ONE 2018, 13, e0200235. [Google Scholar] [CrossRef] [Green Version]
- Moursi, M.M.; Arimond, M.; Dewey, K.G.; Treche, S.; Ruel, M.T.; Delpeuch, F. Dietary diversity is a good predictor of the micronutrient density of the diet of 6-to 23-month-old children in Madagascar. J. Nutr. 2008, 138, 2448–2453. [Google Scholar] [CrossRef]
- Akerele, D.; Sanusi, R.; Fadare, O.; Ashaolu, O. Factors influencing nutritional adequacy among rural households in Nigeria: How does dietary diversity stand among influencers? Ecol. Food Nutr. 2017, 56, 187–203. [Google Scholar] [CrossRef]
- Ekesa, B.; Blomme, G.; Garming, H. Dietary diversity and nutritional status of pre-school children from Musa-dependent households in Gitega (Burundi) and Butembo (Democratic Republic of Congo). Afr. J. Food Agric. Nutr. Dev. 2011, 11. [Google Scholar] [CrossRef] [Green Version]
- Powell, B.; Kerr, R.B.; Young, S.L.; Johns, T. The determinants of dietary diversity and nutrition: Ethnonutrition knowledge of local people in the East Usambara Mountains, Tanzania. J. Ethnobiol. Ethnomed. 2017, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manyike, P.C.; Chinawa, J.M.; Ubesie, A.; Obu, H.A.; Odetunde, O.I.; Chinawa, A.T. Prevalence of malnutrition among pre-school children in, South-east Nigeria. Ital. J. Pediatrics 2014, 40, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawarazuka, N. The contribution of fish intake, aquaculture, and small-scale fisheries to improving nutrition security: A literature review. WorldFish Center Working Paper 2010, 2106, 51. [Google Scholar]
- Frempong, R.B.; Annim, S.K. Dietary diversity and child malnutrition in Ghana. Heliyon 2017, 3, e00298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebremichael, D.Y.; Hadush, K.T.; Kebede, E.M.; Zegeye, R.T. Food Insecurity, Nutritional Status, and Factors Associated with Malnutrition among People Living with HIV/AIDS Attending Antiretroviral Therapy at Public Health Facilities in West Shewa Zone, Central Ethiopia. Biomed. Res. Int. 2018, 2018, 1913534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, D.; Saha, K.K.; Nguyen, P.H.; Diressie, M.T.; Ruel, M.T.; Menon, P.; Rawat, R. Household food insecurity is associated with higher child undernutrition in Bangladesh, Ethiopia, and Vietnam, but the effect is not mediated by child dietary diversity. J. Nutr. 2013, 143, 2015–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motbainor, A.; Worku, A.; Kumie, A. Stunting is associated with food diversity while wasting with food insecurity among underfive children in East and West Gojjam Zones of Amhara Region, Ethiopia. PLoS ONE 2015, 10, e0133542. [Google Scholar] [CrossRef]
- De Onis, M.; Branca, F. Childhood stunting: A global perspective. Matern. Child Nutr. 2016, 12, 12–26. [Google Scholar] [CrossRef]
- Abdurahman, A.A.; Mirzaei, K.; Dorosty, A.R.; Rahimiforoushani, A.; Kedir, H. Household food insecurity may predict underweightand wasting among children aged 24–59 months. Ecol. Food Nutr. 2016, 55, 456–472. [Google Scholar] [CrossRef]
- Batis, C.; Aburto, T.C.; Sánchez-Pimienta, T.G.; Pedraza, L.S.; Rivera, J.A. Adherence to dietary recommendations for food group intakes is low in the Mexican population. J. Nutr. 2016, 146, 1897S–1906S. [Google Scholar] [CrossRef] [Green Version]
- Campbell, R.K.; Hurley, K.M.; Shamim, A.A.; Shaikh, S.; Chowdhury, Z.T.; Mehra, S.; De Pee, S.; Ahmed, T.; West, K.P., Jr.; Christian, P. Effect of complementary food supplementation on breastfeeding and home diet in rural Bangladeshi children. Am. J. Clin. Nutr. 2016, 104, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Negash, C.; Whiting, S.J.; Henry, C.J.; Belachew, T.; Hailemariam, T.G. Association between maternal and child nutritional status in Hula, rural Southern Ethiopia: A cross sectional study. PLoS ONE 2015, 10, e0142301. [Google Scholar] [CrossRef] [PubMed]
- Abdi, M.; Nibret, E.; Munshea, A. Prevalence of intestinal helminthic infections and malnutrition among schoolchildren of the Zegie Peninsula, northwestern Ethiopia. J. Infect. Public Health 2017, 10, 84–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphries, D.L.; Dearden, K.A.; Crookston, B.T.; Woldehanna, T.; Penny, M.E.; Behrman, J.R. Household food group expenditure patterns are associated with child anthropometry at ages 5, 8 and 12 years in Ethiopia, India, Peru and Vietnam. Econ. Hum. Biol. 2017, 26, 30–41. [Google Scholar] [CrossRef]
- Bliss, J.R.; Njenga, M.; Stoltzfus, R.J.; Pelletier, D.L. Stigma as a barrier to treatment for child acute malnutrition in M arsabit C ounty, K enya. Matern. Child Nutr. 2016, 12, 125–138. [Google Scholar] [CrossRef]
- Nair, M.K.; Augustine, L.F.; Konapur, A. Food-Based Interventions to Modify Diet Quality and Diversity to Address Multiple Micronutrient Deficiency. Front. Public Health 2016, 3, 277. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |


{kind=link}
| Variables | Category | Frequency | Percentage |
|---|---|---|---|
| Child sex | Girls | 181 | 48 |
| Boys | 198 | 52 | |
| Birth order | First | 154 | 41 |
| Middle | 52 | 14 | |
| Last | 173 | 46 | |
| Full-term baby | Yes | 333 | 88 |
| No | 46 | 12 | |
| Child breast-fed | Yes | 326 | 86 |
| No | 53 | 14 | |
| Length of breast-feeding | Less than 6 months | 106 | 28 |
| Between 6 and 12 months | 75 | 20 | |
| Above 12 months | 144 | 38 | |
| Mixed feeding | Yes | 151 | 40 |
| No | 228 | 60 | |
| Introduction of solid food | Less than 6 months | 188 | 50 |
| Between 6 and 12 months | 169 | 45 | |
| Immediately at 1 year | 22 | 6 | |
| Mothers’ age (years) | <25 | 93 | 25 |
| 26–34 | 168 | 44 | |
| ≥35 | 118 | 31 | |
| Employment status | Employed | 108 | 28 |
| Unemployed | 271 | 72 | |
| Marital status | Single | 303 | 80 |
| Married | 76 | 20 | |
| Household monthly income | <USD 296.37 | 267 | 70 |
| ≥USD 296.37 | 112 | 30 | |
| Receiving social grant | Yes | 326 | 86 |
| No | 53 | 14 | |
| Level of education | High literacy | 350 | 92 |
| Low literacy | 29 | 8 | |
| Number of household members | 1 to 4 | 281 | 74 |
| ≥5 | 98 | 26 | |
| Housing | Brick house | 135 | 36 |
| Non-brick | 244 | 64 | |
| Access to electricity | Yes | 338 | 89 |
| No | 41 | 11 | |
| Access to water | Yes | 292 | 77 |
| No | 87 | 23 | |
| Type of toilet | Flush toilet | 333 | 88 |
| Pit toilet | 46 | 12 |
| Nutritional Status Indicators | All n = 379 | Boys n = 198 | Girls n = 181 | p-Value |
|---|---|---|---|---|
| Weight (kg) | 15.2 ± 2.50 | 15.3±2.60 | 15.1±2.39 | 0.342 |
| Height (cm) | 98.3 ± 7.04 | 97.9±7.04 | 98.9±7.02 | 0.157 |
| HAZ-mean | −1.29 (−2.14; −0.40) | −1.46 (−2.30; −0.53) | −1.10(1.93; −0.30) | 0.154 |
| Normal | 258 (68) | 127 (64) | 131 (71) | 0.016 |
| Stunting | 109 (29) | 66 (33) | 43 (24) | |
| Tallness | 12 (3) | 5 (3) | 7 (4) | |
| WAZ-mean | −0.72(−1.36; 0.06) | −0.73 (−1.34; 0.07) | −0.71 (−1.45; 0.01) | 0.864 |
| Normal | 311 (82) | 163 (83) | 148 (82) | 0.796 |
| Underweight | 49 (13) | 24 (12) | 25 (14) | |
| Growth problem | 19 (5) | 11 (6) | 8 (4) | |
| BAZ-mean | 0.16 (−0.59; 1.07) | −0.34 (−0.44; 1.44) | −0.37 (−0.84; 0.78) | 0.002 * |
| Normal | 259 (68) | 125(63) | 134 (74) | 0.057 |
| Thinness | 22 (6) | 11 (6) | 11 (6) | |
| Overweight risk | 70 (19) | 42 (21) | 28 (15) | |
| Overweight/obesity | 28 (7) | 20 (10) | 8 (4) |
| Variables | Sex | |||
|---|---|---|---|---|
| All | Boys | Girls | p-Value | |
| DDS mean | 4.39 ± 1.55 | 4.4 ± 1.4 | 4.4 ± 1.7 | 0.775 |
| Low DDS | 230 (61) | 121 (61) | 109 (60) | 0.859 |
| Medium DDS | 149 (39) | 77 (39) | 72 (40) | |
| Age Group | ||||
| Variables | 3 Years | 4 Years | 5 Years | p-Value |
| DDS mean | 4.6 ± 1.5 | 4.4 ± 1.6 | 4.2 ± 1.5 | 0.533 |
| Low DDS | 36 (58) | 121 (60) | 73 (63) | 0.738 |
| Medium DDS | 26 (42) | 81 (40) | 42 (37) | |
| Variable | Univariate a | Multivariate b | ||
|---|---|---|---|---|
| All | OR (95% CI) | p Value | AOR (95% CI) | p Value |
| HAZ | −0.05 (−0.18 to 0.07) | 0.401 | −1.35 (−2.88 to 0.17) | 0.081 |
| WAZ | −0.12 (−0.26 to 0.02) | 0.087 | 1.93 (−0.35 to 4.22) | 0.097 |
| BAZ | −0.08 (−019 to 0.0.3) | 0.146 | −1.37 (−2.87 to 0.14) | 0.076 |
| Stunting c | 1.01 (0.64 to 1.60) | 0.960 | 0.61 (0.28 to 1.21) | 0.176 |
| Underweight d | 1.54 (0.85 to 2.84) | 0.156 | 1.95 (0.88 to 5.06) | 0.131 |
| Thinness e | 1.82 (0.78 to 4.36) | 0.181 | 1.15 (0.38 to 3.40) | 0.803 |
| Variable | Univariate a | Multivariate b | ||
|---|---|---|---|---|
| 3-Year-Olds | OR (95% CI) | p Value | AOR (95% CI) | p Value |
| HAZ | 0.17 (−0.14 to 0.48) | 0.284 | −1.57 (−8.45 to 5.31) | 0.650 |
| WAZ | −0.06 (−0.37 to 0.25) | 0.692 | 2.52 (−7.58 to 12.62) | 0.620 |
| BAZ | −0.16 (−0.40 to 0.08) | 0.183 | −1.83 (−8.57 to 4.92) | 0.590 |
| Stunting c | 1.38 (0.48 to 4.08) | 0.565 | 1.05 (0.22 to 5.10) | 0.948 |
| Underweight d | 3.01 (0.77 to 11.72) | 0.112 | 2.19 (0.34 to 14.37) | 0.411 |
| Thinness e | 2.80 (0.45 to 17.32) | 0.268 | 1.69 (0.17 to 16.42) | 0.649 |
| 4-Year-Olds | OR (95% CI) | p Value | AOR (95% CI) | p Value |
| HAZ | −0.03 (−0.20 to 0.13) | 0.706 | −1.47 (−3.61 to 0.66) | 0.175 |
| WAZ | −0.05 (−0.24 to 0.15) | 0.646 | 2.15 (−1.04 to 5.35) | 0.186 |
| BAZ | −0.02 (−0.19 −0.4) | 0.765 | −1.47 (−3.60–0.67) | 0.171 |
| Stunting | 0.69 (0.37 to 1.28) | 0.238 | 0.25 (0.10 to 0.92) | 0.035 * |
| Underweight | 0.98 (0.41–2.30) | 0.954 | 2.38 (0.65 to 8.72) | 0.190 |
| Thinness | 0.96 (0.26 to 3.55) | 0.948 | 0.60 (0.12 to 3.02) | 0.536 |
| 5-Year-Olds | OR (95% CI) | p Value | AOR (95% CI) | p Value |
| HAZ | −0.23 (−0.46 to 0.02) | 0.077 | −1.12 (−3.81 to 1.53) | 0.398 |
| WAZ | −0.32 (−0.57 to −0.07) | 0.013 * | 1.38 (−2.70 to 5.46) | 0.505 |
| BAZ | −0.17 (−0.37 to 0.04) | 0.110 | −1.08 (−3.73 to 1.57) | 0.420 |
| Stunting | 1.83 (0.76 to 4.39) | 0.179 | 1.38 (0.44 to 4.36) | 0.585 |
| Underweight | 2.04 (0.64 to 6.54) | 0.230 | 1.27 (0.26 to 6.24) | 0.771 |
| Thinness | 3.20 (0.56 to 18.40) | 0.192 | 2.00 (0.23 to 17.56) | 0.530 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modjadji, P.; Molokwane, D.; Ukegbu, P.O. Dietary Diversity and Nutritional Status of Preschool Children in North West Province, South Africa: A Cross Sectional Study. Children 2020, 7, 174. https://0-doi-org.brum.beds.ac.uk/10.3390/children7100174
Modjadji P, Molokwane D, Ukegbu PO. Dietary Diversity and Nutritional Status of Preschool Children in North West Province, South Africa: A Cross Sectional Study. Children. 2020; 7(10):174. https://0-doi-org.brum.beds.ac.uk/10.3390/children7100174
Chicago/Turabian StyleModjadji, Perpetua, Dineo Molokwane, and Patricia Ogechi Ukegbu. 2020. "Dietary Diversity and Nutritional Status of Preschool Children in North West Province, South Africa: A Cross Sectional Study" Children 7, no. 10: 174. https://0-doi-org.brum.beds.ac.uk/10.3390/children7100174