Child Pain Intensity and Parental Attitudes toward Complementary and Alternative Medicine Predict Post-Tonsillectomy Analgesic Use

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Parental CAM Attitudes
2.3. Child Pain Intensity
2.4. Clinical Outcomes
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Post-Tonsillectomy Home Analgesic Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cullen, K.A.; Hall, M.J.; Golosinskiy, A. Ambulatory Surgery in the United States, 2006; National Health Statistics; National Center for Health Statistics: Hyattsville, MD, USA, 2009.
- Short, H.L.; Sarda, S.; Travers, C.; Hockenberry, J.M.; McCarthy, I.; Raval, M.V. Trends in common surgical procedures at children’s and nonchildren’s hospitals between 2000 and 2009. J. Pediatr. Surg. 2018, 53, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Erickson, B.K.; Larson, D.R.; St Sauver, J.L.; Meverden, R.A.; Orvidas, L.J. Changes in incidence and indications of tonsillectomy and adenotonsillectomy, 1970–2005. Otolaryngol. Head Neck Surg. 2009, 140, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Fortier, M.A.; MacLaren, J.E.; Martin, S.R.; Perret-Karimi, D.; Kain, Z.N. Pediatric pain after ambulatory surgery: Where’s the medication? Pediatrics 2009, 124, e588–e595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baugh, R.F.; Archer, S.M.; Mitchell, R.B.; Rosenfeld, R.M.; Amin, R.; Burns, J.J.; Darrow, D.H.; Giordano, T.; Litman, R.S.; Li, K.K.; et al. Clinical practice guideline: Tonsillectomy in children. Otolaryngol. Neck Surg. 2011, 144, S1–S30. [Google Scholar] [CrossRef] [Green Version]
- Brigger, M.T.; Brietzke, S.E. Outpatient tonsillectomy in children: A systematic review. Otolaryngol. Neck Surg. 2006, 135, 1–7. [Google Scholar] [CrossRef]
- Swallow, J.; Briggs, M.; Semple, P. Pain at home: Children’s experience of tonsillectomy. J. Child Health Care 2000, 4, 93–98. [Google Scholar] [CrossRef]
- Walker, S.M. Pain after surgery in children: Clinical recommendations. Curr. Opin. Anaesthesiol. 2015, 28, 570–576. [Google Scholar] [CrossRef] [Green Version]
- Benyamin, R.; Trescot, A.; Datta, S.; Buenaventura, R.; Adlaka, R.; Sehgal, N.; Glaser, S.E.; Vallejo, R. Opioid complications and side effects. Pain Physician 2008, 11, S105–S120. [Google Scholar]
- Chua, K.-P.; Shrime, M.G.; Conti, R.M. Effect of FDA investigation on opioid prescribing to children after tonsillectomy/adenoidectomy. Pediatrics 2017, 140, e20171765. [Google Scholar] [CrossRef] [Green Version]
- Evans, S.; Tsao, J.C.I.; Zeltzer, L.K. Paediatric pain management: Using complementary and alternative medicine. Rev. Pain 2008, 2, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Chambers, C.T.; Reid, G.J.; McGrath, P.J.; Finley, G.A.; Ellerton, M. A randomized trial of a pain education booklet: Effects on parents’ attitudes and postoperative pain management. Children’s Health Care. 1997, 26, 1–13. [Google Scholar] [CrossRef]
- MacLaren Chorney, J.; Twycross, A.; Mifflin, K.; Archibald, K. Can we improve parents' management of their children’s postoperative pain at home? Pain. Res. Manag. 2014, 19, e115–e123. [Google Scholar] [CrossRef] [Green Version]
- Rony, R.Y.Z.; Fortier, M.A.; Chorney, J.M.; Perret, D.; Kain, Z.N. Parental postoperative pain management: Attitudes, assessment, and management. Pediatrics 2010, 125, e1372–e1378. [Google Scholar] [CrossRef] [PubMed]
- Rosales, A.; Fortier, M.A.; Campos, B.; Kain, Z.N. Postoperative pain management in Latino families: Parent beliefs about analgesics predict analgesic doses provided to children. Pediatr. Anesth. 2016, 26, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorodzinsky, A.Y.; Bernacki, J.M.; Davies, W.H.; Drendel, A.L.; Weisman, S.J. Community Parents’ Use of Non-Pharmacological Techniques for Childhood Pain Management. Children’s Health Care 2012, 41, 1–15. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Patterson, C.; Arthur, H. A complementary alternative medicine questionnaire for young adults. Integr. Med. Insights 2009, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Redmann, A.J.; Wang, Y.; Furstein, J.; Myer, C.M.; de Alarcón, A. The use of the FLACC pain scale in pediatric patients undergoing adenotonsillectomy. Int. J. Pediatr. Otorhinolaryngol. 2017, 92, 115–118. [Google Scholar] [CrossRef]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Linear Mixed-Effects Models Using “Eigen” and S4 (lme4). Available online: http://lme4.r-forge.r-project.org/ (accessed on 30 July 2020).
- Finley, A.G.; McGrath, P.J.; Forward, P.S.; McNeill, G.; Fitzgerald, P. Parents’ management of children’s pain following ‘minor’ surgery. Pain 1996, 64, 83–87. [Google Scholar] [CrossRef]
- Crandall, M.; Lammers, C.; Senders, C.; Braun, J.V.; Savedra, M. Children’s pre-operative tonsillectomy pain education: Clinical outcomes. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1523–1533. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.X.; Tunkel, D.E. Control of pain after tonsillectomy in children: A review. JAMA Otolaryngol. Neck Surg. 2017, 143, 937. [Google Scholar] [CrossRef] [PubMed]
- Hamunen, K.; Kontinen, V. Systematic review on analgesics given for pain following tonsillectomy in children. Pain 2005, 117, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Oremule, B.; Johnson, M.; Sanderson, L.; Lutz, J.; Dodd, J.; Hans, P. Oral morphine for pain management in paediatric patients after tonsillectomy and adenotonsillectomy. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 2166–2169. [Google Scholar] [CrossRef]
- Bellman, M.H.; Paley, C.E. Pain control in children. Parents underestimate children’s pain. BMJ 1993, 307, 1563. [Google Scholar] [CrossRef] [Green Version]
- Schechter, N.L.; Allen, D.A.; Hanson, K. Status of pediatric pain control: A comparison of hospital analgesic usage in children and adults. Pediatrics 1986, 77, 11–15. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | Pediatric Patients (n = 33) |
|---|---|
| Patient Demographics | |
| Age (years), mean (SD) | 8.5 (2.7) |
| Sex, n (%) | |
| Female | 16 (49%) |
| Male | 17 (51%) |
| BMI, mean (SD) | 18.8 (5.1) |
| Indication for surgery | |
| Obstructive sleep apnea | 16 (49%) |
| Adenotonsillar hypertrophy | 4 (12%) |
| Snoring/sleep-disordered breathing | 6 (18%) |
| Recurrent pharyngitis | 3 (9%) |
| Other | 4 (12%) |
| Post-Tonsillectomy | |
| Diary days completed, median (IQR) | 6 (4–7) |
| Acetaminophen total doses, median (IQR) | 14 (12–18) |
| Ibuprofen total doses, median (IQR) | 15 (11–18) |
| Oxycodone total doses, median (IQR) | 1 (0–2) |
| Variable | b | 95% CI | SE | z | p |
|---|---|---|---|---|---|
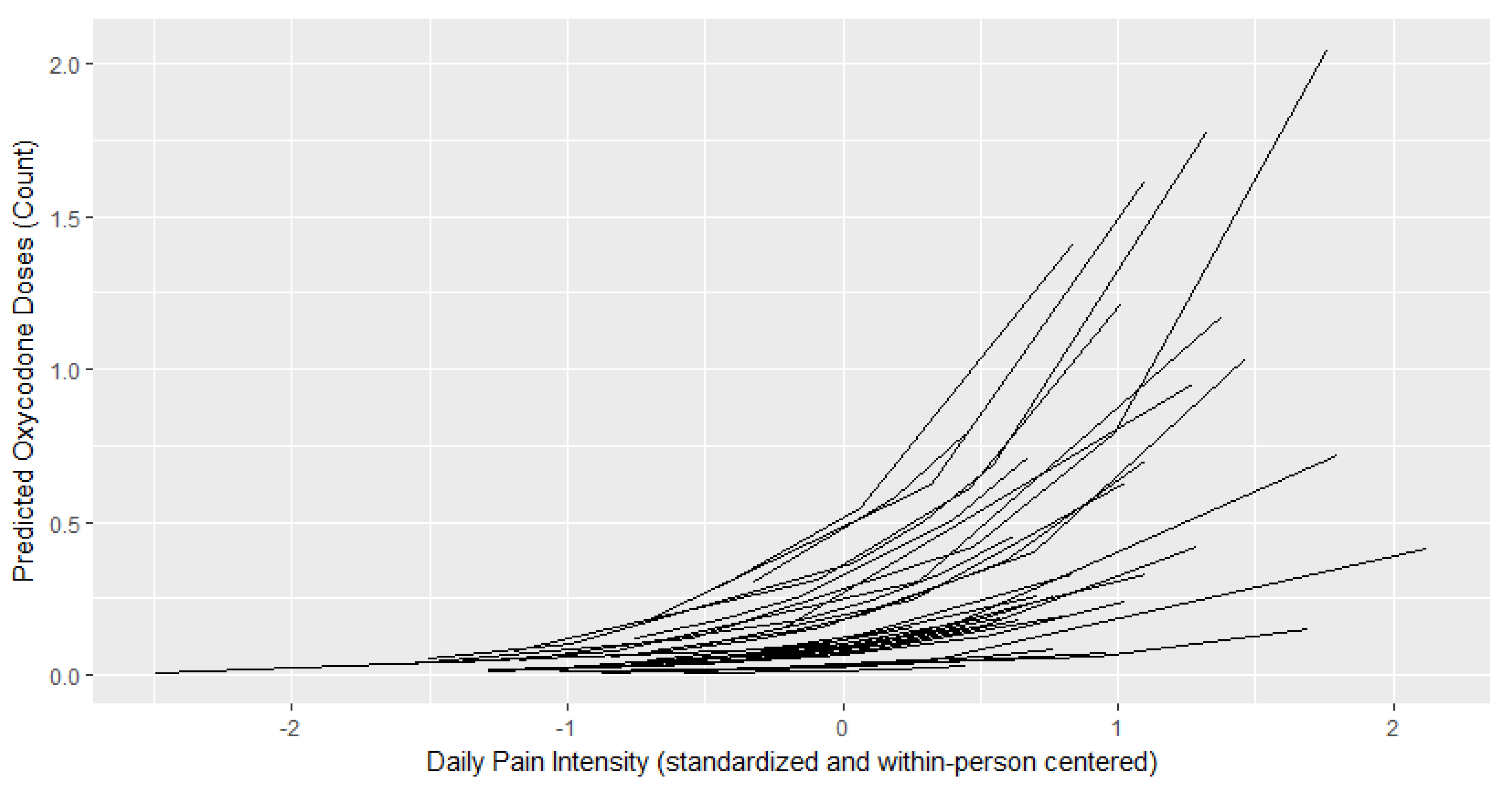
| Model 1—Number of Oxycodone Doses | |||||
| Intercept | 2.241 | −0.47–5.448 | 1.473 | 1.521 | 0.128 |
| Daily pain intensity | 1.23 | 0.790–1.696 | 0.230 | 5.348 | <0.001 |
| Average postoperative pain | 0.766 | 0.208–1.402 | 0.291 | 2.632 | 0.008 |
| CAM attitudes | −1.192 | −2.128–-0.406 | 0.419 | −2.848 | 0.004 |
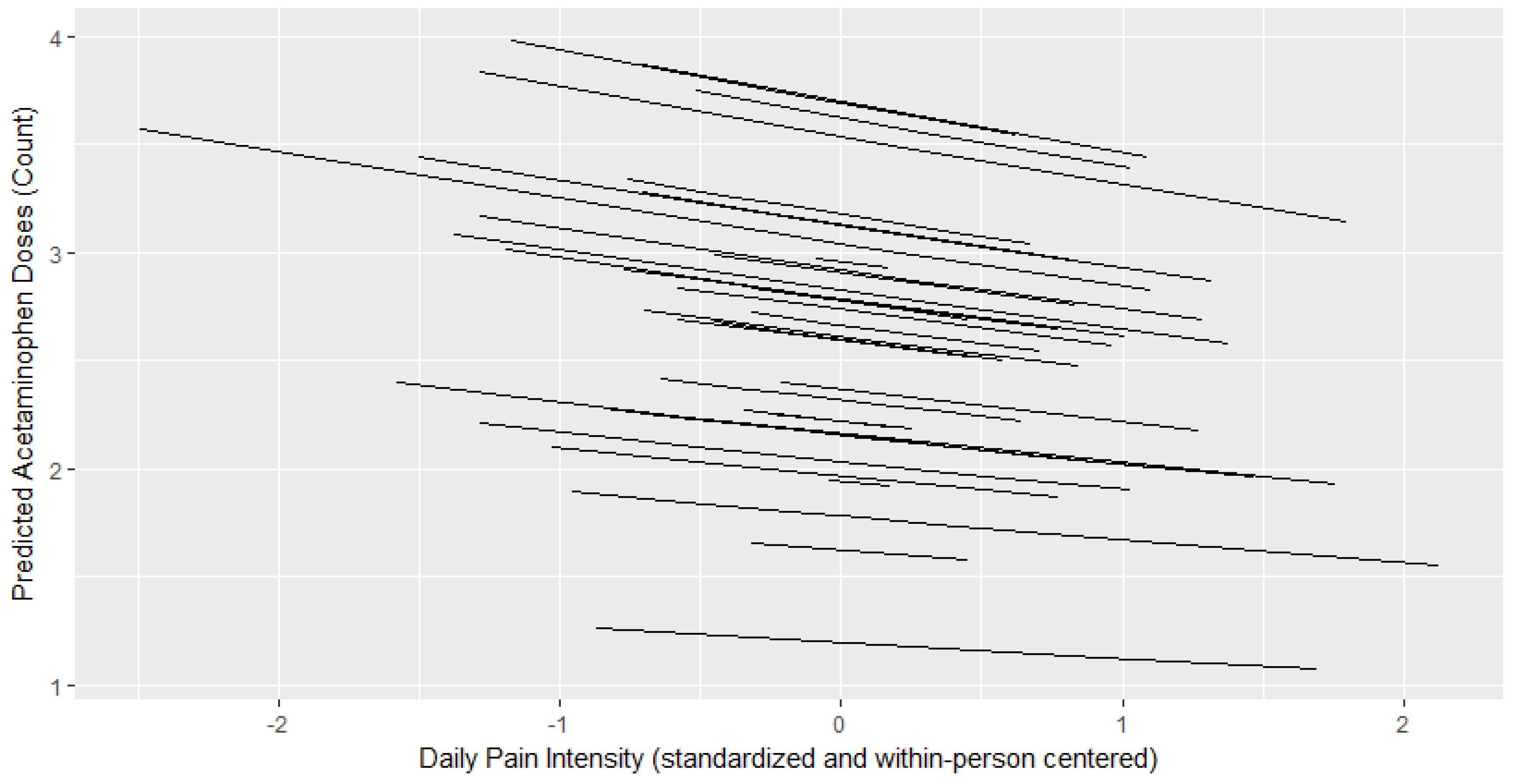
| Model 2—Number of Acetaminophen Doses | |||||
| Intercept | 1.163 | 0.212–2.111 | 0.464 | 2.504 | 0.012 |
| Daily pain intensity | −0.065 | −0.191–0.062 | 0.064 | −1.009 | 0.313 |
| Average postoperative pain | 0.184 | −0.007–0.382 | 0.0953 | 1.931 | 0.054 |
| CAM attitudes | −0.062 | −0.317–0.187 | 0.123 | −0.507 | 0.612 |
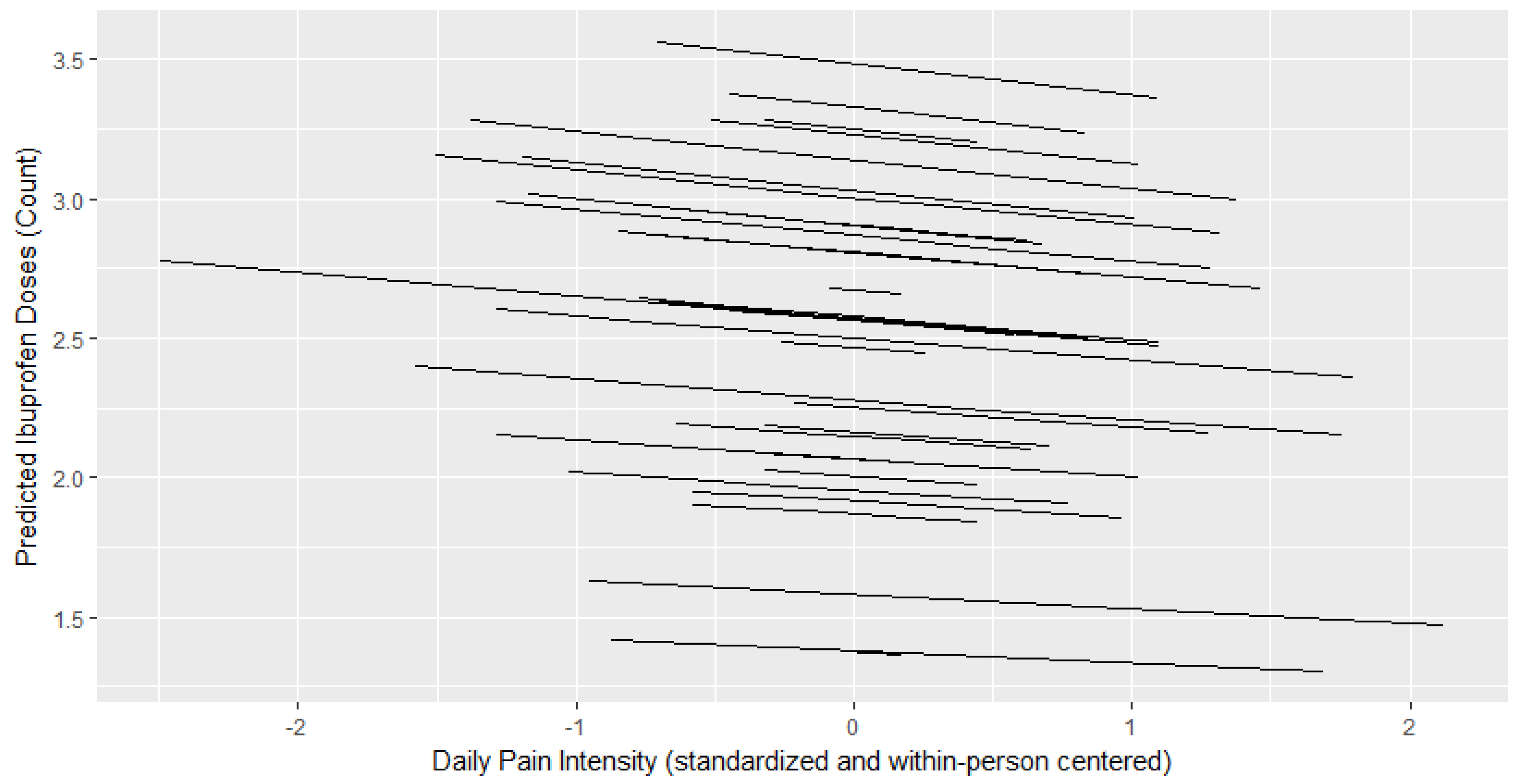
| Model 3—Number of Ibuprofen Doses | |||||
| Intercept | 1.631 | 0.826–2.455 | 0.395 | 4.151 | <0.001 |
| Daily pain intensity | −0.032 | −0.161–0.097 | 0.066 | −0.4932 | 0.623 |
| Average postoperative pain | 0.244 | 0.081–0417 | 0.082 | 3.000 | 0.003 |
| CAM attitudes | −0.197 | −0.421–0.015 | 0.106 | −1.861 | 0.063 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Delaney, K.; Napier, M.; Card, E.; Lipscomb, B.; Werkhaven, J.; Whigham, A.S.; Franklin, A.D.; Bruehl, S.; Stone, A.L. Child Pain Intensity and Parental Attitudes toward Complementary and Alternative Medicine Predict Post-Tonsillectomy Analgesic Use. Children 2020, 7, 236. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110236
Lee J, Delaney K, Napier M, Card E, Lipscomb B, Werkhaven J, Whigham AS, Franklin AD, Bruehl S, Stone AL. Child Pain Intensity and Parental Attitudes toward Complementary and Alternative Medicine Predict Post-Tonsillectomy Analgesic Use. Children. 2020; 7(11):236. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110236
Chicago/Turabian StyleLee, Jaclyn, Katherine Delaney, Molly Napier, Elizabeth Card, Brittany Lipscomb, Jay Werkhaven, Amy S. Whigham, Andrew D. Franklin, Stephen Bruehl, and Amanda L. Stone. 2020. "Child Pain Intensity and Parental Attitudes toward Complementary and Alternative Medicine Predict Post-Tonsillectomy Analgesic Use" Children 7, no. 11: 236. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110236