Restoration of an Upper Anterior Tooth in an Adolescent with Autism Spectrum Disorder—A Student Case Report

 , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction/Background
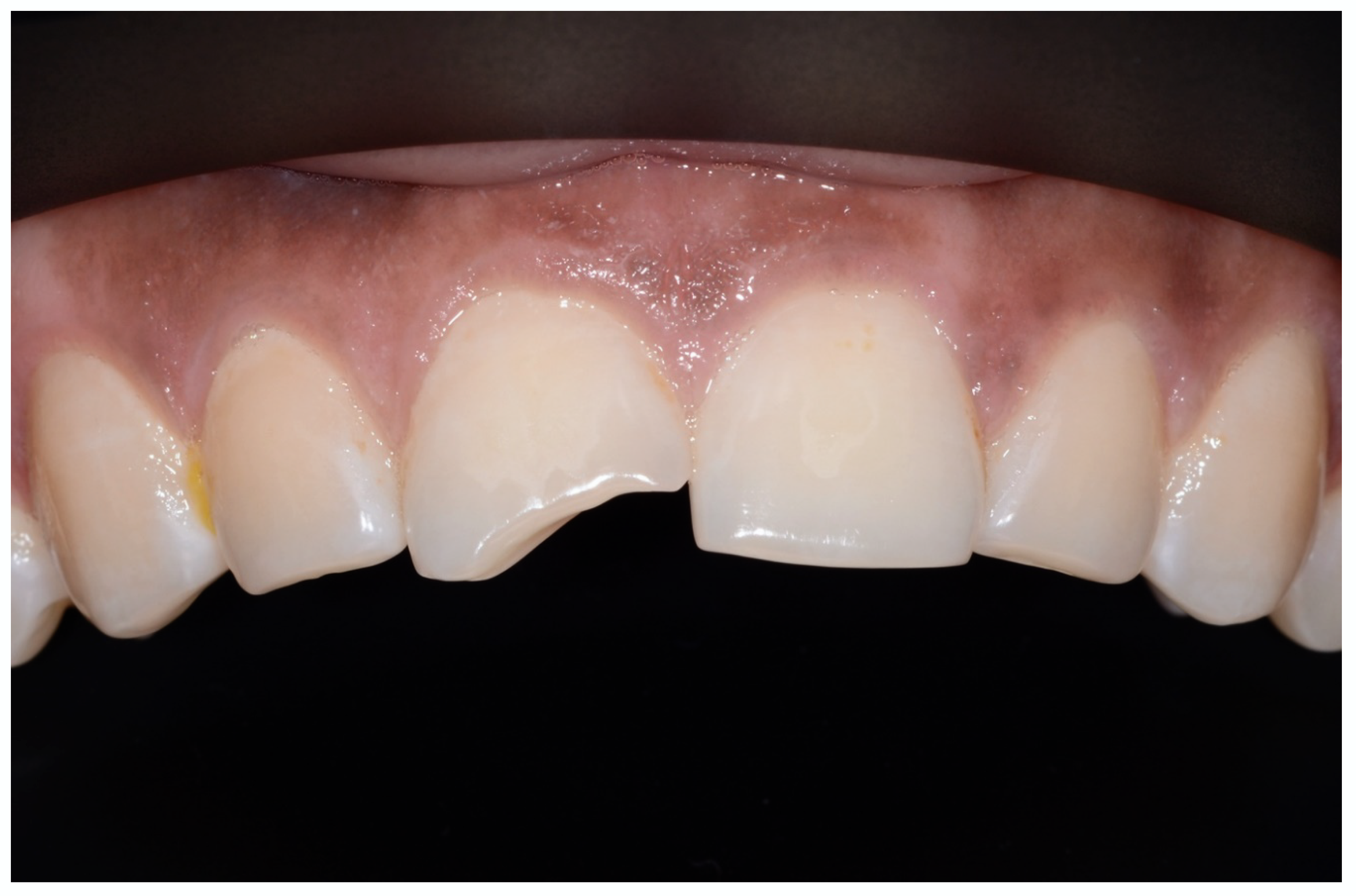
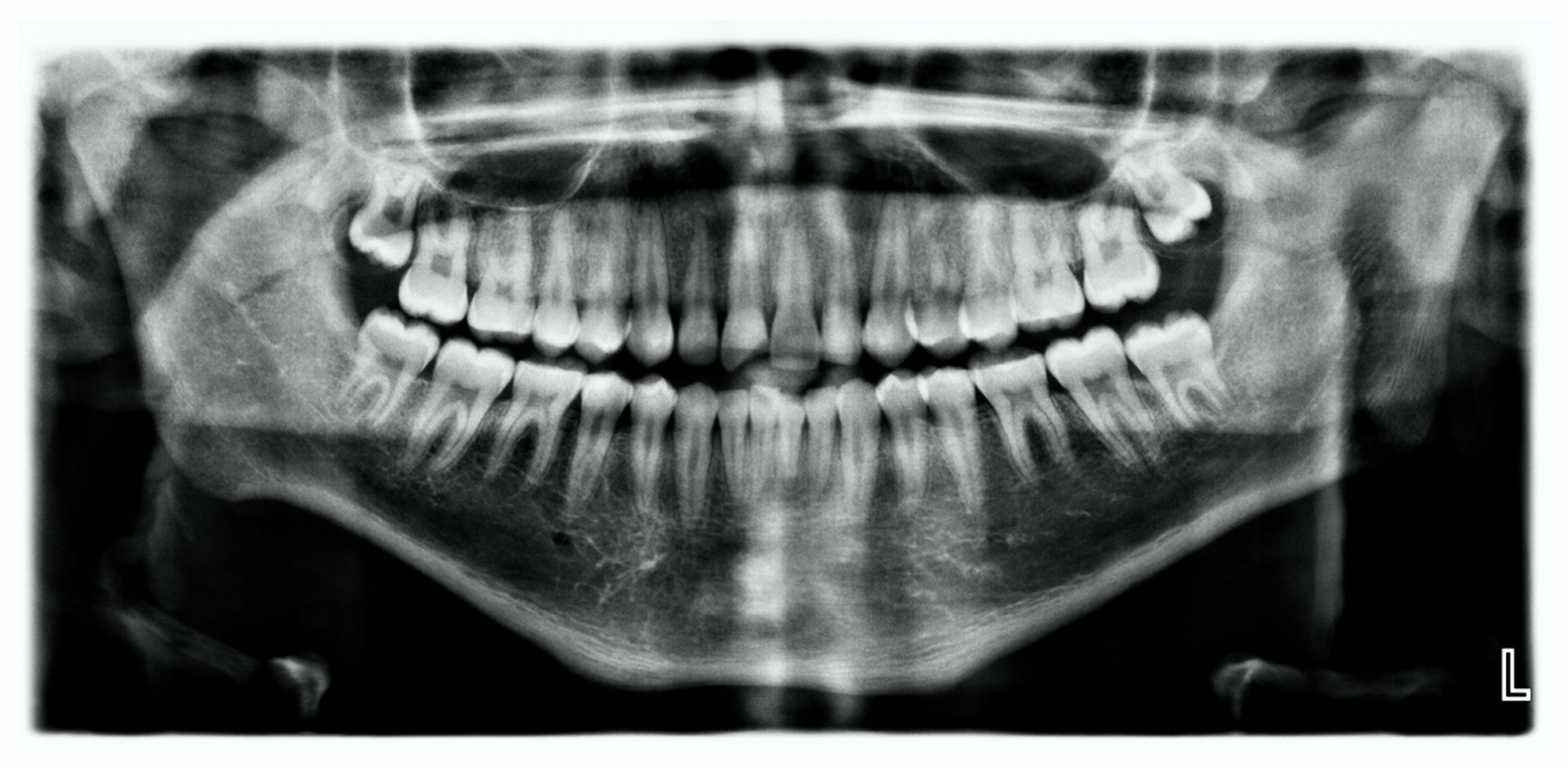
2. Case Presentation
2.1. Background/Treatment Plan
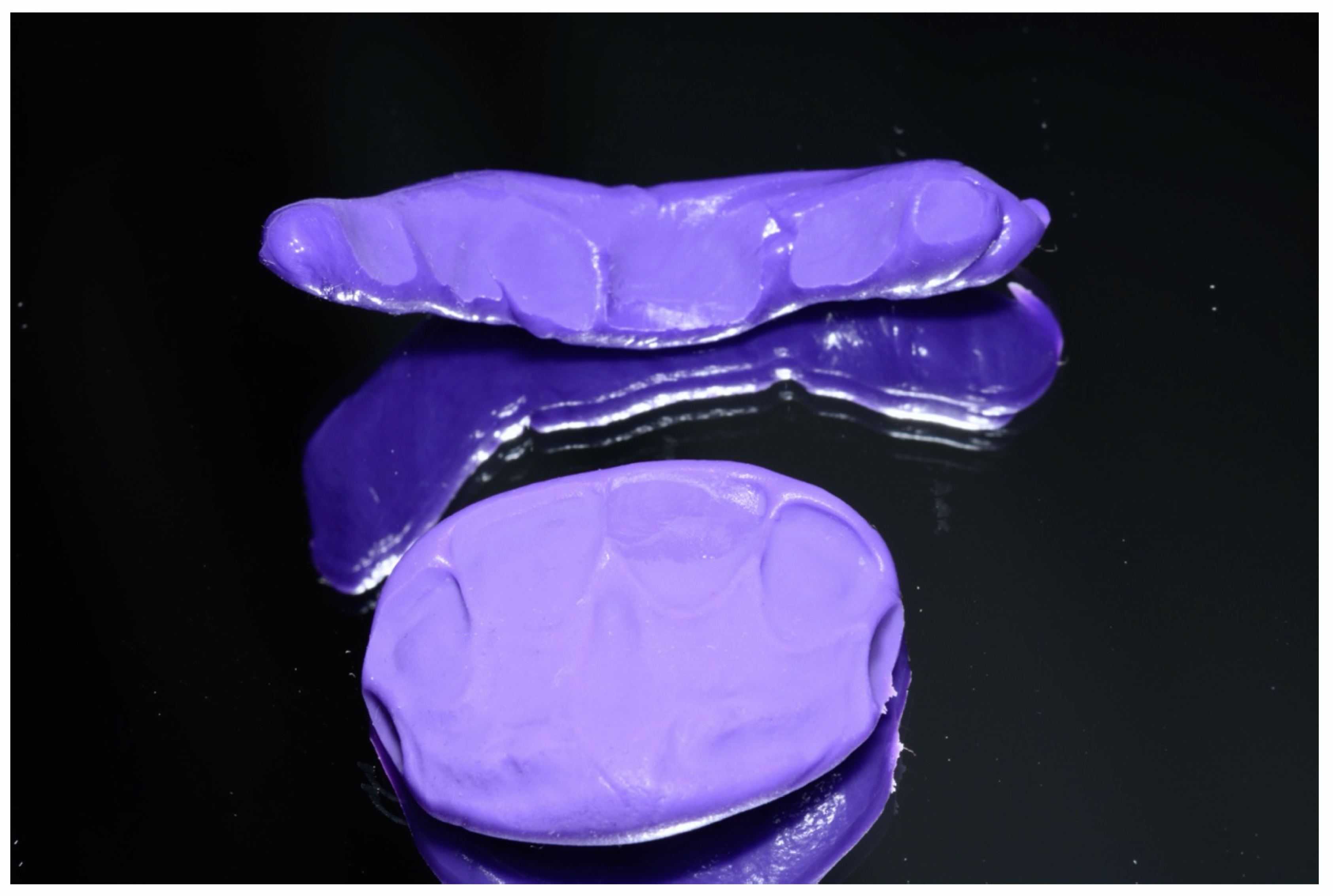
2.2. Therapy
2.3. Consent for Publication
3. Discussion
4. Conclusions
Practical Application
- Creation of a dental environment that meets the psychological and physical needs of people with (early childhood) autism.
- Inclusion of visual-haptic elements as part of the behavioral facilitation before and during dental treatment.
- Choice of a sufficiently long treatment period so that the patient can get used to the dental setting in several short preparatory sessions prior to invasive treatment.
- Adaptation of the duration of each treatment session to a length suitable for the patient, based on the patient’s age and the expected stress level of the upcoming preparation or treatment step.
Author Contributions
Funding
Conflicts of Interest
References
- Armstrong, D.; Matt, M. Autoextraction in an autistic dental patient: A case report. Spec. Care Dent. 1999, 19, 72–74. [Google Scholar] [CrossRef]
- Dick, J.; Clough, S. Learning disability and obesity: A case report of challenges and reasonable adjustments. Br. Dent. J. 2019, 227, 19–24. [Google Scholar] [CrossRef]
- Fetner, M.; Cascio, C.J.; Essick, G. Nonverbal patient with autism spectrum disorder and obstructive sleep apnea: Use of desensitization to acclimatize to a dental appliance. Pediatr. Dent. 2014, 36, 499–501. [Google Scholar]
- Johnson, C.D.; Matt, M.K.; Dennison, D.; Brown, R.S.; Koh, S. Preventing factitious gingival injury in an autistic patient. J. Am. Dent. Assoc. 1996, 127, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A.; Sugnani, S.; Kalra, N.; Tyagi, R. Dental Management of Autistic Child. J. Case Rep. 2012, 1–3. [Google Scholar] [CrossRef]
- Lu, Y.Y.; Wei, I.H.; Huang, C.C. Dental health—A challenging problem for a patient with autism spectrum disorder. Gen. Hosp. Psychiatry 2013, 35, 214.e1–214.e3. [Google Scholar] [CrossRef] [PubMed]
- Medina, A.C.; Sogbe, R.; Gómez-Rey, A.M.; Mata, M. Factitial oral lesions in an autistic paediatric patient. Int. J. Paediatr. Dent. 2003, 13, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Monroy, P.G.; da Fonseca, M.A. The Use of Botulinum Toxin-A in the Treatment of Severe Bruxism in a Patient with Autism: A Case Report. Spec. Care Dent. 2006, 26, 37–39. [Google Scholar] [CrossRef]
- Muthu, M.S.; Prathibha, K.M. Management of a child with autism and severe bruxism: A case report. J. Indian Soc. Pedod. Prev. Dent. 2008, 26, 82–84. [Google Scholar] [CrossRef]
- Perez, E.; Behar-Horenstein, L.S.; Guelmann, M. Crown-root Fracture Restoration on a Patient with Autism Spectrum Disorder. J. Contemp. Dent. Pract. 2016, 17, 769–773. [Google Scholar] [CrossRef]
- Ross-Russell, M.; Sloan, P. Autoextraction in a child with autistic spectrum disorder. Br. Dent. J. 2005, 198, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.C. Autoextraction of twelve permanent teeth in a child with autistic spectrum disorder. Int. J. Paediatr. Dent. 2016, 26, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Kanner, L. Autistic disturbances of affective contact. Nervous Child 1943, 2, 217–250. [Google Scholar]
- Newschaffer, C.J.; Croen, L.A.; Daniels, J.; Giarelli, E.; Grether, J.K.; Levy, S.E.; Mandell, D.S.; Miller, L.A.; Pinto-Martin, J.; Reaven, J.; et al. The epidemiology of autism spectrum disorders. Annu. Rev. Public Health 2007, 28, 235–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, L.I.; Polido, J.C.; Najera, S.O.; Cermak, S.A. Oral care experiences and challenges in children with autism spectrum disorders. Pediatr. Dent. 2012, 34, 387–391. [Google Scholar] [PubMed]
- Weil, T.N.; Inglehart, M.R. Three- to 21-year-old patients with autism spectrum disorders: Parents’ perceptions of severity of symptoms, oral health, and oral health-related behavior. Pediatr. Dent. 2012, 34, 473–479. [Google Scholar]
- Elmore, J.L.; Bruhn, A.M.; Bobzien, J.L. Interventions for the Reduction of Dental Anxiety and Corresponding Behavioral Deficits in Children with Autism Spectrum Disorder. J. Dent. Hyg. 2016, 90, 111–120. [Google Scholar]
- Lam, P.P.; Du, R.; Peng, S.; McGrath, C.P.; Yiu, C.K. Oral health status of children and adolescents with autism spectrum disorder: A systematic review of case-control studies and meta-analysis. Autism 2020, 1362361319877337. [Google Scholar] [CrossRef]
- Marshall, J.; Sheller, B.; Williams, B.J.; Mancl, L.; Cowan, C. Cooperation predictors for dental patients with autism. Pediatr. Dent. 2007, 29, 369–376. [Google Scholar]
- Muotri, A.R. Autism spectrum disorders: Challenges and perspectives. Dev. Neurobiol. 2018, 78, 431–433. [Google Scholar] [CrossRef]
- Klein, U.; Nowak, A.J. Autistic disorder: A review for the pediatric dentist. Pediatr. Dent. 1998, 20, 312–317. [Google Scholar] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; 10th revision; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; 11th revision; World Health Organization: Geneva, Switzerland, 2019; Available online: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/437815624 version 04/2019 (accessed on 30 March 2020).
- Nelson, T.; Chim, A.; Sheller, B.L.; McKinney, C.M.; Scott, J.M. Predicting successful dental examinations for children with autism spectrum disorder in the context of a dental desensitization program. J. Am. Dent. Assoc. 2017, 148, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Corridore, D.; Zumbo, G.; Corvino, I.; Guaragna, M.; Bossu, M.; Polimeni, A.; Vozza, I. Prevalence of oral disease and treatment types proposed to children affected by Autistic Spectrum Disorder in Pediatric Dentistry: A Systematic Review. Clin. Ter. 2020, 171, e275–e282. [Google Scholar] [CrossRef]
- Salhia, H.O.; Al-Nasser, L.A.; Taher, L.S.; Al-Khathaami, A.M.; El-Metwally, A.A. Systemic review of the epidemiology of autism in Arab Gulf countries. Neurosciences 2014, 19, 291–296. [Google Scholar]
- Fombonne, E. Epidemiological surveys of autism and other pervasive developmental disorders: An update. J. Autism Dev. Disord. 2003, 33, 365–382. [Google Scholar] [CrossRef] [PubMed]
- Altun, C.; Guven, G.; Yorbik, O.; Acikel, C. Dental injuries in autistic patients. Pediatr. Dent. 2010, 32, 343–346. [Google Scholar] [PubMed]
- Elsabbagh, M.; Divan, G.; Koh, Y.J.; Kim, Y.S.; Kauchali, S.; Marcin, C.; Montiel-Nava, C.; Patel, V.; Paula, C.S.; Wang, C.; et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012, 5, 160–179. [Google Scholar] [CrossRef] [Green Version]
- Hossain, M.D.; Ahmed, H.U.; Jalal Uddin, M.M.; Chowdhury, W.A.; Iqbal, M.S.; Kabir, R.I.; Chowdhury, I.A.; Aftab, A.; Datta, P.G.; Rabbani, G.; et al. Autism Spectrum disorders (ASD) in South Asia: A systematic review. BMC Psychiatry 2017, 17, 281. [Google Scholar] [CrossRef] [Green Version]
- Mugayar, L.R. Autismus-Spektrum-Störungen: Ein Fenster öffnen. Quintessenz 2015, 7, 795–801. [Google Scholar]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child. Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef]
- Fahl, N., Jr. Mastering Composite Artistry to Create Anterior Masterpieces—Part 2. J. Cosmet. Dent. 2011, 26, 42–55. [Google Scholar]
- Paolone, G. Direkte Kompositrestaurationen an den Frontzähnen: Herstellung der Symmetrie bei zentralen Schneidezähnen. Int. J. Esthet. Dent. 2014, 9, 14–27. [Google Scholar]
- Vanini, L. Conservative Composite Restorations that Mimic Nature. J. Cosmet. Dent. 2010, 26, 80–98. [Google Scholar]
- Kuhaneck, H.M.; Chisholm, E.C. Improving dental visits for individuals with autism spectrum disorders through an understanding of sensory processing. Spec. Care Dent. 2012, 32, 229–233. [Google Scholar] [CrossRef]
- Weil, T.N.; Inglehart, M.R. Dental education and dentists’ attitudes and behavior concerning patients with autism. J. Dent. Educ. 2010, 74, 1294–1307. [Google Scholar] [CrossRef]
- Weil, T.N.; Bagramian, R.A.; Inglehart, M.R. Treating patients with autism spectrum disorder—SCDA members’ attitudes and behavior. Spec. Care Dent. 2011, 31, 8–17. [Google Scholar] [CrossRef]
- Murshid, E.Z. Effectiveness of a preparatory aid in facilitating oral assessment in a group of Saudi children with autism spectrum disorders in Central Saudi Arabia. Saudi Med. J. 2017, 38, 533–540. [Google Scholar] [CrossRef]
- Kühnisch, J. Kinderzahnmedizin, 1st ed.; Quintessence Publishing: Berlin, Germany, 2020. [Google Scholar]
- Petrova, E.G.; Hyman, M.; Estrella, M.R.; Inglehart, M.R. Children with special health care needs: Exploring the relationships between patients’ level of functioning, their oral health, and caregivers’ oral health-related responses. Pediatr. Dent. 2014, 36, 233–239. [Google Scholar]
- Nogueira de Miranda, E.S.S.A.L.; Magno, M.B.; Rodrigues Campos Soares, T. The relationship between special needs and dental trauma. a systematic review and meta analysis. Dent. Traumatol. 2019. [Google Scholar] [CrossRef]
- da Silva, S.N.; Gimenez, T.; Souza, R.C.; Mello-Moura, A.C.V.; Raggio, D.P.; Morimoto, S.; Lara, J.S.; Soares, G.C.; Tedesco, T.K. Oral health status of children and young adults with autism spectrum disorders: Systematic review and meta-analysis. Int. J. Paediatr. Dent. 2017, 27, 388–398. [Google Scholar] [CrossRef]
- Diab, H.M.; Motlaq, S.S.; Alsharare, A.; Alshammery, A.; Alshammery, N.; Khawja, S.G.; Shah, A.H. Comparison of Gingival Health and Salivary Parameters among Autistic and Non-Autistic School Children in Riyadh. J. Clin. Diagn. Res. 2016, 10, ZC110–ZC113. [Google Scholar] [CrossRef] [PubMed]
- Jaber, M.A. Dental caries experience, oral health status and treatment needs of dental patients with autism. J. Appl. Oral Sci. 2011, 19, 212–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, R.Y.; Yiu, C.K.; King, N.M.; Wong, V.C.; McGrath, C.P. Oral health among preschool children with autism spectrum disorders: A case-control study. Autism 2015, 19, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Fahlvik-Planefeldt, C.; Herrstrom, P. Dental care of autistic children within the non-specialized Public Dental Service. Swed. Dent. J. 2001, 25, 113–118. [Google Scholar] [PubMed]
- Loo, C.Y.; Graham, R.M.; Hughes, C.V. The caries experience and behavior of dental patients with autism spectrum disorder. J. Am. Dent. Assoc. 2008, 139, 1518–1524. [Google Scholar] [CrossRef]
- Schmidt, P.; Schulte, A.G.; Fricke, O. Verhaltensbedingte dentale und orale Befunde bei Menschen mit Autismus-Spektrum-Störung—Eine ausgewählte Übersicht [Behavioral dental and oral findings in people with autism spectrum disorder—A selected overview]. Mon. Kinderheilkd. 2020, in press. [Google Scholar]
- Schmidt, P.; Petrakakis, P.; Schulte, A. Caries prevalence in 6- to 10-year-old German Schoolchildren with and without Disability. Community Dent. Health 2020. [Google Scholar] [CrossRef]
- Ward, L.M.; Cooper, S.A.; Hughes-McCormack, L.; Macpherson, L.; Kinnear, D. Oral health of adults with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2019, 63, 1359–1378. [Google Scholar] [CrossRef] [Green Version]
- Schulte, A.G.; Egermann, M.; Schmidt, P.; Ehlers, J. Self-evaluation of undergraduate dental students in regard to patients with disabilities. Dtsch. Zahnaerztl. Z. 2020, in press. [Google Scholar]
- United Nations General Assembly. Convention on the Rights of Persons with Disabilities; A/RES/61/106 Adopted on 13 December 2006, Entry into force: 3 May 2008; United Nations General Assembly: New York, NY, USA, 2008. [Google Scholar]
- Bundesgesetzblatt Teil 1, Nummer 4 vom 28.01.1955. Prüfungsordnung für Zahnärzte. Available online: http://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&jumpTo=bgbl155004.pdf (accessed on 17 April 2020).
- Heinrich-Weltzien, R.; Wagner, A.; Micheelis, W. Behandlung von Kindern mit Behinderungen. Befragung der Thüringer Zahnärzteschaft zu Fachwissen und subjektiver Belastung. Thüringer Zahnärzte Blatt 2013, 22, 18–20. [Google Scholar]
- Schulte, A.G.; Elsässer, G.; Bissar, A.; Heinrich-Weltzien, R. Professional knowledge of German dentists regarding treatment of patients with disabilities. J. Disabil. Oral Health 2012, 13, 1120, abstract. [Google Scholar]
- Dao, L.P.; Zwetchkenbaum, S.; Inglehart, M.R. General dentists and special needs patients: Does dental education matter? J. Dent. Educ. 2005, 69, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- McKinney, C.M.; Nelson, T.; Scott, J.M.; Heaton, L.J.; Vaughn, M.G.; Lewis, C.W. Predictors of unmet dental need in children with autism spectrum disorder: Results from a national sample. Acad. Pediatr. 2014, 14, 624–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rich, J.P., III; Straffon, L.; Inglehart, M.R. General dentists and pediatric dental patients: The role of dental education. J. Dent. Educ. 2006, 70, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Vainio, L.; Krause, M.; Inglehart, M.R. Patients with special needs: Dental students’ educational experiences, attitudes, and behavior. J. Dent. Educ. 2011, 75, 13–22. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diekamp, M.; Jenter, L.; Schulte, A.G.; Fricke, O.; Schmidt, P. Restoration of an Upper Anterior Tooth in an Adolescent with Autism Spectrum Disorder—A Student Case Report. Children 2020, 7, 237. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110237
Diekamp M, Jenter L, Schulte AG, Fricke O, Schmidt P. Restoration of an Upper Anterior Tooth in an Adolescent with Autism Spectrum Disorder—A Student Case Report. Children. 2020; 7(11):237. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110237
Chicago/Turabian StyleDiekamp, Max, Leonie Jenter, Andreas G. Schulte, Oliver Fricke, and Peter Schmidt. 2020. "Restoration of an Upper Anterior Tooth in an Adolescent with Autism Spectrum Disorder—A Student Case Report" Children 7, no. 11: 237. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110237