What Solutions Exist for Developmental Delays Facing Indigenous Children Globally? A Co-Designed Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
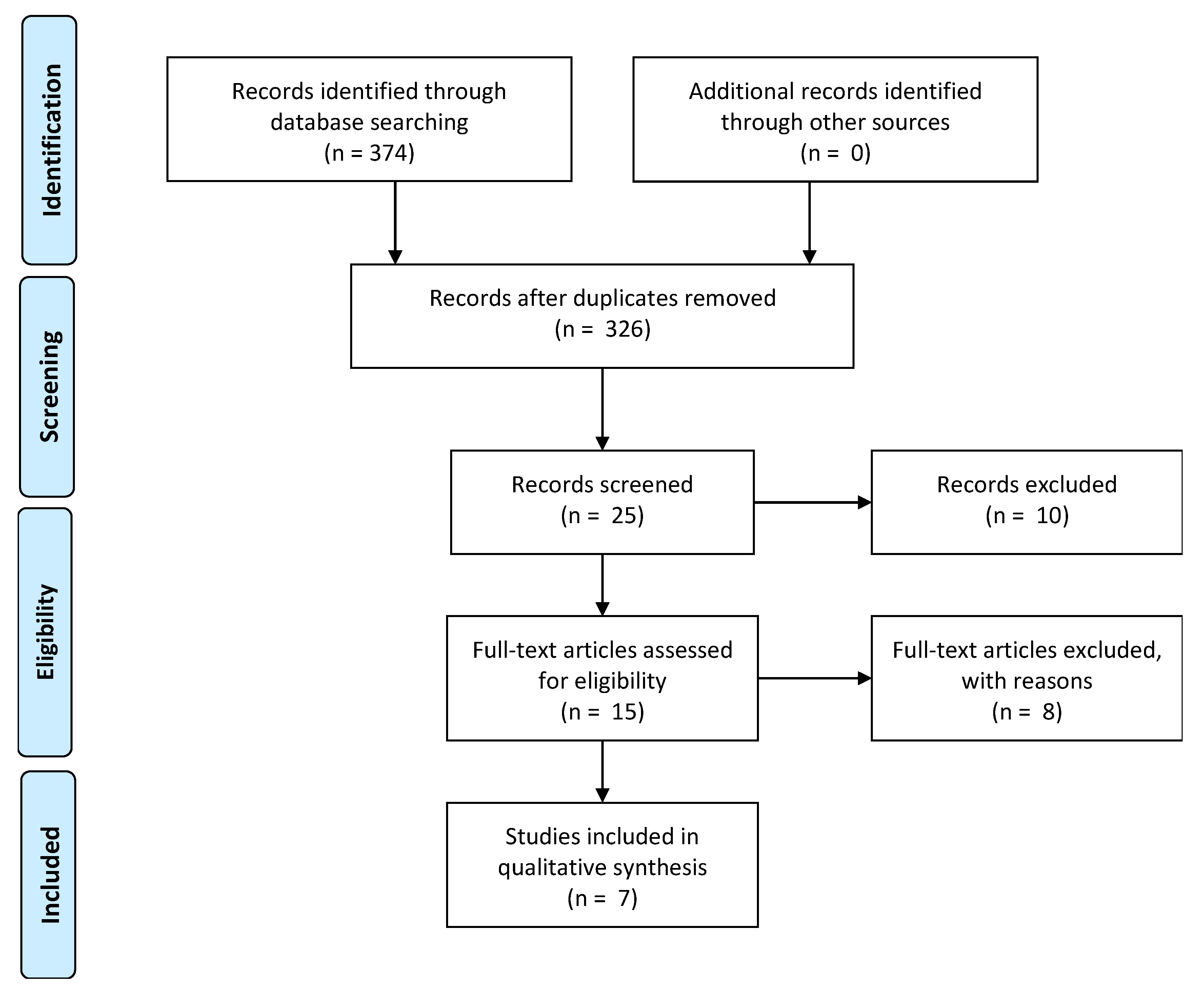
2.2. Search Strategy and Inclusion Criteria
2.3. Data Extraction
2.4. Data Synthesis and Interpretation
3. Results
3.1. Theme 1: Storytelling to Improve Educational Outcomes
3.2. Theme 2: Family Involvement Improved Development
3.3. Theme 3: Culturally Adapted Cognitive Behavioral Therapy to Reduce Trauma
3.4. Theme 4: Rewards-Based Teaching to Improve Child Attention in an Educational Setting
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Winkleby, A.M.; Jatulis, E.D.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [Green Version]
- Metzler, M.; Merrick, M.T.; Klevens, J.; Ports, K.A.; Ford, D.C. Adverse childhood experiences and life opportunities: Shifting the narrative. Child. Youth Serv. Rev. 2017, 72, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Hart, M. Indigenous Worldviews, Knowledge, and Research: The Development of an Indigenous Research Paradigm. J. Indig. Voices Soc. Work 2010, 1, 1–16. [Google Scholar]
- Paradies, Y. Colonisation, racism and indigenous health. J. Popul. Res. 2016, 33, 83–96. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples: 2015; AIHW: Canberra, Australia, 2015.
- Department of the Prime Minister and Cabinet. Closing the Gap Prime Minister’s Report 2018; Department of the Prime Minister and Cabinet: Canberra, Australia, 2018.
- Van Huizen, T.; Plantenga, J. Do children benefit from universal early childhood education and care? A meta-analysis of evidence from natural experiments. Econ. Educ. Rev. 2018, 66, 206–222. [Google Scholar] [CrossRef]
- Biddle, N. Ranking Regions: Revisiting an Index of Relative Indigenous Socioeconomic Outcomes; Working Paper No. 50; Centre for Aboriginal Economic Policy Research: Canberra, Australia, 2009. [Google Scholar]
- Gerlach, A.; Browne, A.J.; Greenwood, M. Engaging Indigenous families in a community-based Indigenous early childhood programme in British Columbia, Canada: A cultural safety perspective. Health Soc. Care Community 2017, 25, 1763–1773. [Google Scholar] [CrossRef]
- Kitson, R.; Bowes, J. Incorporating Indigenous Ways of Knowing in Early Education for Indigenous Children. Australas. J. Early Child. 2010, 35, 81–89. [Google Scholar] [CrossRef]
- Prochner, L. Early Childhood Education Programs for Indigenous Children in Canada, Australia and New Zealand: An Historical Review. Australas. J. Early Child. 2004, 29, 7–16. [Google Scholar] [CrossRef]
- Os, D.J.T.K.-V.D.; Jongmans, M.J.; Volman, M.J.M.; Lauteslager, P.E.M. Parent-Implemented Language Interventions for Children with a Developmental Delay: A Systematic Review. J. Policy Pract. Intellect. Disabil. 2017, 14, 129–137. [Google Scholar]
- Cappiello, M.M.; Gahagan, S. Early Child Development and Developmental Delay in Indigenous Communities. Pediatr. Clin. N. Am. 2009, 56, 1501–1517. [Google Scholar] [CrossRef]
- Brinkman, S.A.; Gialamas, A.; Rahman, A.; Mittinty, M.N.; A Gregory, T.; Silburn, S.; Goldfeld, S.; Zubrick, S.R.; Carr, V.; Janus, M.; et al. Jurisdictional, socioeconomic and gender inequalities in child health and development: Analysis of a national census of 5-year-olds in Australia. BMJ Open 2012, 2, e001075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawson, D.M.; Quinn, J. Complex Trauma in Children and Adolescents: Evidence-Based Practice in Clinical Settings. J. Clin. Psychol. 2013, 69, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J. Trauma Trails, Recreating Song Lines. The Transgenerational Effects of Trauma in Indigenous Australia; Spinifex Press: Melbourne, Australia, 2000. [Google Scholar]
- Anderson, L.M.; Shinn, C.; Charles, J.S.; Fullilove, M.T.; Scrimshaw, S.C.; Fielding, J.E.; Normand, J.; Sanchez-Way, R.; Richardson, T. Community Interventions to Promote Healthy Social Environments: Early Childhood Development and Family Housing: A Report on Recommendations of the Task Force on Community Preventive Services. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2002, 51, 1–9. [Google Scholar]
- National Health and Medical Research Council (NHMRC). Ethical Guidelines for Research with Aboriginal and Torres Strait Islander Peoples; National Health and Medical Research Council (NHMRC): Canberra, Australia, 2018.
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme CASP—Casp Systematic Review Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Systematic-Review-Checklist_2018.pdf (accessed on 12 December 2018).
- Virginia, B.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar]
- BigFoot, D.S.; Schmidt, S.R. Honoring Children, Mending the Circle: Cultural Adaptation of Trauma-Focused Cognitive-Behavioral Therapy for American Indian and Alaska Native Children. J. Clin. Psychol. 2010, 66, 847–856. [Google Scholar] [CrossRef]
- Morsette, A.; Swaney, G.; Stolle, D.; Schuldberg, D.; Pol, R.V.D.; Young, M. Cognitive Behavioral Intervention for Trauma in Schools (CBITS): School-based treatment on a rural American Indian reservation. J. Behav. Ther. Exp. Psychiatry 2009, 40, 169–178. [Google Scholar] [CrossRef]
- Spencer, T.D.; Kajian, M.; Petersen, D.B.; Bilyk, N. Effects of an Individualized Narrative Intervention on Children’s Storytelling and Comprehension Skills. J. Early Interv. 2013, 35, 243–269. [Google Scholar] [CrossRef]
- De Rios, M.D. Magical Realism: A Cultural Intervention for Traumatized Hispanic Children. Cult. Divers. Ment. Health 1997, 3, 159–170. [Google Scholar] [CrossRef]
- Kellam, S.G.; Brown, C.H.; Poduska, J.M.; Ialongo, N.S.; Wang, W.; Toyinbo, P.; Petras, H.; Ford, C.; Windham, A.; Wilcox, H.C. Effects of a universal classroom behavior management program in first and second grades on young adult behavioral, psychiatric, and social outcomes. Drug Alcohol Depend. 2008, 95, S5–S28. [Google Scholar] [CrossRef] [Green Version]
- Vazir, S.; Naidu, A.N.; Vidyasagar, P. Nutritional status, psychosocial development and the home environment of Indian rural children. Indian Pediatr. 1998, 35, 959–966. [Google Scholar] [PubMed]
- Fazel, M.; Doll, H.; Stein, A. A School-Based Mental Health Intervention for Refugee Children: An Exploratory Study. Clin. Child Psychol. Psychiatry 2009, 14, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J. Treating acute posttraumatic reactions in children and adolescents. Biol. Psychiatry 2003, 53, 827–833. [Google Scholar] [CrossRef]
- Tingstrom, D.H.; Sterling-Turner, H.E.; Wilczynski, S.M. The Good Behavior Game: 1969–2002. Behav. Modif. 2006, 30, 225–253. [Google Scholar] [CrossRef] [PubMed]
- Boyle, C.A.; Boulet, S.; Schieve, L.A.; Cohen, R.A.; Blumberg, S.J.; Yeargin-Allsopp, M.; Visser, S.; Kogan, M.D. Trends in the Prevalence of Developmental Disabilities in Us Children, 1997–2008. Pediatrics 2011, 127, 1034–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natalie, S.; Shonkoff, J.P.; Albert, M.A.; Yoshikawa, H.; Jacobs, A.; Stoltz, R.; Williams, D.R. Racial Disparities in Child Adversity in the U.S.: Interactions with Family Immigration History and Income. Am. J. Prev. Med. 2016, 50, 47–56. [Google Scholar]
- Spencer, T.D.; Slocum, T.A. The Effect of a Narrative Intervention on Story Retelling and Personal Story Generation Skills of Preschoolers with Risk Factors and Narrative Language Delays. J. Early Interv. 2010, 32, 178–199. [Google Scholar] [CrossRef]
- Heaton, B.; Gebel, C.; Crawford, A.; Barker, J.C.; Henshaw, M.; Garcia, R.I.; Riedy, C.; Wimsatt, M.A. Using Storytelling to Address Oral Health Knowledge in American Indian and Alaska Native Communities. Prev. Chronic Dis. 2018, 15, 63. [Google Scholar] [CrossRef] [Green Version]
- Geia, L.K.; Hayes, B.; Usher, K. Yarning/Aboriginal storytelling: Towards an understanding of an Indigenous perspective and its implications for research practice. Contemp. Nurse 2013, 46, 13–17. [Google Scholar] [CrossRef]
- BigFoot, D.S.; Funderburk, B. Honoring Children, Making Relatives: The Cultural Translation of Parent-Child Interaction Therapy for American Indian and Alaska Native Families. J. Psychoact. Drugs 2011, 43, 309–318. [Google Scholar] [CrossRef]
- Hajizadeh, N.; Stevens, E.R.; Applegate, M.; Huang, K.-Y.; Kamboukos, D.; Braithwaite, R.S.; Brotman, L.M. Potential return on investment of a family-centered early childhood intervention: A cost-effectiveness analysis. BMC Public Health 2017, 17, 796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCalman, J.; Heyeres, M.; Campbell, S.; Bainbridge, R.; Chamberlain, C.; Strobel, N.A.; Ruben, A. Family-centred interventions by primary healthcare services for Indigenous early childhood wellbeing in Australia, Canada, New Zealand and the United States: A systematic scoping review. BMC Pregnancy Childbirth 2017, 17, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodkind, J.R.; LaNoue, M.D.; Milford, J. Adaptation and Implementation of Cognitive Behavioral Intervention for Trauma in Schools with American Indian Youth. J. Clin. Child Adolesc. Psychol. 2010, 39, 858–872. [Google Scholar] [CrossRef]
- Goodkind, J.R.; LaNoue, M.; Freeland, C.L.A.L.; Freund, R. Feasibility, Acceptability, and Initial Findings from a Community-Based Cultural Mental Health Intervention for American Indian Youth and Their Families. J. Community Psychol. 2012, 40, 381–405. [Google Scholar] [CrossRef] [Green Version]
- Fortier, J.; Chartier, M.; Turner, S.; Murdock, N.; Turner, F.; Sareen, J.; O Afifi, T.; Katz, L.Y.; Brownell, M.; Bolton, J.; et al. Adapting and enhancing PAX Good Behavior Game for First Nations communities: A mixed-methods study protocol developed with Swampy Cree Tribal Council communities in Manitoba. BMJ Open 2018, 8, e018454. [Google Scholar] [CrossRef]
- Pressick, E.L.; Gray, M.A.; Cole, R.L.; Burkett, B. A systematic review on research into the effectiveness of group-based sport and exercise programs designed for Indigenous adults. J. Sci. Med. Sport 2016, 19, 726–732. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author, Year Published | Morsette et al. (2009) [23] | BigFoot et al. (2010) [22] | Kellam et al. (2008) [26] | Vazir et al. (1998) [27] | De Rios (1997) [25] | Fazel et al. (2009) [28] | Spencer et al. (2013) [24] |
| Population (N; Race, Age) | 48 Native American, 6th grade (11–12 years) | 1 Native American, 14 years | 1196 urban African American, 1st grade (6–7 years) | 3668 rural Native American, 0–6 years | 2 Hispanic, 6 and 8 years | 47 refugees, 4–19 years | 4 Hispanic, 1 Native American (4 years) |
| Type of Developmental Delay | Psychological symptoms following childhood trauma | Trauma exposure related | Behavioural disturbance | Psychosocial and physical delay | Psychosocial reactions to single event trauma | Emotional coping | Developmental disabilities |
| Study Aim | Decrease psychological trauma or post-traumatic stress disorder (PTSD) symptoms | Propose a form of culturally adapted trauma focused therapy | Improve positive classroom outcomes | Assess the psychosocial development of well nourished and malnourished children | Determine whether a novel type of therapy be adapted to a cultural context | Assess intervention effects of for poorly adjusting children | Improve the storytelling ability of learning delayed children |
| Design | Pre-post study | Case study | Cluster randomised controlled study | Cross-sectional study | Case study | Exploratory study | Pre-post study |
| Intervention | Trauma based, culturally adapted cognitive behaviour therapy | Trauma based, culturally adapted cognitive behaviour therapy | Good Behavior Game | Not applicable (N/A) | Storytelling to guide therapy | Mental health service help at school; support from parents at home | Use of storytelling computer software to improve storytelling ability |
| Findings | Improved life equivalent scores and decrease child Post-traumatic stress disorder symptom score scores | The model gives a framework that supports traditional beliefs and children-centred parenting practices | At 15 years follow-up, drug use and incarceration were lower in the intervention group compared to control | Paternal childcare involvement especially, spending time, telling stories, taking child for outings important for positive psychosocial development | Therapy can provide a culturally appropriate intervention to treat the psychological sequelae of trauma | Children receiving direct intervention from mental health services improved in peer problem scoring | There was improved storytelling with Story Champs software |
| Summary | Culturally adapted Cognitive Behavior Therapy (CBT) may ease psychological distress in adolescents | CBT may be a good form of treatment for adolescents who have been exposed to trauma | Good-Behaviour Game may produce long term positive outcomes | Physically and psychosocially well nourished children do better in school compared to those who are deprived | Play therapy, drawing, storytelling may be effective therapy in overcoming trauma in children | Mental health services and family support may benefit poorly adjusted children in the school setting | Story telling can improve the cognition and learning ability of children if adapted prior to formative education |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macniven, R.; Jeffries, T.L., Jr.; Meharg, D.; Talbot, F.; Rambaldini, B.; Edwards, E.; Hickie, I.B.; Sloan, M.; Gwynne, K. What Solutions Exist for Developmental Delays Facing Indigenous Children Globally? A Co-Designed Systematic Review. Children 2020, 7, 285. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120285
Macniven R, Jeffries TL Jr., Meharg D, Talbot F, Rambaldini B, Edwards E, Hickie IB, Sloan M, Gwynne K. What Solutions Exist for Developmental Delays Facing Indigenous Children Globally? A Co-Designed Systematic Review. Children. 2020; 7(12):285. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120285
Chicago/Turabian StyleMacniven, Rona, Thomas Lee Jeffries, Jr., David Meharg, Folau Talbot, Boe Rambaldini, Elaine Edwards, Ian B. Hickie, Margaret Sloan, and Kylie Gwynne. 2020. "What Solutions Exist for Developmental Delays Facing Indigenous Children Globally? A Co-Designed Systematic Review" Children 7, no. 12: 285. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120285