Pediatric Spontaneous Pneumomediastinum after a Push-Up Exercise: An Uncommon Complication of a Common Exercise


{kind=link}
{kind=link}
Abstract
:1. Introduction
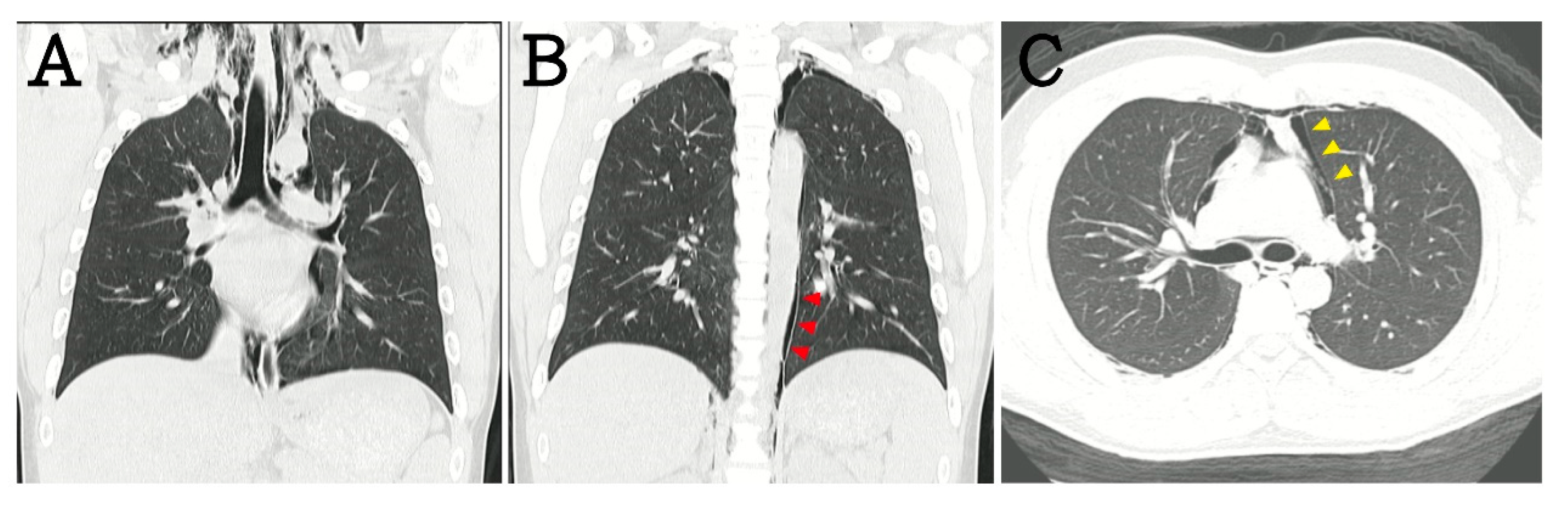
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chalumeau, M.; Le Clainche, L.; Sayeg, N.; Sannier, N.; Michel, J.L.; Marianowski, R.; Jouvet, P.; Scheinmann, P.; de Blic, J. Spontaneous pneumomediastinum in children. Pediatric Pulmonol. 2001, 31, 67–75. [Google Scholar] [CrossRef]
- Benlamkaddem, S.; Berdai, M.A.; Labib, S.; Harandou, M. A Case of Spontaneous Pneumomediastinum with Subcutaneous Emphysema in Children. Children 2018, 5, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, I.S.; Lee, Y.H.; Yamout, S.Z.; Fakir, S.; Reynolds, A.M. Ultrasound guided percutaneous relief of tension pneumomediastinum in a 1-day-old newborn. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, K.L.; Imamuddin, S.; Kumar, A.P. Isolated tension pneumopericardium in a case of acute lymphoblastic leukemia. Indian Heart J. 2013, 65, 705–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valiyakath, D.; Al Busaidi, T.; Al Shamsi, S.; Al Sawafi, Y. Pneumorrhachis with Spontaneous Pneumomediastinum: Should It Raise Special Concerns? Oman Med. J. 2018, 33, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Pradilla, G.; Witham, T.F.; Gokaslan, Z.L.; Bydon, A. The clinical significance of pneumorachis: A case report and review of the literature. J. Trauma 2010, 68, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Dionísio, P.; Martins, L.; Moreira, S.; Manique, A.; Macedo, R.; Caeiro, F.; Boal, L.; Bárbara, C. Spontaneous pneumomediastinum: Experience in 18 patients during the last 12 years. J. Bras. Pneumol. Publicacao Soc. Bras. Pneumol. E Tisilogia 2017, 43, 101–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dajer-Fadel, W.L.; Argüero-Sánchez, R.; Ibarra-Pérez, C.; Navarro-Reynoso, F.P. Systematic review of spontaneous pneumomediastinum: A survey of 22 years’ data. Asian Cardiovasc. Thorac. Ann. 2014, 22, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Takada, K.; Matsumoto, S.; Hiramatsu, T.; Kojima, E.; Watanabe, H.; Sizu, M.; Okachi, S.; Ninomiya, K. Management of spontaneous pneumomediastinum based on clinical experience of 25 cases. Respir. Med. 2008, 102, 1329–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihos, P.; Potaris, K.; Gakidis, I.; Mazaris, E.; Sarras, E.; Kontos, Z. Sports-related spontaneous pneumomediastinum. Ann. Thorac. Surg. 2004, 78, 983–986. [Google Scholar] [CrossRef] [PubMed]
- Murayama, S.; Gibo, S. Spontaneous pneumomediastinum and Macklin effect: Overview and appearance on computed tomography. World J. Radiol. 2014, 6, 850–854. [Google Scholar] [CrossRef] [PubMed]
- Bonardi, C.M.; Spadini, S.; Fazio, P.C.; Galiazzo, M.; Voltan, E.; Coscini, N.; Padalino, M.; Daverio, M. Nontraumatic tension pneumopericardium in nonventilated pediatric patients: A review. J. Card Surg. 2019, 34, 829–836. [Google Scholar] [CrossRef]
- Edmonds, L.; Ireland, S. What is that around the heart? Pneumopericardium. J. Paediatr. Child. Health 2015, 51, 347–348. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsay, C.-Y.; Chen, Y.-L.; Chen, C.-S.; Lin, P.-C.; Wu, M.-Y. Pediatric Spontaneous Pneumomediastinum after a Push-Up Exercise: An Uncommon Complication of a Common Exercise. Children 2020, 7, 287. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120287
Tsay C-Y, Chen Y-L, Chen C-S, Lin P-C, Wu M-Y. Pediatric Spontaneous Pneumomediastinum after a Push-Up Exercise: An Uncommon Complication of a Common Exercise. Children. 2020; 7(12):287. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120287
Chicago/Turabian StyleTsay, Chih-Yi, Yu-Long Chen, Chien-Sheng Chen, Po-Chen Lin, and Meng-Yu Wu. 2020. "Pediatric Spontaneous Pneumomediastinum after a Push-Up Exercise: An Uncommon Complication of a Common Exercise" Children 7, no. 12: 287. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120287