Genetic Sequence Variants in TLR4, MBL or IL-1 Receptor Antagonist is not Associated to Increased Risk for Febrile Neutropenia in Children with ALL

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Data Collection
2.3. Gene Sequence Variant Analysis
2.4. Statistical Analysis
3. Results
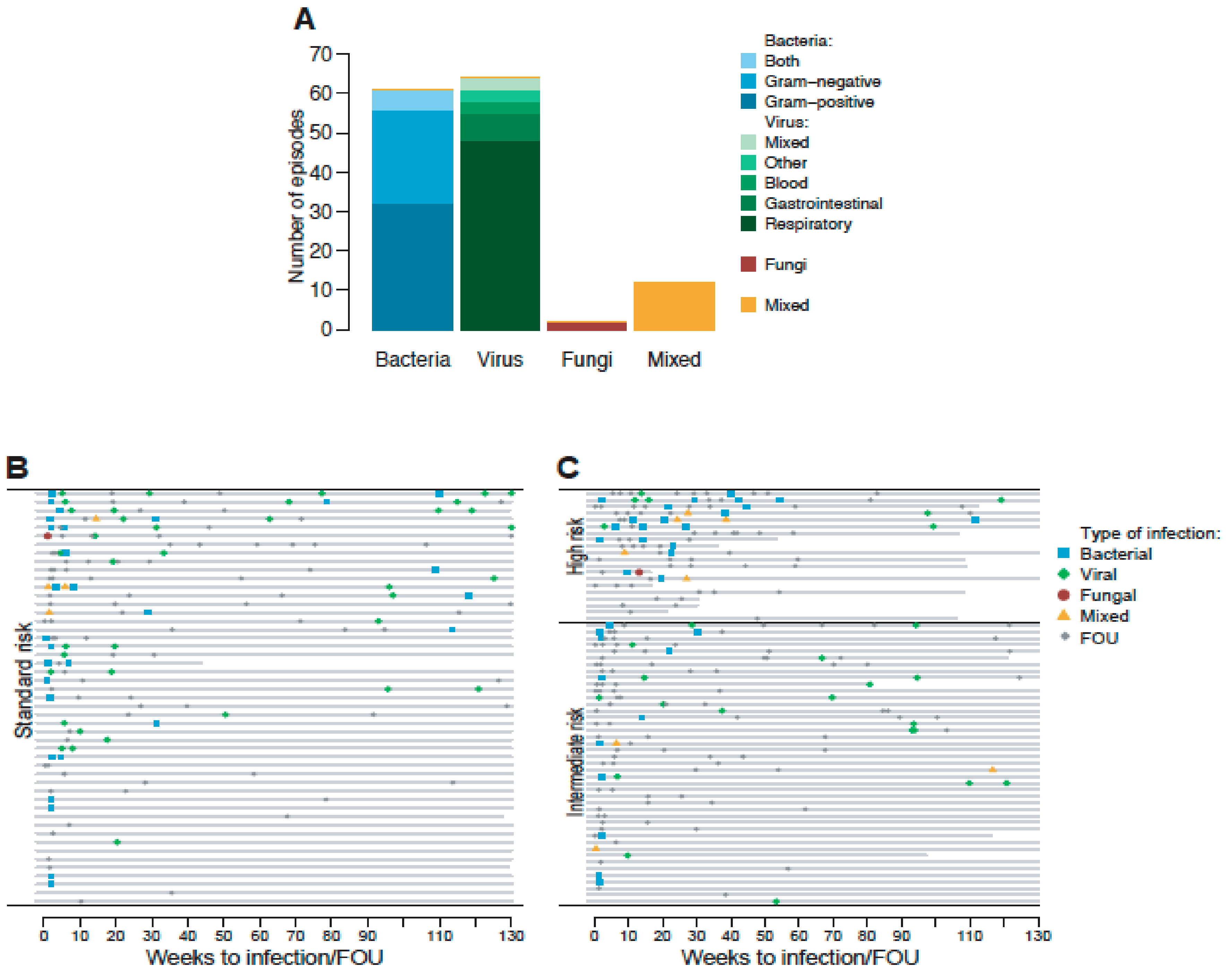
3.1. Patient Characteristics and Episodes of FN
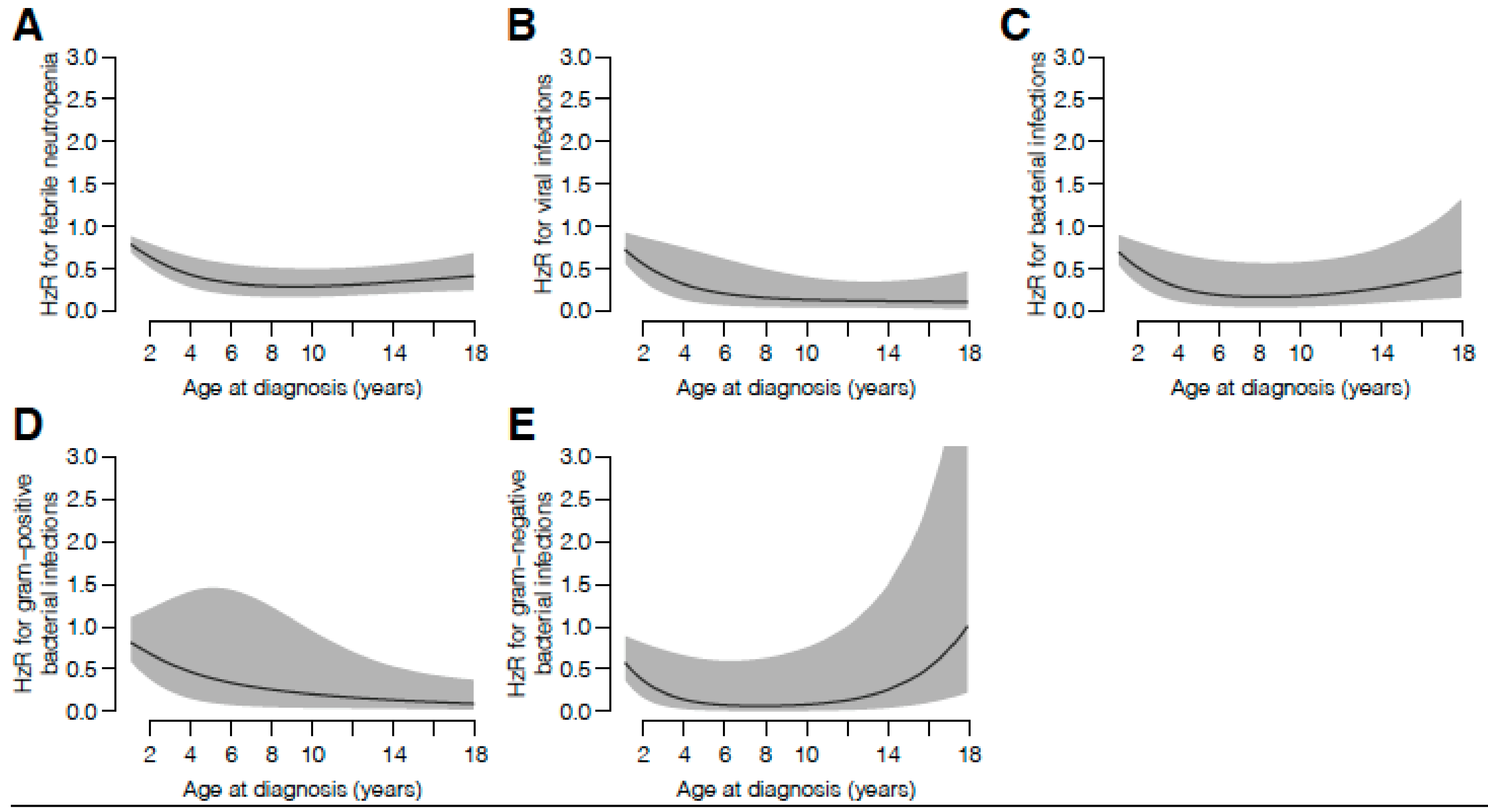
3.2. Genetic Sequence Variants and the Overall Risk of FN and MDI
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Schmiegelow, K.; Forestier, E.; Hellebostad, M.; Heyman, M.; Kristinsson, J.; Soderhall, S.; Taskinen, M. Long-term results of NOPHO ALL-92 and ALL-2000 studies of childhood acute lymphoblastic leukemia. Leukemia 2010, 24, 345–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandeberg, M.A.; Johansson, E.; Wettergren, L.; Björk, O.; Hertting, O.; Nilsson, A. Antibiotic use during infectious episodes in the first 6 months of anticancer treatment-A Swedish cohort study of children aged 7–16 years. Pediatr. Blood Cancer 2017, 64, e26397. [Google Scholar] [CrossRef] [PubMed]
- Lund, B.; Åsberg, A.; Heyman, M.; Kanerva, J.; Harila-Saari, A.; Hasle, H.; Söderhäll, S.; Jónsson, Ó.G.; Lydersen, S.; Schmiegelow, K.; et al. Risk factors for treatment related mortality in childhood acute lymphoblastic leukaemia. Pediatr. Blood Cancer 2010, 56, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Inaba, H.; Pei, D.; Wolf, J.; Howard, S.C.; Hayden, R.T.; Go, M.; Varechtchouk, O.; Hahn, T.; Buaboonnam, J.; Metzger, M.L.; et al. Infection-related complications during treatment for childhood acute lymphoblastic leukemia. Ann. Oncol. 2017, 28, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-J.; Chang, H.-H.; Yang, Y.-L.; Lu, M.-Y.; Shao, P.-L.; Fu, C.-M.; Chou, A.-K.; Liu, Y.-L.; Lin, K.-H.; Huang, L.-M.; et al. Infectious complications in children with acute lymphoblastic leukemia treated with the Taiwan Pediatric Oncology Group protocol: A 16-year tertiary single-institution experience. Pediatr. Blood Cancer 2017, 64, e26535. [Google Scholar] [CrossRef] [PubMed]
- Söderman, M.; Rhedin, S.; Tolfvenstam, T.; Rotzén-Östlund, M.; Albert, J.; Broliden, K.; Lindblom, A. Frequent Respiratory Viral Infections in Children with Febrile Neutropenia—A Prospective Follow-Up Study. PLoS ONE 2016, 11, e0157398. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Tarrés, M.; Arredondo-García, J.L.; Rivera-Luna, R.; Klünder-Klünder, M.; Mancilla-Ramírez, J.; Sánchez-Urbina, R.; Vázquez-Cruz, M.Y.; Juárez-Villegas, L.E.; Palomo-Colli, M.A. Interleukin-1 Receptor Antagonist Gene Polymorphism Increases Susceptibility to Septic Shock in Children With Acute Lymphoblastic Leukemia. Pediatr. Infect. Dis. J. 2013, 32, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Neth, O.; Hann, I.; Turner, M.W.; Klein, N.J. Deficiency of mannose-binding lectin and burden of infection in children with malignancy: A prospective study. Lancet 2001, 358, 614–618. [Google Scholar] [CrossRef]
- Dommett, R.; Chisholm, J.; Turner, M.; Bajaj-Elliott, M.; Klein, N.J. Mannose-binding Lectin Genotype Influences Frequency and Duration of Infectious Complications in Children With Malignancy. J. Pediatr. Hematol. 2013, 35, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Pana, Z.D.; Samarah, F.; Papi, R.; Antachopoulos, C.; Papageorgiou, T.; Farmaki, E.; Hatzipantelis, E.; Tragiannidis, A.; Vavatsi-Christaki, N.; Kyriakidis, D.; et al. Mannose binding lectin and ficolin-2 polymorphisms are associated with increased risk for bacterial infections in children with B acute lymphoblastic leukemia. Pediatr. Blood Cancer 2014, 61, 1017–1022. [Google Scholar] [CrossRef]
- Pehlivan, M.; Sahin, H.H.; Ozdilli, K.; Onay, H.; Ozcan, A.; Ozkinay, F.; Pehlivan, S. Gene Polymorphisms and Febrile Neutropenia in Acute Leukemia—No Association with IL-4, CCR-5, IL-1RA, but the MBL-2, ACE, and TLR-4 Are Associated with the Disease in Turkish Patients: A Preliminary Study. Genet. Test. Mol. Biomarkers 2014, 18, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Schnetzke, U.; Spies-Weisshart, B.; Yomade, O.; Fischer, M.; Rachow, T.; Schrenk, K.; Gläser, A.; Von Lilienfeld-Toal, M.; Hochhaus, A.; Scholl, S. Polymorphisms of Toll-like receptors (TLR2 and TLR4) are associated with the risk of infectious complications in acute myeloid leukemia. Genes Immun. 2014, 16, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Miedema, K.G.E.; Poele, E.M.T.; Tissing, W.J.E.; Postma, D.S.; Koppelman, G.H.; de Pagter, A.P.; Kamps, W.A.; Alizadeh., B.Z.; de Bont, E.S.J.M. Association of polymorphisms in the TLR4 gene with the risk of developing neutropenia in children with leukemia. Leukemia 2011, 25, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Fekete, F.; Fadgyas, B.; Papp, E.; Szilágyi, Á; Prohászka, Z.; Müller, B.; Kovács, G. The role of mannose binding lectin on fever episodes in pediatric oncology patients. Pathol. Oncol. Res. 2015, 22, 139–143. [Google Scholar] [CrossRef]
- Lausen, B.F.; Andreassen, B.; Schmiegelow, K.; Madsen, H.O.; Garred, P. Infections during induction therapy of childhood acute lymphoblastic leukemia—No association to mannose? Binding lectin deficiency. Eur. J. Haematol. 2006, 76, 481–487. [Google Scholar] [CrossRef]
- Arnalich, F.M.; López-Maderuelo, D.; Codoceo, R.; Lopez, J.; Solis-Garrido, L.M.; Capiscol, C.; Fernandez-Capitán, C.; Madero, R.; Montiel, C. Interleukin-1 receptor antagonist gene polymorphism and mortality in patients with severe sepsis. Clin. Exp. Immunol. 2002, 127, 331–336. [Google Scholar] [CrossRef]
- Fang, X.M.; Schroder, S.; Hoeft, A.; Stuber, F. Comparison of two polymorphisms of the interleukin-1 gene family: Interleukin-1 receptor antagonist polymorphism contributes to susceptibility to severe sepsis. Crit Care Med. 1999, 27, 1330–1334. [Google Scholar] [CrossRef]
- Freifeld, A.G.; Bow, E.J.; Sepkowitz, K.A.; Boeckh, M.J.; Ito, J.I.; Mullen, C.A.; Raad, I.I.; Rolston, K.V.; Young, J.-A.; Wingard, J. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the iInfectious Diseases Society of America. Clin. Infect. Dis. 2011, 52, 56–93. [Google Scholar] [CrossRef] [Green Version]
- Tiveljung-Lindell, A.; Rotzén-Östlund, M.; Gupta, S.; Ullstrand, R.; Grillner, L.; Zweygberg-Wirgart, B.; Allander, T. Development and implementation of a molecular diagnostic platform for daily rapid detection of 15 respiratory viruses. J. Med. Virol. 2009, 81, 167–175. [Google Scholar] [CrossRef]
- Henke-Gendo, C.; Harste, G.; Juergens-Saathoff, B.; Mattner, F.; Deppe, H.; Heim, A. New Real-Time PCR Detects Prolonged Norovirus Excretion in Highly Immunosuppressed Patients and Children. J. Clin. Microbiol. 2009, 47, 2855–2862. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, A.; Adams, O.; Laws, H.-J.; Schroten, H.; Tenenbaum, T. Quantitative detection of norovirus excretion in pediatric patients with cancer and prolonged gastroenteritis and shedding of norovirus. J. Med. Virol. 2008, 80, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarlow, J.K.; Blakemore, A.I.F.; Lennard, A.; Solari, R.; Hughes, H.N.; Steinkasserer, A.; Duff, G.W. Polymorphism in human IL-1 receptor antagonist gene intron 2 is caused by variable numbers of an 86-bp tandem repeat. Qual. Life Res. 1993, 91, 403–404. [Google Scholar] [CrossRef] [PubMed]
- Wahlund, M.; Nilsson, A.; Kahlin, A.Z.; Broliden, K.; Myrberg, I.H.; Appell, M.L.; Berggren, A. The Role of TPMT, ITPA, and NUDT15 Variants during Mercaptopurine Treatment of Swedish Pediatric Patients with Acute Lymphoblastic Leukemia. J. Pediatr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.K.; Gill, R.D. Cox’s Regression Model for Counting Processes: A Large Sample Study. Ann. Statist. 1982, 10, 1110–1120. [Google Scholar] [CrossRef]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Therneau, T.M. A Package for Survival Analysis in S. Available online: https://CRAN.R-project.org/package=survival (accessed on 4 February 2020).
- R Core Team. R: A Language and Environment for Statistical Computing. 2018. Available online: https://www.r-project.org/ (accessed on 13 February 2012).
- Lindblom, A.; Bhadri, V.; Söderhäll, S.; Öhrmalm, L.; Wong, M.; Norbeck, O.; Lindau, C.; Rotzén-Östlund, M.; Allander, T.; Catchpoole, D.; et al. Respiratory viruses, a common microbiological finding in neutropenic children with fever. J. Clin. Virol. 2010, 47, 234–237. [Google Scholar] [CrossRef]
- Torres, J.P.; De la Maza, V.; Kors, L.; Villarroel, M.; Piemonte, P.; Izquierdo, G.; Salgado, C.; Tordecilla, J.; Contardo, V.; Farfán, M.J.; et al. Respiratory Viral Infections and Coinfections in Children With Cancer, Fever and Neutropenia: Clinical Outcome of Infections Caused by Different Respiratory Viruses. Pediatr. Infect. Dis. J. 2016, 35, 949–954. [Google Scholar] [CrossRef]
- Suryadevara, M.; Tabarani, C.M.; Bartholoma, N.; Rosenberg, H.F.; Domachowske, J.B. Nasopharyngeal Detection of Respiratory Viruses in Febrile Neutropenic Children. Clin. Pediatr. 2012, 51, 1164–1167. [Google Scholar] [CrossRef]
- Koskenvuo, M.; Möttönen, M.; Rahiala, J.; Saarinen-Pihkala, U.M.; Riikonen, P.; Waris, M.; Ziegler, T.; Uhari, M.; Salmi, T.T.; Ruuskanen, O. Respiratory Viral Infections in Children With Leukemia. Pediatr. Infect. Dis. J. 2008, 27, 974–980. [Google Scholar] [CrossRef]
- Aldemir-Kocabaş, B.; Karbuz, A.; Pekpak, E.; Karahan, Z.C.; Dolapçi, I.; Ince, E.; Uysal, Z.; Yavuz, G.; Çiftçi, E.; Ince, E. Effects of respiratory viruses on febrile neutropenia attacks in children. Turk. J. Pediatr. 2017, 59, 511. [Google Scholar] [CrossRef]
- Koskenvuo, M.; Möttönen, M.; Rahiala, J.; Saarinen-Pihkala, U.M.; Riikonen, P.; Waris, M.; Ziegler, T.; Uhari, M.; Ruuskanen, O.; Salmi, T.T. Mixed Bacterial-Viral Infections in Septic Children With Leukemia. Pediatr. Infect. Dis. J. 2007, 26, 1133–1136. [Google Scholar] [CrossRef] [PubMed]
- Wahlund, M.; Sinha, I.; Broliden, K.; Saghafian-Hedengren, S.; Nilsson, A.; Berggren, A. The Feasibility of Host Transcriptome Profiling as a Diagnostic Tool for Microbial Etiology in Childhood Cancer Patients with Febrile Neutropenia. Int. J. Mol. Sci. 2020, 21, 5305. [Google Scholar] [CrossRef] [PubMed]
- Agnese, D.M.; Calvano, J.E.; Hahm, S.J.; Coyle, S.M.; Corbett, S.A.; Calvano, S.E.; Lowry, S.F. Human Toll-Like Receptor 4 Mutations but Not CD14 Polymorphisms Are Associated with an Increased Risk of Gram-Negative Infections. J. Infect. Dis. 2002, 186, 1522–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenz, E.; Mira, J.P.; Frees, K.L.; Schwartz, D.A. Relevance of Mutations in the TLR4 Receptor in Patients with Gram-Negative Septic Shock. Arch. Intern. Med. 2002, 162, 1028–1032. [Google Scholar] [CrossRef]
- Awomoyi, A.A.; Rallabhandi, P.; Pollin, T.I.; Lorenz, E.; Sztein, M.B.; Boukhvalova, M.S.; Hemming, V.G.; Blanco, J.C.G.; Vogel, S.N. Association of TLR4 Polymorphisms with Symptomatic Respiratory Syncytial Virus Infection in High-Risk Infants and Young Children. J. Immunol. 2007, 179, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Frakking, F.; Van De Wetering, M.; Brouwer, N.; Dolman, K.; Geissler, J.; Lemkes, B.; Caron, H.; Kuijpers, T. The role of mannose-binding lectin (MBL) in paediatric oncology patients with febrile neutropenia. Eur. J. Cancer 2006, 42, 909–916. [Google Scholar] [CrossRef]
- Danis, V.A.; Millington, M.; Hyland, V.J.; Grennan, D. Cytokine production by normal human monocytes: Inter-subject variation and relationship to an IL-1 receptor antagonist (IL-1Ra) gene polymorphism. Clin. Exp. Immunol. 1995, 99, 303–310. [Google Scholar] [CrossRef]
- Hurme, M.; Santtila, S. IL-1 receptor antagonist (IL-1Ra) plasma levels are co-ordinately regulated by both IL-1Ra and IL-1beta genes. Eur. J. Immunol. 1998, 28, 2598–2602. [Google Scholar] [CrossRef]
- Bhadri, V.A.; Beckett, S.M.; Duncan, C.; Marshall, G.M.; Ashton, L.J. Variation in Toll-like receptor 9 gene modifies the risk of infection in children treated for acute lymphoblastic leukemia. Leuk. Lymphoma 2012, 53, 1828–1830. [Google Scholar] [CrossRef]
- Kidas, E.; Möricke, A.; Beier, R.; Welte, K.; Schrappe, M.; Stanulla, M.; Grigull, L. Genetic polymorphisms of the lymphotoxin alpha gene are associated with increased risk for lethal infections during induction therapy for childhood acute leukemia: A case-control study. Int. J. Hematol. 2009, 89, 584–591. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Gender | |
| Female | 58 (47.5) |
| Male | 64 (52.4) |
| Risk Group | |
| Standard risk | 54 (44.3) |
| Intermediate risk | 48 (39.3) |
| High risk | 20 (16.4) |
| Protocol | |
| NOPHO ALL-2000 | 43 (35.2) |
| NOPHO ALL-2008 | 79 (64.8) |
| Phenotype of ALL | |
| Pre-B ALL | 106 (86.9) |
| T-cell ALL | 16 (13.1) |
| Outcome | |
| Relapse * | 8 (6.6) |
| HSCT | 2 (1.6) |
| Death during follow up | 2 (1.6) |
| Median (range; IQR) | |
| Age at diagnosis (years) | 5.4 (1.1–17.9; 3.3–10.4) |
| Febrile Neutropenia (n = 380) | Bacterial BSI (n = 61) | Viral Infection (n = 64) | ||||
|---|---|---|---|---|---|---|
| Sequence Variant | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted |
| TLR4 rs2737190 | 1.03 (0.78–1.35; 0.83) | 1.01 (0.82–1.24; 0.93) | 1.02 (0.59- 1.75; 0.94) | 0.93 (0.59–1.46; 0.74) | 0.88 (0.48–1.62; 0.69) | 0.96 (0.56–1.66; 0.89) |
| TLR4 rs1927911 | 0.93 (0.71–1.21; 0.6) | 0.96 (0.78–1.18; 0.69) | 0.98 (0.57–1.70; 0.95) | 0.97 (0.61–1.55; 0.90) | 0.70 (0.39–1.27; 0.24) | 0.74 (0.43–1.26; 0.27) |
| TLR4 rs10759931 | 0.93 (0.71–1.23; 0.62) | 0.94 (0.77–1.15; 0.55) | 0.89 (0.50–1.61; 0.71) | 0.88 (0.56–1.41; 0.60) | 2.46 (1.17–5.18; 0.017) | 2.38 (1.24–4.57; 0.0094) |
| TLR4 rs11536889 | 0.96 (0.72–1.28; 0.79) | 1.09 (0.86–1.39; 0.45) | 0.82 (0.46–1.45; 0.49) | 1.02 (0.59–1.76; 0.94) | 1.59 (0.86–2.96; 0.14) | 1.94 (1.14–3.31; 0.015) |
| TLR4 rs4986790 | 1.04 (0.63–1.72; 0.87) | 1.04 (0.73–1.48; 0.84) | 1.25 (0.52–2.99; 0.62) | 1.23 (0.63–2.39; 0.54) | 0.80 (0.28–2.27; 0.68) | 0.92 (0.35–2.39; 0.87) |
| TLR4 rs4986791 | 0.94 (0.61–1.45; 0.79) | 0.90 (0.66–1.22; 0.48) | 0.93 (0.42–2.04; 0.85) | 0.80 (0.44–1.47; 0.48) | 0.73 (0.29–1.85; 0.5) | 0.74 (0.31–1.75; 0.49) |
| TLR4 rs4986790 and rs4986791 | 0.96 (0.64–1.45; 0.86) | 0.94 (0.70–1.27; 0.68) | 1.18 (0.57–2.45; 0.66) | 1.06 (0.58–1.91; 0.85) | 0.69 (0.27–1.76; 0.43) | 0.71 (0.30–1.70; 0.44) |
| MBL rs1800450, rs5030737 and rs1800451 | 1.09 (0.83–1.43; 0.53) | 1.09 (0.89–1.35; 0.41) | 0.70 (0.37–1.32; 0.27) | 0.78 (0.44–1.38; 0.39) | 0.78 (0.37–1.67; 0.53) | 0.79 (0.40–1.58; 0.51) |
| IL1RN*2 | 1.08 (0.83–1.41; 0.55) | 1.07 (0.86–1.34; 0.52) | 0.49 (0.28–0.88; 0.016) | 0.51 (0.31–0.84; 0.009) | 1.65 (0.88–3.10; 0.12) | 1.47 (0.84–2.58; 0.17) |
| IL1RN*3 | 1.24 (0.58–2.68; 0.58) | 0.87 (0.58–1.30; 0.49) | 0.25 (0.04–1.54; 0.14) | 0.16 (0.05–0.51; 0.0022) | 1.72 (0.62–4.74; 0.3) | 1.09 (0.47–2.54; 0.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wahlund, M.; Lindqvist Appell, M.; Hed Myrberg, I.; Berggren, A.; Nilsson, A. Genetic Sequence Variants in TLR4, MBL or IL-1 Receptor Antagonist is not Associated to Increased Risk for Febrile Neutropenia in Children with ALL. Children 2020, 7, 296. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120296
Wahlund M, Lindqvist Appell M, Hed Myrberg I, Berggren A, Nilsson A. Genetic Sequence Variants in TLR4, MBL or IL-1 Receptor Antagonist is not Associated to Increased Risk for Febrile Neutropenia in Children with ALL. Children. 2020; 7(12):296. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120296
Chicago/Turabian StyleWahlund, Martina, Malin Lindqvist Appell, Ida Hed Myrberg, Anna Berggren, and Anna Nilsson. 2020. "Genetic Sequence Variants in TLR4, MBL or IL-1 Receptor Antagonist is not Associated to Increased Risk for Febrile Neutropenia in Children with ALL" Children 7, no. 12: 296. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120296