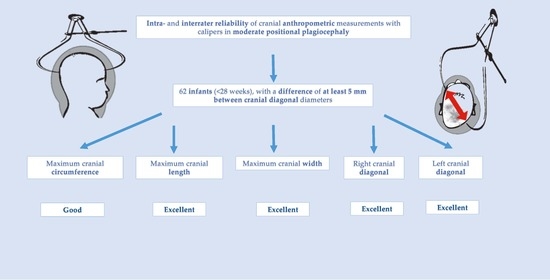
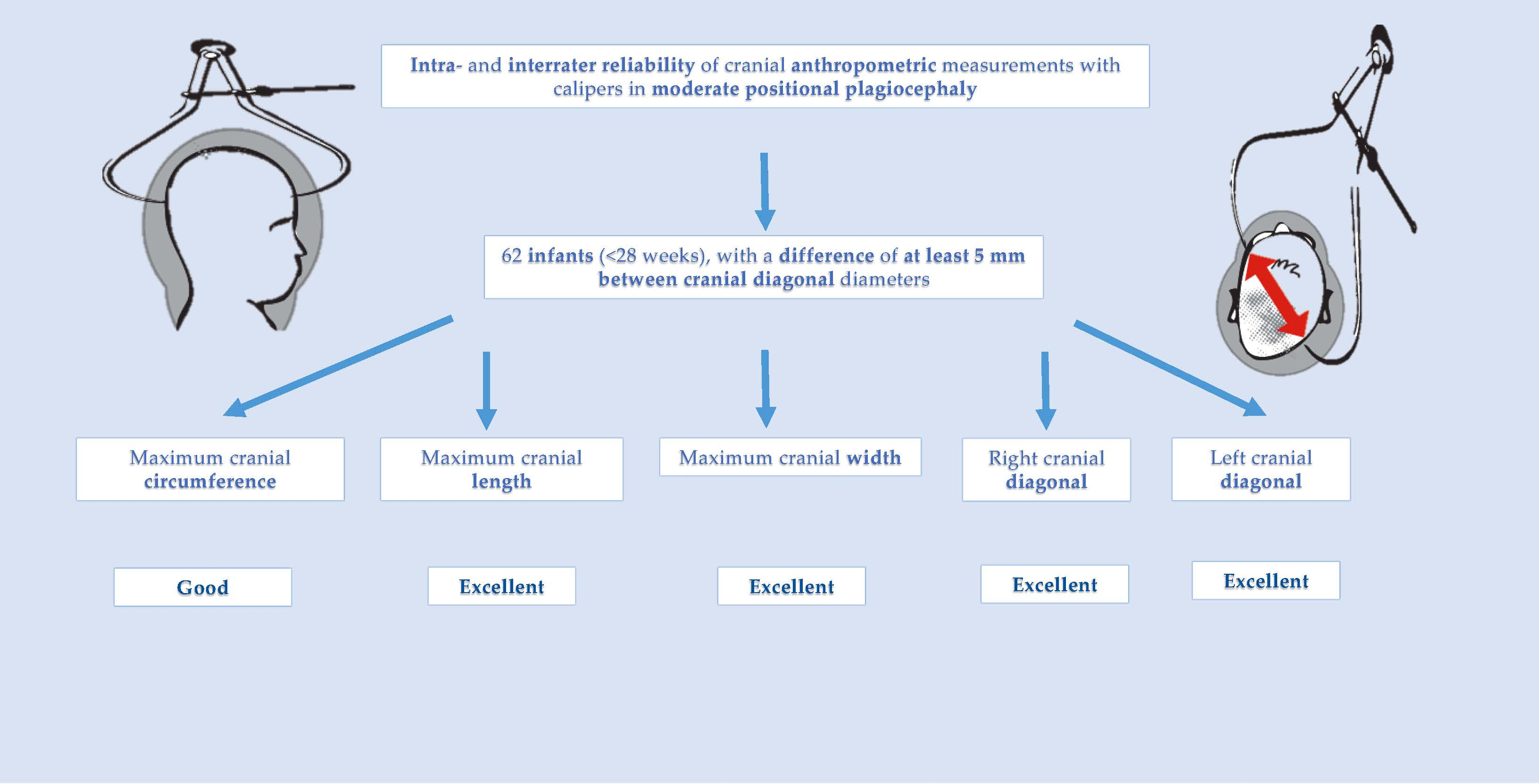
Interrater and Intrarater Reliability of Cranial Anthropometric Measurements in Infants with Positional Plagiocephaly


 ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurements
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stellwagen, L.; Hubbard, E.; Chambers, C.; Jones, K.L. Torticollis, facial asymmetry and plagiocephaly in normal newborns. Arch. Dis. Child. 2008, 93, 827–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, R.; Walker, M.L. Posterior plagiocephaly. Child’s Nerv. Syst. 2012, 28, 1389–1393. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Proctor, M. Diagnosis and management of deformational plagiocephaly: A review. J. Neurosurg. Pediatr. 2009, 3, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Baumler, C.; Leboucq, N.; Captier, G. Étude de l’asymétrie mandibulaire dans les plagiocéphalies sans synostose. Rev. Stomatol. Chir. Maxillofac. 2007, 108, 424–430. [Google Scholar] [CrossRef]
- Peitsch, W.K.; Keefer, C.H.; LaBrie, R.A.; Mulliken, J.B. Incidence of Cranial Asymmetry in Healthy Newborns. Pediatrics 2002, 110, e72. [Google Scholar] [CrossRef] [Green Version]
- Littlefield, T.R.; Saba, N.M.; Kelly, K.M. On the current incidence of deformational plagiocephaly: An estimation based on prospective registration at a single center. In Proceedings of the Seminars in Pediatric Neurology; Elsevier: Amsterdam, The Netherlands, 2004; Volume 11, pp. 301–304. [Google Scholar]
- Hutchison, B.L.; Hutchison, L.a.D.; Thompson, J.M.D.; Mitchell, E.A. Plagiocephaly and brachycephaly in the first two years of life: A prospective cohort study. Pediatrics 2004, 114, 970–980. [Google Scholar] [CrossRef] [Green Version]
- Bialocerkowski, A. Physiotherapy reduces the risk of deformational plagiocephaly in infants who have a preferred head position when lying supine. Aust. J. Physiother. 2008, 54, 283. [Google Scholar] [CrossRef]
- Koren, A.; Reece, S.M.; Kahn-D’angelo, L.; Medeiros, D. Parental Information and Behaviors and Provider Practices Related to Tummy Time and Back to Sleep. J. Pediatr. Health Care 2010, 24, 222–230. [Google Scholar] [CrossRef]
- Argenta, L.; David, L.; Thompson, J. Clinical classification of positional plagiocephaly. J. Craniofacial Surg. 2004, 15, 368–372. [Google Scholar] [CrossRef]
- Spermon, J.; Spermon-Marijnen, R.; Scholten-Peeters, W. Clinical classification of deformational plagiocephaly according to Argenta: A reliability study. J. Craniofacial Surg. 2008, 19, 664–668. [Google Scholar] [CrossRef]
- Hutchison, B.L.; Stewart, A.W.; de Chalain, T.B.; Mitchell, E.A. A randomized controlled trial of positioning treatments in infants with positional head shape deformities. Acta Pediatr. Int. J. Paediatr. 2010, 99, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Aarnivala, H.; Vuollo, V.; Heikkinen, T.; Harila, V.; Holmström, L.; Pirttiniemi, P.; Valkama, A.M. Accuracy of measurements used to quantify cranial asymmetry in deformational plagiocephaly. J. Cranio Maxillofac. Surg. 2017, 45, 1349–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collett, B.R.; Gray, K.E.; Starr, J.R.; Heike, C.L.; Cunningham, M.L.; Speltz, M.L.; Heike, C.L.; Collett, B.R.; Cunningham, M.L.; Starr, J.R.; et al. Development at Age 36 Months in Children With Deformational Plagiocephaly. Pediatrics 2013, 131, e109–e115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Wijk, R.M.; Van Til, J.A.; Groothuis-Oudshoorn, C.G.M.; L’Hoir, M.P.; Boere-Boonekamp, M.M.; Ijzerman, M.J. Parents’ decision for helmet therapy in infants with skull deformation. Child’s Nerv. Syst. 2014, 30, 1225–1232. [Google Scholar] [CrossRef]
- Van Adrichem, L.L.N.A.; van Vlimmeren, L.L.A.; Čadanová, D.; Helders, P.J.M.; Engelbert, R.H.H.; Van Neck, H.J.W.; Koning, A.H.J. Validation of a simple method for measuring cranial deformities (plagiocephalometry). J. Craniofacial Surg. 2008, 19, 15–21. [Google Scholar] [CrossRef]
- Mortenson, P.A.; Steinbok, P. Quantifying positional plagiocephaly: Reliability and validity of anthropometric measurements. J. Craniofacial Surg. 2006, 17, 413–419. [Google Scholar] [CrossRef]
- Mulliken, J.B. Analysis of posterior plagiocephaly: Deformational versus synostotic. Plast. Reconstr. Surg. 1999, 103, 371–380. [Google Scholar] [CrossRef]
- Lee, R.P.; Teichgraeber, J.F.; Baumgartner, J.E.; Waller, A.L.; English, J.D.; Lasky, R.E.; Miller, C.C.; Gateno, J.; Xia, J.J. Long-Term Treatment Effectiveness of Molding Helmet Therapy in the Correction of Posterior Deformational Plagiocephaly: A Five-Year Follow-Up. Cleft Palate Craniofacial J. 2008, 45, 240–245. [Google Scholar] [CrossRef]
- Rogers, G.F.; Miller, J.; Mulliken, J.B. Comparison of a Modifiable Cranial Cup versus Repositioning and Cervical Stretching for the Early Correction of Deformational Posterior Plagiocephaly. Plast. Reconstr. Surg. 2008, 121, 941–947. [Google Scholar] [CrossRef]
- Wilbrand, J.-F.; Wilbrand, M.; Pons-Kuehnemann, J.; Blecher, J.-C.; Christophis, P.; Howaldt, H.-P.; Schaaf, H. Value and reliability of anthropometric measurements of cranial deformity in early childhood. J. Cranio Maxillofac. Surg. 2011, 39, 24–29. [Google Scholar] [CrossRef]
- Skolnick, G.B.; Naidoo, S.D.; Nguyen, D.C.; Patel, K.B.; Woo, A.S. Evidence for Use of Frontozygomaticus and Contralateral Eurion as Hand-Caliper Landmarks for Assessment of Deformational Plagiocephaly. J. Craniofacial Surg. 2016, 27, 1498–1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loveday, B.P.T.; de Chalain, T.B. Active counterpositioning or orthotic device to treat positional plagiocephaly? J. Craniofacial Surg. 2001, 12, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Kluba, S.; Kraut, W.; Reinert, S.; Krimmel, M. What is the optimal time to start helmet therapy in positional plagiocephaly? Plast. Reconstr. Surg. 2011, 128, 492–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilbrand, J.F.; Schmidtberg, K.; Bierther, U.; Streckbein, P.; Pons-Kuehnemann, J.; Christophis, P.; Hahn, A.; Schaaf, H.; Howaldt, H.P. Clinical classification of infant nonsynostotic cranial deformity. J. Pediatr. 2012, 161, 1120–1125. [Google Scholar] [CrossRef]
- Holowka, M.A.; Reisner, A.; Giavedoni, B.; Lombardo, J.R.; Coulter, C. Plagiocephaly severity scale to aid in clinical treatment recommendations. J. Craniofacial Surg. 2017, 28, 717–722. [Google Scholar] [CrossRef]
- Steinberg, J.P.; Rawlani, R.; Humphries, L.S.; Rawlani, V.; Vicari, F.A. Effectiveness of Conservative Therapy and Helmet Therapy for Positional Cranial Deformation. Plast. Reconstr. Surg. 2015, 135, 833–842. [Google Scholar] [CrossRef]
- Kelly, K.M.; Littlefield, T.R.; Pomatto, J.K.; Ripley, C.E.; Beals, S.P.; Joganic, E.F. Importance of Early Recognition and Treatment of Deformational Plagiocephaly with Orthotic Cranioplasty. Cleft Palate Craniofacial J. 1999, 36, 127–130. [Google Scholar] [CrossRef]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Leibson, T.; Koren, G. Informed Consent in Pediatric Research. Pediatr. Drugs 2015, 17, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Cho, I.K.; Eom, J.R.; Lee, J.W.; Yang, J.D.; Chung, H.Y.; Cho, B.C.; Choi, K.Y. A Clinical Photographic Method to Evaluate the Need for Helmet Therapy in Deformational Plagiocephaly. J. Craniofacial Surg. 2018, 29, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Roosenboom, J.; Lee, M.K.; Hecht, J.T.; Heike, C.L.; Wehby, G.L.; Christensen, K.; Feingold, E.; Marazita, M.L.; Maga, A.M.; Shaffer, J.R. Mapping genetic variants for cranial vault shape in humans. PLoS ONE 2018, 13, e0196148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernet, O.; de Ribaupierre, S.; Cavin, B.; Rilliet, B. Treatment of posterior positional plagiocephaly. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2008, 15, 1829. [Google Scholar] [CrossRef] [PubMed]
- Mawji, A.; Vollman, A.R.; Hatfield, J.; McNeil, D.A.; Sauvé, R. The incidence of positional plagiocephaly: A cohort study. Pediatrics 2013, 132, 298–304. [Google Scholar] [CrossRef] [Green Version]
- Skolnick, G.B.; Naidoo, S.D.; Patel, K.B.; Woo, A.S. Analysis of Digital Measures of Cranial Vault Asymmetry for Assessment of Plagiocephaly. J. Craniofacial Surg. 2014, 25, 1178–1182. [Google Scholar] [CrossRef]
- Skolnick, G.B.; Naidoo, S.D.; Nguyen, D.C.; Patel, K.B.; Woo, A.S. Comparison of Direct and Digital Measures of Cranial Vault Asymmetry for Assessment of Plagiocephaly. J. Craniofacial Surg. 2015, 26, 1900–1903. [Google Scholar] [CrossRef]
- Mendonca, D.A.; Naidoo, S.D.; Skolnick, G.; Skladman, R.; Woo, A.S. Comparative Study of Cranial Anthropometric Measurement by Traditional Calipers to Computed Tomography and Three-dimensional Photogrammetry. J. Craniofacial Surg. 2013, 24, 1106–1110. [Google Scholar] [CrossRef]
- Purnell, C.A.; Benz, A.W.; Gosain, A.K. Assessment of Head Shape by Craniofacial Teams. J. Craniofacial Surg. 2015, 26, 1808–1811. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infants with PP (n = 62) | Descriptive | |
|---|---|---|
| Gender | Females (n = 27) | 43.5% |
| Males (n = 35) | 56.5% | |
| Age (weeks) | 16.0 (13.0; 19.0) ** | |
| CI (%) | 86.8 ± 7.4 * | |
| CVA (mm) | 8.2 (6.0; 11.6) ** | |
| CVAI (%) | 6.4 (5.0; 9.4) ** | |
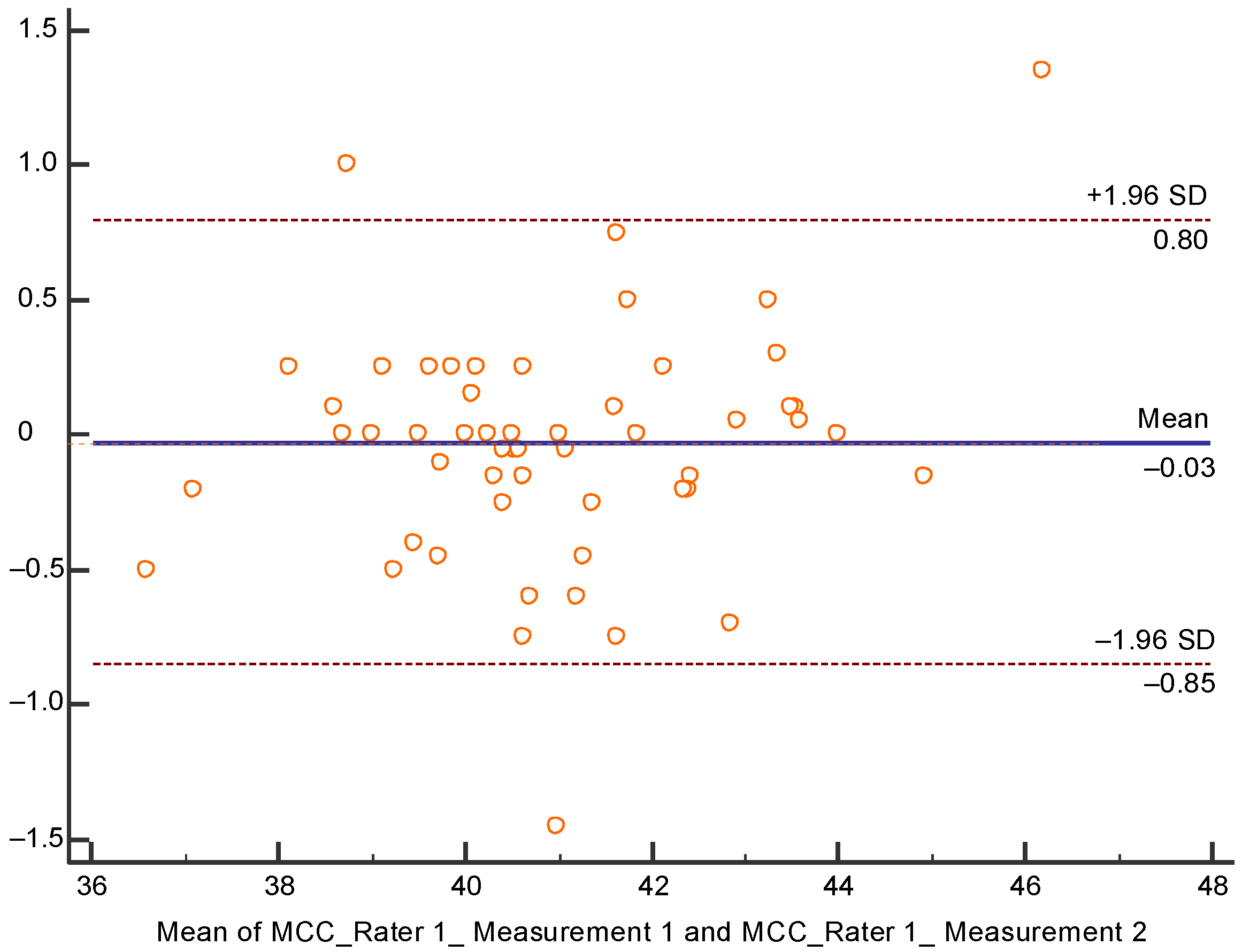
| Infants with PP (n = 62) | Rater 1 | Descriptive | Kolmogorov-Smirnov. Sig. |
|---|---|---|---|
| MCC | Measurement 1 | 40.4 (39.4; 42.0) ** | 0.016 |
| Measurement 2 | 40.8 ± 1.8 * | 0.200 |
| Infants with PP (n = 62) | Rater 1 | Descriptive | Kolmogorov-Smirnov. Sig. | ICC | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| MCL | Measurement 1 | 132.6 ± 7.5 * | 0.077 | 0.987 | 0.978 | 0.992 | 0.000 |
| Measurement 2 | 132.8 ± 7.4 * | 0.200 | |||||
| MCW | Measurement 1 | 114.8 ± 8.1 * | 0.200 | 0.977 | 0.962 | 0.986 | 0.000 |
| Measurement 2 | 115.5 ± 7.6 * | 0.200 | |||||
| Right cranial diagonal | Measurement 1 | 127.6 ± 8.2 * | 0.200 | 0.990 | 0.983 | 0.994 | 0.000 |
| Measurement 2 | 128.1 ± 7.9 * | 0.200 | |||||
| Left cranial diagonal | Measurement 1 | 130.5 ± 8.7 * | 0.200 | 0.983 | 0.972 | 0.990 | 0.000 |
| Measurement 2 | 131.1 ± 8.2 * | 0.200 | |||||
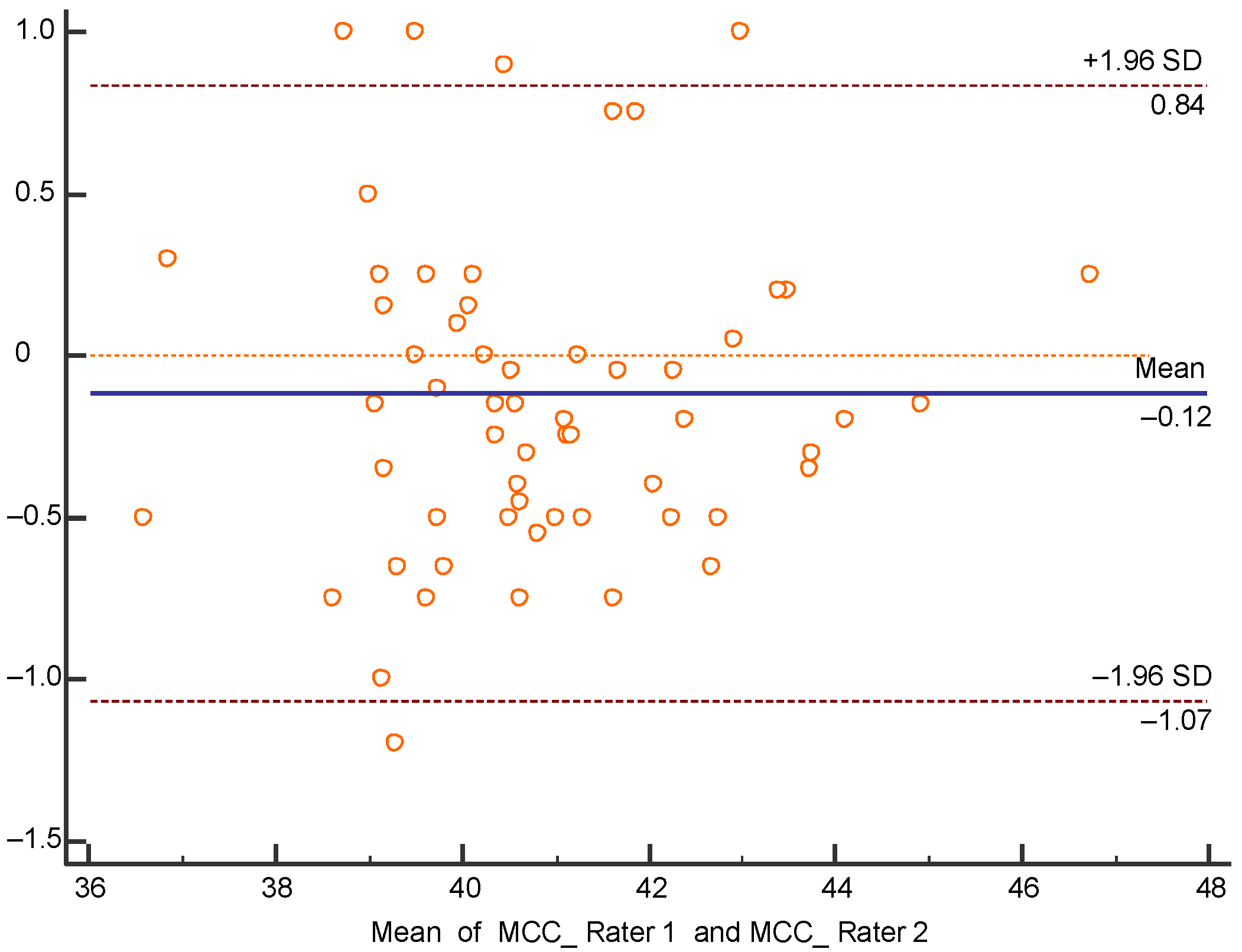
| Infants with PP (n = 62) | Raters | Descriptive | Kolmogorov-Smirnov. Sig. |
|---|---|---|---|
| MCC | Rater 1 | 40.4 (39.4; 42.0) ** | 0.016 |
| Rater 2 | 40.9 ± 1.8 * | 0.100 | |
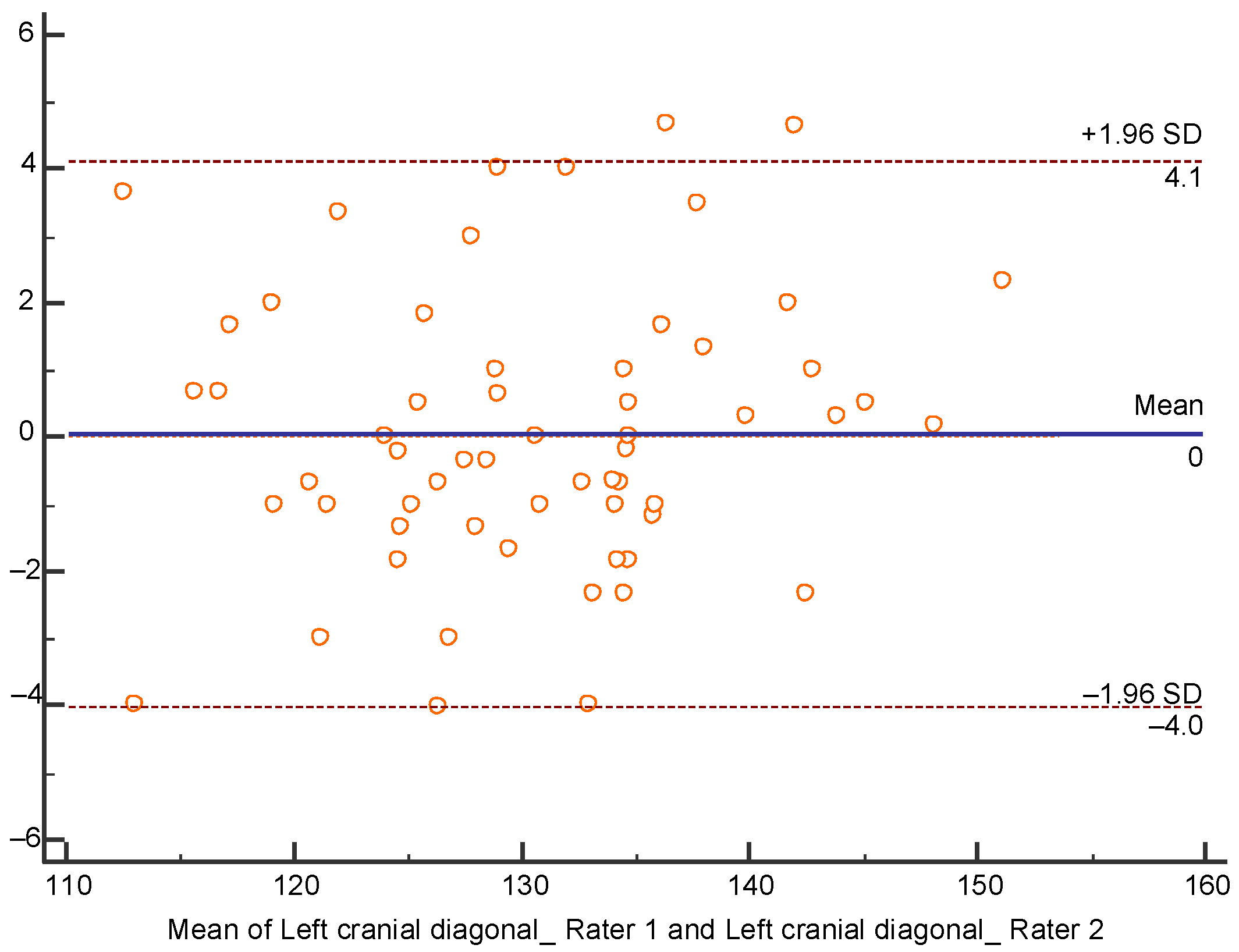
| Left cranial diagonal | Rater 1 | 130.5 ± 8.7 * | 0.200 |
| Rater 2 | 130.5 (125.1; 135.4) ** | 0.038 |
| Infants with PP (n = 62) | Raters | Descriptive | Kolmogorov-Smirnov. Sig. | ICC | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| MCL | Rater 1 | 132.6 ± 7.5 * | 0.077 | 0.983 | 0.972 | 0.990 | 0.000 |
| Rater 2 | 133.4 ± 7.0 * | 0.200 | |||||
| MCW | Rater 1 | 114.8 ± 8.1 * | 0.200 | 0.978 | 0.963 | 0.987 | 0.000 |
| Rater 2 | 116.2 ± 7.8 * | 0.200 | |||||
| Right cranial diagonal | Rater 1 | 127.6 ± 8.2 * | 0.200 | 0.986 | 0.977 | 0.992 | 0.000 |
| Rater 2 | 127.4 ± 8.2 * | 0.200 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pastor-Pons, I.; Lucha-López, M.O.; Barrau-Lalmolda, M.; Rodes-Pastor, I.; Rodríguez-Fernández, Á.L.; Hidalgo-García, C.; Tricás-Moreno, J.M. Interrater and Intrarater Reliability of Cranial Anthropometric Measurements in Infants with Positional Plagiocephaly. Children 2020, 7, 306. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120306
Pastor-Pons I, Lucha-López MO, Barrau-Lalmolda M, Rodes-Pastor I, Rodríguez-Fernández ÁL, Hidalgo-García C, Tricás-Moreno JM. Interrater and Intrarater Reliability of Cranial Anthropometric Measurements in Infants with Positional Plagiocephaly. Children. 2020; 7(12):306. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120306
Chicago/Turabian StylePastor-Pons, Iñaki, María Orosia Lucha-López, Marta Barrau-Lalmolda, Iñaki Rodes-Pastor, Ángel Luis Rodríguez-Fernández, César Hidalgo-García, and Jose Miguel Tricás-Moreno. 2020. "Interrater and Intrarater Reliability of Cranial Anthropometric Measurements in Infants with Positional Plagiocephaly" Children 7, no. 12: 306. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120306