The Transport and Outcome of Sick Outborn Neonates Admitted to a Regional and District Hospital in the Upper West Region of Ghana: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Method
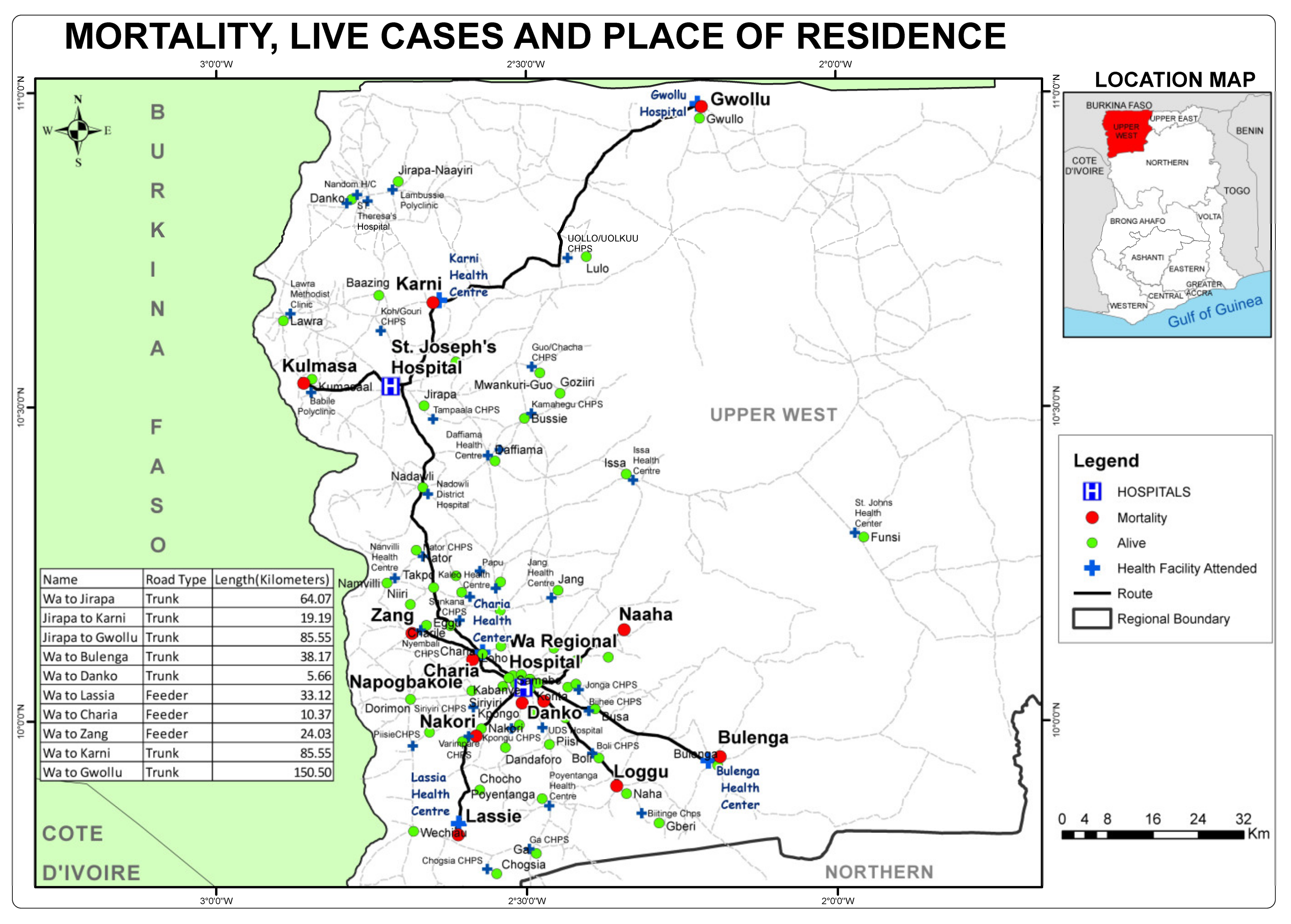
2.1. Study Location
2.2. Study Design
2.3. Sampling and Sample Size
2.4. Study Population
2.5. Data Collection
2.6. Data Analysis
2.7. Ethical Clearance
3. Results
3.1. Patient Characteristics
3.2. Distance Travelled
3.3. Mode of Transport
3.4. Travel Time
3.5. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IQR | Inter-quartile range |
| NICU | Neonatal intensive care unit |
| SD | Standard deviation |
| SDG | Sustainable development goals |
| SJH | St Joseph’s Hospital |
| UK | United Kingdom |
| UWRH | Upper West Regional Hospital |
References
- Lawn, J.E.; Cousens, S.; Zupan, J. 4 million neonatal deaths: When? Where? Why? Lancet 2005, 365, 891–900. [Google Scholar] [CrossRef]
- UNICEF, WHO, World Bank, UN-DESA Population Levels and Trends in Child Mortality: Report 2015: the UN Inter-Agency Group for Child Mortality Estimation; United Nations Children’s Fund: New York, NY, USA, 2015.
- Bhutta, Z.A.; Das, J.K.; Bahl, R.; Lawn, J.E.; Salam, R.A.; Paul, V.K.; Walker, N. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 2014, 384, 347–370. [Google Scholar] [CrossRef]
- Vesel, L.; Manu, A.; Lohela, T.J.; Gabrysch, S.; Okyere, E.; ten Asbroek, A.H.; Kirkwood, B.R. Quality of newborn care: a health facility assessment in rural Ghana using survey, vignette and surveillance data. BMJ Open 2013, 3, e002326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Standards for Improving Quality of Maternal and Newborn Care in Health Facilities; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Målqvist, M.; Sohel, N.; Do, T.T.; Eriksson, L.; Persson, L.-Å. Distance decay in delivery care utilisation associated with neonatal mortality. A case referent study in northern Vietnam. BMC Public Health 2010, 10, 762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazzano, A.N.; Kirkwood, B.R.; Tawiah-Agyemang, C.; Owusu-Agyei, S.; Adongo, P.B. Beyond symptom recognition: care-seeking for ill newborns in rural Ghana. Trop. Med. Int. Health 2008, 13, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Storrs, C.N.; Taylor, M.R. Transport of sick newborn babies. Br. Med. J. 1970, 3, 328–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nlend, A.E.N.; Zeudja, C.; Nsoa, L. Transfert et transport des nouveau-nés en situation de détresse vitale à Yaoundé, Cameroun: analyse situationnelle dans un hôpital de référence. Pan. Afr. Med. J. 2016, 25. [Google Scholar] [CrossRef]
- Niermeyer, S.; Domek, G. Neonatal transport in developing country settings: A systematic review. Pan American Health Organisation, Montevido. 2016. Available online: http://iris.paho.org/xmlui/handle/123456789/31317 (accessed on 24 February 2020).
- Okwaraji, Y.B.; Edmond, K.M. Proximity to health services and child survival in low-and middle-income countries: a systematic review and meta-analysis. BMJ Open 2012, 2, e001196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeps, A.; Gabrysch, S.; Niamba, L.; Sié, A.; Becher, H. The effect of distance to health-care facilities on childhood mortality in rural Burkina Faso. Am. J. Epidemiol. 2011, 173, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Karra, M.; Fink, G.; Canning, D. Facility distance and child mortality: A multi-country study of health facility access, service utilization, and child health outcomes. Int. J. Epidemiol. 2017, 46, 817–826. [Google Scholar] [CrossRef] [Green Version]
- King, G.; Zeng, L. Logistic regression in rare events data. Political Analysis. Polit Anal. 2001, 9, 137–163. [Google Scholar] [CrossRef] [Green Version]
- Cornette, L. Contemporary neonatal transport: problems and solutions. Arch. Dis. Childhood Fetal Neonatal Ed. 2004, 89, F212–F214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.S. Regionalization of neonatal intensive care in Korea. Korean J. Pediatr. 2011, 54, 481–488. [Google Scholar] [CrossRef] [Green Version]
- Rathod, D.; Adhisivam, B.; Bhat, B.V. Transport of sick neonates to a tertiary care hospital, south India: condition at arrival and outcome. Trop Doct. 2015, 45, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Nalwadda, C.K.; Waiswa, P.; Kiguli, J.; Namazzi, G.; Namutamba, S.; Tomson, G.; Guwatudde, D. High Compliance with Newborn Community-to-Facility Referral in Eastern Uganda: An Opportunity to Improve Newborn Survival. PLoS ONE 2013, 8, e81610. [Google Scholar] [CrossRef] [Green Version]
- Kozuki, N.; Guenther, T.; Vaz, L.; Moran, A.; Soofi, S.B.; Kayemba, C.N.; Doherty, T. A systematic review of community-to-facility neonatal referral completion rates in Africa and Asia. BMC Public Health 2015, 15, 989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, M.P.; Gupta, R.; Sehgal, R. Neonatal transport in India: From public health perspective. Med J. Dr DY Patil Univ. 2016, 9, 566. [Google Scholar] [CrossRef]
- Hedstrom, A.; Ryman, T.; Otai, C.; Nyonyintono, J.; McAdams, R.M.; Lester, D.; Batra, M. Demographics, clinical characteristics and neonatal outcomes in a rural Ugandan NICU. BMC Pregnancy Childbirth 2014, 14, 327. [Google Scholar] [CrossRef] [Green Version]
- Elwan, A. Mortality Among Outborn Versus Inborn Neonates: A Retrospective Comparative Study. Med. J. Cairo Univ. 2009, 77, 209–217. [Google Scholar]
- Ghana Statistical Service. 2010 Population & Housing Census: National Analytical Report; Ghana Statistical Service: Accra, Ghana, 2013. [Google Scholar]
- Ghana Health Service. Upper West Region—Upper West Regional Directorate. Upper West Region. 2019. Available online: http://www.ghanahealthservice.org/rhdcategory.php?ghsrid=3&cid=39 (accessed on 16 February 2019).
- Fleming, S.; Thompson, M.; Stevens, R.; Heneghan, C.; Plüddemann, A.; Maconochie, I.; Mant, D. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet 2011, 377, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Thermal Control of the Newborn: A Practical Guide; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Mears, M.; Chalmers, S. Neonatal pre-transport stabilisation–caring for infants the STABLE way. Infant 2005, 1, 34–37. [Google Scholar]
- Lee, K.-S. Neonatal transport metrics and quality improvement in a regional transport service. Transl. Pediatr. 2019, 8, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, K.C.; Gupta, R.; Sharma, S.; Sehgal, R.; Roy, M.P. Mortality in newborns referred to tertiary hospital: An introspection. J. Family Med. Prim. Care 2015, 4, 435–438. [Google Scholar] [PubMed]
- Abdulraheem, M.A.; Tongo, O.O.; Orimadegun, A.E.; Akinbami, O.F. Neonatal transport practices in Ibadan, Nigeria. Pan Afr. Med J. 2016, 24. [Google Scholar] [CrossRef] [PubMed]
- Baidya, M.; Shirin, M.; Saha, L.C. Transport Factors Affecting the Outcome of Referred Neonates Admitted in A Tertiary Care Hospital. Bangladesh J. Child Health 2017, 41, 159–164. [Google Scholar] [CrossRef]
- Dey, S.K.; Sharker, S.; Jahan, I.; Moni, S.C.; Shabuj, K.H.; Chisti, M.J.; Shahidullah, M. Neonatal Transport—Experience of a Tertiary Care Hospital of Bangladesh. Mymensingh Med. J. 2017, 26, 169–174. [Google Scholar] [PubMed]
- Whyte, H.E.; Jefferies, A.L. The interfacility transport of critically ill newborns. None 2015, 20, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Nimbalkar, S.; Patel, H.; Dongara, A.; Patel, D.V.; Bansal, S. Usage of EMBRACETM in Gujarat, India: Survey of Paediatricians. Adv. Prev. Med. 2014. [Google Scholar] [CrossRef] [Green Version]
- Agourram, B.; Bach, V.; Tourneux, P.; Krim, G.; Delanaud, S.; Libert, J.-P. Why wrapping premature neonates to prevent hypothermia can predispose to overheating. J. Appl. Physiol. 2010, 108, 1674–1681. [Google Scholar] [CrossRef] [Green Version]
- Bowman, E.D.; Roy, R.N.D. Control of temperature during newborn transport: an old problem with new difficulties. J. Paediatr. Child Health 1997, 33, 398–401. [Google Scholar] [CrossRef]
- Advanced Life Support Group (ALSG). Advanced Paediatric Life Support: The Practical Approach, 5th ed.; BMJ Books: London, UK, 2011. [Google Scholar]
- Dawson, J.A.; Kamlin, C.O.F.; Wong, C.; Te Pas, A.B.; Vento, M.; Cole, T.J.; Morley, C.J. Changes in heart rate in the first minutes after birth. Arch. Dis. Childhood Fetal Neonatal Ed. 2010, 95, F177–F181. [Google Scholar] [CrossRef] [PubMed]
- Chong, S.L.; Ong, G.Y.K.; Chin, W.Y.W.; Chua, J.M.; Nair, P.; Ong, A.S.Z.; Maconochie, I. A retrospective review of vital signs and clinical outcomes of febrile infants younger than 3 months old presenting to the emergency department. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, M.P.; Lake, D.E.; O’Shea, T.M.; Moorman, J.R. Heart rate characteristics and clinical signs in neonatal sepsis. Pediatric Res. 2007, 61, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Henry, S.; Trotman, H. Challenges in neonatal transport in Jamaica: A resource-limited setting. J. Trop. Pediatrics 2017, 63, 307–313. [Google Scholar]
- Narli, N.; Kırımi, E.; Uslu, S. Turkish Neonatal Society guideline on the safe transport of newborn. Turk Pediatri Ars. 2018, 25, S18–S31. [Google Scholar] [CrossRef] [PubMed]
- Jajoo, M.; Kumar, D.; Dabas, V.; Mohta, A. Neonatal transport: The long drive has not even begun. Indian J. Community Med. 2017, 42, 244. [Google Scholar] [CrossRef] [PubMed]
- Ashokcoomar, P.; Naidoo, R. An analysis of inter-healthcare facility transfer of neonates within the eThekwini Health District of KwaZulu-Natal, South Africa. South Afr. Med J. 2016, 106, 514–518. [Google Scholar] [CrossRef]
- Punitha, P.; Kumaravel, K.S.; Pugalendhiraja, K.V. A Study on The Current Status of Neonatal Transport to A Special Newborn Care Unit. Stanley Med J. 2016, 3, 55–58. [Google Scholar]
- Sumankuuro, J.; Crockett, J.; Wang, S. Perceived barriers to maternal and newborn health services delivery: a qualitative study of health workers and community members in low and middle-income settings. BMJ Open 2018, 8, e021223. [Google Scholar] [CrossRef]
- Tette, E.; Nuertey, B.D.; Azusong, E.A.; Gandau, N.B. The Profile, Health Seeking Behavior, Referral Patterns, and Outcome of Outborn Neonates Admitted to a District and Regional Hospital in the Upper West Region of Ghana: A Cross-Sectional Study. Children 2020, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narang, M.; Kaushik, J.S.; Sharma, A.K.; Faridi, M.M.A. Predictors of mortality among the neonates transported to referral centre in Delhi, India. Indian J. Public Health 2013, 57, 100. [Google Scholar] [CrossRef] [PubMed]
- Arul, G.S.; Spicer, R.D. Where should paediatric surgery be performed? Archives Dis. Child. 1998, 79, 65–72. [Google Scholar] [CrossRef]
- El Hasbaoui, B.; Karboubi, L.; Benjelloun, B.S. Newborn haemorrhagic disorders: About 30 cases. Pan Afr. Med. J. 2017, 28, 123. [Google Scholar] [CrossRef]
- Kumar, P.P.; Kumar, C.D.; Shaik, F.A.; Ghanta, S.B.; Venkatalakshmi, A. Prolonged neonatal interhospital transport on road: relevance for developing countries. Indian J. Pediatrics 2010, 77, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Britto, J.; Nadel, S.; Maconochie, I.; Levin, M.; Habibi, P. Morbidity and severity of illness during interhospital transfer: impact of a specialised paediatric retrieval team. BMJ 1995, 311, 836–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Droogh, J.M.; Smit, M.; Absalom, A.R.; Ligtenberg, J.J.; Zijlstra, J.G. Transferring the critically ill patient: are we there yet? Critical Care 2015, 19, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Accorsi, S.; Somigliana, E.; Solomon, H.; Ademe, T.; Woldegebriel, J.; Almaz, B.; Seifu, A. Cost-effectiveness of an ambulance-based referral system for emergency obstetrical and neonatal care in rural Ethiopia. BMC Pregnancy Childbirth 2017, 17, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghana Health Service. Ghana National Newborn Health Strategy and Action Plan 2019-2023; Ghana Health Service: Accra, Ghana, 2019.
- Stroud, M.H.; Trautman, M.S.; Meyer, K.; Moss, M.M.; Schwartz, H.P.; Bigham, M.T.; Meyer, M.T. Pediatric and neonatal interfacility transport: results from a national consensus conference. Pediatrics 2013, 132, 359–366. [Google Scholar] [CrossRef] [Green Version]
- Tette, E.M.; Neizer, M.; Nyarko, M.Y.; Sifah, E.K.; Nartey, E.T.; Donkor, E.S. Changing patterns of disease and mortality at the Children’s Hospital, Accra: are infections rising? PLoS ONE 2016, 11, e0150387. [Google Scholar] [CrossRef] [Green Version]
- Awoonor-Williams, J.K.; Bailey, P.E.; Yeji, F.; Adongo, A.E.; Baffoe, P.; Williams, A.; Mercer, S. Conducting an audit to improve the facilitation of emergency maternal and newborn referral in northern Ghana. Global Public Health 2015, 10, 1118–1133. [Google Scholar] [CrossRef]
- Grimes, D.A.; Schulz, K.F. Descriptive studies: what they can and cannot do. Lancet 2002, 359, 145–149. [Google Scholar] [CrossRef]
- Aggarwal, R.; Ranganathan, P. Study designs: Part 2—Descriptive studies. Perspect. Clin. Res. 2019, 10, 34–36. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Characteristics | Outcome | ||
|---|---|---|---|
| Survived | Died | ||
| n (%) | n (%) | χ2 (p-value) | |
| All participants | 141 (92.2) | 12 (7.8) | |
| Sex of neonate | |||
| Female | 56 (39.7) | 9 (75.0) | 5.634 (0.018) |
| Male | 85 (60.3) | 3 (25.0) | |
| Birth weight in grams | |||
| <2500 g | 15 (10.6) | 6 (50.0) | 14.468 (0.001) |
| ≥2500 g | 126 (89.4) | 6 (50.0) | |
| Gestational age at birth | |||
| <37 completed weeks | 20 (14.2) | 6 (50.0) | 10.057 (0.002) |
| ≥37 completed weeks | 121 (85.8) | 6 (50.5) | |
| Mother in attendance at NICU | |||
| Mother in attendance | 134 (95.0) | 11 (91.7) | 0.253 (0.615) |
| Mother did not attend * | 7 (5.0) | 1 (8.3) | |
| Accompanied to NICU by | |||
| child’s father | 66 (57.4) | 2 (22.2) | 5.721 (0.221) |
| Other family member | 34 (29.6) | 6 (66.7) | |
| Friend | 13 (11.3.) | 1 (11.1) | |
| Not indicated | 2 (1.7) | - | |
| Time from onset of symptoms to arrival at hospital | |||
| Within 24 h | 37 (26.2) | 2 (16.7) | 0.534 (0.465) |
| More than 24 h | 104 (73.8) | 10 (83.3) | |
| Survived | Died | |
|---|---|---|
| Transport Characteristics | N = 141 | N = 12 |
| n (%) | n (%) | |
| Mode of Transport | ||
| Walked | 6 (4.3) | 2 (16.7) |
| Taxi | 50 (36.0) | 2 (16.7) |
| Public transport (Bus) | 40 (28.8) | 5 (41.7) |
| Motor bike | 39 (28.1) | 2 (16.7) |
| Motor king (Tricycle) | 2 (1.4) | 1 (8.3) |
| Ambulance | 1 (0.7) | - |
| * Unspecified | 2 (1.4) | - |
| Self-reported experienced delay in reaching NICU | ||
| Yes | 29 (20.9) | 2 (16.7) |
| No | 110 (79.1) | 10 (83.3) |
| Sources of delay among those reporting delay | ||
| Bad road | 19 (54.3) | |
| No available vehicle | 8 (22.9) | 2 (100.0) |
| The place was far | 1 (2.9) | |
| Financial problem | 5 (14.3) | |
| Other | 2 (5.7) | |
| Time taken to be seen by doctor on arrival | ||
| Less than 30 min | 35 (24.8) | 7 (58.3) |
| 30–60 min | 101 (71.6) | 5 (41.6) |
| More than 60 min | 5 (3.5) | - |
| Outcome | |||
|---|---|---|---|
| Survived | Died | ||
| Clinical Characteristics | N = 141 | N = 12 | |
| n, % | n, % | ||
| Temperature ranges (°C) | |||
| Moderate to severe hypothermia | 34.0–35.5 | 18 (12.8) | 2 (16.7) |
| Mild hypothermia | 35.6–36.4 | 49 (34.8) | 6 (50.0) |
| Normal | 36.5–37.5 | 15 (10.6) | 3 (25.0) |
| High (low grade to moderate fever) | 37.6–38.4 | 45 (31.9) | 1 (8.3) |
| High (moderate fever to hyperpyrexia) | ≥38.5 | 14 (9.9) | - |
| Heart rate (beats per min) | |||
| Low | <110 | 36 (25.5) | 5 (41.7) |
| Normal | 111–160 | 99 (70.2) | 5 (41.7) |
| High | >160 | 6 (4.3) | 2 (16.7) |
| Respiratory rate (breaths/min) | |||
| Low | <30 | 10 (7.1) | - |
| Normal | 30–60 | 51 (36.4) | 6 (50.0) |
| High | >60 | 79 (56.4) | 6 (50.0) |
| General condition | |||
| Stable | 35 (24.8) | 1 (8.3) | |
| * Unstable | 106 (75.2) | 11 (91.7) | |
| Main diagnosis | |||
| ** Neonatal sepsis | 26 (17.0) | 2 (1.3) | |
| Asphyxia | 14 (9.1) | 2 (1.3) | |
| *** Malaria | 13 (8.5) | ||
| Neonatal jaundice | 13 (8.5) | ||
| Congenital malformation **** | 13 (8.5) | ||
| Abdominal distension | 11 (7.2) | 1 (0.7) | |
| Prematurity | 9 (5.9) | 3 (1.9) | |
| Impetigo | 9 (5.9) | ||
| Circumcision bleeding | 8 (5.2) | 1 (0.7) | |
| Ophthalmia neonatorum | 8 (5.2) | ||
| Pneumonia | 5 (3.2) | ||
| Low birth weight | 4 (2.6) | 2 (1.3) | |
| Birth injury | 3 (1.9) | ||
| Gastroenteritis | 3 (1.9) | ||
| Meconium aspiration | 3 (1.9) | 1 (0.7) | |
| Other ***** | 11 (7.5) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tette, E.M.A.; Nuertey, B.D.; Akaateba, D.; Gandau, N.B. The Transport and Outcome of Sick Outborn Neonates Admitted to a Regional and District Hospital in the Upper West Region of Ghana: A Cross-Sectional Study. Children 2020, 7, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/children7030022
Tette EMA, Nuertey BD, Akaateba D, Gandau NB. The Transport and Outcome of Sick Outborn Neonates Admitted to a Regional and District Hospital in the Upper West Region of Ghana: A Cross-Sectional Study. Children. 2020; 7(3):22. https://0-doi-org.brum.beds.ac.uk/10.3390/children7030022
Chicago/Turabian StyleTette, Edem M. A., Benjamin D. Nuertey, Dominic Akaateba, and Naa Barnabas Gandau. 2020. "The Transport and Outcome of Sick Outborn Neonates Admitted to a Regional and District Hospital in the Upper West Region of Ghana: A Cross-Sectional Study" Children 7, no. 3: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/children7030022