Grief and Bereavement in Parents After the Death of a Child in Low- and Middle-Income Countries

 ,
,
Abstract
:1. Introduction
2. Methods
3. Current State of Bereavement Research in High-Income Countries
3.1. Definitions
3.2. Parental adverse effects
3.3. Supportive interventions
3.4. Health-Related Grief and Bereavement in LMICs
3.5. Perinatal Death
3.6. Infant Mortality
3.7. Infectious Disease
3.8. Interventions
3.9. Provider Comfort and Perceived Need
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- 2014 World Population Data Sheet; Population Reference Bureau: Washington, DC, USA, 2014; Available online: http://www.prb.org/pdf14/2014-world-population-data-sheet_eng.pdf (accessed on 1 February 2020).
- Knaul, F.M.; Farmer, P.E.; Krakauer, E.L.; De Lima, L.; Bhadelia, A.; Jiang Kwete, X.; Arreola-Ornelas, H.; Gómez-Dantés, O.; Rodriguez, N.M.; Alleyne, G.A.O.; et al. Alleviating the access abyss in palliative care and pain relief—An imperative of universal health coverage: The Lancet Commission report. Lancet 2018, 391, 1391–1454. [Google Scholar] [CrossRef]
- Integrating Palliative Care and Symptom Relief into Paediatrics: A WHO Guide for Health-Care Planners, Implementers and Managers; World Health Organization: Geneva, Switzerland, 2018; Licence: CC BY-NC-SA 3.0 IGO.
- Levine, D.; Lam, C.G.; Cunningham, M.J.; Remke, S.; Chrastek, J.; Klick, J.; Macauley, R.; Baker, J.N. Best practices for pediatric palliative cancer care: A primer for clinical providers. J. Support. Oncol. 2013, 32, 114–125. [Google Scholar] [CrossRef]
- Weaver, M.; Carter, B.; Keefer, P.; Korones, D.N.; Miller, E.G. Essentials: Pediatric Palliative Care and Hospice; American Academy of Hospice and Palliative Medicine: Chicago, IL, USA, 2017. [Google Scholar]
- Resolution WHA67.19. Strengthening of palliative care as a component of comprehensive care throughout the life course. In Proceedings of the Sixty-seventh World Health Assembly, Geneva, Switzerland, 19–24 May 2014; Available online: http://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_R19-en.pdf (accessed on 1 February 2020).
- Knapp, C.; Woodworth, L.; Wright, M.; Downing, J.; Drake, R.; Fowler-Kerry, S.; Hain, R.; Marston, J. Paediatric palliative care provision around the world: A systematic review. Pediatr. Blood Cancer 2011, 57, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Connor, S.R.; Sepulveda Bermedo, M.C. Global Atlas of Palliative Care at the End of Life; Worldwide Palliative Care Alliance: London, UK, 2014. [Google Scholar]
- Caruso Brown, A.E.; Howard, S.C.; Baker, J.N.; Ribeiro, R.C.; Lam, C.G. Reported availability and gaps of paediatric palliative care in low- and middle-income countries: A systematic review of published data. J. Pall. Med. 2014, 17, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downing, J.; Powell, R.A.; Marston, J.; Huwa, C.; Chandra, L.; Garchakova, A.; Harding, R. Children’s palliative care in low-and middle-income countries. Arch. Dis. Child. 2015, 101, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Friedrichsdorf, S.J.; Remke, S.; Hauser, J.; Foster, L.; Postier, A.; Kolste, A.; Wolfe, J. Development of a Pediatric Palliative Care Curriculum and Dissemination Model: Education in Palliative and End-of-Life Care (EPEC) Pediatrics. J. Pain Symptom Manag. 2019, 58, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.; Barnes, A.; Gardiner, C. Reframing Global Palliative Care Advocacy for the Sustainable Development Goal Era: A Qualitative Study of the Views of International Palliative Care Experts. J. Pain Symptom Manag. 2018, 56, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Delgado, E.; Barfield, R.C.; Baker, J.N.; Hinds, P.S.; Yang, J.; Nambayan, A.; Quintana, Y.; Kane, J.R. Availability of palliative care services for children with cancer in economically diverse regions of the world. Eur. J. Cancer 2010, 46, 2260–2266. [Google Scholar] [CrossRef] [Green Version]
- Hollander, T. Ambiguous Loss and Complicated Grief: Understanding the Grief of Parents of the Disappeared in Northern Uganda. J. Fam. Theory Rev. 2016, 8, 294–307. [Google Scholar] [CrossRef]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing narrative literature reviews for 43 peer-reviewed journals: Secrets of the trade. J. Chiropr. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Stroebe, M.S.; Hansson, R.O.; Schut, H.; Stroebe, W. Handbook of Bereavement Research and Practice: Advances in Theory and Intervention; American Psychological Association: Washington, DC, USA, 2008. [Google Scholar]
- Bonanno, G.A.; Kaltman, S. The varieties of grief experience. Clin. Psychol. Rev. 2001, 21, 705–734. [Google Scholar] [CrossRef]
- Maciejewski, P.K.; Zhang, B.; Block, S.D.; Prigerson, H.G. An empirical examination of the stage theory of grief. JAMA 2007, 297, 716–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, C.M. A comparison of adult bereavement in the death of a spouse, child and parent. Omega 1980, 10, 303–322. [Google Scholar] [CrossRef]
- Kreicbergs, U.; Valdimarsdóttir, U.; Onelöv, E.; Henter, J.L.; Steineck, G. Talking about death with children who have severe malignant disease. New Engl. J. Med. 2004, 351, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Kreicbergs, U.; Lannen, P.; Onelov, E.; Wolfe, J. Parental grief after losing a child to cancer: Impact of professional and social support on long-term outcomes. J. Clin. Oncol. 2007, 25, 3307–3312. [Google Scholar] [CrossRef]
- Li, J.; Laursen, T.M.; Precht, D.H.; Olsen, J.; Mortensen, P.B. Hospitalization for mental illness among parents after the death of a child. N. Engl. J. Med. 2005, 352, 1190–1196. [Google Scholar] [CrossRef]
- Murphy, S.A.; Johnson, L.C.; Wu, L.; Fan, J.J.; Lohan, J. Bereaved parents’ outcomes 4 to 60 months after their children’s deaths by accident, suicide, or homicide: A comparative study demonstrating differences. Death Stud. 2003, 27, 39–61. [Google Scholar] [CrossRef]
- Rodgers, C.H.; Floyd, F.J.; Seltzer, M.M.; Greenberg, J.; Hong, J. Long-term effects of the death of a child on parents’ adjustment in midlife. J. Fam. Psychol. 2008, 22, 203–211. [Google Scholar] [CrossRef]
- Barrera, M.; O’Connor, K.; D’Agostino, N.M.; Spencer, L.; Nicholas, D.; Jovcevska, V.; Tallet, S.; Schneiderman, G. Early parental adjustment and bereavement after childhood cancer death. Death Stud. 2009, 33, 497–520. [Google Scholar] [CrossRef]
- Bergstraesser, E.; Inglin, S.; Hornung, R.; Landolt, M.A. Dyadic Coping of Parents After the Death of a Child. Death Stud. 2015, 39, 128–138. [Google Scholar] [CrossRef]
- Song, J.; Floyd, F.J.; Seltzer, M.M.; Greenberg, J.S.; Hong, J. Long-term effects of child death on parents’ health-related quality of life: A dyadic analysis. Fam. Relat. 2010, 59, 269–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youngblut, J.M.; Brooten, D.; Cantwell, G.P.; del Moral, T.; Totapally, B. Parent health and functioning 13 months after infant or child NICU/PICU death. Pediatrics 2013, 132, e1295–e1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Hansen, D.; Mortensen, P.B.; Olsen, J. Myocardial infarction in parents who lost a child: A nationwide prospective cohort study in Denmark. Circulation 2002, 106, 1634–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Precht, D.H.; Mortensen, P.B.; Olsen, J. Mortality in parents after death of a child in Denmark: A nationwide follow-up study. Lancet 2003, 361, 363–367. [Google Scholar] [CrossRef]
- Forte, A.L.; Hill, M.; Pazder, R.; Feudtner, C. Bereavement care interventions: A systematic review. BMC Palliat. Care 2004, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Endo, K.; Yonemoto, N.; Yamada, M. Interventions for bereaved parents following a child’s death: A systematic review. Palliat. Med. 2015, 29, 590–604. [Google Scholar] [CrossRef]
- Ainscough, T.; Fraser, L.; Taylor, J.; Beresford, B.; Booth, A. Bereavement support effectiveness for parents of infants and children: A systematic review. BMJ Support Palliat Care 2019. E-pub ahead of print 03 October 2019. [Google Scholar] [CrossRef]
- Montgomery, L.; Owen-Pugh, V. Bereavement counselling in Uganda and Northern Ireland: A comparison. Br. J. Guid. Couns. 2017, 46, 91–103. [Google Scholar] [CrossRef]
- Papadatou, D. Childhood death and bereavement across cultures. In Death and Bereavement Across Cultures, 2nd ed.; Parkers, C., Laungani, P., Young, B., Eds.; Routledge: New York, NY, USA, 2015; pp. 151–165. [Google Scholar]
- Shakespeare, C.; Merriel, A.; Bakhbakhi, D.; Baneszova, R.; Barnard, K.; Lynch, M.; Storey, C.; Belncowe, H.; Boyle, F.; Flenady, V.; et al. Parents’ and healthcare professionals’ experiences of care after stillbirth in low- and middle-income countries: A systematic review and meta-summary. BJOG 2019, 126, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Lizcano Pabon, L.D.M.; Moreno Fergusson, M.E.; Palacios, A.M. Experience of Perinatal Death From the Father’s Perspective. Nurs. Res. 2019, 68, E1–E9. [Google Scholar] [CrossRef]
- Roberts, L.; Montgomery, S.; Ganesh, G.; Kaur, H.P.; Singh, R. Addressing Stillbirth in India Must Include Men. Issues Ment. Heal. Nurs. 2017, 38, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.C.; Opoku, C.; Gold, K.J. "They Say I Should not Think About It:": A Qualitative Study Exploring the Experience of Infant Loss for Bereaved Mothers in Kumasi, Ghana. Omega 2016, 77, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Fouts, H.N.; Silverman, L.S. Parenting and environmental risk: An examination of child loss and maternal involvement among Bofi foragers in Central Africa. Hum. Nat. 2015, 26, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.D.; Lederman, R.I.; Lichtenthal, W.G.; Morris, S.E.; Human, M.; Elliott, A.J.; Tobacco, D.; Angal, J.; Odendaal, H.; Kinney, H.C.; et al. The Grief of Mothers After the Sudden Unexpected Death of Their Infants. Pediatrics 2018, 141, e20173651. [Google Scholar] [CrossRef] [Green Version]
- Demmer, C. Experiences of women who have lost young children to AIDS in KwaZulu-Natal, South Africa: A qualitative study. J. Int. AIDS Soc. 2010, 13, 50. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, H.; Cimete, G. The effect of a grief support program on Turkish parents whose babies have died. Death Stud. 2017, 41, 602–610. [Google Scholar] [CrossRef]
- Hunt, J. The nine-cell bereavement table. Bereave. Care 2002, 21, 40–41. [Google Scholar] [CrossRef]
- Hunt, J.; Andrew, G.; Weitz, P. Improving support for bereaved people within their communities. Bereave. Care 2007, 26, 26–29. [Google Scholar] [CrossRef]
- Chan, M.F.; Lou, F.L.; Arthur, D.G. A survey comparing the attitudes toward perinatal bereavement care of nurses from three Asian cities. Eval. Heal. Prof. 2010, 33, 514–533. [Google Scholar] [CrossRef]
- Kiguli, J.; Mausoko, S.; Kerber, K.; Peterson, S.; Waiswa, P. Weeping in silence: A community experience of stillbirths in rural eastern Uganda. Glob. Heal. Action 2015, 8, 24011. [Google Scholar] [CrossRef]
- Sisay, M.M.; Yirgu, R.; Gobezayehu, A.G.; Sibley, L.M. A qualitative study of attitudes and values surrounding stillbirth and neonatal mortality among grandmothers, mothers, and unmarried girls in rural Amhara and Oromiya regions, Ethiopia: unheard souls in the backyard. J. Midwifery Women’s Heal. 2014, 59 (Suppl. 1), S110–S117. [Google Scholar] [CrossRef] [PubMed]
- Gysels, M.; Pell, C.; Straus, L.; Pool, R. End of life care in sub-Saharan Africa: A systematic review of the qualitative literature. BMC Palliat. Care 2011, 10, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mburu, G.; Oxenham, D.; Hodgson, I.; Nakiyemba, A.; Seeley, J.; Bermejo, A. Community systems strengthening for HIV care: experiences from Uganda. J. Soc. Work. End-Of-Life Palliat. Care 2013, 9, 343–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Paper | Year | Type of Paper | Countries Evaluated | Key Findings |
|---|---|---|---|---|
| Stillbirth | ||||
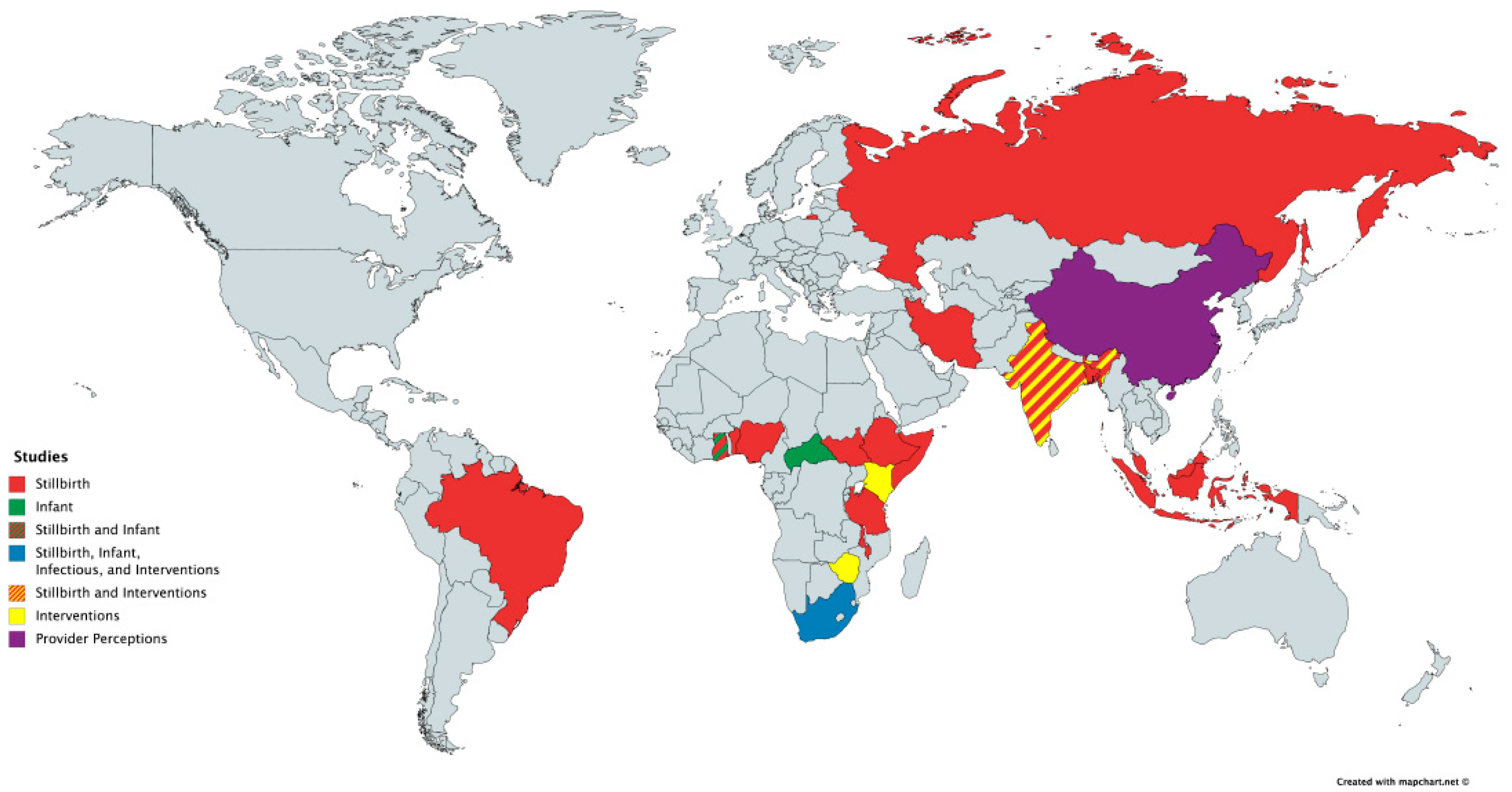
| Shakespeare et al. [36] | 2019 | Systematic Review | Bangladesh, Benin, Brazil, China, Ethiopia, Ghana, India, Indonesia, Iran, Malawi, Malaysia, Nigeria, Russia, Somalia, South Africa, Tanzania, Uganda | Common themes from the review include: positive community support, as opposed to stigmatization and blame, can improve the bereavement experience. Women’s experience of grief is often unrecognized by the healthcare community and wider society and that access to timely and culturally appropriate psychological support is valued. |
| Lizcano Pabon et al. [37] | 2019 | Qualitative Study | Columbia | Fathers often suffer alone as they focus on the suffering of their partner. They felt neglected and forgotten by the hospital staff and were not allowed in the room to support their partners or to have meaningful moments with their child. |
| Roberts et al. [38] | 2017 | Mixed Methods Study | India | Women were discouraged from grieving a stillbirth and pushed to conceive again. Men with a history of stillbirths had greater anxiety and depression and perceived less social support and were also more likely to be emotionally or physically abusive. |
| Infant | ||||
| Meyer et al. [39] | 2016 | Qualitative Study | Ghana | Mother’s were discouraged in discussing or thinking about their child after they had died. Few mothers felt that this avoidance was beneficial in their grief process. |
| Fouts and Silverman [40] | 2015 | Observational Study | Central African Republic | Those children whose mother had lost 2 children were significantly more likely to be held and have significant physical contact than those children whose mothers had lost 0 to 1 child and they were also held more as compared to those children whose mothers had lost 3 or more children. |
| Goldstein et al. [41] | 2018 | Cross-Sectional Survey | South Africa | High rates of prolonged grief disorder were not significantly different despite extremely varied and diverse cultural contexts. While culture may impact grief expression, there is an ingrained response to child loss that is maintained regardless of cultural circumstances. |
| Infectious | ||||
| Demmer et al. [42] | 2010 | Qualitative Study | South Africa | Several stressors impact a mother’s grief including remaining silent about their grief due to the fear and persistent stigma about Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS). The mothers also felt guilt for feeling like they were the cause of their child’s sickness. They struggled to find time to grieve as they faced the challenges of extreme poverty. |
| Interventions | ||||
| Yildiz et al. [43] | 2017 | Intervention study with pre- and post-test control group | Turkey | A grief support program was created for parents whose child had died. The intervention included brochures and other literature about grief and bereavement as well as interactions with a researcher at various time points. There was no difference between the control and intervention groups at 3 and 6 months. At 12 months, there was a difference that was not statistically significant. |
| Hunt 2002, Hunt et al. 2007 [44,45] | 2002, 2007 | Intervention tool development and qualitative feedback | India, Kenya, South Africa, Zimbabwe | Participants trained with this tool learned the impact that culture has in determining grief reactions and that the bereaved may behave normally but that this does not mean they are not feeling pain. |
| Provider Perceptions | ||||
| Chan et al. [46] | 2010 | Cross-Sectional Survey | China, Singapore | More senior nurses, those who had previous encounters with bereaved parents, and those that had received training on palliative care and bereavement, felt more comfortable working with bereaved families. Most of the nurses in the study agreed or strongly agreed that training in bereavement care is important. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McNeil, M.J.; Namisango, E.; Hunt, J.; Powell, R.A.; Baker, J.N. Grief and Bereavement in Parents After the Death of a Child in Low- and Middle-Income Countries. Children 2020, 7, 39. https://0-doi-org.brum.beds.ac.uk/10.3390/children7050039
McNeil MJ, Namisango E, Hunt J, Powell RA, Baker JN. Grief and Bereavement in Parents After the Death of a Child in Low- and Middle-Income Countries. Children. 2020; 7(5):39. https://0-doi-org.brum.beds.ac.uk/10.3390/children7050039
Chicago/Turabian StyleMcNeil, Michael J., Eve Namisango, Jennifer Hunt, Richard A. Powell, and Justin N. Baker. 2020. "Grief and Bereavement in Parents After the Death of a Child in Low- and Middle-Income Countries" Children 7, no. 5: 39. https://0-doi-org.brum.beds.ac.uk/10.3390/children7050039