Simple Method for the Objective Activity Type Assessment with Preschoolers, Children and Adolescents

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
2.2.1. Preschool Children
2.2.2. Children and Adolescent
2.3. Instrumentation
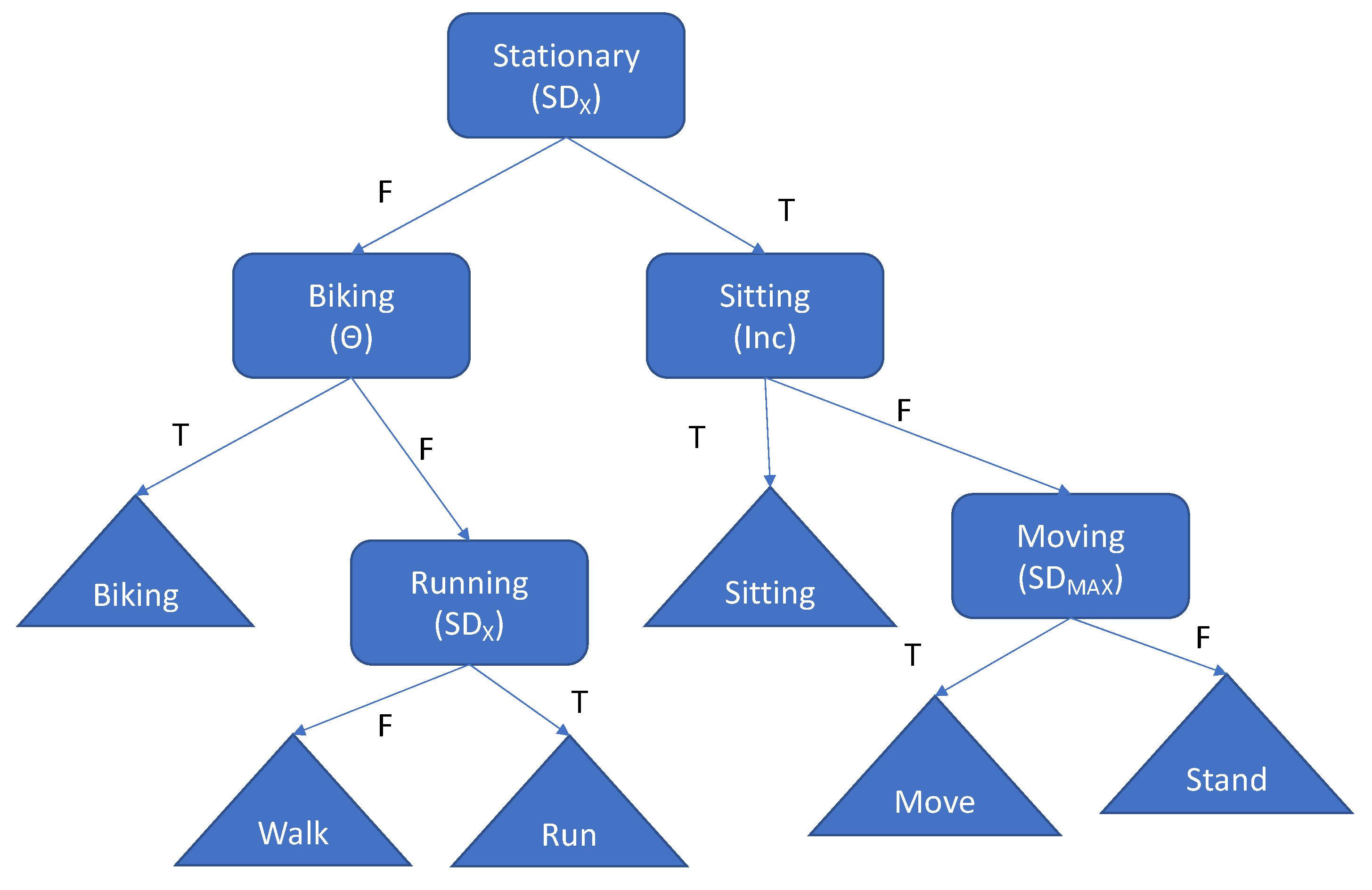
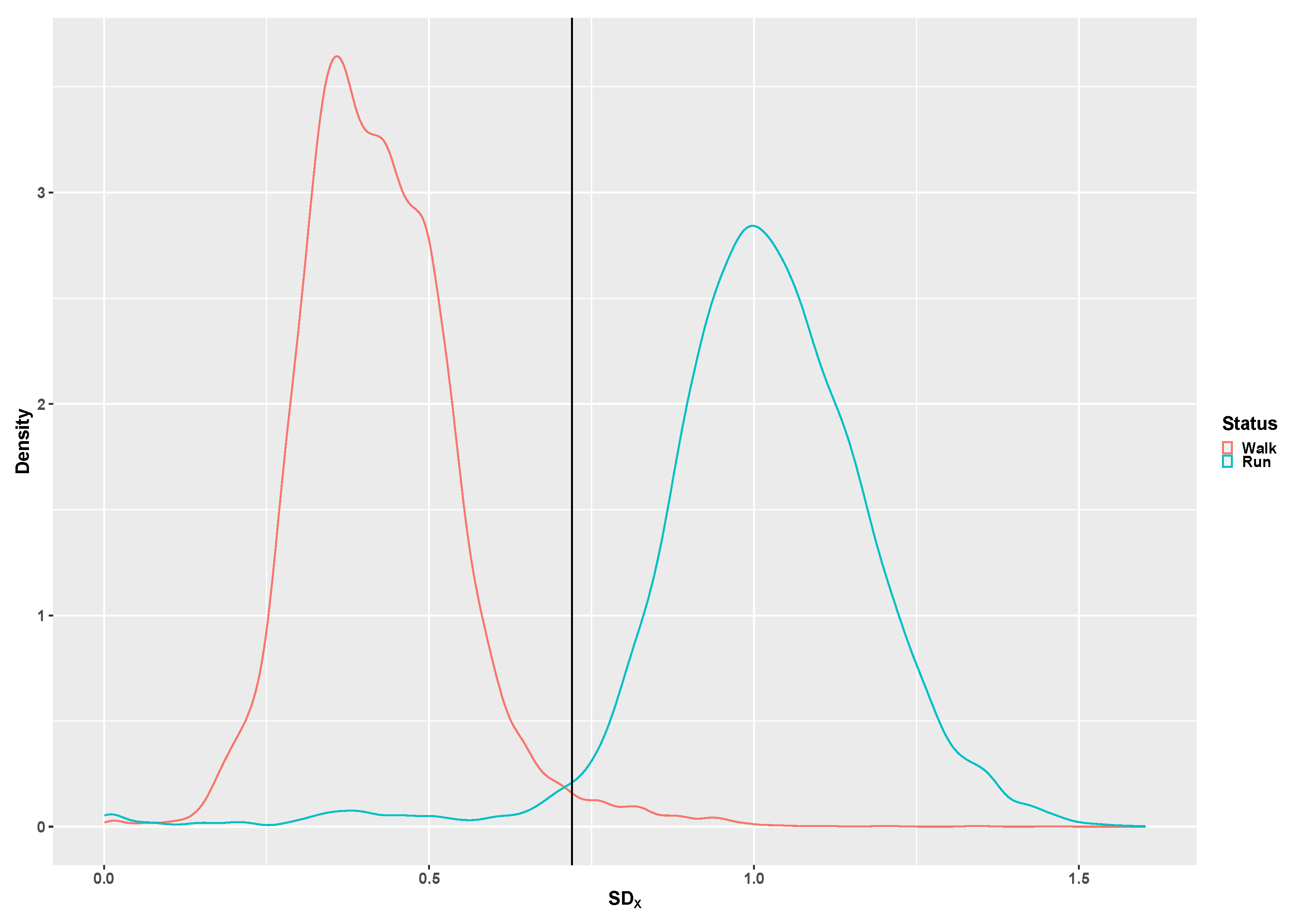
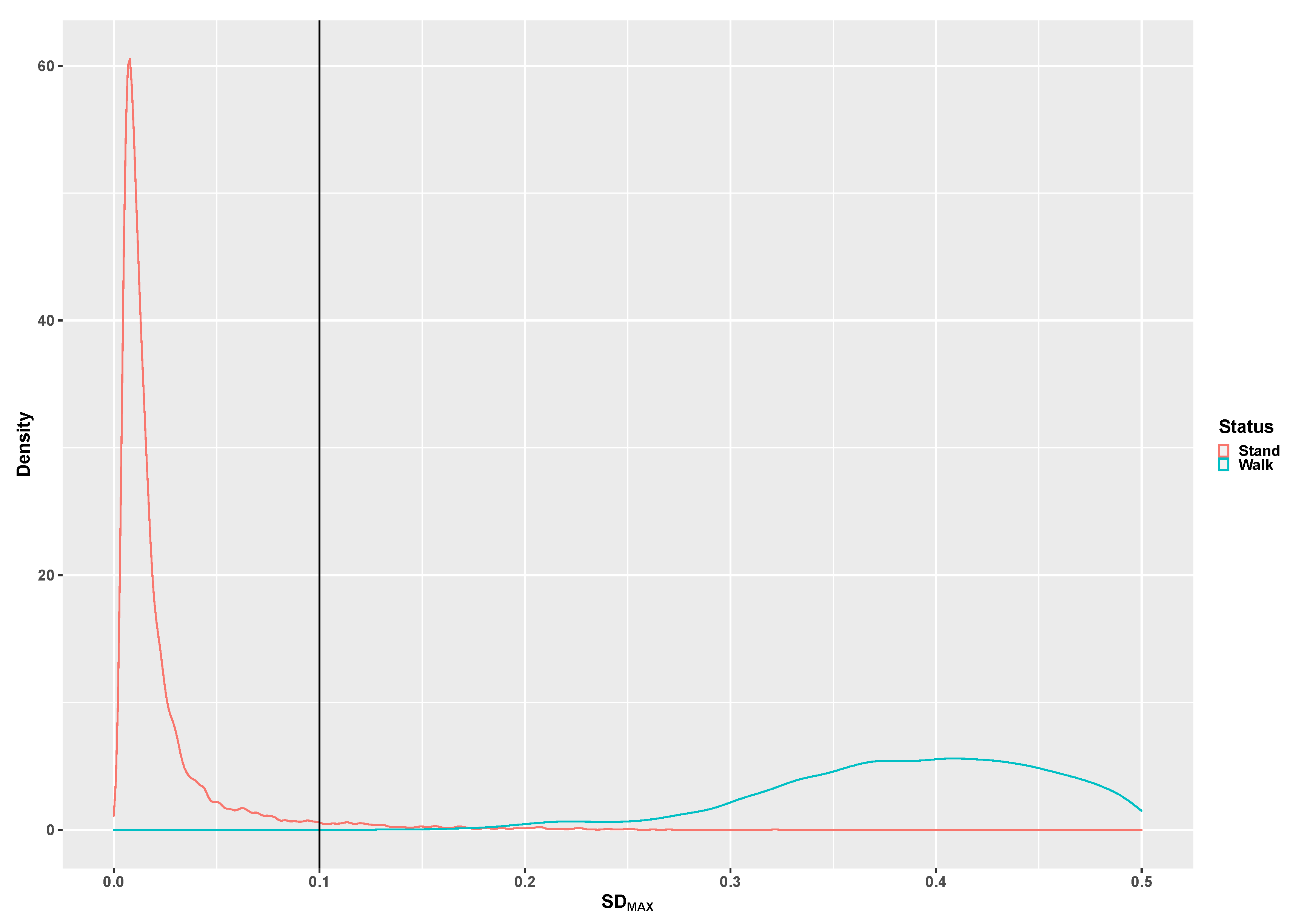
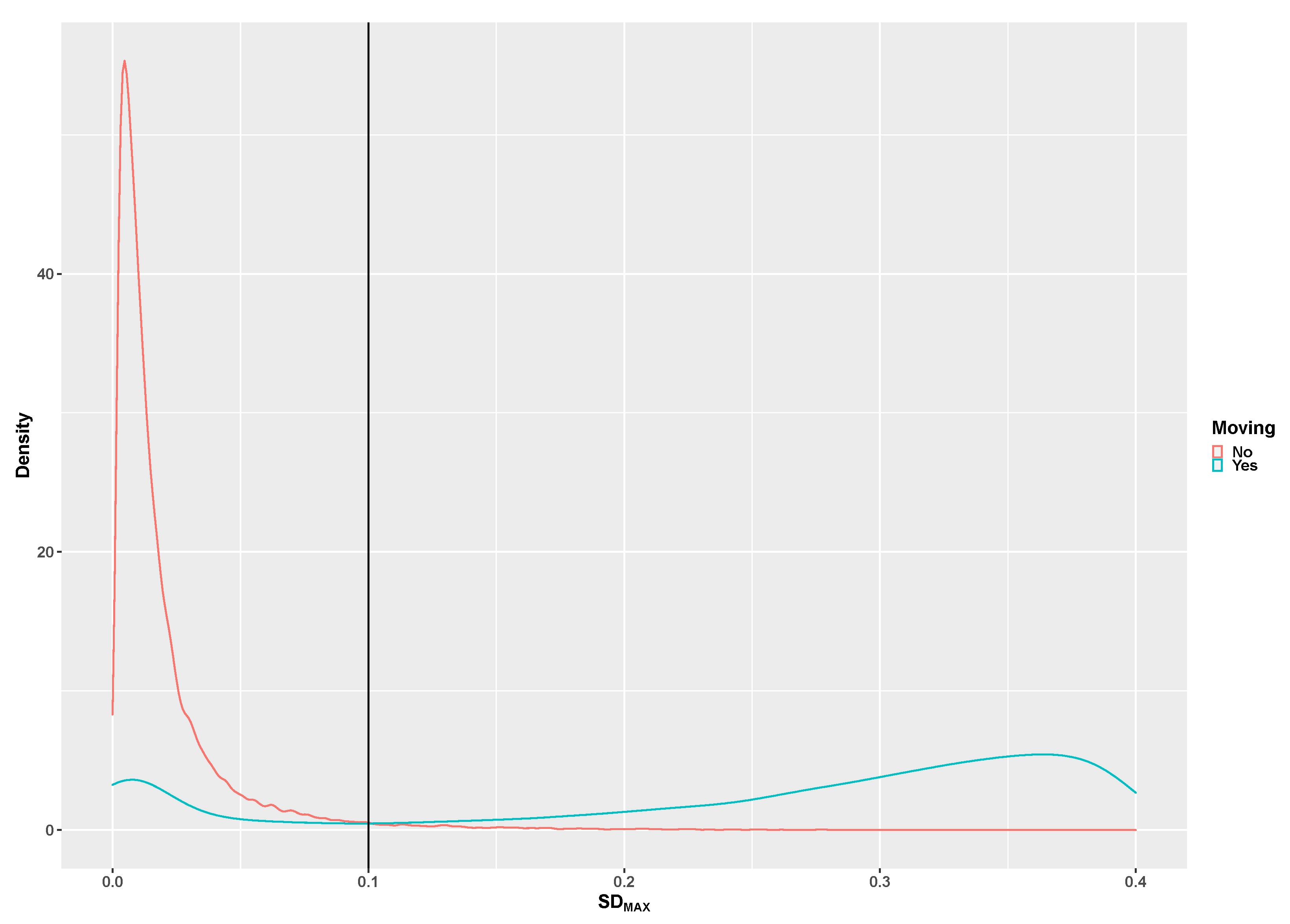
2.4. Classification Method
2.5. Statistical Considerations
3. Results
3.1. Descriptive Statistics
3.2. Algorithm Development
3.3. Algorithm Validation
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lou, D. Sedentary behaviors and youth: Current trends and the impact on health. In Proceedings of the Active Living Research, San Diego, CA, USA, January 2014. [Google Scholar]
- Panahi, S.; Tremblay, A. Sedentariness and Health: Is Sedentary Behavior More Than Just Physical Inactivity? Front. Public Health 2018, 6, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkin, A.J.; Foley, L.; Corder, K.; Ekelund, U.; van Sluijs, E.M. Determinants of Three-Year Change in Children’s Objectively Measured Sedentary Time. PLoS ONE 2016, 11, e0167826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sievanen, H.; Kujala, U.M. Accelerometry-Simple, but challenging. Scand. J. Med. Sci. Sports 2017, 27, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Sirard, J.R.; Pate, R.R. Physical activity assessment in children and adolescents. Sports Med. 2001, 31, 439–454. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of accelerometer cut points for predicting activity intensity in youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef]
- Rowlands, A.V.; Cliff, D.P.; Fairclough, S.J.; Boddy, L.M.; Olds, T.S.; Parfitt, G.; Noonan, R.J.; Downs, S.J.; Knowles, Z.R.; Beets, M.W. Moving Forward with Backward Compatibility: Translating Wrist Accelerometer Data. Med. Sci. Sports Exerc. 2016, 48, 2142–2149. [Google Scholar] [CrossRef] [Green Version]
- van Loo, C.M.; Okely, A.D.; Batterham, M.J.; Hinkley, T.; Ekelund, U.; Brage, S.; Reilly, J.J.; Trost, S.G.; Jones, R.A.; Janssen, X.; et al. Wrist Accelerometer Cut-points for Classifying Sedentary Behavior in Children. Med. Sci. Sports Exerc. 2016. [Google Scholar] [CrossRef] [Green Version]
- Hildebrand, M.; Hansen, B.H.; van Hees, V.T.; Ekelund, U. Evaluation of raw acceleration sedentary thresholds in children and adults. Scand. J. Med. Sci. Sports 2016. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Noonan, R.; Rowlands, A.V.; Van Hees, V.; Knowles, Z.; Boddy, L.M. Wear Compliance and Activity in Children Wearing Wrist- and Hip-Mounted Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 245–253. [Google Scholar] [CrossRef]
- Schneller, M.B.; Bentsen, P.; Nielsen, G.; Brond, J.C.; Ried-Larsen, M.; Mygind, E.; Schipperijn, J. Measuring Children’s Physical Activity: Compliance Using Skin-taped Accelerometers. Med. Sci. Sports Exerc. 2017. [Google Scholar] [CrossRef] [Green Version]
- Duncan, S.; Stewart, T.; Mackay, L.; Neville, J.; Narayanan, A.; Walker, C.; Berry, S.; Morton, S. Wear-Time Compliance with a Dual-Accelerometer System for Capturing 24-h Behavioural Profiles in Children and Adults. Int. J. Environ. Res. Public Health 2018, 15, 1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminian, S.; Hinckson, E.A. Examining the validity of the ActivPAL monitor in measuring posture and ambulatory movement in children. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 119. [Google Scholar] [CrossRef] [Green Version]
- Ridley, K.; Ridgers, N.D.; Salmon, J. Criterion validity of the activPAL and ActiGraph for assessing children’s sitting and standing time in a school classroom setting. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Loo, C.M.; Okely, A.D.; Batterham, M.J.; Hinkley, T.; Ekelund, U.; Brage, S.; Reilly, J.J.; Jones, R.A.; Janssen, X.; Cliff, D.P. Validation of thigh-based accelerometer estimates of postural allocation in 5-12 year-olds. J. Sci. Med. Sport 2017, 20, 273–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skotte, J.; Korshøj, M.; Kristiansen, J.; Hanisch, C.; Holtermann, A. Detection of physical activity types using triaxial accelerometers. J. Phys. Act. Health 2014, 11, 76–84. [Google Scholar] [CrossRef]
- Stewart, T.; Narayanan, A.; Hedayatrad, L.; Neville, J.; Mackay, L.; Duncan, S. A Dual-Accelerometer System for Classifying Physical Activity in Children and Adults. Med. Sci. Sports Exerc. 2018, 50, 2595–2602. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Watson, K.B.; Ridley, K.; Zakeri, I.F.; McMurray, R.; Pfeiffer, K.A.; Crouter, S.E.; Herrmann, S.D.; Bassett, D.R.; Long, A.; et al. A youth compendium of physical activities: activity codes and metabolic intensities. Med. Sci. Sports Exerc. 2018, 50, 246–256. [Google Scholar] [CrossRef]
- Jackson, D.G. OMGui Software. Available online: https://github.com/digitalinteraction/openmovement/wiki/AX3-GUI (accessed on 1 April 2020).
- Trost, S.G.; Zheng, Y.; Wong, W.K. Machine learning for activity recognition: Hip versus wrist data. Physiol. Meas. 2014, 35, 2183–2189. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Narayanan, A.; Stewart, T.; Mackay, L. A Dual-Accelerometer System for Detecting Human Movement in a Free-living Environment. Med. Sci. Sports Exerc. 2020, 52, 252–258. [Google Scholar] [CrossRef]
- Staudenmayer, J.; Pober, D.; Crouter, S.; Bassett, D.; Freedson, P. An artificial neural network to estimate physical activity energy expenditure and identify physical activity type from an accelerometer. J. Appl. Physiol. (1985) 2009, 107, 1300–1307. [Google Scholar] [CrossRef]
- Colley, R.C.; Harvey, A.; Grattan, K.P.; Adamo, K.B. Impact of accelerometer epoch length on physical activity and sedentary behaviour outcomes for preschool-aged children. Health Rep. 2014, 25, 3–9. [Google Scholar] [PubMed]
- Nettlefold, L.; Naylor, P.J.; Warburton, D.E.; Bredin, S.S.; Race, D.; McKay, H.A. The Influence of Epoch Length on Physical Activity Patterns Varies by Child’s Activity Level. Res. Q. Exerc. Sport 2016, 87, 110–123. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.C.; Olson, J.; Pepper, S.L.; Porszasz, J.; Barstow, T.J.; Cooper, D.M. The level and tempo of children’s physical activities: An observational study. Med. Sci. Sports Exerc. 1995, 27, 1033–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hees, V.T.; Sabia, S.; Jones, S.E.; Wood, A.R.; Anderson, K.N.; Kivimaki, M.; Frayling, T.M.; Pack, A.I.; Bucan, M.; Trenell, M.I.; et al. Estimating sleep parameters using an accelerometer without sleep diary. Sci. Rep. 2018, 8, 12975. [Google Scholar] [CrossRef]
- Lyden, K.; John, D.; Dall, P.; Granat, M.H. Differentiating Sitting and Lying Using a Thigh-Worn Accelerometer. Med. Sci. Sports Exerc. 2016, 48, 742–747. [Google Scholar] [CrossRef] [Green Version]
- Barreira, T.V.; Redmond, J.G.; Brutsaert, T.D.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T.; Tudor-Locke, C. Can an automated sleep detection algorithm for waist-worn accelerometry replace sleep logs? Appl. Physiol. Nutr. Metab. 2018, 43, 1027–1032. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T. Fully automated waist-worn accelerometer algorithm for detecting children’s sleep-period time separate from 24-h physical activity or sedentary behaviors. Appl. Physiol. Nutr. Metab. 2014, 39, 53–57. [Google Scholar] [CrossRef]
- Bellettiere, J.; Zhang, Y.; Berardi, V.; Full, K.M.; Kerr, J.; LaMonte, M.J.; Evenson, K.R.; Hovell, M.; LaCroix, A.Z.; Di, C. Parameterizing and validating existing algorithms for identifying out-of-bed time using hip-worn accelerometer data from older women. Physiol. Meas. 2019, 40, 075008. [Google Scholar] [CrossRef]
- Full, K.M.; Kerr, J.; Grandner, M.A.; Malhotra, A.; Moran, K.; Godoble, S.; Natarajan, L.; Soler, X. Validation of a physical activity accelerometer device worn on the hip and wrist against polysomnography. Sleep Health 2018, 4, 209–216. [Google Scholar] [CrossRef]
- Tracy, J.D.; Acra, S.; Chen, K.Y.; Buchowski, M.S. Identifying bedrest using 24-h waist or wrist accelerometry in adults. PLoS ONE 2018, 13, e0194461. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Order | Intensity Category | Activity | Description of Activity School Study | Description of Activity Preschool Study |
|---|---|---|---|---|
| 1 | Sedentary | Sitting | Sitting on a chair close to a table with arms in the lap | * Sitting on the buttocks on the floor playing with Lego or Geomac toys. |
| 2 | Sedentary | Sitting playing | Playing the Fruit Ninja game on an iPad | Sitting on a chair close to a table playing with Lego or Geomac toys at the table. |
| 3 | Light | Standing playing | Playing a game on the iPad while standing | * Standing close to a table playing with Lego or Geomac toy at the table. |
| 4 | Light | Slow walking | Slow walking speed | Walks at the child’s preferred walking speed together with the instructor. |
| 5 | Moderate | Brisk walking | Brisk walking speed | Walks fast trying to catch up with the instructor without running. |
| 6 | Vigorous | Running | Running at the subjects own preferred running speed | Runs at the child’s preferred running speed together with the instructor. |
| 7 | Very vigorous | Basketball | One-to-one competitive basketball game play | Not performed |
| 8 | Very vigorous | Playground | ** Running and walking around the school playground in a follow my leader activity | Walking, crawling, jumping and running through a predefined obstacle course |
| 9 | Moderate/vigorous | Biking | Commuting cycling on subjects’ own bike | Cycling on an adjustable child running bike at the child´s preferred speed. |
| 10 | Sedentary | Sitting | Sitting close to a table with arms in the lap | |
| 11 | Light | Swing | Not performed | ***Sitting on a swing in self-selected effort |
| Pre-School | Children | Adolescents | ||||
|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Sensitivity | Specificity | Sensitivity | Specificity | |
| Sitting | 100.0 | 100.0 | 99.8 | 99.7 | 100.0 | 99.3 |
| Standing | 100.0 | 99.8 | 100.0 | 99.8 | 100.0 | 100.0 |
| Biking | 64.8 | 100.0 | 85.8 | 100.0 | 94.9 | 100.0 |
| Walking | 82.6 | 98.1 | 93.3 | 100.0 | 100.0 | 99.9 |
| Running | 92.4 | 95.0 | 99.9 | 97.3 | 99.6 | 99.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brønd, J.C.; Grøntved, A.; Andersen, L.B.; Arvidsson, D.; Olesen, L.G. Simple Method for the Objective Activity Type Assessment with Preschoolers, Children and Adolescents. Children 2020, 7, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/children7070072
Brønd JC, Grøntved A, Andersen LB, Arvidsson D, Olesen LG. Simple Method for the Objective Activity Type Assessment with Preschoolers, Children and Adolescents. Children. 2020; 7(7):72. https://0-doi-org.brum.beds.ac.uk/10.3390/children7070072
Chicago/Turabian StyleBrønd, Jan Christian, Anders Grøntved, Lars Bo Andersen, Daniel Arvidsson, and Line Grønholt Olesen. 2020. "Simple Method for the Objective Activity Type Assessment with Preschoolers, Children and Adolescents" Children 7, no. 7: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/children7070072