Defining a “Good Death” in Pediatric Oncology: A Mixed Methods Study of Healthcare Providers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Qualitative Analysis
3.3. Mixed Methods Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Theme * | Definition | Sample Quote |
|---|---|---|
| Acceptance ** | Recognition and internalization of death as an inevitable or impending outcome | The cultural shift now is that we’re just a little bit more accepting, and sometimes no matter what we do. We can’t save everybody. |
| Adolescent Development | Unique socio-developmental aspects specific to AYAs | Adolescents, where they are in their development, they live in two worlds, where they can say oh my gosh I’m dying and they are planning where they are going to go to college simultaneously. |
| Balance ** | Finding equity between two opposing forces/opinions; needs of patient and family, hope and truth, good and bad death elements | There is a balance between respecting their [the family’s] wishes at the same time to help them [the child] view the process, but it’s tricky. |
| Communication ** | Interchange of information regarding prognosis, options, and preferences | It was a hard thing to realize that if we had just found a way to break down that communication barrier between the parents and the child that we could have saved the child the experience of a prolonged death. |
| Control ** | Exercising direction over aspects surrounding the process of dying | I think [it’s important] that the family have the death go in the way that they had envisioned it. |
| Expectation/Anticipation of Death ** | Predicting and planning for timing and manner of death | I think the truth is patients are as prepared as we make them. |
| Failure | Concept that death in pediatric cancer is always a bad outcome; often associated with a negative EOL experience | It’s never end point we’re hoping for so it feels to everyone often a bit like a failure. |
| Fear/Worry | Expressing the emotion of fear regarding care or outcome; often associated with a negative EOL experience | Nobody fears death, everybody fears dying. |
| Finances/Resources/Healthcare System | Aspects of the medical system related to finances or allocation of resources | We’re very busy, and there’s a set amount of time that we have for each patient...and we kind of have to budget. |
| Finding/Creating Meaning ** | Uncovering or creating the significance and purpose of death and dying process | I had an adolescent—[who said] that, ‘I know I’m going to die of this cancer, and I just want somebody to be able to study this. To help some other generation of kids with leukemia’. |
| Guilt/Regret/Remorse | Expressing a feeling (or perceived feeling) of regret/remorse/blame | I have had kids tell me, many many years later I wish I had been able to be with my sibling when they had died. |
| Hope | Faith or belief in the possibility of a good outcome or cure; positive or negative influence on EOL experience | We’re hoping we’re going to cure you, but that doesn’t always work and we have to think about what are our goals if we can’t cure you. |
| Injustice | Unfairness of illness/death in a child; often associated with a negative EOL experience | Parents shouldn’t be burying their kids, and kids should have the ability to grow up and lead these wonderful, productive adult lives, and for those to be cut short, it doesn’t seem right. |
| Knowledge/Research ** | Expressing need to learn more about providing good end of life care | If I know that people are actually researching what a good death is, that gives me a lot of confidence and hope in being able to be a provider that cares well for these patients. |
| Location Where Death Occurs | Referencing the physical location where the patient dies or prefers to die | I do think that it is easier to have a good death outside of the hospital. |
| Meeting Families Where they Are ** | Eliciting and accommodating patient/family preferences | … What you need to do more than anything is listen to the cues of your families. it’s meeting the family in the process, where they’re at. |
| Metaphor (Fight) | Concept of a fight against cancer; conflict, war, battle; positive or negative | Us versus cancer, right. And that fight mentality I think can be very positive. |
| Multidisciplinary ** | Recognizing multiple members of the medical team, and the importance of patients/families having a varied team | I think that it’s very important to work as a team; not everyone can do everything. |
| Protection/Selflessness | Concern for the wellbeing of others; trying to prevent suffering or harm | Once they [adolescents] know they’re going to die, their concern is for other people, and not for themselves. |
| HCP Experience Doing EOL Work | General experience providers have caring for patients with cancer, especially around the time of death; positive or negative | It is incredibly hard to say that there is nothing else that we can do; I can’t imagine how hard that is to hear but it is a very hard thing to say as well. |
| Relationships ** | Interpersonal dynamic between providers and patients/families | Everyone has a different degree of how close they get to families and how sad they get. |
| Religion/Spirituality | Specific religion or spiritual practice; concept of a metaphysical power or god; positive or negative | The families that are spiritual or religious, my sense is it helps them try to put together some sense of meaning. |
| Resolution ** | Some form of closure or completion | If I can’t go to the memorial, I will just try to go some place and stop and think about them. I am trying to be there with you and say goodbye. |
| Response to Death and the Dying Process | Description of response to a death/dying; coping strategies, emotions, etc.; positive or negative | That was a horrible death, it was horrible for them, it was horrible for all the staff. Because all the dad could do was rage against everyone. |
| Support/Community ** | Social network available to patient/family | For adolescents the peer support group is more important than their parents in terms of how they see the world and who they see themselves to be. |
| Symptom Management ** | Pharmacologic and non-pharmacologic means of minimizing mental and physical distress around death | First of all, a good death needs to be a comfortable death. The symptom piece of it needs to be managed. |
References
- Steinhauser, K.E.; Christakis, N.A.; Clipp, E.C.; McNeilly, M.; McIntyre, L.; Tulsky, J.A. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000, 284, 2476–2482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinhauser, K.E.; Clipp, E.C.; McNeilly, M.; Christakis, N.A.; McIntyre, L.M.; Tulsky, J.A. In search of a good death: Observations of patients, families, and providers. Ann. Intern. Med. 2000, 132, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Linda, L.E. The promise of a good death. Lancet 1998, 351, SII21–SII29. [Google Scholar] [CrossRef]
- Foley, K.M.; Hellen, G. Improving Palliative Care for Cancer; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Ferris, F.D.; Bruera, E.; Cherny, N.; Cummings, C.; Currow, D.; Dudgeon, D.; JanJan, N.; Strasser, F.; von Gunten, C.F.; von Roenn, J.H. Palliative cancer care a decade later: Accomplishments, the need, next steps—From the American Society of Clinical Oncology. J. Clin. Oncol. 2009, 27, 3052–3058. [Google Scholar] [CrossRef]
- National Consensus Project for Quality Palliative Care. Clinical Practice Guidelines for Quality Palliative Care, 4th ed.; National Coalition for Hospice and Palliative Care: Richmond, VA, US, 2018; Available online: https://www.nationalcoalitionhpc.org/ncp (accessed on 16 June 2020).
- Ahluwalia, S.C.; Chen, C.; Raaen, L.; Motala, A.; Walling, A.M.; Chamberlin, M.; O’Hanlon, C.; Larkin, J.; Lorenz, K.; Akinniranye, O.; et al. A systematic review in support of the national consensus project clinical practice guidelines for quality palliative care. J. Pain Symptom Manag. 2018, 56, 831–870. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, A.R.; Wolfe, J. Palliative care for adolescents and young adults with cancer. Clin. Oncol. Adolesc. Young Adults 2013, 3, 41–48. [Google Scholar]
- Webb, N.M.; Tucker, D. Young adults’ opinions about hospice and home death. J. Palliat. Med. 2009, 12, 337–342. [Google Scholar] [CrossRef]
- Lyon, M.E.; Jacobs, S.; Briggs, L.; Cheng, Y.I.; Wang, J. Family-Centered advance care planning for teens with cancer. JAMA Pediatrics 2013, 167, 460–467. [Google Scholar] [CrossRef] [Green Version]
- Hinds, P.S.; Drew, D.; Oakes, L.L.; Fouladi, M.; Spunt, S.L.; Church, C.; Furman, W.L. End-Of-Life care preferences of pediatric patients with cancer. J. Clin. Oncol. 2005, 23, 9146–9154. [Google Scholar] [CrossRef] [Green Version]
- Wiener, L.; Zadeh, S.; Battles, H.; Baird, K.; Ballard, E.; Osherow, J. Allowing adolescents and young adults to plan their End-Of-Life care. Pediatrics 2012, 130, 897–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pritchard, S.; Cuvelier, G.; Harlos, M.; Barr, R. Palliative care in adolescents and young adults with cancer. Cancer 2011, 117, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feudtner, C.; Rosenberg, A.R.; Boss, R.D.; Wiener, L.; Lyon, M.E.; Hinds, P.S.; Bluebond-Langner, M.; Wolfe, J. Challenges and Priorities for Pediatric Palliative Care Research in the US and Similar Practice Settings: Report From a Pediatric Palliative Care Research Network Workshop. J. Pain Symptom Manag. 2019, 58, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, J.; Grier, H.E.; Klar, N.; Levin, S.B.; Ellenbogen, J.M.; Salem-Schatz, S.; Emanuel, E.J.; Weeks, J.C. Symptoms and suffering at the end of life in children with cancer. N. Engl. J. Med. 2000, 342, 326–333. [Google Scholar] [CrossRef]
- Wolfe, J.; Klar, N.; Grier, H.E.; Duncan, J.; Salem-Schatz, S.; Emanuel, E.J.; Weeks, J.C. Understanding of prognosis among parents of children who died of cancer: Impact on treatment goals and integration of palliative care. JAMA 2000, 284, 2469–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contro, N.; Larson, J.; Scofield, S.; Sourkes, B.; Cohen, H. Family perspectives on the quality of pediatric palliative care. Arch. Pediatrics Adolesc. Med. 2002, 156, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robbins, J.R.; Deepak, K.; Fabian, J. Palliative care education for oncologists: How are we doing? Ann. Palliat. Med. 2019, 8, 364–371. [Google Scholar] [CrossRef]
- Rosenberg, A.R.; Meaghann, S.W.; Lori, W. Who is responsible for delivering palliative care to children with cancer? Pediatric Blood Cancer 2018, 65, e26889. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Creswell, J.W.; Cheryl, N.P. Qualitative inquiry and research design: Choosing among five approaches. Sage Publ. 2015, 16, 473–475. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis; Sage: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Creswell, J.W.; Vicki, L.P.C. Designing and Conducting Mixed Methods Research; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Glare, P.; Virik, K.; Jones, M.; Hudson, M.; Eychmuller, S.; Simes, J.; Christakis, N. A systematic review of physicians’ survival predictions in terminally ill cancer patients. BMJ 2003, 327, 195. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, A.R.; Bradford, M.C.; Barton, K.S.; Etsekson, N.; McCauley, E.; Curtis, J.R.; Wolfe, J.; Baker, K.S.; Yi-Frazier, J.P. Hope and benefit finding: Results from the PRISM randomized controlled trial. Pediatr. Blood Cancer 2019, 66, e27485. [Google Scholar] [CrossRef] [PubMed]
- Barton, K.S.; Tate, T.; Lau, N.; Taliesin, K.B.; Waldman, E.D.; Rosenberg, A.R. I’m not a spiritual person. How hope might facilitate conversations about spirituality among teens and young adults with cancer. J. Pain Symptom Manag. 2018, 55, 1599–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feudtner, C. The breadth of hopes. N. Engl. J. Med. 2009, 361, 2306–2307. [Google Scholar] [CrossRef] [PubMed]
- Hilden, J.M.; Emanuel, E.J.; Fairclough, D.L.; Link, M.P.; Foley, K.M.; Clarridge, B.C.; Schnipper, L.E.; Mayer, R.J. Attitudes and practices among pediatric oncologists regarding End-Of-Life care: Results of the 1998 American Society of Clinical Oncology survey. J. Clin. Oncol. 2001, 19, 205–212. [Google Scholar] [CrossRef]


| Total = 19 | |
|---|---|
| n (%) | |
| Role | |
| Pediatric Oncology Physician/Fellow | 8 (42) |
| Pediatric Oncology Advanced Practice Provider (NP/PA) | 4 (21) |
| Pediatric Oncology Nurse | 2 (11) |
| Other (Child Life Specialist, Chaplain, Physical Therapist, Educator) | 5 (26) |
| Sex | |
| Male | 5 (26) |
| Female | 14 (74) |
| Race/Ethnicity | |
| Hispanic/Latino | 0 (0) |
| American Indian/Alaska Native | 1 (5) |
| Asian | 3 (16) |
| Black | 1 (5) |
| White | 15 (79) |
| Experience in End of Life Care | |
| Number of Years in Position (median, range) | 8 (<1–18) |
| Number of AYA/pediatric patient deaths per year | |
| 1–5 | 14 (74) |
| 6–10 | 3 (16) |
| 11–15 | 2 (10) |
| Number of AYA/pediatric patients cared for per month (mean, range) | 20 (5–75) |
| Received training in: a | |
| Communication | |
| Yes | 10 (53) |
| No | 9 (47) |
| Talking about death and dying | |
| Yes | 10 (53) |
| No | 9 (47) |
| Providing end of life/hospice/palliative care | |
| Yes | 12 (63) |
| No | 7 (37) |
| Comfort level in discussing death/dying with: b | Mean (range) |
| Patients | 6.8 (2–10) |
| Parents/caregivers | 7.2 (3–10) |
| Theme * | Definition | Exemplary Quotes |
|---|---|---|
| Communication | Interchange of information regarding prognosis, options, and preferences | “It was a hard thing to realize that if we had just found a way to break down that communication barrier between the parents and the child that we could have saved the child the experience of a prolonged death”. |
| Symptom Management | Means of minimizing mental and physical distress around death | “First of all, a good death needs to be a comfortable death. The symptom piece of it needs to be managed”. |
| Acceptance | Recognition and internalization of death as an inevitable outcome | “The cultural shift now is that we’re just a little bit more accepting, and sometimes no matter what we do... we can’t save everybody”. |
| Meeting Families Where They Are | Eliciting and accommodating patient/family preferences | “What you need to do more than anything is listen to the cues of your families it’s meeting the family in the process, where they’re at”. |
| Expectation/Anticipation of Death | Predicting and planning for timing and manner of death | “I think the truth is patients are as prepared as we make them”. |
| Support/Community | Social network available to patient/family | “For adolescents the peer support group is more important than their parents in terms of how they see the world and who they see themselves to be”. |
| Control | Exercising direction over aspects surrounding the dying process | “I think [it’s important] that the family have the death go in the way that they had envisioned it”. |
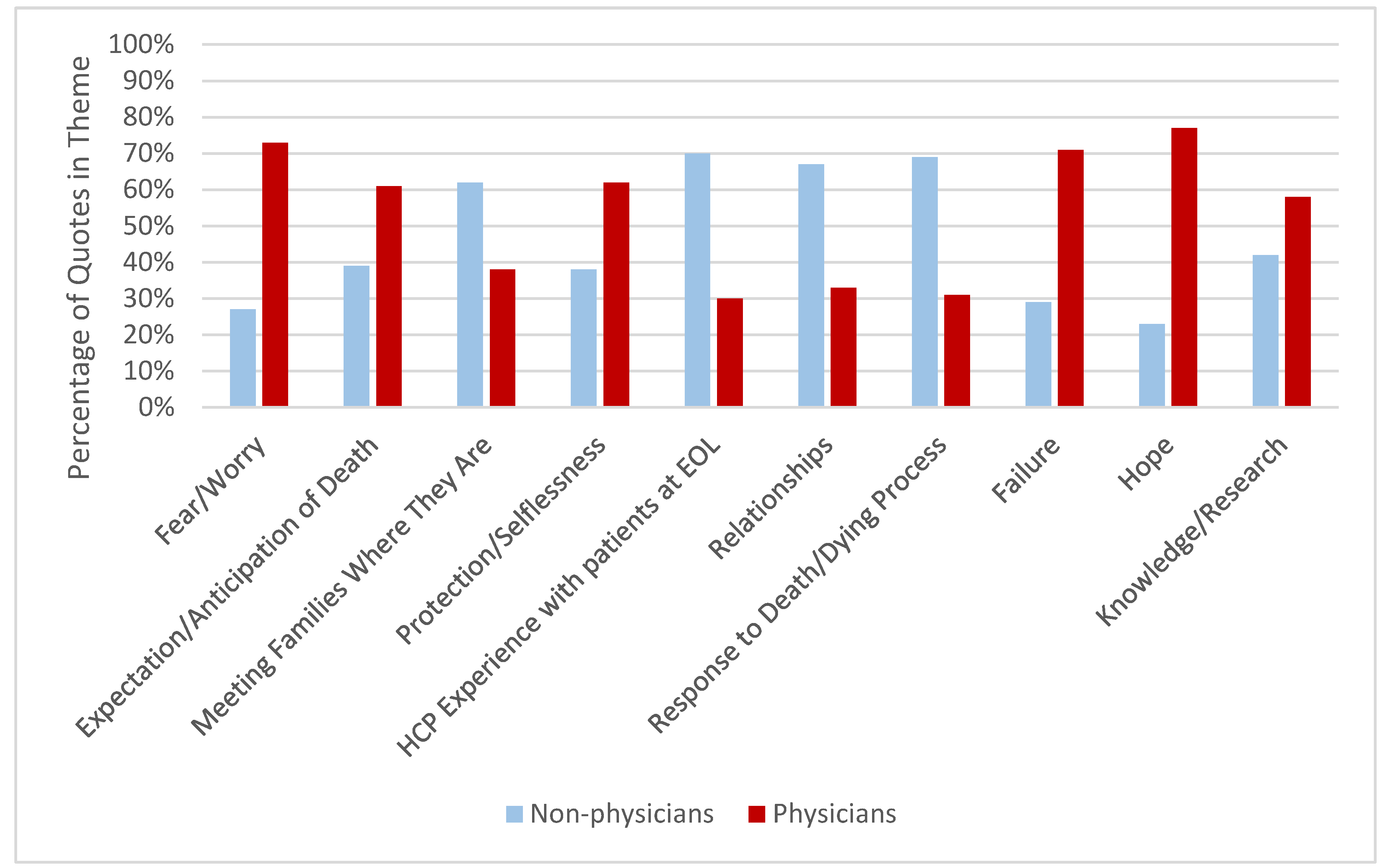
| Count (%) | Count (%) | p-Value b | |
|---|---|---|---|
| Theme * | Non-Physician (n = 11) | Physician (n = 8) | |
| Expectation/Anticipation of Death | 27 (39) | 43 (61) | 0.07 |
| Fear/Worry | 6 (27) | 16 (73) | 0.06 |
| Meeting Families Where They Are | 43 (62) | 26 (38) | 0.05 |
| Protection/Selflessness | 16 (38) | 26 (62) | 0.16 |
| HCP Experience Working With Patients at EOL | 85 (70) | 37 (30) | <0.001 |
| Relationships | 68 (67) | 33 (33) | 0.007 |
| Response to Death and the Dying Process | 43 (69) | 19 (31) | 0.003 |
| Hope | 3 (23) | 10 (77) | 0.1 |
| Failure | 5 (29) | 12 (71) | 0.15 |
| Knowledge/Research | 16 (42) | 22 (58) | 0.42 |
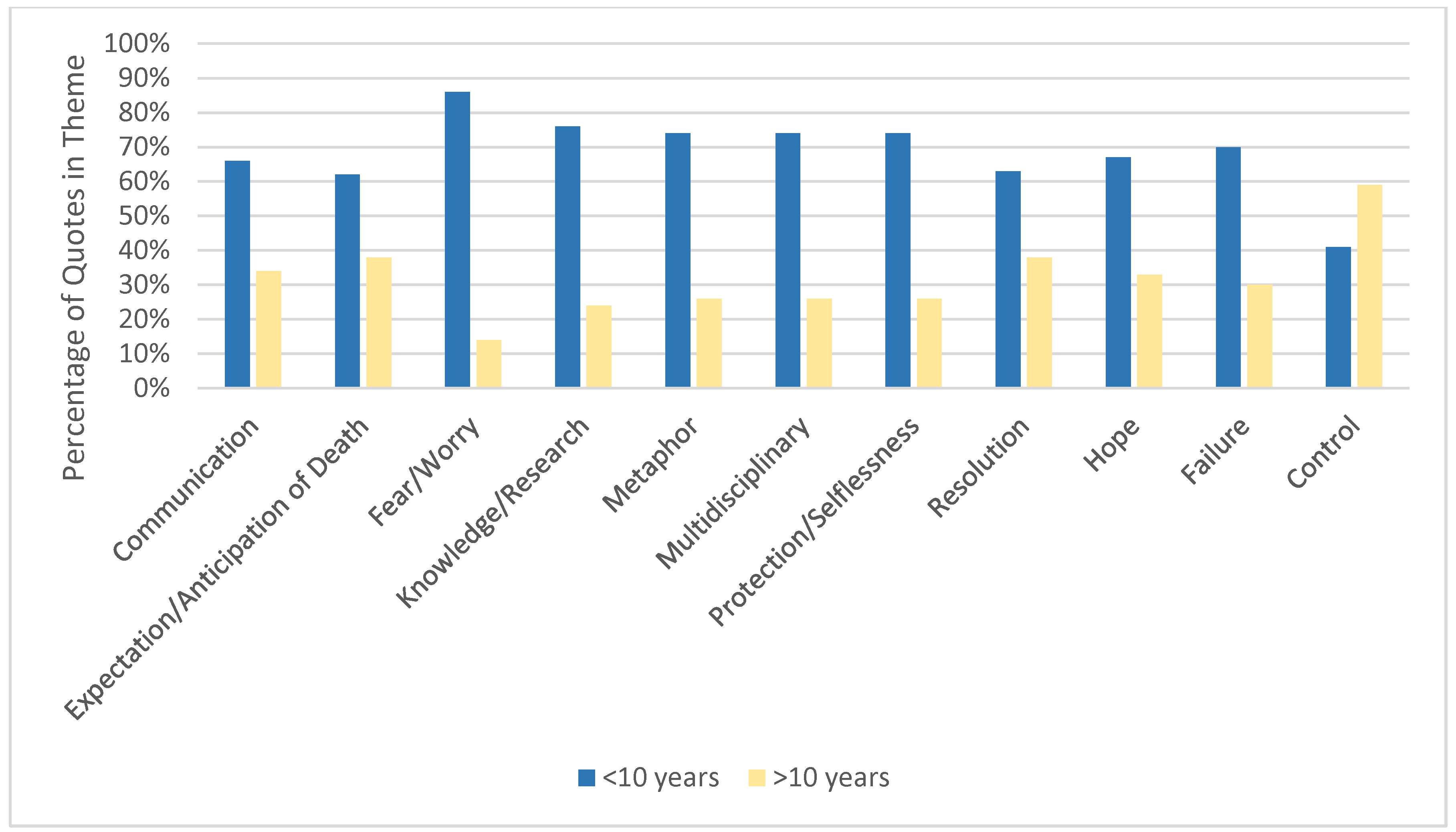
| <10 years (n = 11) | >10 years (n = 8) | ||
| Communication | 98 (66) | 51 (34) | <0.001 |
| Expectation/Anticipation of Death | 42 (62) | 26 (38) | 0.07 |
| Fear/Worry | 18 (86) | 3 (14) | 0.002 |
| Metaphor | 20 (74) | 7 (26) | 0.02 |
| Multidisciplinary | 29 (74) | 10 (26) | 0.004 |
| Protection/Selflessness | 31 (74) | 11 (26) | 0.003 |
| Resolution | 20 (63) | 12 (38) | 0.2 |
| Hope | 8 (67) | 4 (33) | 0.4 |
| Failure | 14 (70) | 6 (30) | 0.1 |
| Knowledge/Research | 29 (76) | 9 (24) | 0.002 |
| Control | 24 (41) | 35 (59) | 0.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, M.R.; Barton, K.S.; Kingsley, J.M.; Heunis, J.; Rosenberg, A.R. Defining a “Good Death” in Pediatric Oncology: A Mixed Methods Study of Healthcare Providers. Children 2020, 7, 86. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080086
Taylor MR, Barton KS, Kingsley JM, Heunis J, Rosenberg AR. Defining a “Good Death” in Pediatric Oncology: A Mixed Methods Study of Healthcare Providers. Children. 2020; 7(8):86. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080086
Chicago/Turabian StyleTaylor, Mallory R., Krysta S. Barton, Jenny M. Kingsley, Julia Heunis, and Abby R. Rosenberg. 2020. "Defining a “Good Death” in Pediatric Oncology: A Mixed Methods Study of Healthcare Providers" Children 7, no. 8: 86. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080086