Evaluating and Enhancing the Preparation of Patients and Families before Pediatric Surgery

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, Survey Participants and Size
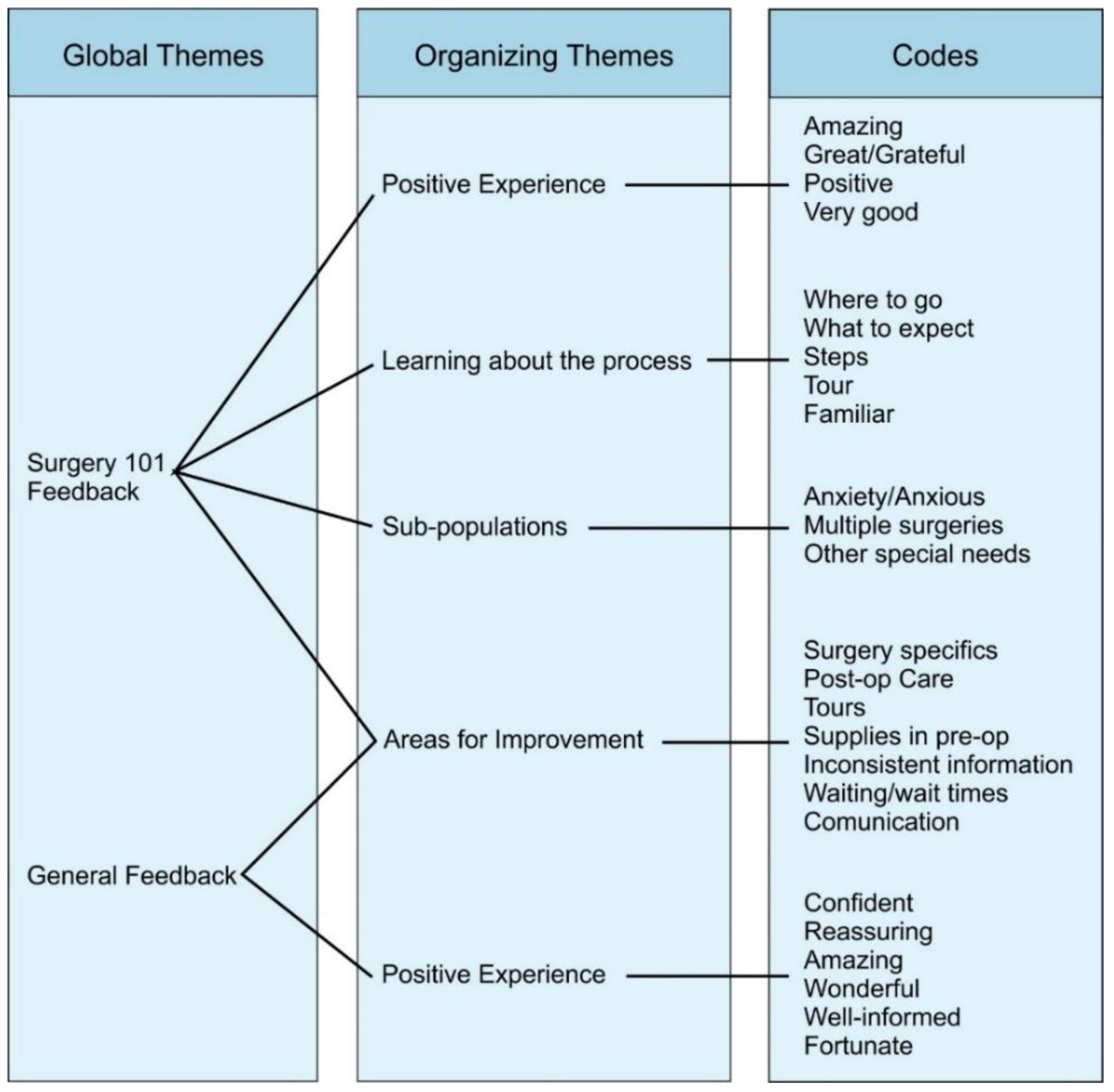
2.2. Thematic Analysis
2.3. Statistical Analysis
3. Results
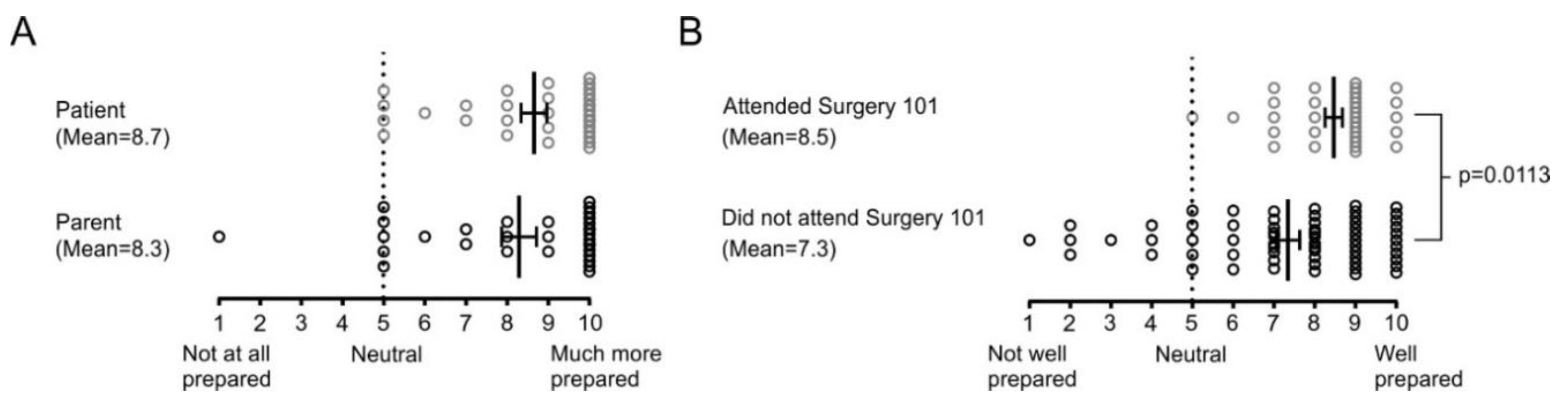
3.1. Surgery 101 Better Prepares Families for Surgery
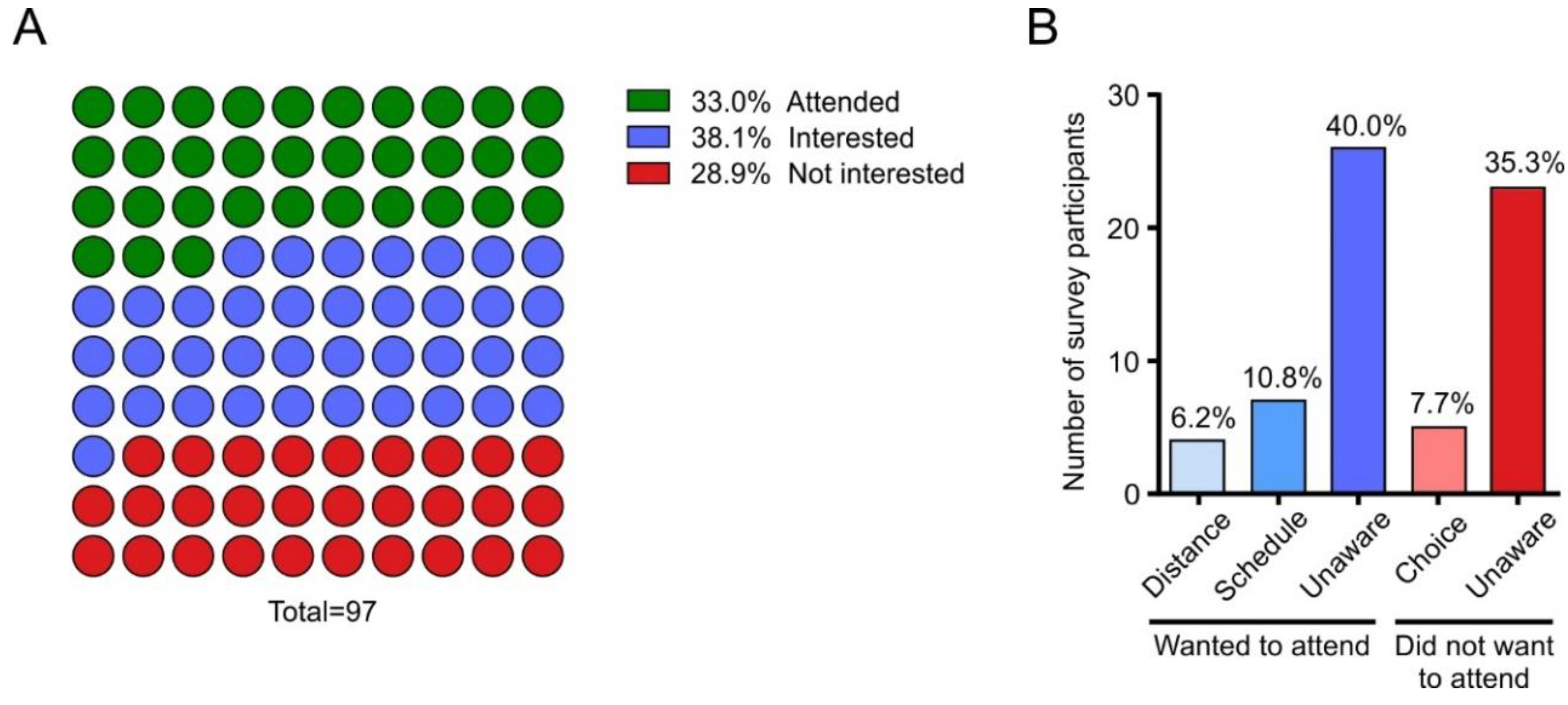
3.2. Surgery 101 Is Not Widely Accessible to Potential Participants
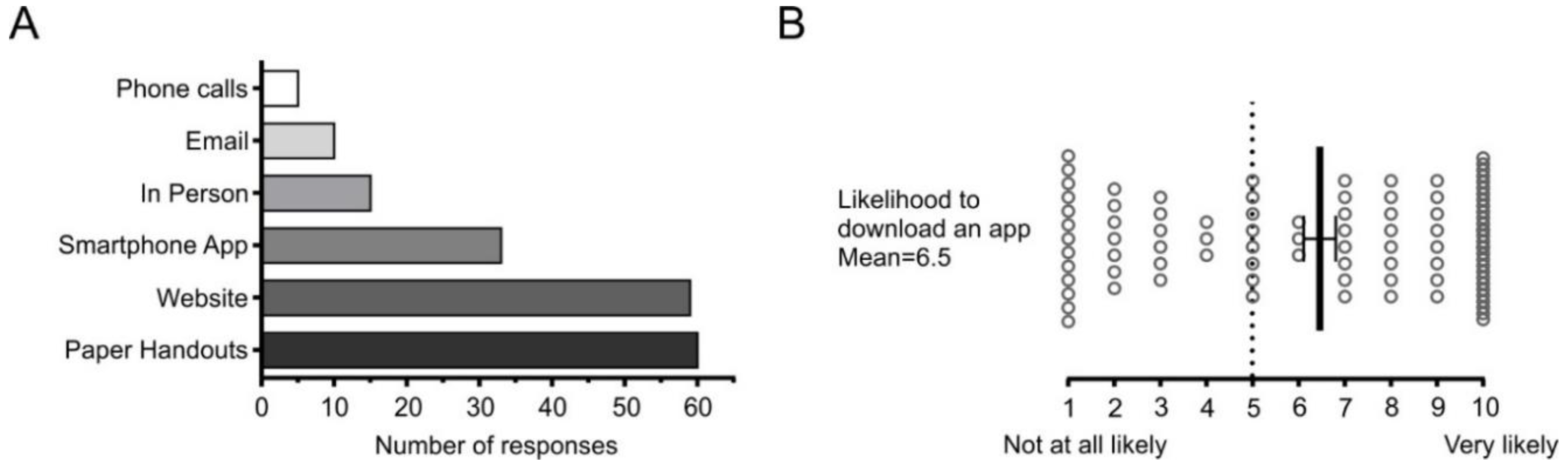
3.3. Accessibility of the Information in Surgery 101 Can be Improved
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Canadian Medical Protective Association. Surgical Safety in Canada: A 10-Year Review of CMPA and HIROC Medico-Legal Data. Available online: https://www.patientsafetyinstitute.ca/en/toolsResources/Surgical-Safety-in-Canada/Pages/default.aspx (accessed on 1 June 2020).
- Wright, J.G.; Menaker, R.J.; Houle, A.M.; Leclerc, S.; Mayer, S.K.; Willis, B.; Corsten, G.; Blair, G.K.; Jones, S.; Hyndman, W.; et al. Waiting for children’s surgery in Canada: The Canadian Paediatric Surgical Wait Times project. Can. Med. Assoc. J. 2011, 183, E559–E564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visintainer, M.A.; Wolfer, J.A. Psychological Preparation for Surgical Pediatric Patients: The Effect on Children’s and Parents’ Stress Responses and Adjustment. Pediatrics 1975, 56, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Kain, Z.N.; Mayes, L.C.; O’Connor, T.Z.; Cicchetti, D.V. Preoperative anxiety in children: Predictors and outcomes. Arch. Pediatr. Adolesc. Med. 1996, 150, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Kain, Z.N.; Mayes, L.C.; Caldwell-Andrews, A.A.; Karas, D.E.; McClain, B.C. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics 2006, 118, 651–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grocott, M.P.W.; Plumb, J.O.M.; Edwards, M.; Fecher-Jones, I.; Levett, D.Z.H. Re-designing the pathway to surgery: Better care and added value. Perioper. Med. 2017, 6, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rankinen, S.; Salanterä, S.; Heikkinen, K.; Johansson, K.; Kaljonen, A.; Virtanen, H.; Leino-Kilpi, H. Expectations and received knowledge by surgical patients. Int. J. Qual. Health Care 2007, 19, 113–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullen, M.G.; Michaels, A.D.; Mehaffey, H.J.; Guidry, C.A.; Turrentine, L.E.; Hedrick, T.L.; Friel, C.M. Risk associated with complications and mortality after urgent surgery vs elective and emergency surgery: Implications for defining “quality” and reporting outcomes for urgent surgery. JAMA Surg. 2017, 152, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, S.C.; Arriaga, P.; Esteves, F. Providing preoperative information for children undergoing surgery: A randomized study testing different types of educational material to reduce children’s preoperative worries. Health Educ. Res. 2014, 29, 1058–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogusaite, L.; Razlevice, I.; Lukosiene, L.; Macas, A. Evaluation of preoperative information needs in pediatric anesthesiology. Med. Sci. Monit. 2018, 24, 8773–8780. [Google Scholar] [CrossRef] [PubMed]
- Kain, Z.N.; Caldwell-Andrews, A.A.; Mayes, L.C.; Weinberg, M.E.; Wang, S.M.; MacLaren, J.E.; Blount, R.L. Family-centered preparation for surgery improves perioperative outcomes in children: A randomized controlled trial. Anesthesiology 2007, 106, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Warnock, G.L. The use of apps in surgery. Can. J. Surg. 2012, 55, 77. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.J.; Fayed, I.; Henault, S.; Kalantar, B.; Voyadzis, J.-M. Use of a Smartphone Application for Spine Surgery Improves Patient Adherence with Preoperative Instructions and Decreases Last-minute Surgery Cancellations. Cureus 2019, 11, e4192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera-Usagre, M.; Santana, V.; Burgos-Pol, R.; Oliva, J.P.; Sabater, E.; Rita-Acosta, M.; Casado, M.A.; Cruces, S.; Pacheco, M.; Perez, C.S. Effect of a mobile app on preoperative patient preparation for major ambulatory surgery: Protocol for a randomized controlled trial. J. Med. Internet Res. 2019, 21, e10938. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Participants | 97 |
| Sex (%) | |
| Male | 59 (60.8) |
| Female | 38 (39.2) |
| Type of surgical procedure (%) | |
| Dental | 4 (4.1) |
| ENT | 25 (25.8) |
| GI | 16 (16.5) |
| Neurosurgery | 2 (2.0) |
| Ophthalmology | 7 (7.2) |
| Orthopedics | 9 (9.3) |
| Plastics | 5 (5.2) |
| Thoracic | 1 (1.0) |
| Urology/Gynecology | 28 (28.9) |
| Age at operation (years) | |
| Mean | 5.8 |
| Median | 5 |
| Range | <1–16 |
| Length of hospital stay (%) | |
| <24 h | 34 (35.1) |
| >24 h | 63 (64.9) |
| Time notified before surgery (%) | |
| <7 days | 15 (15.4) |
| 7–28 days | 28 (28.9) |
| >28 days | 54 (55.7) |
| Distanced travelled for procedure (%) | |
| Within Calgary | 72 (74.3) |
| <100 km | 17 (17.5) |
| 100–250 km | 6 (6.2) |
| >250 km | 2 (2.0) |
| Time elapsed since surgery (%) | |
| <1 month | 35 (36.1) |
| 1–6 months | 32 (33.0) |
| 6–12 months | 11 (11.3) |
| >12 months | 19 (19.6) |
| Characteristic | Surgery 101 n (%) | Non-Surgery 101 n (%) |
|---|---|---|
| Participants | 32 | 65 |
| Sex (%) | ||
| Male | 23 (71.9) | 36 (55.4) |
| Female | 9 (28.1) | 29 (44.6) |
| Type of surgical procedure (%) | ||
| Dental | 1 (3.2) | 3 (4.6) |
| ENT | 10 (31.2) | 15 (23.1) |
| GI | 4 (12.5) | 12 (18.5) |
| Neurosurgery | 0 (0) | 2 (3.1) |
| Ophthalmology | 4 (12.5) | 3 (4.6) |
| Orthopedics | 2 (6.2) | 7 (10.8) |
| Plastics | 1 (3.2) | 4 (6.1) |
| Thoracic | 0 (0) | 1 (1.5) |
| Urology/Gynecology | 10 (31.2) | 18 (27.7) |
| Age at operation (years) | ||
| Mean | 5.5 | 5.9 |
| Median | 5 | 4 |
| Range | 1–12 | <1–16 |
| Length of hospital stay (%) | ||
| <24 h | 13 (40.6) | 21 (32.3) |
| >24 h | 19 (59.4) | 44 (67.7) |
| Time notified before surgery (%) | ||
| <7 days | 2 (6.2) | 13 (20.0) |
| 7–28 days | 8 (25.0) | 20 (30.8) |
| >28 days | 22 (68.8) | 32 (49.2) |
| Distanced travelled for procedure (%) | ||
| Within Calgary | 25 (78.1) | 47 (72.3) |
| <100 km | 4 (12.5) | 13 (20.0) |
| 100–250 km | 3 (9.4) | 3 (4.6) |
| >250 km | 0 (0) | 2 (3.1) |
| Time elapsed since surgery (%) | ||
| <1 month | 11 (34.3) | 24 (36.9) |
| 1–6 months | 14 (43.7) | 18 (27.7) |
| 6–12 months | 6 (18.8) | 5 (7.7) |
| >12 months | 1 (3.2) | 18 (27.7) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Newell, C.; Leduc-Pessah, H.; Bell-Graham, L.; Rasic, N.; Carter, K. Evaluating and Enhancing the Preparation of Patients and Families before Pediatric Surgery. Children 2020, 7, 90. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080090
Newell C, Leduc-Pessah H, Bell-Graham L, Rasic N, Carter K. Evaluating and Enhancing the Preparation of Patients and Families before Pediatric Surgery. Children. 2020; 7(8):90. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080090
Chicago/Turabian StyleNewell, Christopher, Heather Leduc-Pessah, Lisa Bell-Graham, Nivez Rasic, and Kerryn Carter. 2020. "Evaluating and Enhancing the Preparation of Patients and Families before Pediatric Surgery" Children 7, no. 8: 90. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080090