The Effectiveness of Hippotherapy to Recover Gross Motor Function in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis


 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
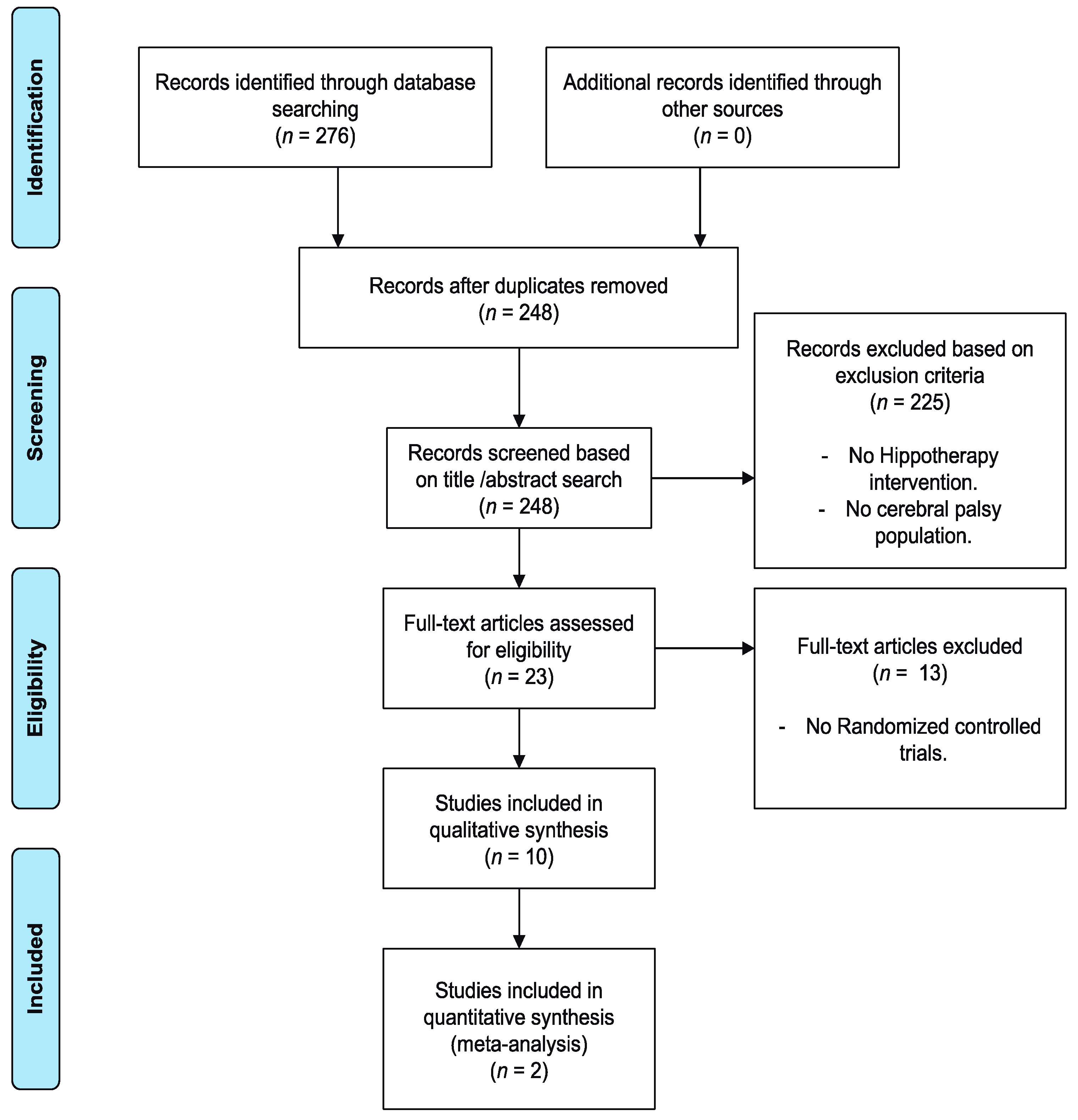
2.3. Study Selection Process and Data Extraction
2.4. Assessment of the Methodological Quality of the Studies
3. Results
3.1. Methodological Quality of the Studies
3.2. Main Characteristics of the Studies Included in the Systematic Review
3.3. Meta-Analysis of the Study Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Petersen, R.; Procter, C.; Donald, K.A. Assessment and Management of the Child with Cerebral Palsy. In Clinical Child Neurology; Springer International Publishing: Cham, Switzerland, 2020; pp. 175–203. [Google Scholar]
- Longo, E.; Regalado, I.C.R.; Galvão, E.R.V.P.; Ferreira, H.N.C.; Badia, M.; Baz, B.O. I Want to Play: Children With Cerebral Palsy Talk About Their Experiences on Barriers and Facilitators to Participation in Leisure Activities. Pediatr. Phys. Ther. 2020, 32, 190–200. [Google Scholar] [PubMed]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.-C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy. JAMA Pediatr. 2017, 171, 897. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Romero, J.G.; Molina-Aroca, A.; Moral-Munoz, J.A.; Luque-Moreno, C.; Lucena-Anton, D. Effectiveness of mechanical horse-riding simulators on postural balance in neurological rehabilitation: Systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucena-Anton, D.; Rosety-Rodríguez, I.; Moral-Munoz, J.A. Effects of a hippotherapy intervention on muscle spasticity in children with cerebral palsy: A randomized controlled trial. Complement Ther. Clin Pract. 2018, 31, 188–192. [Google Scholar] [CrossRef]
- Koca, T.T. What is hippotherapy? The indications and effectiveness of hippotherapy. North Clin. Istanbul. 2016, 2, 247–252. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Mc Namara, M.; Paton, M.C.B.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [Green Version]
- Alonso, P.M. Physiotherapy interventions through hippotherapy in the treatment of cerebral palsy. A literature review. Rehabilitación 2020, 54, 96–106. [Google Scholar]
- Martín-Valero, R.; Vega-Ballón, J.; Perez-Cabezas, V. Benefits of hippotherapy in children with cerebral palsy: A narrative review. Eur. J. Paediatr. Neurol. 2018, 22, 1150–1160. [Google Scholar] [CrossRef]
- Zadnikar, M.; Kastrin, A. Effects of hippotherapy and therapeutic horseback riding on postural control or balance in childrenwith cerebral palsy: A meta-analysis. Dev. Med. Child Neurol. 2011, 53, 684–691. [Google Scholar] [CrossRef]
- Alotaibi, M.; Long, T.; Kennedy, E.; Bavishi, S. The efficacy of GMFM-88 and GMFM-66 to detect changes in gross motor function in children with cerebral palsy (CP): A literature review. Disabil. Rehabil. 2014, 36, 617–627. [Google Scholar] [CrossRef]
- Whalen, N.C.; Case-Smith, J. Therapeutic effects of horseback riding therapy on gross motor function in children with cerebral palsy: A Systematic Review. Phys. Occup. Ther. Pediatr. 2012, 32, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Catalá-López, F.; Moher, D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [Green Version]
- McGibbon, N.H.; Benda, W.; Duncan, B.R.; Silkwood-Sherer, D. Immediate and long-term effects of Hippotherapy on symmetry of adductor muscle activity and functional ability in children with spastic cerebral palsy. Arch Phys. Med. Rehabil. 2009, 90, 966–974. [Google Scholar] [CrossRef]
- Kwon, J.-Y.; Chang, H.J.; Yi, S.-H.; Lee, J.Y.; Shin, H.-Y.; Kim, Y.-H. Effect of hippotherapy on gross motor function in children with cerebral palsy: A randomized controlled trial. J. Altern Complement Med. 2015, 21, 15–21. [Google Scholar] [CrossRef]
- Matusiak-Wieczorek, E.; Małachowska-Sobieska, M.; Synder, M. Influence of Hippotherapy on Body Balance in the Sitting Position Among Children with Cerebral Palsy. Ortop. Traumatol. Rehabil. 2016, 18, 165–175. [Google Scholar] [CrossRef]
- Benda, W.; McGibbon, N.H.; Grant, K.L. Improvements in muscle symmetry in children with cerebral palsy after equine-assisted therapy (Hippotherapy). J. Altern Complement Med. 2003, 9, 817–825. [Google Scholar] [CrossRef]
- Kang, H.; Jung, J.; Yu, J. Effects of Hippotherapy on the Sitting Balance of Children with Cerebral Palsy: A Randomized Control Trial. J. Phys. Ther. Sci. 2012, 24, 833–836. [Google Scholar] [CrossRef] [Green Version]
- El-Meniawy, G.H.; Thabet, N.S. Modulation of back geometry in children with spastic diplegic cerebral palsy via hippotherapy training. Egypt J. Med. Hum. Genet. 2012, 13, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Park, E.S.; Rha, D.-W.; Shin, J.S.; Kim, S.; Jung, S. Effects of Hippotherapy on gross motor function and functional performance of children with cerebral palsy. Yonsei Med. J. 2014, 55, 1736–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alemdaroğlu, E.; Oken, O.; Ucan, H.; Ersöz, M.; Köseoğlu, B.F.; Kapıcıoğlu, M. İsmail S.; Yanıkoğlu, I. Horseback riding therapy in addition to conventional rehabilitation program decreases spasticity in children with cerebral palsy: A small sample study. Complement Ther. Clin. Pract. 2016, 23, 26–29. [Google Scholar] [CrossRef]
- Deutz, U.; Heussen, N.; Weigt-Usinger, K.; Leiz, S.; Raabe, C.; Polster, T.; Steinbüchel, D.; Moll, C.; Lücke, T.; Krägeloh-Mann, I.; et al. Impact of Hippotherapy on Gross Motor Function and Quality of Life in Children with Bilateral Cerebral Palsy: A Randomized Open-Label Crossover Study. Neuropediatrics 2018, 49, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.; Rosenbaum, P.; Avery, L.; Lane, M. Gross Motor Function Measure (GMFM-66 and GMFM-88) User’s Manual: Clinics in Development Medicine; Mac Keith Press: London, UK, 2002. [Google Scholar]
- Wei, S.; Wang, S.J.; Liao, Y.G.; Hong, Y.; Xu, X.J.; Shao, X.M. Reliability and validity of the GMFM-66 in 0- to 3-year-old children with cerebral palsy. Am. J. Phys. Med. Rehabil. 2006, 85, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Casady, R.L.; Nichols-Larsen, D.S. The effect of hippotherapy on ten children with cerebral palsy. Pediatr. Phys. Ther. 2004, 16, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Bertoti, D.B. Effect of therapeutic horseback riding on posture in children with cerebral palsy. Phys. Ther. 1988, 68, 1505–1512. [Google Scholar] [PubMed]
- De Miguel, A.; De Miguel, M.D.; Lucena-Anton, D.; Rubio, M.D. Effects of hypotherapy on the motor function of persons with Down’s syndrome: A systematic review. Rev. Neurol. 2018, 67, 233–241. [Google Scholar]
- Srinivasan, S.M.; Cavagnino, D.T.; Bhat, A.N. Effects of Equine Therapy on Individuals with Autism Spectrum Disorder: A Systematic Review. Rev. J. Autism Dev. Disord. 2018, 5, 156–175. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Benda et al., 2003 [19] | - | Yes | Yes | No | No | No | No | Yes | No | Yes | Yes | 5 |
| McGibbon et al., 2009 [16] | - | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 7 |
| Kang et al., 2012 [20] | - | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| El-Meniawy and Thabet 2012 [21] | - | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4 |
| Park et al., 2014 [22] | - | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Kwon et al., 2015 [17] | - | Yes | No | Yes | Yes | No | Yes | Yes | No | Yes | Yes | 7 |
| Matusiak-Wieczorek et al., 2016 [18] | - | Yes | No | No | No | No | No | No | No | Yes | Yes | 3 |
| Alemdaroglu et al., 2016 [23] | - | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4 |
| Deutz et al., 2017 [24] | - | Yes | No | Yes | No | No | Yes | No | No | Yes | No | 4 |
| Lucena-Antón et al., 2018 [5] | - | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Study | Participants (n) | Age (Years) ± SD | Female/Male | GMFCS Levels | Type: Diplegia/Hemiplegia (n) | Diagnosis |
|---|---|---|---|---|---|---|
| Benda et al., 2003 [19] | IG: (n = 7) | 4–12 | ND | ND | ND | Spastic (n = 15) |
| CG: (n = 8) | ||||||
| N = 15 | ||||||
| McGibbon et al., 2009 [16] | Phase 1: | IG: 8.5 | IG: 9/16 | I: (n = 27) | IG: 12/4 | Spastic (n = 38) |
| IG: (n = 25) | II: (n = 9) | |||||
| CG: (n = 19) | CG: 13/3 | |||||
| N = 44 | CG: 8.8 | CG: 11/11 | III: (n = 5) | Mixed (n = 6) | ||
| Phase 2: | Quadriplegia: 9 | |||||
| IG: (n = 6) | IV: (n = 6) | |||||
| Kang et al., 2012 [20] | IG1:(n = 14) | IG1: 8.2 ± 1.1 | IG1: 7/7 | ND | IG1: 5/9 | ND |
| IG2: (n = 15) | IG2: 8.2 ± 1.2 | IG2: 7/8 | IG2: 5/10 | |||
| CG: (n = 15) | CG: 7.8 ± 1.5 | CG: 7/7 | CG: 5/9 | |||
| N = 44 | ||||||
| El-Meniawy and Thabet 2012 [21] | IG: (n = 15) | 7.02 ± 0.5 | ND | ND | ND | Spastic (n = 30) |
| CG: (n = 15) | ||||||
| N = 30 | ||||||
| Park et al., 2014 [22] | IG: (n = 34) | IG: 6.68 ± 2.6 | IG: 19/15 | I: (n = 14) | IG: 32/2 | Spastic (n = 55) |
| CG: (n = 21) | CG: 7.76 ± 3.7 | CG: 11/10 | II: (n = 15) | |||
| III: (n = 11) | CG: 19/2 | |||||
| IV: (n = 15) | ||||||
| N = 55 | ||||||
| Kwon et al., 2015 [17] | IG: (n = 45) | IG: 5.7 ± 1.9 | IG: 25/20 | I: (n = 24) | IG: 41/4 | Spastic (n = 84) |
| CG: (n = 46) | II: (n = 24) | |||||
| N = 91 | CG: 5.9 ± 1.8 | CG: 17/29 | III: (n = 23) | CG: 40/6 | Dyskinetic (n = 4) | |
| IV: (n = 20) | Ataxic (n = 3) | |||||
| Matusiak-Wieczorek et al., 2016 [18] | IG: (n = 19) | IG: 8.42 ± 2.2 | IG: 9/10 | I: (n = 23) | IG: 6/13 | Spastic (n = 39) |
| CG: (n = 20) | CG: 8.3 ± 2.6 | CG: 9/11 | II: (n = 16) | CG: 5/15 | ||
| N = 39 | ||||||
| Alemdaroğlu et al., 2016 [23] | IG: (n = 9) | 7.5 ± 1.7 | 7/9 | IG: I–IV | ND | Spastic (n = 16) |
| CG: (n = 7) | CG: I–V | |||||
| N = 16 | ||||||
| Deutz et al., 2017 [24] | IG: (n = 35) | IG: 9.29 ± 3.7 | IG: 12/23 | II: (n = 27) | IG: 35/0 | Spastic (n = 73) |
| CG: (n = 38) | CG: 8.87 ± 2.9 | CG: 17/21 | III: (n = 17) | CG: 38/0 | ||
| N = 73 | IV: (n = 29) | |||||
| Lucena-Antón et al., 2018 [5] | IG: (n = 22) | IG: 9.5 ± 2.7 | IG: 9/13 | IV–V | ND | Spastic (n = 44) |
| CG: (n = 22) | CG: 8.2 ± 2.4 | CG: 7/15 | ||||
| N = 44 |
| Study | Participants | Intervention | Frequency | Session Duration | Total Duration | Outcomes | Measuring Instruments | Results |
|---|---|---|---|---|---|---|---|---|
| Benda et al., 2003 [19] | IG: (n = 7) | IG: HPT | One session | 8 min | One session | Muscle activity in the paravertebral, hip abductors/adductors when sitting, standing, and walking | EMG | IG got better results than CG. Mean change improvements: IG = 64.6% (SD = 28.3) vs. CG = −12.8% (SD = 88.8); (p = 0.051) |
| CG: (n = 8) | CG: Exercises on a barrel | |||||||
| McGibbon et al., 2009 [16] | Phase 1: | IG: HPT | Phase 1: One session | Phase 1: 10 min | Phase 1: One session | Hip adductors muscle activity | SEMG | Phase 1: The IG significantly improved the muscle asymmetry of hip adductors (p < 001; d = 1.32) |
| IG: (n = 25) | ||||||||
| CG: (n = 19) | ||||||||
| Phase 2: | CG: Exercises on a barrel | Phase 2: Once a week | Phase 2: 40 min | Phase 2: 36 weeks | Phase 2: After 12 weeks, 4 of 6 children improved the muscle symmetry of hip adductors | |||
| IG: (n = 6) | ||||||||
| Kang et al., 2012 [20] | IG1:(n = 15) | IG1: HPT | Once a week | 30 min | 8 weeks | Sitting balance | Force plate | The results showed that pathway and velocity significantly decreased in the HPT group (p < 0.05) compared to the PT and CON groups |
| IG2: (n = 15) | IG2: PT | |||||||
| CG: (n = 15) | CG: Non treatment | |||||||
| El-Meniawy and Thabet 2012 [21] | IG: (n = 15) | IG: HPT | IG: Once a week | IG: 30 min | 12 weeks | Back geometry parameters: lateral deviation, trunk imbalance, pelvic tilt, rotation | Formetric instrument system | The results showed improvements in favor of the IG in all the outcomes (p < 0.05) |
| CG: (n = 15) | CG: Exercise | CG: 3 times/week | CG: 1 h | |||||
| Park et al., 2014 [22] | IG: (n = 34) | IG: HPT | 2 times/week | 45 min | 8 weeks | Gross motor function | GMFM-66 | Significant results were obtained in IG after the intervention compared to the CG: GMFM-66 (all dimensions); GMFM-88 (B and C dimensions); and 3 domains of the PEDI-FSS: (p < 0.05) |
| CG: (n = 21) | CG: Non treatment | Functional performance | GMFM-88 | |||||
| PEDI-FSS | ||||||||
| Kwon et al., 2015 [17] | IG: (n = 45) | IG: HPT | 2 times/week | 30 min | 8 weeks | Gross motor function. | GMFM-66 | Significant results were found between groups (p < 0.05): GMFM- 66, GMFM-88 (total score and dimensions B, C, D, and E). Moreover, significant results were found in balance (p < 0.05) |
| CG: (n = 46) | CG: Aerobic exercise | Balance | GMFM-88 PBS | |||||
| Matusiak-Wieczorek et al., 2016 [18] | IG: (n = 19) | IG: HPT | Once a week | 30 min | 12 weeks | Body balance in sitting position | SAS | Significant results were obtained in IG for arm function and control of trunk position: (p = 0.018) |
| CG: (n = 20) | CG: NI | |||||||
| Alemdaroğlu et al., 2016 [23] | IG: (n = 9) | IG: HPT | IG: 2 times/week | 30 min | 5 weeks | Gross motor function, hip adductors spasticity, balance, hip abduction angle, knee distance | GMFMCS | Significant improvements were observed between groups in spasticity (p = 0.016). Not significant results were found in other outcomes |
| MAS | ||||||||
| CG: (n = 7) | CG: PT | CG: 5 times/week | MFRT | |||||
| Goniometer | ||||||||
| Deutz et al., 2017 [24] | IG: (n = 35) | IG: HPT | 1–2 times/week | ND | 16–20 weeks | Gross motor function and quality of life | GMFM-66 KIDSCREEN-27 questionnaire | Improvements were observed in GMFM-66 dimension E for IG (p = 0.02) compared to CG. Not significant results were found in quality of life |
| CG: (n = 38) | CG: PT | CHQ | ||||||
| Lucena-Antón et al., 2018 [5] | IG: (n = 22) | IG: HPT | IG: Once a week | 45 min | 12 weeks | Hip adductors spasticity | MAS | Significant results were obtained between groups for IG in spasticity (p = 0.04 for left adductors and p = 0.047 for right adductors) |
| CG: (n = 22) | CG: PT | CG: 2 times/week |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guindos-Sanchez, L.D.; Lucena-Anton, D.; Moral-Munoz, J.A.; Salazar, A.; Carmona-Barrientos, I. The Effectiveness of Hippotherapy to Recover Gross Motor Function in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis. Children 2020, 7, 106. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090106
Guindos-Sanchez LD, Lucena-Anton D, Moral-Munoz JA, Salazar A, Carmona-Barrientos I. The Effectiveness of Hippotherapy to Recover Gross Motor Function in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis. Children. 2020; 7(9):106. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090106
Chicago/Turabian StyleGuindos-Sanchez, Laura De, David Lucena-Anton, Jose A. Moral-Munoz, Alejandro Salazar, and Ines Carmona-Barrientos. 2020. "The Effectiveness of Hippotherapy to Recover Gross Motor Function in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis" Children 7, no. 9: 106. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090106