Application of Low-Intensity Modified Constraint-Induced Movement Therapy to Improve the Affected Upper Limb Functionality in Infantile Hemiplegia with Moderate Manual Ability: Case Series

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
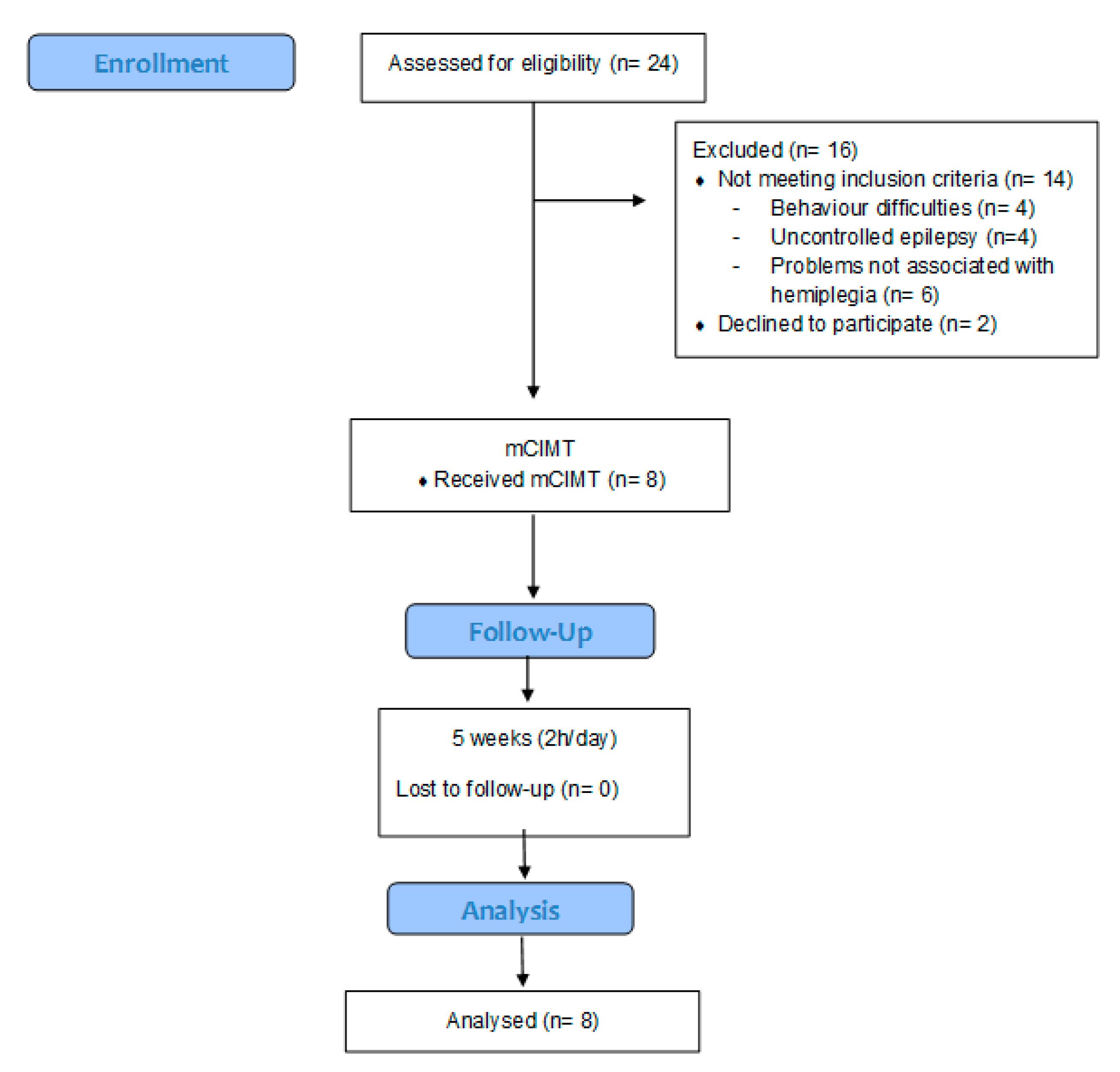
2. Materials and Methods
2.1. Intervention Method
2.2. Data Collection
2.2.1. Studied Variables and Measuring Instruments
Quality of Movement and Bimanual Dexterity of Both Upper Extremities
Active Extension of the Wrist and Active Supination of the Forearm in the Affected Upper Limb
Grasp Strength in the Affected Hand
Spontaneous Use, Dynamic Positioning of the Affected Upper Limb, Grasping and Releasing Action (Wrist Position in Neutral Flexion–Extension), and Level of Functionality and Integration of the Affected Upper Limb in Various Activities of Daily Living
2.3. Statistical Analysis
3. Results
3.1. Quality of Movement of the Upper Limb
3.2. Grasp Strength
3.3. Active Elbow Extension and Forearm Supination
3.4. Spontaneous Use, Dynamic Joint Position of the Affected Upper Limb, Grasp and Release Action (Wrist Position in Neutral Flexion–Extension), and Level of Functionality and Integration of the Affected Upper Limb in Different Activities of Daily Living
4. Discussion
Limitations and Future Lines of Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Monge Pereira, E.; Molina Rueda, F.; Alguacil Diego, I.M.; Cano de la Cuerda, R.; de Mauro, A.; Miangolarra Page, J.C. Empleo de sistemas de realidad virtual como método de propiocepción en parálisis cerebral: Guía de práctica clínica. Neurologia 2014, 29, 550–559. [Google Scholar] [CrossRef]
- Sgandurra, G.; Ferrari, A.; Cossu, G.; Guzzetta, A.; Biagi, L.; Tosetti, M.; Fogassi, L.; Cioni, G. Upper limb children action-observation training (UP-CAT): A randomised controlled trial in Hemiplegic Cerebral Palsy. BMC Neurol. 2011, 11, 80. [Google Scholar] [CrossRef] [Green Version]
- Eliasson, A.C.; Forssberg, H.; Hung, Y.C.; Gordon, A.M. Development of hand function and precision grip control in individuals with cerebral palsy: A 13-year follow-up study. Pediatrics 2006, 118. [Google Scholar] [CrossRef]
- Huang, W.C.; Chen, Y.J.; Chien, C.L.; Kashima, H.; Lin, K. Constraint-induced movement therapy as a paradigm of translational research in neurorehabilitation: Reviews and prospects. Am. J. Transl. Res. 2011, 3, 48–60. [Google Scholar]
- Wittenberg, G. Experience, cortical remapping and recovery in brain disease. Neurobiol. Dis. 2010, 37, 252–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liepert, J.; Bauder, H.; Miltner, W.H.R.; Taub, E.; Weiller, C. Treatment-induced cortical reorganization after stroke in humans. Stroke 2000, 31, 1210–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, J.; Gordon, A.M. A critical review of constraint-induced movement therapy and forced use in children with hemiplegia. Neural Plast. 2005, 12, 245–261. [Google Scholar] [CrossRef]
- Hoare, B.J.; Wallen, M.A.; Thorley, M.N.; Jackman, M.L.; LM, C.; Imms, C. Constraint-induced movement therapy in children with unilateral cerebral palsy. Cochrane Database Syst. Rev. 2019, 1–274. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Krumlinde-Sundholm, L.; Gordon, A.M.; Feys, H.; Klingels, K.; Aarts, P.B.M.; Rameckers, E.; Autti-Rämö, I.; Hoare, B. Guidelines for future research in constraint-induced movement therapy for children with unilateral cerebral palsy: An expert consensus. Dev. Med. Child Neurol. 2014, 56, 125–137. [Google Scholar] [CrossRef] [Green Version]
- Deppe, W.; Thuemmler, K.; Fleischer, J.; Berger, C.; Meyer, S.; Wiedemann, B. Modified constraint-induced movement therapy versus intensive bimanual training for children with hemiplegia-a randomized controlled trial. Clin. Rehabil. 2013, 27, 909–920. [Google Scholar] [CrossRef]
- Chen, Y.P.; Pope, S.; Tyler, D.; Warren, G.L. Effectiveness of constraint-induced movement therapy on upper-extremity function in children with cerebral palsy: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2014, 28, 939–953. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, A.C.; Nordstrand, L.; Ek, L.; Lennartsson, F.; Sjöstrand, L.; Tedroff, K.; Krumlinde-Sundholm, L. The effectiveness of Baby-CIMT in infants younger than 12 months with clinical signs of unilateral-cerebral palsy; an explorative study with randomized design. Res. Dev. Disabil. 2018, 72, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Zafer, H.; Amjad, I.; Malik, A.N.; Shaukat, E. Effectiveness of constraint induced movement therapy as compared to bimanual therapy in upper motor function outcome in child with hemiplegic cerebral palsy. Pakistan J. Med. Sci. 2016, 32, 181–184. [Google Scholar] [CrossRef]
- Dong, V.A.; Fong, K.N.K.; Chen, Y.-F.; Tseng, S.S.W.; Wong, L.M.S. ‘Remind-to-move’ treatment versus constraint-induced movement therapy for children with hemiplegic cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2017, 59, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Christmas, P.M.; Sackley, C.; Feltham, M.G.; Cummins, C. A randomized controlled trial to compare two methods of constraint-induced movement therapy to improve functional ability in the affected upper limb in pre-school children with hemiplegic cerebral palsy: CATCH TRIAL. Clin. Rehabil. 2018, 32, 909–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, S.M.S.; Sourtiji, H.; Taghizadeh, A. Effect of child friendly constraint induced movement therapy on unimanual and bimanual function in hemiplegia. Iran. Rehabil. J. 2010, 8, 50–54. [Google Scholar]
- Rostami, H.R.; Arastoo, A.A.; Nejad, S.J.; Mahany, M.K.; Malamiri, R.A.; Goharpey, S. Effects of modified constraint-induced movement therapy in virtual environment on upper-limb function in children with spastic hemiparetic cerebral palsy: A randomised controlled trial. NeuroRehabilitation 2012, 31, 357–365. [Google Scholar] [CrossRef]
- MostafaKhan, H.S.E.; Rassafiani, M.; Hosseini, S.A.; Akbarfahimi, N.; Hosseini, S.S.; Sortiji, H.; Nobakht, Z. Comparison of combination of CIMT and BIM training with CIMT alone on fine motor skills of children with Hemiplegic cerebral palsy. Iran. Rehabil. J. 2013, 11, 46–51. [Google Scholar]
- Taub, E.; Ramey, S.L.; DeLuca, S.; Echols, K. Efficacy of Constraint-Induced Movement Therapy for Children with Cerebral Palsy with Asymmetric Motor Impairment. Pediatrics 2004, 113, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Taub, E.; Griffin, A.; Uswatte, G.; Gammons, K.; Nick, J.; Law, C. Treatment of congenital hemiparesis with pediatric constraint-induced movement therapy. J. Child Neurol. 2011, 26, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Al-Oraibi, S.; Eliasson, A.C. Implementation of constraint-induced movement therapy for youngchildren with unilateral cerebral palsy in Jordan: A home-based model. Disabil. Rehabil. 2011, 33, 2006–2012. [Google Scholar] [CrossRef] [PubMed]
- Charles, J.R.; Wolf, S.L.; Schneider, J.A.; Gordon, A.M. Efficacy of a child-friendly form of constraint-induced movement therapy in hemiplegic cerebral palsy: A randomized control trial. Dev. Med. Child Neurol. 2006, 48, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, A.; Gulati, S.; Kabra, M.; Singh, U.P.; Sankhyan, N.; Pandey, R.M.; Kalra, V. Efficacy of modified constraint induced movement therapy in improving upper limb function in children with hemiplegic cerebral palsy: A randomized controlled trial. Brain Dev. 2013, 35, 870–876. [Google Scholar] [CrossRef] [PubMed]
- De Brito Brandão, M.; Mancini, M.C.; Vaz, D.V.; Pereira De Melo, A.P.; Fonseca, S.T. Adapted version of constraint-induced movement therapy promotes functioning in children with cerebral palsy: A randomized controlled trial. Clin. Rehabil. 2010, 24, 639–647. [Google Scholar] [CrossRef]
- Eugster-Buesch, F.; De Bruin, E.D.; Boltshauser, E.; Steinlin, M.; Küenzle, C.; Müller, E.; Capone, A.; Pfann, R.; Meyer-Heim, A. Forced-use therapy for children with cerebral palsy in the community setting: A single-blinded randomized controlled pilot trial. J. Pediatr. Rehabil. Med. 2012, 5, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Facchin, P.; Rosa-Rizzotto, M.; Dalla Pozza, L.V.; Turconi, A.C.; Pagliano, E.; Signorini, S.; Tornetta, L.; Trabacca, A.; Fedrizzi, E.; Valentina, A.T.; et al. Multisite trial comparing the efficacy of constraint-induced movement therapy with that of bimanual intensive training in children with hemiplegic cerebral palsy: Postintervention results. Am. J. Phys. Med. Rehabil. 2011, 90, 539–553. [Google Scholar] [CrossRef]
- Gharib, M.; Hosseyni, A.; Fahimmi, N.; Salehi, M. Effect of modified constraint induced movement therapy on quality of upper extremity skills in children with hemiplegic cerebral palsy. Iran. J. Pediatr. 2010, 12, 29–36. [Google Scholar]
- Eliasson, A.C.; Krumlinde-Sundholm, L.; Shaw, K.; Wang, C. Effects of oncstraint-induced movement therapy in young children with hemiplegic cerebral palsy: An adapted model. Dev. Med. Child Neurol. 2005, 47, 266–275. [Google Scholar] [CrossRef]
- Page, S.J.; Sisto, S.; Johnston, M.V.; Levine, P. Modified Constraint-Induced Therapy after Subacute Stroke: A Preliminary Study. Neurorehabil. Neural Repair 2002, 16, 290–295. [Google Scholar] [CrossRef]
- Peurala, S.H.; Kantanen, M.P.; Sjögren, T.; Paltamaa, J.; Karhula, M.; Heinonen, A. Effectiveness of constraint-induced movement therapy on activity and participation after stroke: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2012, 26, 209–223. [Google Scholar] [CrossRef]
- McConnell, K.; Johnston, L.; Kerr, C. Efficacy and acceptability of reduced intensity constraint-induced movement therapy for children aged 9-11 years with hemiplegic cerebral palsy: A pilot study. Phys. Occup. Ther. Pediatr. 2014, 34, 245–259. [Google Scholar] [CrossRef] [PubMed]
- Schweighofer, N.; Han, C.E.; Wolf, S.L.; Arbib, M.A.; Winstein, C.J. A Functional Threshold for Long-Term Use of Hand and Arm Function Can Be Determined: Predictions From a Computational Model and Supporting Data From the Extremity Constraint-Induced Therapy Evaluation (EXCITE) Trial. Phys. Ther. 2009, 89, 1327–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, H.C.; Ada, L. Constraint-induced movement therapy improves upper limb activity and participation in hemiplegic cerebral palsy: A systematic review. J. Physiother. 2016, 62, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eliasson, A.C.; Krumlinde-Sundholm, L.; Rösblad, B.; Beckung, E.; Arner, M.; Öhrvall, A.M.; Rosenbaum, P. The Manual Ability Classification System (MACS) for children with cerebral palsy: Scale development and evidence of validity and reliability. Dev. Med. Child Neurol. 2006, 48, 549–554. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Develpment. Experiments by Nature and Design; Harvard University Press: Cambrigdge, UK, 1979; ISBN 0674224566. [Google Scholar]
- Brown, W.H.; Odom, S.L.; Li, S.; Zercher, C. Ecobehavioral assessment in early childhood programs: A portrait of preschool inclusion. J. Spec. Educ. 1999, 33, 138–153. [Google Scholar] [CrossRef]
- Eliasson, A.; Sjöstrand, L.; Ek, L.; Krumlinde-Sundholm, L.; Tedroff, K. Efficacy of baby-CIMT:study protocol for a randomised controlled trial on infants below age 12 months, with clinical signs of unilateral CP. BMC Pediatr. 2014, 14, 141. [Google Scholar] [CrossRef] [Green Version]
- De Matteo, C.; Law, M.; Russell, D.; Pollock, N.; Rosenbaum, P.; Walter, S. The reliability and validity of the Quality of Upper Extremity Skills Test. Phys. Occup. Ther. Pediatr. 1993, 13, 1–18. [Google Scholar] [CrossRef]
- Thorley, M.; Lannin, N.; Cusick, A.; Novak, I.; Boyd, R. Reliability of the quality of upper extremity skills test for children with cerebral palsy aged 2 to 12 years. Phys. Occup. Ther. Pediatr. 2012, 32, 4–21. [Google Scholar] [CrossRef]
- Gilmore, R.; Sakzewski, L.; Boyd, R. Upper limb activity measures for 5- to 16-year-old children with congenital hemiplegia: A systematic review. Dev. Med. Child Neurol. 2010, 52, 14–21. [Google Scholar] [CrossRef]
- de Carvalho, R.M.F.; Mazzer, N.; Barbieri, C.H. Analysis of the reliability and reproducibility of goniometry compared to hand photogrammetry. Acta Ortop. Bras. 2012, 20, 139–149. [Google Scholar] [CrossRef]
- Davids, J.R.; Peace, L.C.; Wagner, L.V.; Gidewall, M.A.; Blackhurst, D.W.; Roberson, W.M. Validation of the Shriners Hospital for Children Upper Extremity Evaluation (SHUEE) for children with hemiplegic cerebral palsy. J. Bone Jt. Surg. Ser. A 2006, 88, 326–333. [Google Scholar] [CrossRef]
- IBM. SPSS Statistics for Windows, Version 20.0; IBM Corp.: Armonk, NY, USA, 2011. [Google Scholar]
- Gray, L.; Ng, H.; Bartlett, D. The gross motor function classification system: An update on impact and clinical utility. Pediatr. Phys. Ther. 2010, 22, 315–320. [Google Scholar] [CrossRef]
- Steenbergen, B.; Charles, J.; Gordon, A.M. Fingertip force control during bimanual object lifting in hemiplegic cerebral palsy. Exp. Brain Res. 2008, 186, 191–201. [Google Scholar] [CrossRef] [Green Version]
- Forssberg, H.; Eliasson, A.C.; Redon-Zouitenn, C.; Mercuri, E.; Dubowitz, L. Impaired grip-lift synergy in children with unilateral brain lesions. Brain 1999, 122, 1157–1168. [Google Scholar] [CrossRef]
- Charles, J.R.; Msw, P.T.; Physical, D. Movement Therapy Results in Further Improvement. Dev. Med. Child Neurol. 2007, 8, 770–773. [Google Scholar] [CrossRef]
- Abd El-Kafy, E.M.; Elshemy, S.A.; Alghamdi, M.S. Effect of constraint-induced therapy on upper limb functions: A randomized control trial. Scand. J. Occup. Ther. 2014, 21, 11–23. [Google Scholar] [CrossRef]
- Gordon, A.M.; Hung, Y.C.; Brandao, M.; Ferre, C.L.; Kuo, H.C.; Friel, K.; Petra, E.; Chinnan, A.; Charles, J.R. Bimanual training and constraint-induced movement therapy in children with hemiplegic cerebral palsy: A randomized trial. Neurorehabil. Neural Repair 2011, 25, 692–702. [Google Scholar] [CrossRef]
- Boyd, R.N.; Baque, E.; Piovesana, A.; Ross, S.; Ziviani, J.; Sakzewski, L.; Barber, L.; Lloyd, O.; McKinlay, L.; Whittingham, K.; et al. MitiiTM ABI: Study protocol of a randomised controlled trial of a web-based multi-modal training program for children and adolescents with an Acquired Brain Injury (ABI). BMC Neurol. 2015, 15. [Google Scholar] [CrossRef] [Green Version]
- Brusco, N.K.; Taylor, N.F.; Watts, J.J.; Shields, N. Economic evaluation of adult rehabilitation: A systematic review and meta-analysis of randomized controlled trials in a variety of settings. Arch. Phys. Med. Rehabil. 2014, 95. [Google Scholar] [CrossRef]
- Pidcock, F.; Garcia, T.; Trovato, M.; Schultz, S.; Brady, K. Pediatric constraint-induced movement therapy: A promising intervention for childhood hemiparesis. Top. Stroke Rehabil. 2009, 16, 339–345. [Google Scholar] [CrossRef]
- Ramachandran, S.; Thakur, P. Upper extremity constraint-induced movement therapy in infantile hemiplegia. J. Pediatr. Neurosci. 2011, 6, 29–31. [Google Scholar] [CrossRef]
- Argimon-Pallás, J.; Jiménez-Villa, J. Métodos de Investigación Clínica y Epidemiológica, 5th ed.; Elsevier: Barcelona, Spain, 2019; ISBN 978-84-9113-007-9. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Movements to Work in the Affected Upper Limb | Examples of mCIMT Designed Tasks |
|---|---|
| Shoulder flexion and elbow extension |
|
| Forearm supination |
|
| Wrist extension |
|
| Grasp–release |
|
| Dependent | Value 0. Needs help from an adult (does not perform the action). |
| Assisted | Value 1. Needs help from an adult (partially performs the action). |
| Independent | Value 2. Uses the healthy upper limb exclusively. |
| Value 3. Uses the upper limb to provide stability. | |
| Value 4. Uses both upper limbs to execute the action. |
| Sample | Age | Sex | Gest. Week | Lesion | MACS Level | GMFCS Level | Hemiplegia Side | Add. Impair |
|---|---|---|---|---|---|---|---|---|
| Child 1 | 4 | F | Term | Perinatal stroke | II | I | Left | No |
| Child 2 | 5 | M | Term | Perinatal stroke | II | I | Right | No |
| Child 3 | 5 | M | Preterm | Perinatal stroke | II | I | Left | No |
| Child 4 | 5 | M | Preterm | Perinatal stroke | II | I | Left | No |
| Child 5 | 7 | F | Term | Perinatal stroke | II | I | Right | Speech |
| Child 6 | 6 | F | Term | Perinatal stroke | II | I | Right | Speech |
| Child 7 | 8 | F | Preterm | Perinatal stroke | II | I | Left | Speech |
| Child 8 | 8 | M | Term | Perinatal stroke | II | I | Left | No |
| Variables | Results | Friedman’s Test | Wilcoxon’s Test | |||
|---|---|---|---|---|---|---|
| Median (IQR) | Statistical Significance | p Value | Pairwise Comparisons | Statistical Significance | p Value | |
| Quality of Movement in the Upper Limbs (Total Score) | ||||||
| Baseline | 74.16 (63.55, 83.00) | 24.000 | 0.000 * | Baseline–2nd assessment | −2.521 | 0.012 * |
| 2nd assessment | 83.32 (77.18, 88.49) | Baseline–3rd assessment | −2.521 | 0.012 * | ||
| 3rd assessment | 88.70 (84.42, 91.42) | Baseline–4th assessment | −2.521 | 0.012 * | ||
| 4th assessment | 94.07 (90.32, 94.92) | 2nd assessment–3rd assessment | −2.521 | 0.012 * | ||
| 2nd assessment–4th assessment | −2.521 | 0.012 * | ||||
| 3rd assessment–4th assessment | −2.521 | 0.012 * | ||||
| Dissociated Movements | ||||||
| Baseline | 59.38 (53.90, 80.48) | 23.538 | 0.000 * | Baseline–2nd assessment | −2.524 | 0.012 * |
| 2nd assessment | 75.00 (73.83, 82.82) | Baseline–3rd assessment | −2.521 | 0.012 * | ||
| 3rd assessment | 83.60 (81.24, 87.11) | Baseline–4th assessment | −2.521 | 0.012 * | ||
| 4th assessment | 89.84 (84.77, 91.79) | 2nd assessment–3rd assessment | −2.201 | 0.028 * | ||
| 2nd assessment–4th assessment | −2.524 | 0.012 * | ||||
| 3rd assessment–4th assessment | −2.527 | 0.012 * | ||||
| Grasp | ||||||
| Baseline | 62.97 (46.30, 76.86) | 21.808 | 0.000 * | Baseline–2nd assessment | −2.533 | 0.011 * |
| 2nd assessment | 79.60 (59.26, 87.96) | Baseline–3rd assessment | −2.527 | 0.012 * | ||
| 3rd assessment | 87.03 (63.89, 91.67) | Baseline–4th assessment | −2.527 | 0.012 * | ||
| 4th assessment | 96.30 (75.00, 96.30) | 2nd assessment–3rd assessment | −2.200 | 0.028 * | ||
| 2nd assessment–4th assessment | −2.384 | 0.017 * | ||||
| 3rd assessment–4th assessment | −2.384 | 0.017 * | ||||
| Weight Bearing | ||||||
| Baseline | 87.00 (76.50, 93.50) | 19.154 | 0.000 * | Baseline–2nd assessment | −2.536 | 0.011 * |
| 2nd assessment | 98.00 (85.50, 99.50) | Baseline–3rd assessment | −2.524 | 0.012 * | ||
| 3rd assessment | 97.00 (93.00, 99.50) | Baseline–4th assessment | −2.521 | 0.012 * | ||
| 4th assessment | 99.00 (96.00, 100.00) | 2nd assessment–3rd assessment | −1.461 | 0.144 | ||
| 2nd assessment–4th assessment | −1.461 | 0.102 | ||||
| 3rd assessment–4th assessment | −1.604 | 0.109 | ||||
| Protective Extension | ||||||
| Baseline | 80.56 (75.00, 90.27) | 17.431 | 0.001 * | Baseline–2nd assessment | −1.841 | 0.066 |
| 2nd assessment | 83.34 (79.17, 96.53) | Baseline–3rd assessment | −2.207 | 0.027 * | ||
| 3rd assessment | 90.27 (84.73, 97.92) | Baseline–4th assessment | −2.379 | 0.017 * | ||
| 4th assessment | 94.44 (92.36, 99.31) | 2nd assessment–3rd assessment | −1.826 | 0.068 | ||
| 2nd assessment–4th assessment | −2.207 | 0.027 * | ||||
| 3rd assessment–4th assessment | −2.023 | 0.043 * | ||||
| Variable: Grasp Strength | Results | Friedman Test | Wilcoxon Test | |||
|---|---|---|---|---|---|---|
| Median (IQR) | Statistical Significance | p Value | Pairwise Comparisons | Statistical Significance | p Value | |
| Baseline | 2.00 (1.00, 2.75) | 20.069 | 0.000 * | Baseline–2nd assessment | 0.000 | 1.000 |
| 2nd assessment | 2.00 (1.00, 2.75) | Baseline–3rd assessment | −2.000 | 0.046 * | ||
| 3rd assessment | 2.00 (1.25, 3.75) | Baseline–4th assessment | −2.640 | 0.008 * | ||
| 4th assessment | 3.00 (2.25, 4.50) | 2nd assessment–3rd assessment | −2.000 | 0.046 * | ||
| 2nd assessment–4th assessment | −2.640 | 0.008 * | ||||
| 3rd assessment–4th assessment | −2.449 | 0.014 * | ||||
| Variables: Active Elbow Extension | Results | Friedman Test | Wilcoxon Test | |||
|---|---|---|---|---|---|---|
| Median (IQR) | Statistical Significance | p Value | Pairwise Comparisons | Statistical | p Value | |
| Baseline | 12.50 (10.00, 43.75) | 23.423 | 0.000 * | Baseline–2nd assessment | −2.565 | 0.010 * |
| 2nd assessment | 22.50 (20.00, 50.00) | Baseline–3rd assessment | −2.533 | 0.011 * | ||
| 3rd assessment | 27.50 (22.75, 54.50) | Baseline–4th assessment | −2.536 | 0.011 * | ||
| 4th assessment | 33.50 (25.75, 64.25) | 2nd Assessment–3rd assessment | −2.456 | 0.014 * | ||
| 2nd assessment–4th assessment | −2.536 | 0.011 * | ||||
| 3rd assessment–4th assessment | −2.375 | 0.018 * | ||||
| Active Forearm Supination | ||||||
| Baseline | 70.00 (35.50, 75.00) | 23.416 | 0.000 * | Baseline–2nd assessment | −2.588 | 0.010 * |
| 2nd assessment | 75.00 (45.00, 80.00) | Baseline–3rd assessment | −2.536 | 0.011 * | ||
| 3rd assessment | 76.50 (53.50, 82.25) | Baseline–4th assessment | −2.524 | 0.012 * | ||
| 4th assessment | 81.50 (58.75, 87.75) | 2nd Assessment–3rd assessment | −2.032 | 0.042 * | ||
| 2nd assessment–4th assessment | −2.536 | 0.011 * | ||||
| 3rd assessment–4th assessment | −2.527 | 0.012 * | ||||
| Variable | Results | Friedman’s Test | Wilcoxon’s Test | |||
|---|---|---|---|---|---|---|
| Spontaneous Use in the Affected Upper Limb | Median (IQR) | Statistical Significance | p Value | Pairwise Comparisons | Statistical Significance | p Value |
| Baseline | 70.00 (49.45, 87.78) | 18.932 | 0.000 * | Baseline–2nd assessment | −2.371 | 0.018 * |
| 2nd assessment | 85.56 (58.34, 95.00) | Baseline–3rd assessment | −2.366 | 0.018 * | ||
| 3rd assessment | 87.78 (72.78, 95.55) | Baseline–4th assessment | −2.521 | 0.012 * | ||
| 4th assessment | 88.87 (87.11, 97.22) | 2nd assessment–3rd assessment | −2.201 | 0.028 * | ||
| 2nd assessment–4th assessment | −1.963 | 0.050 | ||||
| 3rd assessment–4th assessment | −1.690 | 0.091 | ||||
| Dynamic Joint Position | ||||||
| Baseline | 77.78 (48.24, 86.81) | 23.416 | 0.000 * | Baseline–2nd assessment | −2.366 | 0.018 * |
| 2nd assessment | 80.56 (75.35, 89.93) | Baseline–3rd assessment | −2.521 | 0.012 * | ||
| 3rd assessment | 85.44 (71.87, 9132) | Baseline–4th assessment | −2.521 | 0.012 * | ||
| 4th assessment | 88.20 (84.03, 92.71) | 2nd assessment–3rd assessment | −1.183 | 0.237 | ||
| 2nd assessment–4th assessment | −2.366 | 0.018 * | ||||
| 3rd assessment–4th assessment | −2.023 | 0.043 * | ||||
| Grasp–Release action | ||||||
| Baseline | 58.34 (50.00, 91.67) | 13.568 | 0.004 * | Baseline–2nd assessment | −1.414 | 0.157 |
| 2nd assessment | 75.00 (54.17, 95.83) | Baseline–3rd assessment | −1.890 | 0.059 | ||
| 3rd assessment | 83.33 (66.67, 100.00) | Baseline–4th assessment | −2.226 | 0.026 * | ||
| 4th assessment | 91.67 (83.33, 100.00) | 2nd assessment–3rd assessment | −1.342 | 0.180 | ||
| 2nd assessment–4th assessment | −2.041 | 0.041 * | ||||
| 3rd assessment–4th assessment | −1.857 | 0.063 | ||||
| Variable | Results | Friedman’s Test | Wilcoxon’s Test | |||
|---|---|---|---|---|---|---|
| Upper Limb Dressing | Median (IQR) | Statistical Significance | p Value | Pairwise Comparisons | Statistical Significance | p Value |
| Baseline | 3.50 (2.25, 4.00) | 10.355 | 0.016 * | Baseline–2nd assessment | 0.000 | 1.000 |
| 2nd assessment | 3.50 (2.25, 4.00) | Baseline–3rd assessment | −1.633 | 0.102 | ||
| 3rd assessment | 4.00 (3.25, 4.00) | Baseline–4th assessment | −1.857 | 0.063 | ||
| 4th assessment | 4.00 (4.00, 4.00) | 2nd assessment–3rd assessment | −1.633 | 0.102 | ||
| 2nd assessment–4th assessment | −1.857 | 0.063 | ||||
| 3rd assessment–4th assessment | −1.414 | 0.157 | ||||
| Lower Limb Dressing | ||||||
| Baseline | 3.00 (2.25, 3.00) | 15.245 | 0.002 * | Baseline–2nd assessment | −1.414 | 0.157 |
| 2nd assessment | 3.00 (3.00, 3.75) | Baseline–3rd assessment | −2.000 | 0.046 * | ||
| 3rd assessment | 3.00 (3.00, 4.00) | Baseline–4th assessment | −2.530 | 0.011 * | ||
| 4th assessment | 4.00 (4.00, 4.00) | 2nd assessment–3rd assessment | −1.414 | 0.157 | ||
| 2nd assessment–4th assessment | −2.449 | 0.014 * | ||||
| 3rd assessment–4th assessment | −2.000 | 0.046 * | ||||
| Putting on Splints | ||||||
| Baseline | 3.00 (1.00, 3.75) | 9.923 | 0.019 * | Baseline–2nd assessment | 0.000 | 1.000 |
| 2nd assessment | 3.00 (1.00, 3.75) | Baseline–3rd assessment | −1.633 | 0.102 | ||
| 3rd assessment | 3.00 (1.00, 4.00) | Baseline–4th assessment | −1.857 | 0.063 | ||
| 4th assessment | 4.00 (1.50, 4.00) | 2nd assessment–3rd assessment | −1.633 | 0.102 | ||
| 2nd assessment–4th assessment | −1.857 | 0.063 | ||||
| 3rd assessment–4th assessment | −1.414 | 0.157 | ||||
| Putting on Shoes | ||||||
| Baseline | 2.00 (2.00, 3.50) | 15.188 | 0.002 * | Baseline–2nd assessment | −1.000 | 0.317 |
| 2nd assessment | 2.00 (2.00, 3.75) | Baseline–3rd assessment | −2.121 | 0.034 * | ||
| 3rd assessment | 3.00 (3.00, 4.00) | Baseline–4th assessment | −2.271 | 0.023 * | ||
| 4th assessment | 4.00 (3.25, 4.00) | 2nd assessment–3rd assessment | −1.890 | 0.059 | ||
| 2nd assessment–4th assessment | −2.251 | 0.024 * | ||||
| 3rd assessment–4th assessment | −1.633 | 0.102 | ||||
| Putting on Socks | ||||||
| Baseline | 3.00 (3.00, 3.75) | 15.000 | 0.002 * | Baseline–2nd assessment | 0.000 | 1.000 |
| 2nd assessment | 3.00 (3.00, 3.75) | Baseline–3rd assessment | −2.000 | 0.046 * | ||
| 3rd assessment | 3.00 (3.00, 4.00) | Baseline–4th assessment | −2.333 | 0.020 * | ||
| 4th assessment | 4.00 (4.00, 4.00) | 2nd assessment–3rd assessment | −2.000 | 0.046 * | ||
| 2nd assessment–4th assessment | −2.333 | 0.020 * | ||||
| 3rd assessment–4th assessment | −1.732 | 0.083 | ||||
| Buttoning Up | ||||||
| Baseline | 1.00 (0.00, 3.00) | 5.118 | 0.163 | Baseline–2nd assessment | −1.000 | 0.317 |
| 2nd assessment | 1.50 (0.00, 3.00) | Baseline–3rd assessment | −1.414 | 0.157 | ||
| 3rd assessment | 1.50 (0.00, 3.75) | Baseline–4th assessment | −1.342 | 0.180 | ||
| 4th assessment | 1.50 (0.00, 4.00) | 2nd assessment–3rd assessment | −1.000 | 0.317 | ||
| 2nd assessment–4th assessment | −1.414 | 0.157 | ||||
| 3rd assessment–4th assessment | −1.000 | 0.317 | ||||
| Personal Hygiene | ||||||
| Baseline | 2.00 (2.00, 2.00) | 15.000 | 0.002 * | Baseline–2nd assessment | 0.000 | 1.000 |
| 2nd assessment | 2.00 (2.00, 2.00) | Baseline–3rd assessment | −1.890 | 0.059 | ||
| 3rd assessment | 2.50 (2.00, 4.00) | Baseline–4th assessment | −2.333 | 0.020 * | ||
| 4th assessment | 4.00 (2.25, 4.00) | 2nd assessment–3rd assessment | −1.890 | 0.059 | ||
| 2nd assessment–4th assessment | −2.333 | 0.020 * | ||||
| 3rd assessment–4th assessment | −1.633 | 0.102 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomo-Carrión, R.; Romero-Galisteo, R.-P.; Pinero-Pinto, E.; López-Muñoz, P.; Romay-Barrero, H.; José, F.G.-M.S. Application of Low-Intensity Modified Constraint-Induced Movement Therapy to Improve the Affected Upper Limb Functionality in Infantile Hemiplegia with Moderate Manual Ability: Case Series. Children 2020, 7, 127. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090127
Palomo-Carrión R, Romero-Galisteo R-P, Pinero-Pinto E, López-Muñoz P, Romay-Barrero H, José FG-MS. Application of Low-Intensity Modified Constraint-Induced Movement Therapy to Improve the Affected Upper Limb Functionality in Infantile Hemiplegia with Moderate Manual Ability: Case Series. Children. 2020; 7(9):127. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090127
Chicago/Turabian StylePalomo-Carrión, Rocío, Rita-Pilar Romero-Galisteo, Elena Pinero-Pinto, Purificación López-Muñoz, Helena Romay-Barrero, and Francisco García-Muro San José. 2020. "Application of Low-Intensity Modified Constraint-Induced Movement Therapy to Improve the Affected Upper Limb Functionality in Infantile Hemiplegia with Moderate Manual Ability: Case Series" Children 7, no. 9: 127. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090127