Patterns of Urinary Neutrophil Gelatinase-Associated Lipocalin and Acute Kidney Injury in Neonates Receiving Cardiopulmonary Bypass

Abstract
:1. Introduction
2. Materials and Methods
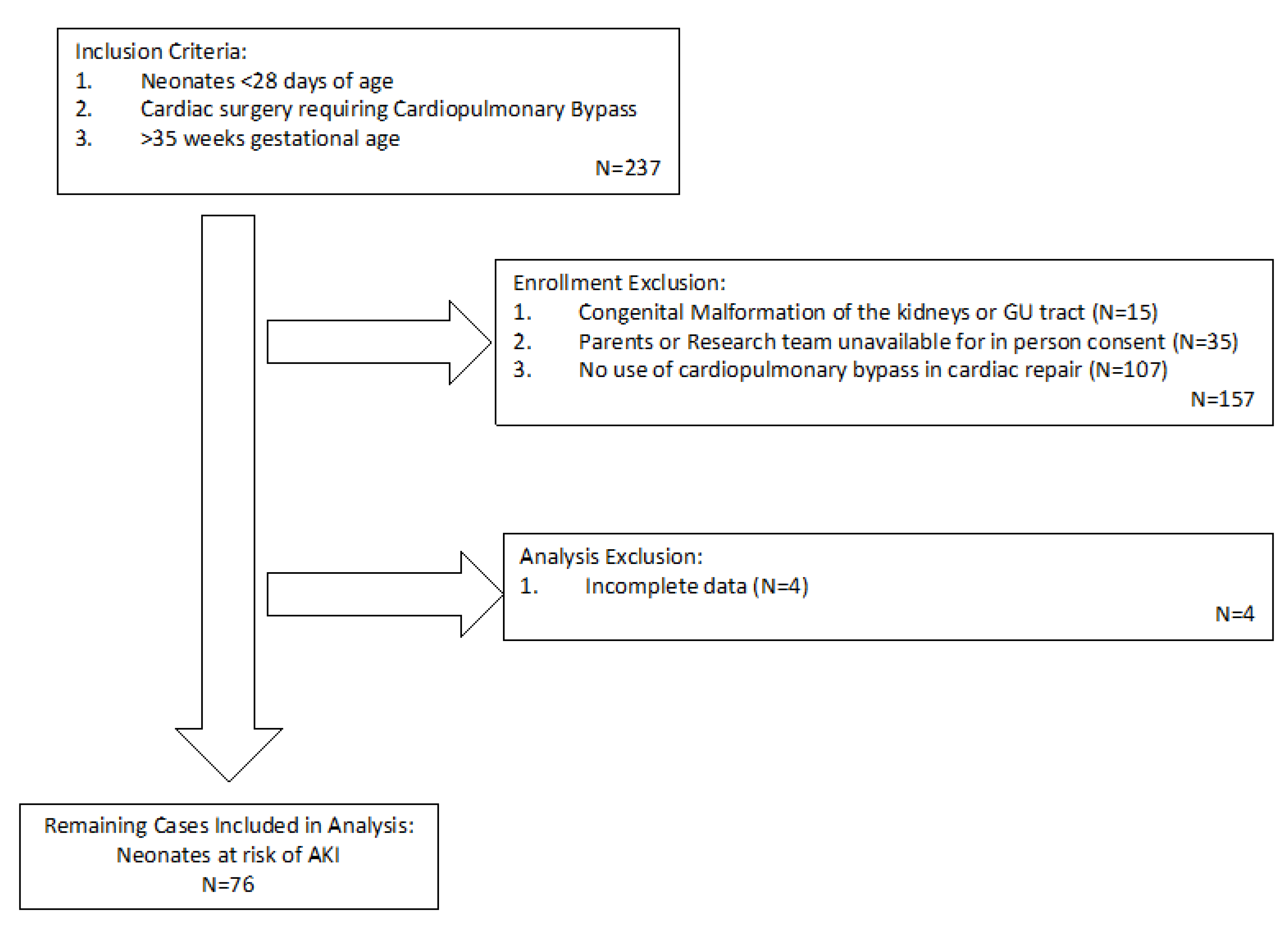
2.1. Subjects and Study Design
2.2. Protocol
2.3. Power Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Akcan-Arikan, A.; Zappitelli, M.; Loftis, L.; Washburn, K.; Jefferson, L.; Goldstein, S. Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int. 2007, 71, 1028–1035. [Google Scholar] [CrossRef] [Green Version]
- Hoste, E.; Clermont, G.; Kersten, A.; Venkataraman, R.; Angus, D.C.; De Bacquer, D.; A Kellum, J. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: A cohort analysis. Crit. Care 2006, 10, R73. [Google Scholar] [CrossRef] [Green Version]
- Askenazi, D.J.; Ambalavanan, N.; Goldstein, S.L. Acute kidney injury in critically ill newborns: What do we know? What do we need to learn? Pediatr. Nephrol. 2009, 24, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Selewski, D.T.; Charlton, J.R.; Jetton, J.G.; Guillet, R.; Mhanna, M.J.; Askenazi, D.J.; Kent, A.L. Neonatal Acute Kidney Injury. Pediatrics 2015, 136, e463–e473. [Google Scholar] [CrossRef] [Green Version]
- Zappitelli, M.; Ambalavanan, N.; Askenazi, D.J.; Moxey-Mims, M.M.; Kimmel, P.L.; Star, R.A.; Abitbol, C.L.; Brophy, P.D.; Hidalgo, G.; Hanna, M.; et al. Developing a neonatal acute kidney injury research definition: A report from the NIDDK neonatal AKI workshop. Pediatr. Res. 2017, 82, 569–573. [Google Scholar] [CrossRef]
- Jetton, J.G.; Boohaker, L.J.; Sethi, S.K.; Wazir, S.; Rohatgi, S.; Soranno, D.E.; Chishti, A.S.; Woroniecki, R.; Mammen, C.; Swanson, J.R.; et al. Incidence and outcomes of neonatal acute kidney injury (AWAKEN): A multicentre, multinational, observational cohort study. Lancet Child Adolesc. Health 2017, 1, 184–194. [Google Scholar] [CrossRef]
- Li, S.; Krawczeski, C.D.; Zappitelli, M.; Devarajan, P.; Thiessen-Philbrook, H.; Coca, S.; Kim, R.W.; Parikh, C.R. Incidence, risk factors, and outcomes of acute kidney injury after pediatric cardiac surgery: A prospective multicenter study. Crit. Care Med. 2011, 39, 1493–1499. [Google Scholar] [CrossRef] [Green Version]
- Zappitelli, M.; Bernier, P.-L.; Saczkowski, R.S.; Tchervenkov, C.I.; Gottesman, R.; Dancea, A.; Hyder, A.; Alkandari, O. A small post-operative rise in serum creatinine predicts acute kidney injury in children undergoing cardiac surgery. Kidney Int. 2009, 76, 885–892. [Google Scholar] [CrossRef] [Green Version]
- Blinder, J.J.; Goldstein, S.L.; Lee, V.-V.; Baycroft, A.; Fraser, C.D.; Nelson, D.; Jefferies, J.L. Congenital heart surgery in infants: Effects of acute kidney injury on outcomes. J. Thorac. Cardiovasc. Surg. 2012, 143, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; et al. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Hazle, M.A.; Gajarski, R.J.; Aiyagari, R.; Yu, S.; Abraham, A.; Donohue, J.; Blatt, N.B. Urinary biomarkers and renal near-infrared spectroscopy predict intensive care unit outcomes after cardiac surgery in infants younger than 6 months of age. J. Thorac. Cardiovasc. Surg. 2013, 146, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Bueva, A.; Guignard, J.-P. Renal function in preterm neonates. Pediatr. Res. 1994, 36, 572–577. [Google Scholar] [CrossRef] [Green Version]
- Bojan, M.; Vicca, S.; Lopez-Lopez, V.; Mogenet, A.; Pouard, P.; Falissard, B.; Journois, D. Predictive performance of urine neutrophil gelatinase-associated lipocalin for dialysis requirement and death following cardiac surgery in neonates and infants. Clin. J. Am. Soc. Nephrol. 2013, 9, 285–294. [Google Scholar] [CrossRef] [Green Version]
- Parravicini, E.; Locatelli, C.; Lorenz, J.M.; Nemerofsky, S.L.; Bateman, D.A. Is urinary neutrophil gelatinase-associated lipocalin able to predict acute kidney injury episodes in very low birth weight infants in clinical settings? Pediatr. Res. 2016, 80, 663–667. [Google Scholar] [CrossRef]
- Jetton, J.G.; Askenazi, D.J. Update on acute kidney injury in the neonate. Curr. Opin. Pediatr. 2012, 24, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, K.J.; Gauvreau, K.; Newburger, J.W.; Spray, T.L.; Moller, J.H.; Iezzoni, L.I. Consensus-based method for risk adjustment for surgery for congenital heart disease. J. Thorac. Cardiovasc. Surg. 2002, 123, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Huynh, T.K.; Bateman, D.A.; Parravicini, E.; Lorenz, J.M.; Nemerofsky, S.L.; Sise, M.E.; Bowman, T.M.; Polesana, E.; Barasch, J.M. Reference values of urinary neutrophil gelatinase-associated lipocalin in very low birth weight infants. Pediatr. Res. 2009, 66, 528–532. [Google Scholar] [CrossRef] [Green Version]
- Mishra, J.; Dent, C.; Tarabishi, R.; Mitsnefes, M.M.; Ma, Q.; Kelly, C.; Ruff, S.M.; Zahedi, K.; Shao, M.; Bean, J.; et al. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet 2005, 365, 1231–1238. [Google Scholar] [CrossRef]
- Krawczeski, C.D.; Woo, J.G.; Wang, Y.; Bennett, M.R.; Ma, Q.; Devarajan, P. Neutrophil gelatinase-associated lipocalin concentrations predict development of acute kidney injury in neonates and children after cardiopulmonary bypass. J. Pediatr. 2011, 158, 1009–1015.e1. [Google Scholar] [CrossRef]
- Kamianowska, M.; Wasilewska, A.; Szczepański, M.; Kulikowska, E.; Bebko, B.; Koput, A. Health term-born girls had higher levels of urine neutrophil gelatinase-associated lipocalin than boys during the first postnatal days. Acta Paediatr. 2016, 105, 1105–1108. [Google Scholar] [CrossRef]
- Bateman, D.A.; Thomas, W.; Parravicini, E.; Polesana, E.; Locatelli, C.; Lorenz, J.M. Serum creatinine concentration in very-low-birth-weight infants from birth to 34-36 wk postmenstrual age. Pediatr. Res. 2015, 77, 696–702. [Google Scholar] [CrossRef] [Green Version]
- Alabbas, A.; Campbell, A.; Skippen, P.W.; Human, D.; Matsell, U.G.; Mammen, C. Epidemiology of cardiac surgery-associated acute kidney injury in neonates: A retrospective study. Pediatr. Nephrol. 2013, 28, 1127–1134. [Google Scholar] [CrossRef]
- Morgan, C.; Zappitelli, M.; Robertson, C.M.; Alton, G.Y.; Sauve, R.S.; Joffe, A.R.; Ross, D.B.; Rebeyka, I.M. Risk factors for and outcomes of acute kidney injury in neonates undergoing complex cardiac surgery. J. Pediatr. 2013, 162, 120–127.e1. [Google Scholar] [CrossRef]
- Krawczeski, C.D.; Goldstein, S.L.; Woo, J.G.; Wang, Y.; Piyaphanee, N.; Ma, Q.; Bennett, M.; Devarajan, P. Temporal relationship and predictive value of urinary acute kidney injury biomarkers after pediatric cardiopulmonary bypass. J. Am. Coll. Cardiol. 2011, 58, 2301–2309. [Google Scholar] [CrossRef] [Green Version]
- Lynch, J.M.; Ko, T.; Busch, D.R.; Newland, J.J.; Winters, M.E.; Mensah-Brown, K.; Boorady, T.W.; Xiao, R.; Nicolson, S.C.; Montenegro, L.M.; et al. Preoperative cerebral hemodynamics from birth to surgery in neonates with critical congenital heart disease. J. Thorac. Cardiovasc. Surg. 2018, 156, 1657–1664. [Google Scholar] [CrossRef]
- Lynch, J.M.; Buckley, E.M.; Schwab, P.J.; McCarthy, A.L.; Winters, M.E.; Busch, D.R.; Xiao, R.; Goff, N.A.; Nicolson, S.C.; Montenegro, L.M.; et al. Time to surgery and preoperative cerebral hemodynamics predict postoperative white matter injury in neonates with hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2014, 148, 2181–2188. [Google Scholar] [CrossRef] [Green Version]
- Adams, P.S.; Vargas, D.; Baust, T.; Saenz, L.; Koh, W.; Blasiole, B.; Callahan, P.M.; Phadke, A.S.; Nguyen, K.; Domnina, Y.; et al. Associations of Perioperative Renal Oximetry Via Near-Infrared Spectroscopy, Urinary Biomarkers, and Postoperative Acute Kidney Injury in Infants After Congenital Heart Surgery: Should Creatinine Continue to Be the Gold Standard? Pediatr. Crit. Care Med. 2019, 20, 27–37. [Google Scholar] [CrossRef]
- Ruf, B.; Bonelli, V.; Balling, G.; Hörer, J.; Nagdyman, N.; Braun, S.L.; Ewert, P.; Reiter, K. Intraoperative renal near-infrared spectroscopy indicates developing acutee kidney injury in infants undergoing cardiac surgery with cardiopulmonary bypass: A case-control study. Crit. Care 2015, 19, 27. [Google Scholar] [CrossRef] [Green Version]
- Parikh, C.R.; Devarajan, P.; Zappitelli, M.; Sint, K.; Thiessen-Philbrook, H.; Li, S.; Kim, R.W.; Koyner, J.L.; Coca, S.; Edelstein, C.L.; et al. Postoperative Biomarkers Predict Acute Kidney Injury and Poor Outcomes after Pediatric Cardiac Surgery. J. Am. Soc. Nephrol. 2011, 22, 1737–1747. [Google Scholar] [CrossRef] [Green Version]
- Bennett, M.; Dent, C.L.; Ma, Q.; Dastrala, S.; Grenier, F.; Workman, R.; Syed, H.; Ali, S.; Barasch, J.; Devarajan, P. Urine NGAL predicts severity of acute kidney injury after cardiac surgery: A prospective study. Clin. J. Am. Soc. Nephrol. 2008, 3, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Basu, R.K.; Wong, H.R.; Krawczeski, C.D.; Wheeler, D.S.; Manning, P.B.; Chawla, L.S.; Devarajan, P.; Goldstein, S.L. Combining functional and tubular damage biomarkers improves diagnostic precision for acute kidney injury after cardiac surgery. J. Am. Coll. Cardiol. 2014, 64, 2753–2762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zappitelli, M.; Greenberg, J.H.; Coca, S.; Krawczeski, C.D.; Li, S.; Thiessen-Philbrook, H.R.; Bennett, M.R.; Devarajan, P.; Parikh, C.R. Association of Definition of Acute Kidney Injury by Cystatin C Rise With Biomarkers and Clinical Outcomes in Children. JAMA Pediatr. 2015, 169, 583–591. [Google Scholar] [CrossRef]
- Surmiak, P.; Baumert, M.; Fiala, M.; Walencka, Z.; Więcek, A. Umbilical Neutrophil Gelatinase-Associated Lipocalin Level as an Early Predictor of Acute Kidney Injury in Neonates with Hypoplastic Left Heart Syndrome. BioMed Res. Int. 2015, 2015, 360209. [Google Scholar] [CrossRef]
- Saeidi, B.; Koralkar, R.; Griffin, R.L.; Halloran, B.; Ambalavanan, N.; Askenazi, D.J. Impact of gestational age, sex, and postnatal age on urine biomarkers in premature neonates. Pediatr. Nephrol. 2015, 30, 2037–2044. [Google Scholar] [CrossRef]
- Bennett, M.R.; Nehus, E.; Haffner, C.; Ma, Q.; Devarajan, P. Pediatric Reference Ranges for Acute Kidney Injury Biomarkers. Pediatr. Nephrol. 2015, 30, 677–685. [Google Scholar] [CrossRef] [Green Version]
- Askenazi, D.J.; Koralkar, R.; Levitan, E.B.; Goldstein, S.L.; Devarajan, P.; Khandrika, S.; Mehta, R.L.; Ambalavanan, N. Baseline values of candidate urine acute kidney injury biomarkers vary by gestational age in premature infants. Pediatr. Res. 2011, 70, 302–306. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, J.H.; Parikh, C.R. Biomarkers for diagnosis and prognosis of AKI in children: One size does not fit all. Clin. J. Am. Soc. Nephrol. 2017, 12, 1551–1557. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A. Accuracy of neutrophil gelatinase-associated lipocalin (NGAL) in diagnosis and prognosis in acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [CrossRef] [Green Version]
- Brion, L.P.; Fleischman, A.R.; McCarton, C.; Schwartz, G.J. A simple estimate of glomerular filtration rate in low birth weight infants during the first year of life: Noninvasive assessment of body composition and growth. J. Pediatr. 1986, 109, 698–707. [Google Scholar] [CrossRef]
- SooHoo, M.; Patel, S.S.; Jaggers, J.; Faubel, S.; Gist, K.M. Acute Kidney Injury Defined by Fluid Corrected Creatinine in Neonates After the Norwood Procedure. World J. Pediatr. Congenit. Hear. Surg. 2018, 9, 513–521. [Google Scholar] [CrossRef]
- Askenazi, D.J.; Saeidi, B.; Koralkar, R.; Ambalavanan, N.; Griffin, R.L. Acute changes in fluid status affect the incidence, associative clinical outcomes and urine biomarker performance in premature infants with acute kidney injury. Pediatr. Nephrol. 2015, 31, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Askenazi, D.; Abitbol, C.; Boohaker, L.; Griffin, R.; Raina, R.; Dower, J.; Davis, T.K.; Ray, P.E.; Perazzo, S.; DeFreitas, M.; et al. Optimizing the AKI definition during first postnatal week using Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates (AWAKEN) cohort. Pediatr. Res. 2018, 85, 329–338. [Google Scholar] [CrossRef]
- Pynn, J.M.; Parravicini, E.; Saiman, L.; Bateman, D.A.; Barasch, J.M.; Lorenz, J.M. Urinary Neutrophil Gelatinase-Associated Lipocalin: Potential Biomarker for Late Onset Sepsis. Pediatr. Res. 2015, 78, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parravicini, E.; Nemerofsky, S.L.; Michelson, K.A.; Huynh, T.K.; Sise, M.E.; Bateman, D.A.; Lorenz, J.M.; Barasch, J.M. Neutrophil Gelatinase-Associated Lipocalin is a promising biomarker for late onset culture-positive sepsis in very low birth weight infants. Pediatr. Res. 2010, 67, 636–640. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| AKI n = 17 | No AKI n = 59 | Total n = 76 | p-Value | |
|---|---|---|---|---|
| Categorical variables, n (%) | ||||
| Male sex | 12 (71) | 37 (63) | 53 (70) | 0.55 |
| Elevated baseline uNGAL >50 ng/mL | 4 (33) | 15 (33) | 19 (33) | 0.99 |
| Elevated baseline uNGAL >100 ng/mL | 2 (25) | 12 (26) | 15 (26) | 0.99 |
| Lower post-operative sCr | 5 (29) | 29 (49) | 34 (45) | 0.15 |
| RACHS-1 score | 0.83 | |||
| Scores 2–3 | 4 (24) | 17 (29) | 21 (28) | |
| Score 4 | 8 (47) | 22 (37) | 30 (39) | |
| Scores 5–6 | 5 (29) | 20 (34) | 25 (33) | |
| Continuous variables, median [IQR] | ||||
| Birthweight (kg) | 3.03 [2.87–3.23] | 3.23 [2.97–3.59] | 3.19 [2.94–3.54] | 0.15 |
| Gestational age (wk) | 38 [37–39] | 39 [38, 39] | 39 [38, 39] | 0.15 |
| Age at surgery (d) | 7 [6–11] | 5 [4–7] | 6 [4–8] | 0.01 |
| Baseline sCr (mg/dL) | 0.46 [0.37–0.60] | 0.50 [0.40–0.64] | 0.50 [0.38–0.64] | 0.51 |
| Baseline uNGAL (ng/mL) | 19 [8–90] | 22 [8–98] | 22 [8–98] | 0.64 |
| Peak uNGAL (ng/mL) | 763 [454–1256] | 319 [119–807] | 436 [125–845] | 0.03 |
| Bypass time (min) | 137 [114–173] | 156 [120.5–182] | 155 [120–182] | 0.51 |
| Cross-clamp time (min) | 76 [56.5–100.5] | 83 [66–101] | 82 [63–102] | 0.52 |
| ACP time (min) | 53 [47.75–58.25] | 55 [30–57.5] | 55 [32–58] | 0.76 |
| Circulatory arrest time (min) | 29 [12–46.5] | 24 [8–36] | 25 [8–38.25] | 0.51 |
| KDIGO Criteria | |||
|---|---|---|---|
| KDIGO Staging | Increased Creatinine | Oliguria | Total (n = 17) |
| Stage 1 | 9 | 3 | 9 |
| Stage 2 | 6 | 3 | 6 |
| Stage 3 | 2 | 2 | 2 |
| Median uNGAL [IQR a] (ng/mL) | Logistic Regression Models b | ||||
|---|---|---|---|---|---|
| Time (h) | AKI | No AKI | p-Value c | OR (95% CI) | p-Value |
| 0 | 19 [8, 90] | 22 [8, 90] | 0.64 | 1.02 (0.65, 1.59) | 0.93 |
| 3 | 70 [28, 662] | 226 [72, 468] | 0.35 | 0.86 (0.57, 1.34) | 0.49 |
| 4 | 230 [24, 459] | 149 [44, 444] | 0.89 | 1.05 (0.71, 1.60) | 0.79 |
| 7 | 361 [106, 838] | 76 [25, 196] | 0.01 | 2.22 (1.34, 4.08) | 0.004 |
| 10 | 405 [107, 773] | 63 [24, 185] | 0.003 | 3.48 (1.58, 8.71) | 0.002 |
| 13 | 259 [41, 570] | 54 [23, 158] | 0.02 | 2.15 (1.25, 4.10) | 0.01 |
| 16 | 61 [42, 470] | 40 [18, 72] | 0.03 | 1.95 (1.14, 3.60) | 0.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brennan, K.G.; Parravicini, E.; Lorenz, J.M.; Bateman, D.A. Patterns of Urinary Neutrophil Gelatinase-Associated Lipocalin and Acute Kidney Injury in Neonates Receiving Cardiopulmonary Bypass. Children 2020, 7, 132. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090132
Brennan KG, Parravicini E, Lorenz JM, Bateman DA. Patterns of Urinary Neutrophil Gelatinase-Associated Lipocalin and Acute Kidney Injury in Neonates Receiving Cardiopulmonary Bypass. Children. 2020; 7(9):132. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090132
Chicago/Turabian StyleBrennan, Kathleen G., Elvira Parravicini, John M. Lorenz, and David A. Bateman. 2020. "Patterns of Urinary Neutrophil Gelatinase-Associated Lipocalin and Acute Kidney Injury in Neonates Receiving Cardiopulmonary Bypass" Children 7, no. 9: 132. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090132