Association between Exercise-Induced Changes in Cardiorespiratory Fitness and Adiposity among Overweight and Obese Youth: A Meta-Analysis and Meta-Regression Analysis


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search
2.3. Study Selection and Data Collection Process
2.4. Risk of Bias in Individual Studies
2.5. Synthesis of Results
3. Results
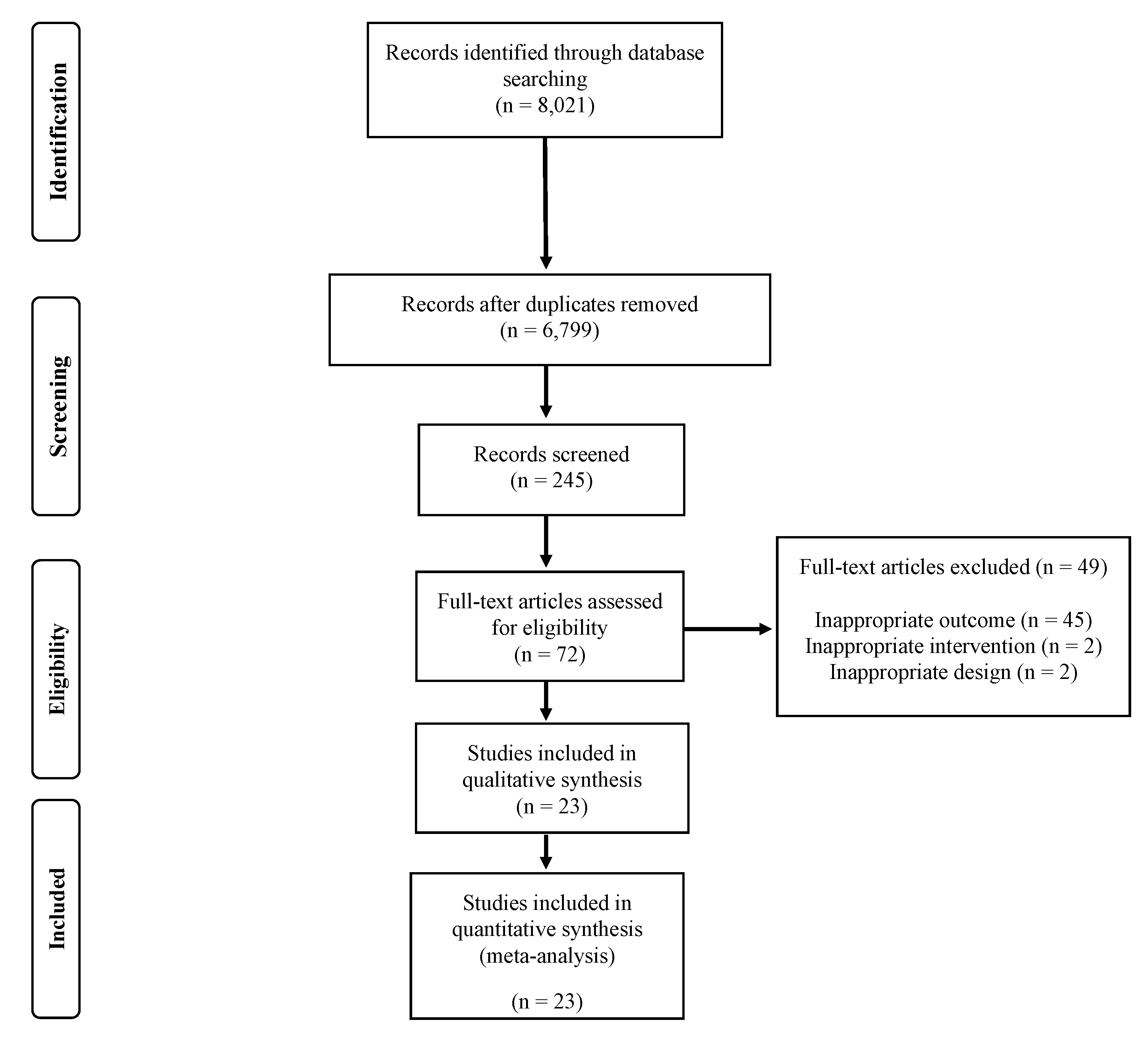
3.1. Study Selection
3.2. Study Characteristics
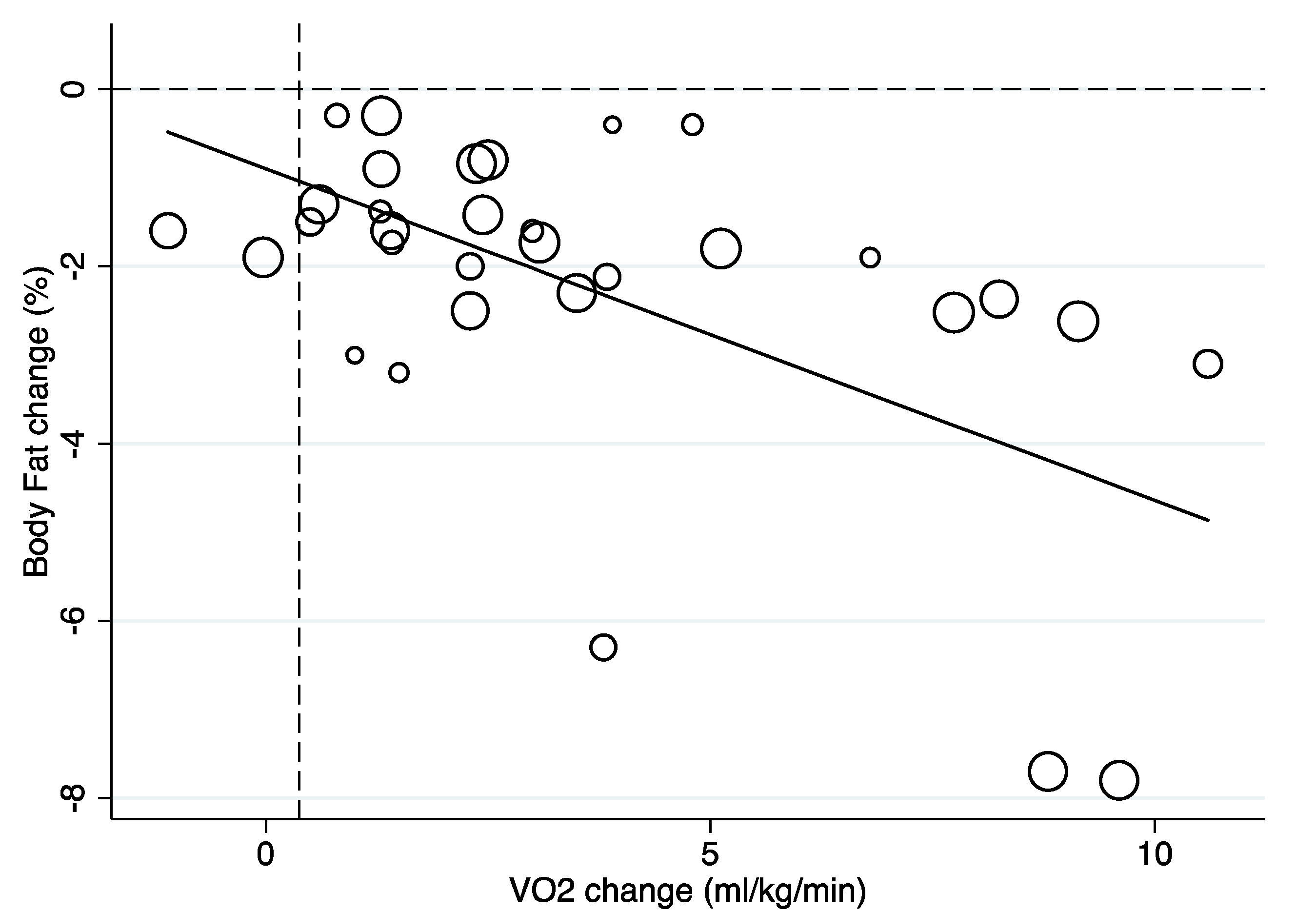
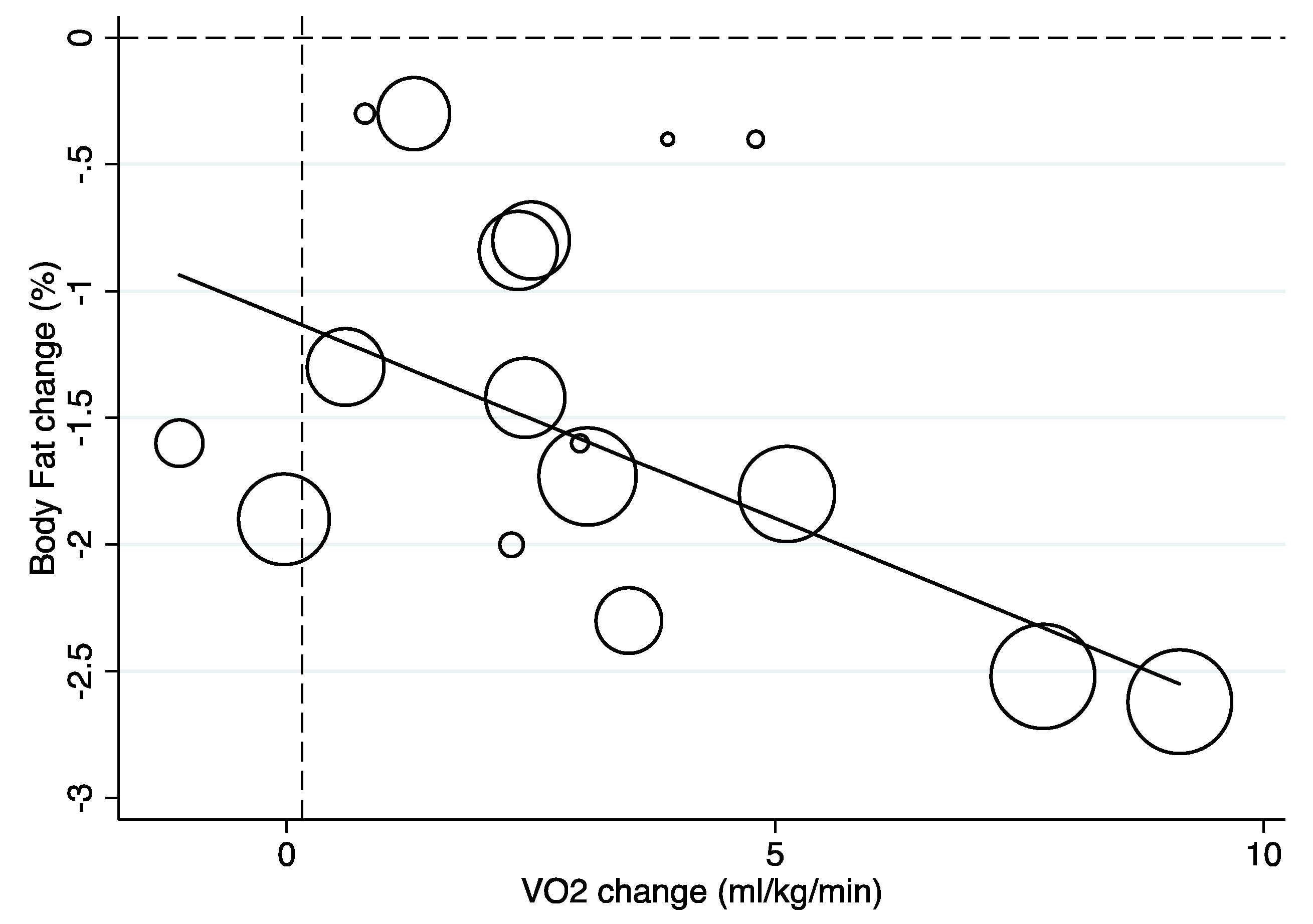
3.3. Synthesis of Results
3.4. Risk of Bias within Studies
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Daniels, S.R.; Arnett, D.K.; Eckel, R.H.; Gidding, S.S.; Hayman, L.L.; Kumanyika, S.; Robinson, T.N.; Scott, B.J.; Jeor, S.S.; Williams, C.L. Overweight in children and adolescents: Pathophysiology, consequences, prevention, and treatment. Circulation 2005, 111, 1999–2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2015, 17, 95–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, G.A.; Kelley, K.S.; Pate, R.R. Exercise and adiposity in overweight and obese children and adolescents: A systematic review with network meta-analysis of randomised trials. BMJ Open 2019, 9, e031220. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramírez-Vélez, R.; Ramirez-Campillo, R.; Peterson, M.; Martinez-Vizcaino, V. Concurrent aerobic plus resistance exercise versus aerobic exercise alone to improve health outcomes in paediatric obesity: A systematic review and meta-analysis. Br. J. Sports Med. 2016, 52, 161–166. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramírez-Vélez, R.; García-Alonso, Y.; Alonso-Martínez, A.M.; Izquierdo, M. Association of cardiorespiratory fitness levels during youth with health risk later in life: A systematic review and meta-analysis. JAMA Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Saavedra, J.M.; Escalante, Y.; García-Hermoso, A. Improvement of aerobic fitness in obese children: A meta-analysis. Pediatr. Obes. 2011, 6, 169–177. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M.R. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Follmann, D.; Elliott, P.; Suh, I.; Cutler, J. Variance imputation for overviews of clinical trials with continuous response. J. Clin. Epidemiol. 1992, 45, 769–773. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberga, A.S.; Prud’Homme, D.; Sigal, R.J.; Goldfield, G.S.; Hadjiyannakis, S.; Phillips, P.; Malcolm, J.; Ma, J.; Doucette, S.; Gougeon, R.; et al. Effects of aerobic training, resistance training, or both on cardiorespiratory and musculoskeletal fitness in adolescents with obesity: The HEARTY trial. Appl. Physiol. Nutr. Metab. 2016, 41, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Sigal, R.J.; Alberga, A.S.; Goldfield, G.S.; Prud’Homme, D.; Hadjiyannakis, S.; Gougeon, R.; Phillips, P.; Tulloch, H.E.; Malcolm, J.; Doucette, S.; et al. Effects of aerobic training, resistance training, or both on percentage body fat and cardiometabolic risk markers in obese adolescents: The healthy eating aerobic and resistance training in youth randomized clinical trial. JAMA Pediatr. 2014, 168, 1006–1014. [Google Scholar] [CrossRef]
- Kelly, A.S.; Wetzsteon, R.J.; Kaiser, D.R.; Steinberger, J.; Bank, A.J.; Dengel, D.R. Inflammation, insulin, and endothelial function in overweight children and adolescents: The role of exercise. J. Pediatr. 2004, 145, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Deldin, A.R.; White, D.; Kim, Y.; Libman, I.; Rivera-Vega, M.; Kuk, J.L.; Sandoval, S.; Boesch, C.; Arslanian, S. Aerobic exercise but not resistance exercise reduces intrahepatic lipid content and visceral fat and improves insulin sensitivity in obese adolescent girls: A randomized controlled trial. Am. J. Physiol. Metab. 2013, 305, E1222–E1229. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Bacha, F.; Hannon, T.; Kuk, J.L.; Boesch, C.; Arslanian, S. Effects of aerobic versus resistance exercise without caloric restriction on abdominal fat, intrahepatic lipid, and insulin sensitivity in obese adolescent boys: A randomized, controlled trial. Diabetes 2012, 61, 2787–2795. [Google Scholar] [CrossRef] [Green Version]
- Maddison, R.; Foley, L.; Ni Mhurchu, C.; Jiang, Y.; Jull, A.; Prapavessis, H.; Hohepa, M.; Rodgers, A. Effects of active video games on body composition: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Sun, M.; Huang, X.-Q.; Yan, Y.; Li, B.; Zhong, W.-J.; Chen, J.-F.; Zhang, Y.-M.; Wang, Z.-Z.; Wang, L.; Shi, X.-C.; et al. One-hour after-school exercise ameliorates central adiposity and lipids in overweight Chinese adolescents: A randomized controlled trial. Chin. Med. J. 2011, 124, 323–329. [Google Scholar]
- Mitchell, B.M.; Gutin, B.; Kapuku, G.K.; Barbeau, P.; Humphries, M.C.; Owens, S.; Vemulapalli, S.; Allison, J. Left ventricular structure and function in obese adolescents: Relations to cardiovascular fitness, percent body fat, and visceral adiposity, and effects of physical training. Pediatrics 2002, 109, e73. [Google Scholar] [CrossRef] [Green Version]
- Racil, G.; Ben Ounis, O.; Hammouda, O.; Kallel, A.; Zouhal, H.; Chamari, K.; Amri, M. Effects of high vs. moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 113, 2531–2540. [Google Scholar] [CrossRef]
- Racil, G.; Zouhal, H.; Elmontassar, W.; Ben Abderrahmane, A.; De Sousa, M.V.; Chamari, K.; Amri, M.; Coquart, J.B. Plyometric exercise combined with high-intensity interval training improves metabolic abnormalities in young obese females more so than interval training alone. Appl. Physiol. Nutr. Metab. 2016, 41, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Saygın, O.; Saygın, O. The effect of twelve week aerobic exercise programme on health related physical fitness components and blood lipids in obese girls. Afr. J. Pharm Pharmacol. 2011, 5, 1441–1445. [Google Scholar] [CrossRef]
- Shaibi, G.Q.; Cruz, M.L.; Ball, G.D.C.; Weigensberg, M.J.; Salem, G.J.; Crespo, N.C.; I Goran, M. Effects of resistance training on insulin sensitivity in overweight latino adolescent males. Med. Sci. Sports Exerc. 2006, 38, 1208–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, A.S.R.; Venâncio, T.L.; Honório, S.A.A.; Martins, J.M.C. Multicomponent training with different frequencies on body composition and physical fitness in obese children. Anais da Acad. Bras. de Ciências 2019, 91. [Google Scholar] [CrossRef] [PubMed]
- Song, J.K.; Stebbins, C.L.; Kim, T.K.; Kim, H.B.; Kang, H.J.; Chai, J.H. Effects of 12 weeks of aerobic exercise on body composition and vascular compliance in obese boys. J. Sports Med. Phys. Fit. 2012, 52, 522–529. [Google Scholar]
- Vasconcellos, F.; Seabra, A.; Cunha, F.; Montenegro, R.; Penha, J.; Bouskela, E.; Neto, J.F.N.; Collett-Solberg, P.; Farinatti, P.D.T.V. Health markers in obese adolescents improved by a 12-week recreational soccer program: A randomised controlled trial. J. Sports Sci. 2015, 34, 564–575. [Google Scholar] [CrossRef]
- Youssef, H.; Groussard, C.; Lemoine-Morel, S.; Jacob, C.; Moussa, E.; Fazah, A.; Pineau, J.C.; Pincemail, J.; Cillard, J.; Delamarche, A. Aerobic training suppresses exercise-induced lipid peroxidation and inflammation in overweight/obese adolescent girls. Pediatr. Exerc. Sci. 2015, 27, 67–76. [Google Scholar] [CrossRef]
- Berntsen, S.; Mowinckel, P.; Carlsen, K.-H.; Carlsen, K.C.L.; Kolsgaard, M.L.P.; Joner, G.; Anderssen, S.A. Obese children playing towards an active lifestyle. Pediatr. Obes. 2010, 5, 64–71. [Google Scholar] [CrossRef]
- Bharath, L.P.; Choi, W.W.; Cho, J.-M.; Skobodzinski, A.A.; Wong, A.; Sweeney, T.E.; Park, S.-Y. Combined resistance and aerobic exercise training reduces insulin resistance and central adiposity in adolescent girls who are obese: Randomized clinical trial. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 118, 1653–1660. [Google Scholar] [CrossRef]
- Carrel, A.L.; Clark, R.R.; Peterson, S.E.; Nemeth, B.A.; Sullivan, J.; Allen, D.B. Improvement of fitness, body composition, and insulin sensitivity in overweight children in a school-based exercise program: A randomized, controlled study. Arch. Pediatr. Adolesc. Med. 2005, 159, 963–968. [Google Scholar] [CrossRef] [Green Version]
- Chae, H.W.; Kwon, Y.-N.; Rhie, Y.-J.; Kim, H.-S.; Kim, Y.-S.; Paik, I.-Y.; Suh, S.-H.; Kim, D.H. Effects of a structured exercise program on insulin resistance, inflammatory markers and physical fitness in obese Korean children. J. Pediatr. Endocrinol. Metab. 2010, 23, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.L.; Pollock, N.K.; Waller, J.L.; Allison, J.D.; Dennis, B.A.; Bassali, R.; Meléndez, A.; Boyle, C.A.; Gower, B.A. Exercise dose and diabetes risk in overweight and obese children. JAMA 2012, 308, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Dias, K.A.; Ingul, C.B.; Tjønna, A.E.; E Keating, S.; Gomersall, S.R.; Follestad, T.; Hosseini, M.S.; Hollekim-Strand, S.M.; Ro, T.B.; Haram, M.; et al. Effect of high-intensity interval training on fitness, fat mass and cardiometabolic biomarkers in children with obesity: A randomised controlled trial. Sports Med. 2017, 48, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Farpour-Lambert, N.J.; Aggoun, Y.; Marchand, L.M.; Martin, X.E.; Herrmann, F.R.; Beghetti, M. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J. Am. Coll. Cardiol. 2009, 54, 2396–2406. [Google Scholar] [CrossRef]
- Lee, K.-J.; Shin, Y.-A.; Lee, K.-Y.; Jun, T.-W.; Song, W. Aerobic exercise training-induced decrease in plasma visfatin and insulin resistance in obese female adolescents. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 275–281. [Google Scholar] [CrossRef]
- Force, U.P.S.T.; Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; et al. Screening for obesity in children and adolescents: US preventive services task force recommendation statement. JAMA 2017, 317, 2417–2426. [Google Scholar] [CrossRef]
- Neufer, P.; Bamman, M.M.; Muoio, D.M.; Bouchard, C.; Cooper, D.M.; Goodpaster, B.H.; Booth, F.W.; Kohrt, W.M.; Gerszten, R.E.; Mattson, M.P.; et al. Understanding the cellular and molecular mechanisms of physical activity-induced health benefits. Cell Metab. 2015, 22, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Information, P.E.K.F.C. Metabolic syndrome update. Trends Cardiovasc. Med. 2016, 26, 364–373. [Google Scholar] [CrossRef]
- Chen, Z.-P.; Stephens, T.J.; Murthy, S.; Canny, B.J.; Hargreaves, M.; Witters, L.A.; E Kemp, B.; McConell, G. Effect of exercise intensity on skeletal muscle AMPK signaling in humans. Diabetes 2003, 52, 2205–2212. [Google Scholar] [CrossRef] [Green Version]
- Hood, D.A.; Uguccioni, G.; Vainshtein, A.; D’Souza, D. Mechanisms of exercise-induced mitochondrial biogenesis in skeletal muscle: Implications for health and disease. Compr. Physiol. 2011, 1, 1119–1134. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Sample, Age (Range or Mean) | Type | Intervention Length (Weeks) | Frequency (Sessions/Week) | Duration (min) | Adherence (%) | Percent Body Fat Assessment | Cardiorespiratory Fitness Assessment |
|---|---|---|---|---|---|---|---|---|
| Alberga 2016 [12]/Sigal 2014 [13], Canada | 304 (70% girls), 14–18 years old | AE, ST, CT | 22 | 4 | 20–45 | 56–64 | Magnetic resonance imaging | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Alves et al. 2019 [24], Portugal | 40 (NR), 12–15 years old | CT | 10 | 2–3 | 60 | NR | Standard formula | 20-m Shuttle Run Test |
| Berntsen 2010 [28], Norway | 60 (51% girls), 7–17 years old | CT | 20 | 2 | 60 | 60 | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Bharath 2018 [29], USA | 40 (100% girls), 14.7 years old | CT | 12 | 5 | 60 | NR | Bioelectrical impedance meter | Treadmill running test. Maximal heart rate was obtained. |
| Carrel 2005 [30], USA | 50 (48% girls), 12.5 years old | AE | 36 | 5 | 45 | NR | Dual-energy X-ray absorptiometry | 4-min submaximal treadmill walk test. Oxygen consumption was measured by indirect calorimetry |
| Chae 2010 [31], South Korea | 38 (45% girls), 9–15 years old | AE | 12 | 2 | 90 | NR | Bioelectrical impedance meter | Treadmill running test. Oxygen consumption was measured by indirect calorimetry |
| Davis 2012 [32], USA | 222 (58% girls), 7–11 years old | AE | 13 | 5 | 20–40 | 84 | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Dias 2018 [33], Australia | 99 (53% girls); 7–16 years old | AE | 12 | 3 | 40–44 | 56–68 | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Farpour-Lambert 2009 [34], Switzerland | 44 (64% girls), 6–11 years old | CT | 12 | 3 | 60 | 83 | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Kelly 2004 [14], USA | 25 (52% girls), 10.9 years old | AE | 8 | 4 | 30–50 | NR | Dual-energy X-ray absorptiometry | Cycle ergometer test. Oxygen consumption was measured by indirect calorimetry |
| Lee 2013 [15], USA | 54 (100% girls), 12–18 years old | AE, ST | 12 | 3 | 60 | 95 | Magnetic resonance imaging | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Lee 2010 [35], South Korea | 18 (100% girls), 16.7 years old | AE | 12 | 4 | 40–50 | NR | Bioelectrical impedance meter | Åstrand protocol with a cycle ergometer |
| Lee 2012 [16], USA | 45 (0% girls), 12–18 years old | AE, ST | 12 | 3 | 60 | 99 | Magnetic resonance imaging | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Maddison 2011 [17], New Zeland | 322 (27% girls), 10–14 years old | AE | - | - | - | - | Bioelectrical impedance meter | 20-m Shuttle Run Test |
| Mitchell 2002 [19], USA | 81 (68% girls), 13–16 years old | AE | 32 | 5 | 29–43 | 51–56 | Magnetic resonance imaging | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Racil 2013 [20], Tunisia | 34 (100% girls), 15.9 years old | AE | 12 | 3 | - | NR | Bioelectrical impedance meter | Run test. Oxygen consumption was measured by indirect calorimetry |
| Racil 2016 [21], Tunisia | 68 (100% girls), 16.6 years old | AE, CT | 12 | 3 | 35 | NR | Bioelectrical impedance meter | Run test. Oxygen consumption was measured by indirect calorimetry |
| Saygın 2011 [22], Turkey | 40 (100% girls), 10–12 years old | AE | 12 | 3 | 50–90 | NR | Skinfolds | 20-m Shuttle Run Test |
| Shaibi 2006 [23], USA | 22 (0% girls), 15.3 years old | ST | 16 | 2 | - | NR | Dual-energy X-ray absorptiometry | Cycle ergometer test. Oxygen consumption was measured by indirect calorimetry |
| Song 2012 [25], USA | 22 (0% girls), 12–13 years old | AE | 12 | 3 | 50 | NR | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Sun 2011 [18], China | 93 (52% girls), 13.6 years old | AE | 10 | 4 | 60 | 57.5 | Dual-energy X-ray absorptiometry | Physical Working Capacity at a heart rate of 170 bpm (PWC170) |
| Vasconcellos 2016 [26], Brazil | 30 (20% girls), 12–17 years old | AE | 12 | 3 | 60 | NR | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
| Youssef 2015 [27], France | 39 (100% girls), 14–18 years old | AE | 12 | 3 | 40 | NR | Dual-energy X-ray absorptiometry | Treadmill test. Oxygen consumption was measured by indirect calorimetry |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Hermoso, A.; Izquierdo, M.; Alonso-Martínez, A.M.; Faigenbaum, A.; Olloquequi, J.; Ramírez-Vélez, R. Association between Exercise-Induced Changes in Cardiorespiratory Fitness and Adiposity among Overweight and Obese Youth: A Meta-Analysis and Meta-Regression Analysis. Children 2020, 7, 147. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090147
García-Hermoso A, Izquierdo M, Alonso-Martínez AM, Faigenbaum A, Olloquequi J, Ramírez-Vélez R. Association between Exercise-Induced Changes in Cardiorespiratory Fitness and Adiposity among Overweight and Obese Youth: A Meta-Analysis and Meta-Regression Analysis. Children. 2020; 7(9):147. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090147
Chicago/Turabian StyleGarcía-Hermoso, Antonio, Mikel Izquierdo, Alicia M. Alonso-Martínez, Avery Faigenbaum, Jordi Olloquequi, and Robinson Ramírez-Vélez. 2020. "Association between Exercise-Induced Changes in Cardiorespiratory Fitness and Adiposity among Overweight and Obese Youth: A Meta-Analysis and Meta-Regression Analysis" Children 7, no. 9: 147. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090147