Longer Exposure to Left-to-Right Shunts Is a Risk Factor for Pulmonary Vein Stenosis in Patients with Trisomy 21

Abstract
:
1. Introduction
2. Materials and Methods
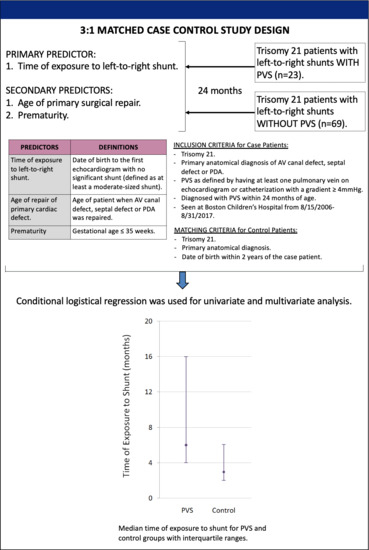
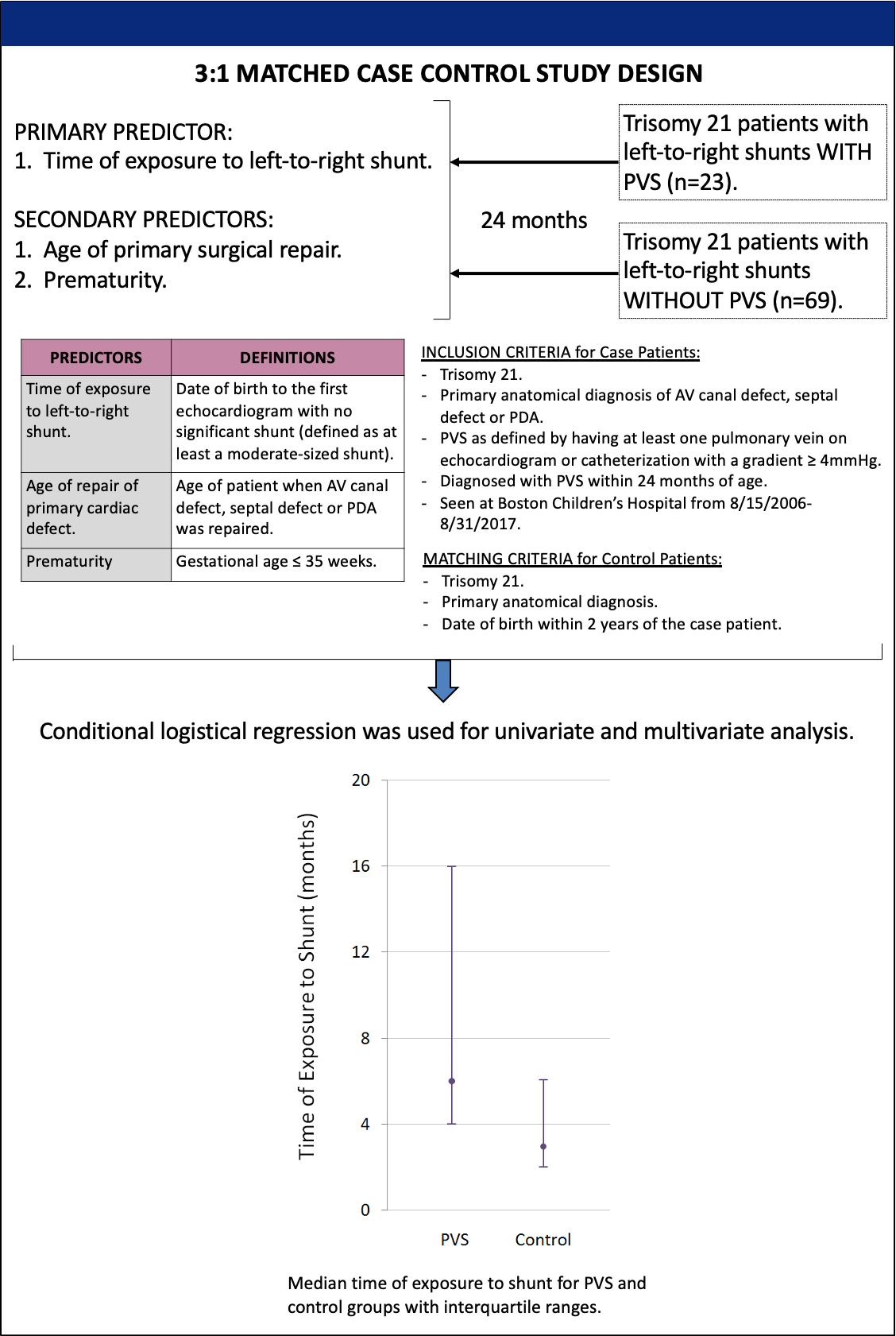
2.1. Patient Selection
2.2. Primary and Secondary Predictors
2.3. Subanalyses
2.4. Ethics Statement
3. Results
3.1. Patient Characteristics
3.2. Primary and Secondary Predictors
3.3. Multivessel PVS
3.4. Subanalysis of Patients Based on Gestational Age
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kalfa, D.; Belli, E.; Bacha, E.; Lambert, V.; di Carlo, D.; Kostolny, M.; Salminen, J.; Nosal, M.; Poncelet, A.; Horer, J.; et al. Primary pulmonary vein stenosis: Outcomes, risk factors and severity score in multicentric study. Ann Thorac. Surg. 2017, 104, 182–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viola, N.; Alghamdi, A.; Perrin, D.; Wilson, G.; Coles, J.; Caldarone, C. Primary pulmonary vein stenosis: The impact of sutureless repair on survival. J. Thorac. Cardiovasc. Surg. 2011, 142, 344–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breinholt, J.; Hawkins, J.; Minich, L.; Tani, L.; Orsmond, G.; Ritter, S.; Shaddy, R.E. Pulmonary vein stenosis with normal connection: Associated cardiac abnormalities and variable outcome. Ann. Thorac. Surg. 1999, 68, 164–168. [Google Scholar] [CrossRef]
- Backes, C.; Nealon, E.; Armstrong, A.; Cua, C.; Mitchell, C.; Krishnan, U.; Vanderlaan, R.D.; Song, M.K.; Viola, N.; Smith, C.V.; et al. Pulmonary Vein Stenosis in Infants: A Systematic Review, Meta-Analysis, and Meta-Regression. J. Pediatrics 2018, 198, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Debbaut, C.; McEnaney, K.; Roberts, A.; Gauvreau, K.; Western, K.; Ireland, C.; Baird, C.; Jenkins, K. Clinical and genetic features of pulmonary vein stenosis. JACC 2014, 63, A524. [Google Scholar] [CrossRef] [Green Version]
- Prosnitz, A.; Leopold, J.; Irons, M.; Jenkins, K.; Roberts, A. Pulmonary vein stenosis in patients with Smith-Lemli-Opitz Syndrome. Congenit. Heart Dis. 2017, 12, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.; Yamada, J.; McEnaney, K.; Jenkins, K.; Chen, M.l. Pulmonary vein stenosis is associated with Trisomy 21. Circulation 2019, 140, A13883. [Google Scholar]
- Riedlinger, W.; Juraszek, A.; Jenkins, K.; Nugent, A.; Balasubramanian, S.; Calicchio, M.; Kieran, M.W.; Collins, T. Pulmonary vein stenosis: Expression of receptor tyrosine kinases by lesional cells. Cardiovasc. Pathol. 2006, 15, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Mahgoub, L.; Kaddoura, T.; Kameny, A.; Lopez Ortego, P.; Vanderlaan, R.; Kakadekar, A.; Dicke, F.; Rebeyka, I.; Calderone, C.A.; Redington, A.; et al. Pulmonary vein stenosis of ex-premature infants with pulmonary hypertension and bronchopulmonary dysplasia, epidemiology, and survival from a multicenter cohort. Pediatric. Pulmonol. 2017, 52, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Drossner, D.; Kim, D.; Maher, K.; Mahle, W. Pulmonary vein stenosis: Prematurity and associated conditions. Pediatrics 2008, 122, e656–e661. [Google Scholar] [CrossRef] [PubMed]
- Gowda, S.; Bhat, D.; Feng, Z.; Chang, C.; Ross, R. Pulmonary Vein Stenosis with Down Syndrome: A Rare and Frequently Fatal Cause of Pulmonary Hypertension in Infants and Children. Congenit. Heart Dis. 2014, 9, E90–E97. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.; Gauvreau, K.; Del Nido, P.; Kieran, M.; Roth, S.; Jenkins, K. Host Factor Vulnerability and Development of Progressive Intraluminal Pulmonary Vein Stenosis after Congenital Heart Surgery. Congenit. Heart Dis. 2009, 4, 86–90. [Google Scholar] [CrossRef]
- Weijerman, M.; van Furth, A.; Noordegraaf, A.; van Wouwe, J.; Broers, C.; Gemke, R. Prevalence, Neonatal Characteristics, and First-Year Mortality of Down Syndrome: A National Study. J. Pediatrics 2008, 152, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Lange, R.; Guenther, T.; Busch, R.; Hess, J.; Schreiber, C. The presence of Down syndrome is not a risk factor in complete atrioventricular septal defect repair. J. Thorac. Cardiovasc. Surg. 2007, 134, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atz, A.; Hawkins, J.; Lu, M.; Cohen, M.; Colan, S.; Jaggers, J.; Lacro, R.V.; McCrindle, B.W.; Margossian, R.; Mosca, R.S.; et al. Surgical Management of Complete Atrioventricular Septal Defect: Associations with Surgical Technique, Age, and Trisomy 21. J. Thorac. Cardiovasc. Surg. 2011, 141, 1371–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, E.; Ibrahimiye, A.; Yerebakan, H.; Yilmaz, B.; Chelliah, A.; Levasseaur, S.; Mosca, R.S.; Chen, J.M.; Chai, P.; Quaegebeur, J.; et al. Early Complete Atrioventricular Canal Repair Yields Outcomes Equivalent to Late Repair. Ann Thorac. Surg. 2015, 99, 2109–2116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muto, A.; Model, L.; Ziegler, K.; Eghbalieh, S.; Dardik, A. Mechanisms of vein graft adaptation to the arterial circulation: Insights into the neotimal algorithm and management strategies. Circ. J. 2010, 74, 1501–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jobe, A. The New BPD: An Arrest in Lung Development. Pediatric Res. 1999, 46, 641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, T.; Smith, A.; Breatnach, C.; Kent, E.; Shanahan, I.; Boyle, M.; Levy, P.T.; Franklin, O.; El-Khuffash, A. Infants Born with Down Syndrome: Burden of Disease in the Early Neonatal Period. J. Pediatrics 2018, 193, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.; Galambos, C.; Ivy, D.; Abman, S.; Wolter-Warmerdam, K.; Hickey, F. Clinical Characteristics and Risk Factors for Developing Pulmonary Hypertension in Children with Down Syndrome. J. Pediatrics 2018, 202, 212–219. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | PVS (n = 23) | No PVS (n = 69) | p-Value |
|---|---|---|---|
| Gestational age at birth | 38 (34, 38) | 38 (37, 38) | <0.01 |
| Sex (female) | 11 (49%) | 33 (49%) | 0.91 |
| Anatomy | |||
| CAVC | 18 (78%) | 54 (78%) | N/A |
| Secundum ASD | 2 (9%) | 5 (7%) | N/A |
| Membranous VSD | 2 (9%) | 9 (13%) | N/A |
| PDA | 1 (4%) | 1 (1%) | N/A |
| Surgical history | |||
| Primary repair | 21 (91%) | 69 (100%) | 0.01 |
| Palliation with PA band | 2 (9%) | 0 | 0.01 |
| Age at primary repair (months) | 5 (4, 7) | 3 (2, 6) | 0.08 |
| Death | 4 (17%) | 0 | <0.01 |
| Pulmonary vein disease | |||
| Age at diagnosis (months) | 5.3 (3.9, 8.6) | N/A | N/A |
| Single vessel | 6 (26%) | N/A | N/A |
| Multivessel | 17 (74%) | N/A | N/A |
| Number of surgeries | 1 (0, 2) | N/A | N/A |
| Number of catheterizations | 1 (0, 15) | N/A | N/A |
| Pulmonary hypertension | |||
| Clinical diagnosis | 14 (60%) | 1 (1.4%) | <0.01 |
| Mean PA pressure > 25 mmHg | 9 (39%) | 0 | <0.01 |
| Sildenafil or oxygen | 14 (60%) | 0 | <0.01 |
| Analysis | PVS (n = 23) | No PVS (n = 69) | p-Value |
|---|---|---|---|
| Univariate | |||
| Time of exposure to shunt (months) | 6 (4, 16) | 3 (2, 6) | 0.002 |
| Age at primary repair (≥4 months) | 17 (81%) | 29 (42%) | 0.003 |
| Premature (birth ≤ 35 weeks GA) | 11 (48%) | 9 (13%) | 0.003 |
| Multivariate | Odds Ratio | 95% CI | |
| Risk of PVS per month of exposure to shunt | 1.21 | (1.06, 1.39) | 0.007 |
| Premature (birth ≤ 35 weeks GA) | 4.77 | (1.36, 16.8) | 0.015 |
| Characteristics | PVS (n = 17) | No PVS (n = 51) | p-Value |
|---|---|---|---|
| Gestational age at birth | 35 (34, 38) | 38 (37, 38) | <0.01 |
| Sex (female) | 10 (59%) | 24 (47%) | 0.41 |
| Anatomy | |||
| CAVC | 12 (71%) | 36 (70%) | N/A |
| Secundum ASD | 3 (18%) | 10 (20%) | N/A |
| Membranous VSD | 2 (12%) | 5 (10%) | N/A |
| Surgical history | |||
| Primary repair | 15 (88%) | 51 (100%) | 0.01 |
| Palliation with PA band | 2 (12%) | 0 | 0.01 |
| Age at primary repair | 5 (3.5, 8.5) | 3 (2, 7) | 0.07 |
| Death | 4 (24%) | 0 | <0.01 |
| Pulmonary vein disease | |||
| Age at diagnosis (months) | 5.4 (3.9, 8.6) | N/A | N/A |
| Number of surgeries | 1 (0, 2) | N/A | N/A |
| Number of catheterizations | 1 (0, 15) | N/A | N/A |
| Pulmonary hypertension | |||
| Clinical diagnosis | 13 (76%) | 1 (2%) | <0.01 |
| Mean PA pressure > 25 mmHg | 8 (74%) | 0 | <0.01 |
| Sildenafil or oxygen | 13 (76%) | 0 | <0.01 |
| Analysis | PVS (n = 17) | No PVS (n = 51) | p-Value |
|---|---|---|---|
| Univariate | |||
| Time of exposure to shunt (months) | 6 (4, 17) | 3 (2, 7) | 0.006 |
| Age at primary repair (≥4 months) | 11 (73%) | 24 (47%) | 0.045 |
| Premature (birth ≤ 35 weeks GA) | 9 (53%) | 7 (14%) | 0.005 |
| Multivariate | Odds Ratio | 95% CI | |
| Risk of PVS per month of exposure to shunt | 1.15 | (1.01, 1.30) | 0.032 |
| Premature (birth ≤ 35 weeks GA) | 4.33 | (1.14, 16.4) | 0.031 |
| Analysis | PVS | No PVS | p-Value |
|---|---|---|---|
| Gestational age at birth ≤ 35 weeks | |||
| Time of exposure to shunt (months) | 6 (4, 24) | 3 (2, 5) | 0.023 |
| Gestational age at birth > 35 weeks | |||
| Time of exposure to shunt (months) | 8 (4, 10) | 3 (2, 6) | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, C.; Gauvreau, K.; Levy, P.; Callahan, R.; Jenkins, K.J.; Chen, M. Longer Exposure to Left-to-Right Shunts Is a Risk Factor for Pulmonary Vein Stenosis in Patients with Trisomy 21. Children 2021, 8, 19. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010019
Choi C, Gauvreau K, Levy P, Callahan R, Jenkins KJ, Chen M. Longer Exposure to Left-to-Right Shunts Is a Risk Factor for Pulmonary Vein Stenosis in Patients with Trisomy 21. Children. 2021; 8(1):19. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010019
Chicago/Turabian StyleChoi, Connie, Kimberlee Gauvreau, Philip Levy, Ryan Callahan, Kathy J. Jenkins, and Minghui Chen. 2021. "Longer Exposure to Left-to-Right Shunts Is a Risk Factor for Pulmonary Vein Stenosis in Patients with Trisomy 21" Children 8, no. 1: 19. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010019