
A Four-Year Follow-Up Case Report of Hypomineralized Primary Second Molars Rehabilitated with Stainless Steel Crowns




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
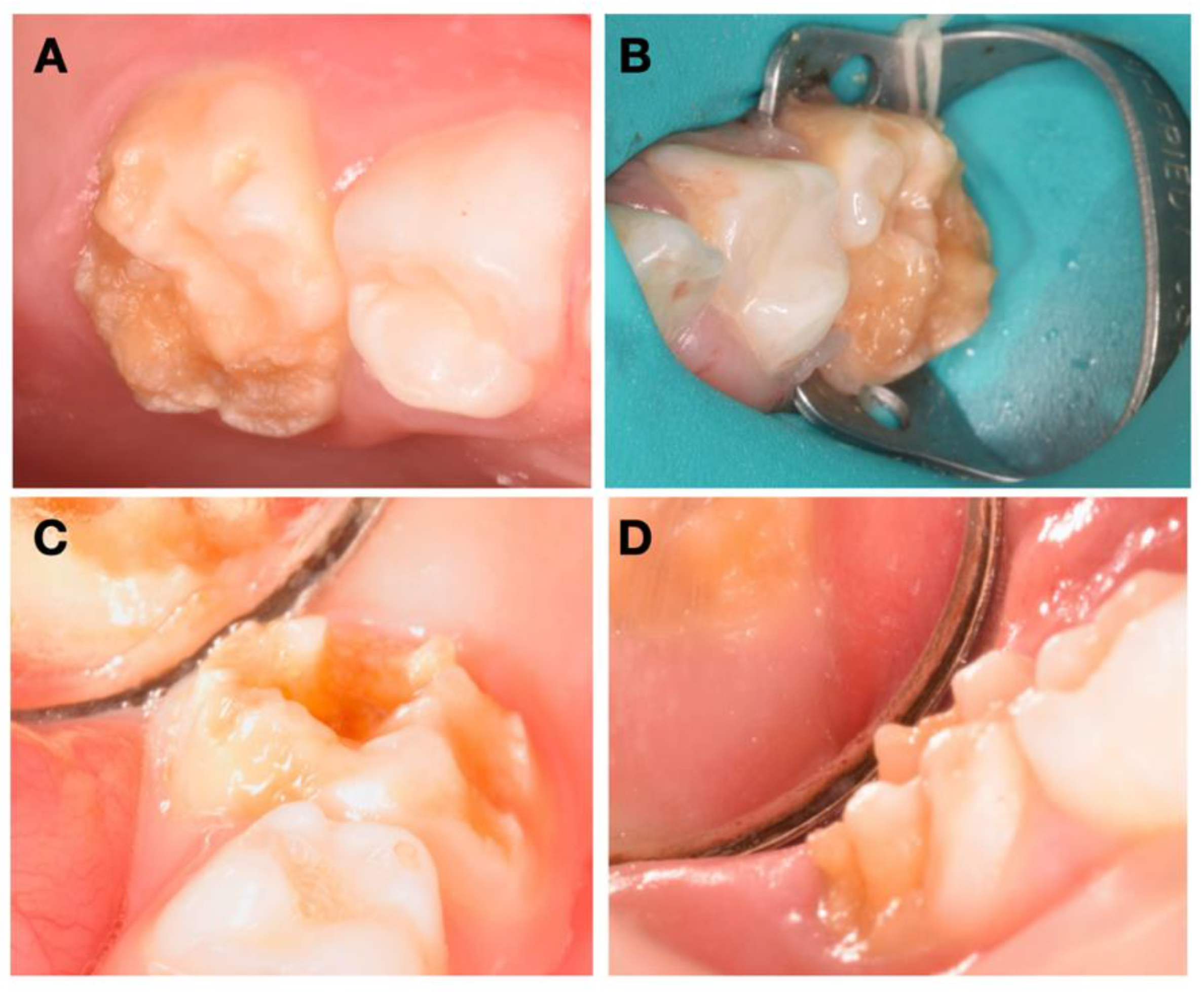
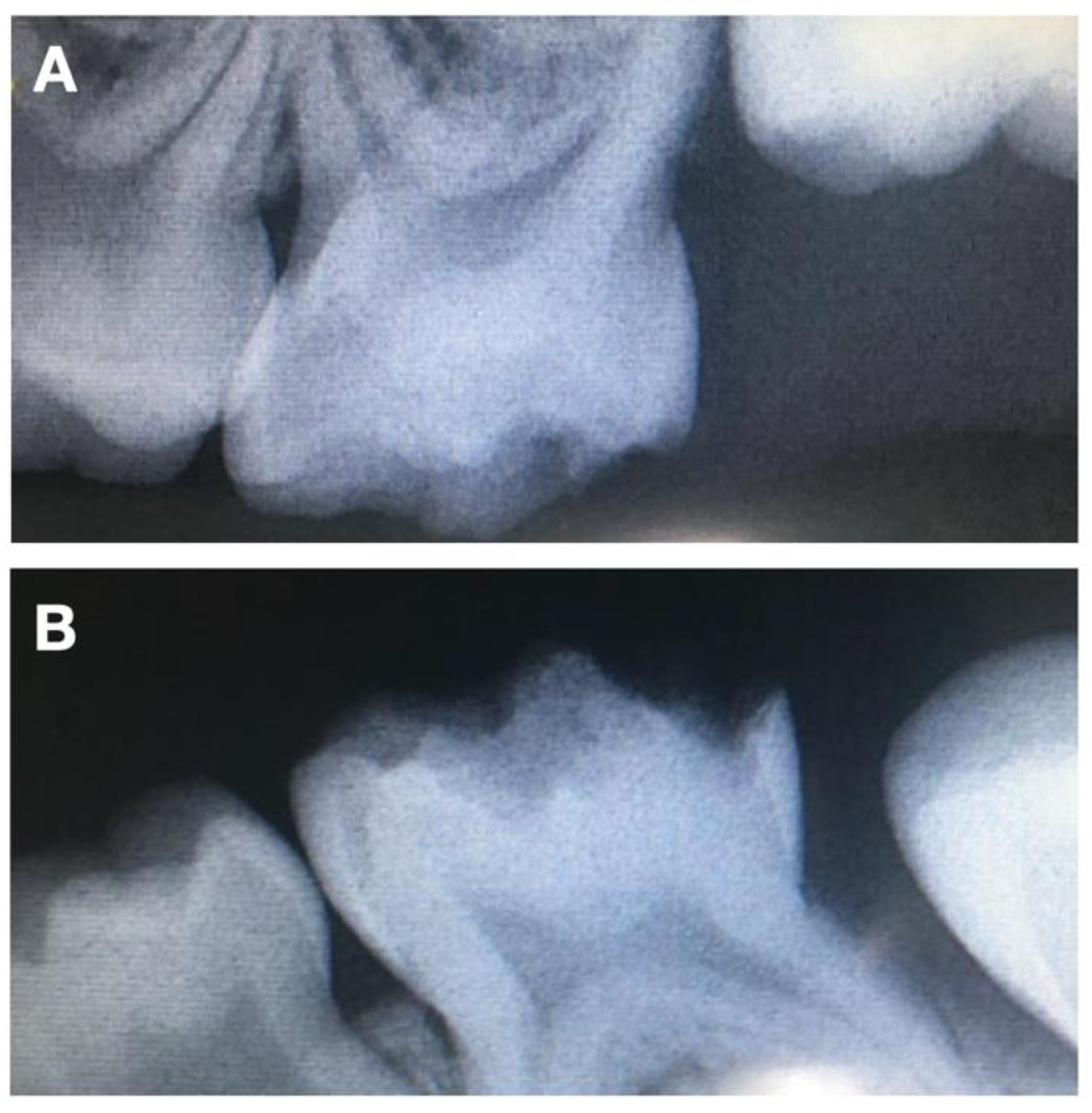
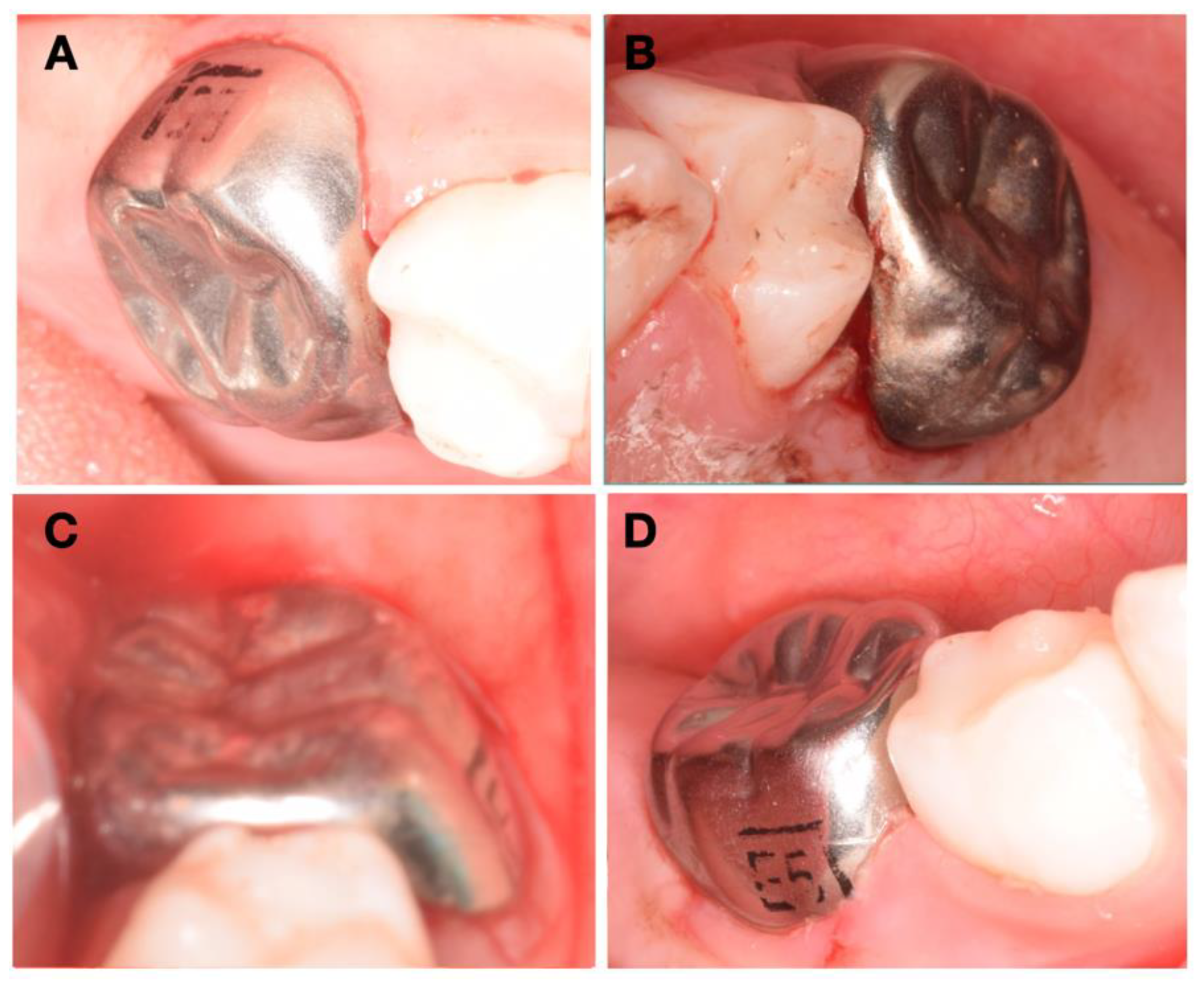
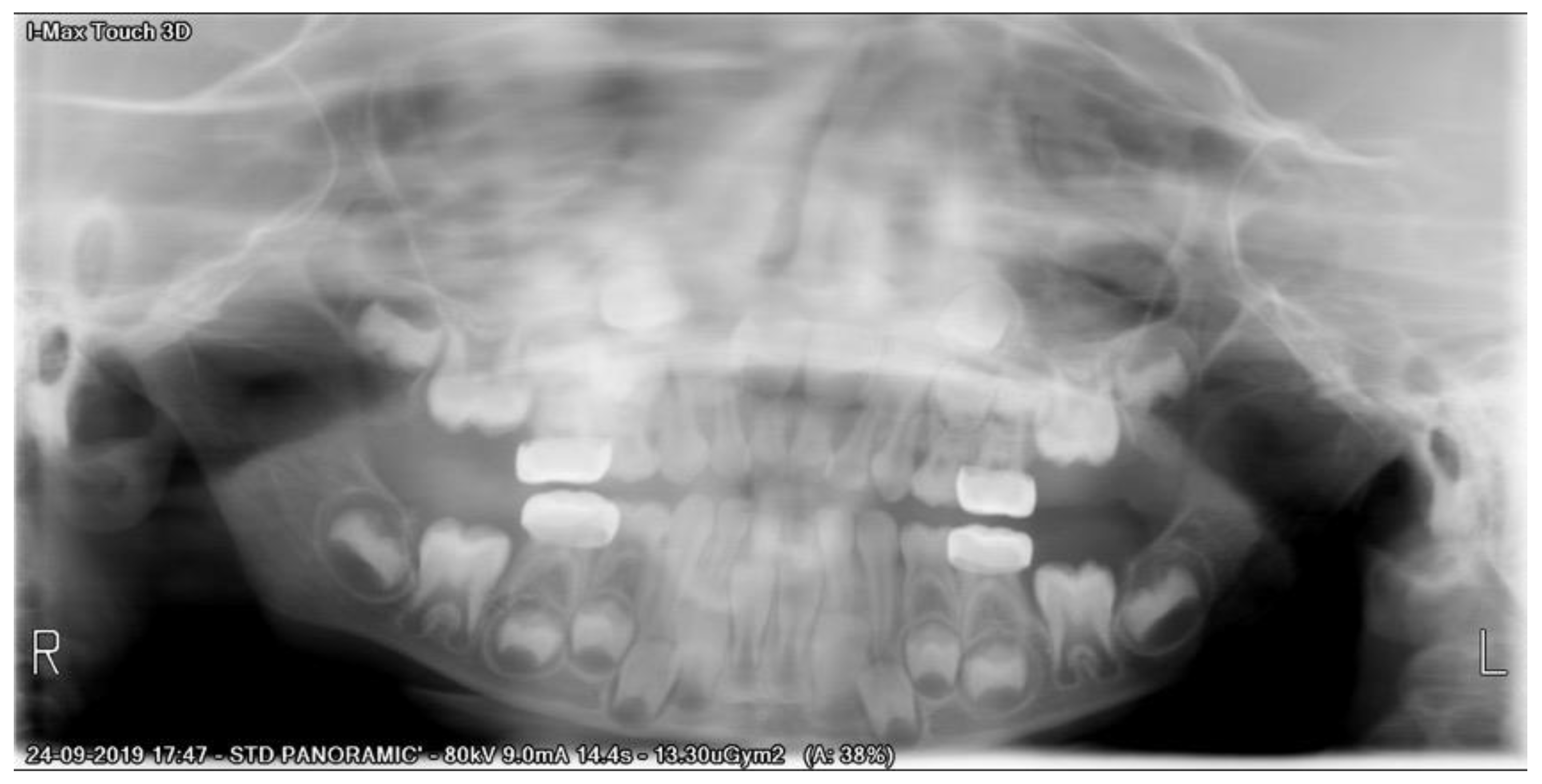
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Owen, M.L.; Ghanim, A.; Elsby, D.; Manton, D.J. Hypomineralized second primary molars: Prevalence, defect characteristics and relationship with dental caries in Melbourne preschool children. Aust. Dent. J. 2018, 63, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Elfrink, M.; Schuller, A.; Weerheijm, K.; Veerkamp, J. Hypomineralized Second Primary Molars: Prevalence Data in Dutch 5-Year-Olds. Caries Res. 2008, 42, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Weerheijm, K.L.; Duggal, M.; Mejàre, I.; Papagiannoulis, L.; Koch, G.; Martens, L.C.; Hallonsten, A.-L. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: A summary of the European meeting on MIH held in Athens, 2003. Eur. J. Paediatr. Dent. 2003, 4, 110–113. [Google Scholar]
- Vlachou, C.; Arhakis, A.; Kotsanos, N. Distribution and morphology of enamel hypomineralisation defects in second primary molars. Eur. Arch. Paediatr. Dent. 2021, 22, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Alifakioti, E.; Arhakis, A.; Oikonomidis, S.; Kotsanos, N. Structural and chemical enamel characteristics of hypomineralised second primary molars. Eur. Arch. Paediatr. Dent. 2021, 22, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Declerck, D.; Mampay, E. Non-invasive treatment approach for hypomineralised second primary molars using preformed metal crowns: Results after 1-year follow-up. Eur. Arch. Paediatr. Dent. 2021, 22, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Jälevik, B. Prevalence and Diagnosis of Molar-Incisor-Hypomineralisation (MIH): A systematic review. Eur. Arch. Paediatr. Dent. 2010, 11, 59–64. [Google Scholar] [CrossRef]
- Van Der Tas, J.T.; Elfrink, M.E.; Heijboer, A.C.; Rivadeneira, F.; Jaddoe, V.W.; Tiemeier, H.; Schoufour, J.D.; Moll, H.A.; Ongkosuwito, E.; Wolvius, E.B.; et al. Foetal, neonatal and child vitamin D status and enamel hypomineralization. Community Dent. Oral Epidemiol. 2018, 46, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Halal, F.; Raslan, N. Prevalence of hypomineralised second primary molars (HSPM) in Syrian preschool children. Eur. Arch. Paediatr. Dent. 2020, 21, 711–717. [Google Scholar] [CrossRef]
- Da Silva Figueiredo Sé, M.J.; Ribeiro, A.P.; dos Santos-Pinto, L.A.; de Cassia Loiola Cordeiro, R.; Cabral, R.N.; Leal, S.C. Are hypomineralized primary molars and canines associated with molar-incisor hypomineralization? Pediatr. Dent. 2017, 39, 445–449. [Google Scholar]
- Elfrink, M.E.C.; Ghanim, A.; Manton, D.J.; Weerheijm, K.L. Standardised studies on Molar Incisor Hypomineralisation (MIH) and Hypomineralised Second Primary Molars (HSPM): A need. Eur. Arch. Paediatr. Dent. 2015, 16, 247–255. [Google Scholar] [CrossRef]
- Goyal, A.; Dhareula, A.; Gauba, K.; Bhatia, S.K. Prevalence, defect characteristics and distribution of other phenotypes in 3- to 6-year-old children affected with Hypomineralised Second Primary Molars. Eur. Arch. Paediatr. Dent. 2019, 20, 585–593. [Google Scholar] [CrossRef]
- Garot, E.; Denis, A.; Delbos, Y.; Manton, D.; Silva, M.; Rouas, P. Are hypomineralised lesions on second primary molars (HSPM) a predictive sign of molar incisor hypomineralisation (MIH)? A systematic review and a meta-analysis. J. Dent. 2018, 72, 8–13. [Google Scholar] [CrossRef]
- Lima, L.R.S.; Pereira, A.S.; De Moura, M.S.; Lima, C.C.B.; Paiva, S.M.; Moura, L.D.F.A.D.D.; Lima, M.D.D.M.D. Pre-term birth and asthma is associated with hypomineralized second primary molars in pre-schoolers: A population-based study. Int. J. Paediatr. Dent. 2019, 30, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Fatturi, A.; Menezes, J.V.N.B.; Fraiz, F.C.; Assunção, L.R.S.; Souza, J.F. Systemic Exposures Associated with Hypomineralized Primary Second Molars. Pediatr. Dent. 2019, 41, 364–370. [Google Scholar]
- Neboda, C.; Anthonappa, R.P.; King, N.M. Preliminary investigation of the variations in root canal morphology of hypomineralised second primary molars. Int. J. Paediatr. Dent. 2018, 28, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Negre-Barber, A.; Montiel-Company, J.M.; Catalá, M.B.; Catala-Pizarro, M.; Silla, J.M.A. Hypomineralized Second Primary Molars as Predictor of Molar Incisor Hypomineralization. Sci. Rep. 2016, 6, 31929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, M.; Kilpatrick, N.; Craig, J.; Manton, D.; Leong, P.; Burgner, D.; Scurrah, K. Etiology of Hypomineralized Second Primary Molars: A Prospective Twin Study. J. Dent. Res. 2018, 98, 77–83. [Google Scholar] [CrossRef]
- Mittal, N.; Sharma, B.B. Hypomineralised second primary molars: Prevalence, defect characteristics and possible association with Molar Incisor Hypomineralisation in Indian children. Eur. Arch. Paediatr. Dent. 2015, 16, 441–447. [Google Scholar] [CrossRef]
- Oyedele, T.A.; Folayan, M.O.; Oziegbe, E.O. Hypomineralised second primary molars: Prevalence, pattern and associated co morbidities in 8- to 10-year-old children in Ile-Ife, Nigeria. BMC Oral Health 2016, 16, 65. [Google Scholar] [CrossRef] [Green Version]
- Hegde, K.S.; Bhat, S.S.; Rao, H.A.; Kumar, B.K. Characteristics of Primary Dentition Occlusion in Preschool Children: An Epidemiological Study. Int. J. Clin. Pediatr. Dent. 2012, 5, 93–97. [Google Scholar] [CrossRef]
- Ahmad, A.J.; Parekh, S.; Ashley, P. Methods of space maintenance for premature loss of a primary molar: A review. Eur. Arch. Paediatr. Dent. 2018, 19, 311–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffding, J.; Kisling, E. Premature loss of primary teeth: Part I, its overall effect on occlusion and space in the permanent dentition. ASDC J. Dent. Child. 1978, 45, 279–283. [Google Scholar]
- Karimizadeh, Z.; Sabeti, A.K.; Rafatjou, R. Maximum equivalent stress induced and the displacement of the developing permanent first molars after the premature loss of primary second molars: A finite element analysis. Dent. Med. Probl. 2020, 57, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.L.; Peng, Y.R.; Zou, J.; Wang, Y. Space maintenance for the premature loss of the second primary molar. Zhonghua Kou Qiang Yi Xue Za Zhi 2019, 54, 851–854. [Google Scholar] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandeira Lopes, L.; Machado, V.; Botelho, J. A Four-Year Follow-Up Case Report of Hypomineralized Primary Second Molars Rehabilitated with Stainless Steel Crowns. Children 2021, 8, 923. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100923
Bandeira Lopes L, Machado V, Botelho J. A Four-Year Follow-Up Case Report of Hypomineralized Primary Second Molars Rehabilitated with Stainless Steel Crowns. Children. 2021; 8(10):923. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100923
Chicago/Turabian StyleBandeira Lopes, Luísa, Vanessa Machado, and João Botelho. 2021. "A Four-Year Follow-Up Case Report of Hypomineralized Primary Second Molars Rehabilitated with Stainless Steel Crowns" Children 8, no. 10: 923. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100923