
Epidemiology and Trends over Time of Foreign Body Injuries in the Pediatric Emergency Department

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
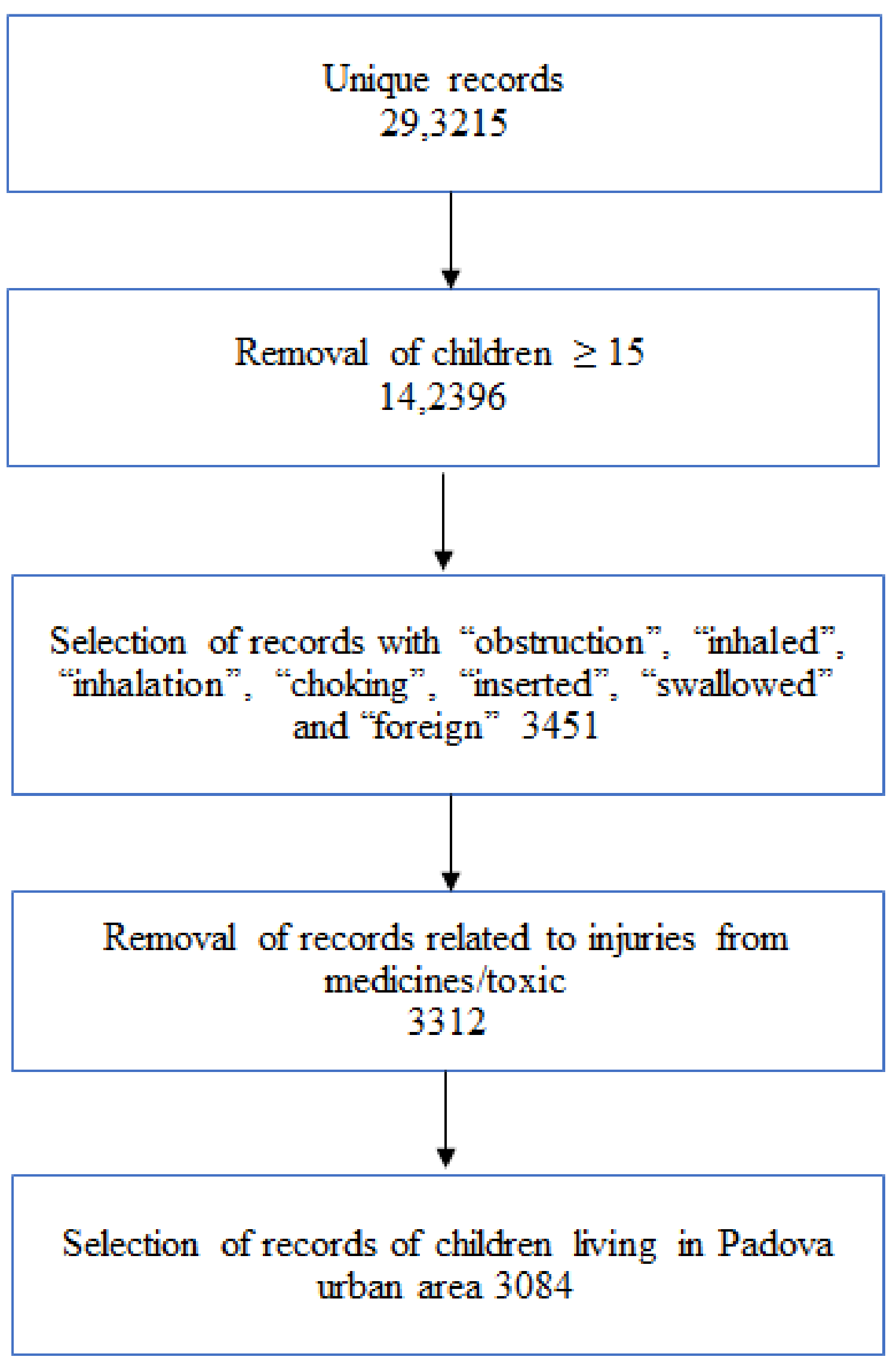
2.3. Inclusion and Exclusion Criteria
2.4. Variables’ Characteristics
2.5. Statistical Analysis
2.6. Outcome Measurements
3. Results
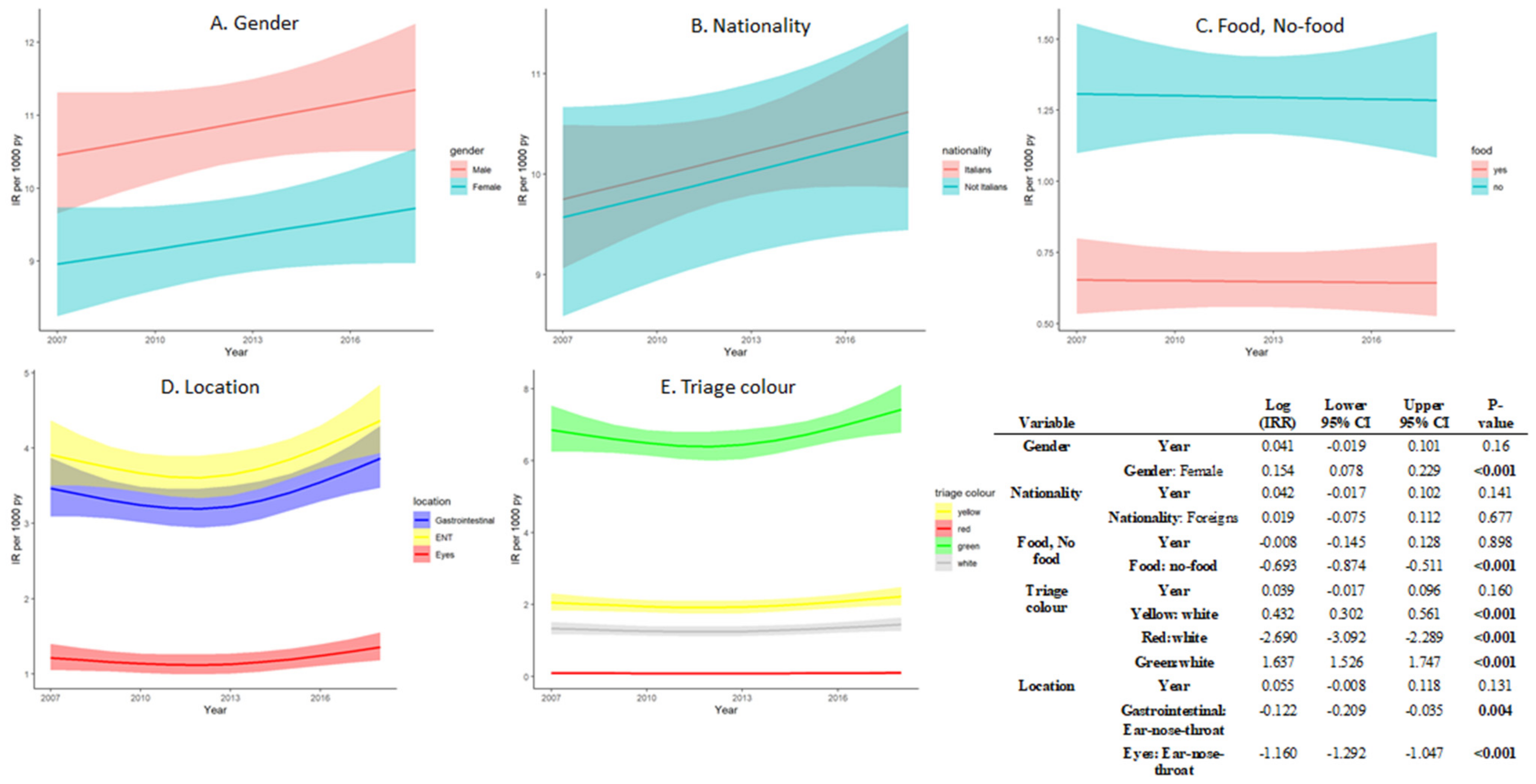
3.1. The Trends over Time of Foreign Body Injuries
3.2. Univariable and Multivariable Models
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Passali, D.; Gregori, D.; Lorenzoni, G.; Cocca, S.; Loglisci, M.; Passali, F.M.; Bellussi, L. Foreign Body Injuries in Children: A Review. Acta Otorhinolaryngol. Ital. 2015, 35, 265–271. [Google Scholar]
- Snidero, S.; Soriani, N.; Baldi, I.; Zobec, F.; Berchialla, P.; Gregori, D. Scale-up Approach in CATI Surveys for Estimating the Number of Foreign Body Injuries in the Aero-Digestive Tract in Children. Int. J. Environ. Res. Public. Health 2012, 9, 4056–4067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregori, D. The Susy Safe Project. A Web-Based Registry of Foreign Bodies Injuries in Children. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1663–1664. [Google Scholar] [CrossRef] [PubMed]
- The Susy Safe Project|Home. Available online: https://www.susysafe.org/index.php?lang=en (accessed on 27 September 2021).
- Ministero della salute Linee Di Indirizzo per La Prevenzione Del Soffocamento Da Cibo in Età Pediatrica 2017. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2618_allegato.pdf (accessed on 14 June 2019).
- Aydın, E.; Azzolina, D.; Baldas, S.; French, M.A.; Gregori, D.; Lorenzoni, G. Comparing Foreign Body Injuries Patterns between Turkey and European Countries: Are Female Turkish Children More Vulnerable? Int. J. Pediatr. Otorhinolaryngol. 2021, 142, 110605. [Google Scholar] [CrossRef] [PubMed]
- Lorenzoni, G.; Umihanić, S.; Azzolina, D.; Manza, E.; Brkić, F.; Gregori, D. A Novel Approach for Comparing Patterns of Foreign Body Injuries across Countries: A Case Study Comparing European Countries and Bosnia and Herzegovina. Int. J. Pediatr. Otorhinolaryngol. 2018, 105, 90–96. [Google Scholar] [CrossRef] [PubMed]
- French, M.A.; Lorenzoni, G.; Azzolina, D.; Baldas, S.; Gregori, D.; Gulati, A. Foreign Body Injuries in Children in India: Recommendations for Prevention from a Comparative Analysis with International Experience. Int. J. Pediatr. Otorhinolaryngol. 2019, 124, 6–13. [Google Scholar] [CrossRef]
- He, S.; Zuo, Z.-L. Different Anatomical Sites of the Foreign Body Injury with 2999 Children during 2012–2016. Chin. J. Traumatol. 2018, 21, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Berdan, E.A.; Sato, T.T. Pediatric Airway and Esophageal Foreign Bodies. Surg. Clin. N. Am. 2017, 97, 85–91. [Google Scholar] [CrossRef]
- Matsa, E.; Shi, J.; Wheeler, K.; McCarthy, T.; McGregor, M.; Leonard, J. Trends in US Emergency Department Visits for Pediatric Acute Ocular Injury. JAMA Ophthalmol. 2018, 136, 895–903. [Google Scholar] [CrossRef]
- Fischer, J.; Krishnamurthy, J.; Hansen, S.; Reeves, P.T. Austere Foreign Body Injuries in Children and Adolescents: A Characterization of Penile, Rectal, and Vaginal Injuries Presenting to Emergency Departments in the United States from 2008 to 2017. Pediatr. Emerg. Care 2019. [Google Scholar] [CrossRef]
- Sih, T.; Bunnag, C.; Ballali, S.; Lauriello, M.; Bellussi, L. Nuts and Seed: A Natural yet Dangerous Foreign Body. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, S49–S52. [Google Scholar] [CrossRef]
- Strickland, M.; Rosenfield, D.; Fecteau, A. Magnetic Foreign Body Injuries: A Large Pediatric Hospital Experience. J. Pediatr. 2014, 165, 332–335. [Google Scholar] [CrossRef]
- Gregori, D.; Salerni, L.; Scarinzi, C.; Morra, B.; Berchialla, P.; Snidero, S.; Corradetti, R.; Passali, D. ESFBI Study Group Foreign Bodies in the Upper Airways Causing Complications and Requiring Hospitalization in Children Aged 0–14 Years: Results from the ESFBI Study. Eur. Arch. Oto-Rhino-Laryngol. 2008, 265, 971–978. [Google Scholar] [CrossRef]
- Gregori, D.; Morra, B.; Berchialla, P.; Salerni, L.; Scarinzi, C.; Snidero, S.; Corradetti, R.; Passali, D. Foreign Bodies in the Ears Causing Complications and Requiring Hospitalization in Children 0–14 Age: Results from the ESFBI Study. Auris. Nasus. Larynx 2009, 36, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregori, D.; Salerni, L.; Scarinzi, C.; Morra, B.; Berchialla, P.; Snidero, S.; Corradetti, R.; Passali, D. ESFBI Study Group Foreign Bodies in the Nose Causing Complications and Requiring Hospitalization in Children 0–14 Age: Results from the European Survey of Foreign Bodies Injuries Study. Rhinology 2008, 46, 28–33. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention (CDC) Nonfatal Choking-Related Episodes among Children-United States, 2001. MMWR Morb. Mortal. Wkly. Rep. 2002, 51, 945–948.
- Passàli, D.; Lauriello, M.; Bellussi, L.; Passali, G.; Passali, F.; Gregori, D. Foreign Body Inhalation in Children: An Update. Acta Otorhinolaryngol. Ital. 2010, 30, 27–32. [Google Scholar]
- Sink, J.R.; Kitsko, D.J.; Mehta, D.K.; Georg, M.W.; Simons, J.P. Diagnosis of Pediatric Foreign Body Ingestion: Clinical Presentation, Physical Examination, and Radiologic Findings. Ann. Otol. Rhinol. Laryngol. 2016, 125, 342–350. [Google Scholar] [CrossRef]
- Rodríguez, H.; Passali, G.C.; Gregori, D.; Chinski, A.; Tiscornia, C.; Botto, H.; Nieto, M.; Zanetta, A.; Passali, D.; Cuestas, G. Management of Foreign Bodies in the Airway and Oesophagus. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, S84–S91. [Google Scholar] [CrossRef]
- Sinikumpu, J.-J.; Serlo, W. Confirmed and Suspected Foreign Body Injuries in Children during 2008–2013: A Hospital-Based Single Center Study in Oulu University Hospital. Scand. J. Surg. 2017, 106, 350–355. [Google Scholar] [CrossRef]
- Timmers, M.; Snoek, K.G.; Gregori, D.; Felix, J.F.; van Dijk, M.; van As, S.A.B. Foreign Bodies in a Pediatric Emergency Department in South Africa. Pediatr. Emerg. Care 2012, 28, 1348–1352. [Google Scholar] [CrossRef]
- Lorenzoni, G.; Azzolina, D.; Soriani, N.; Galadini, M.; Carle, F.; Gregori, D. Temporal and Regional Trends of Choking Injuries in Children in Italy, 2001–2013. Inj. Epidemiol. 2018, 5, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccotti, E.; Magnani, M.; Tubino, B.; Sartini, M.; Di Pietro, P. Assessment of the Triage System in a Pediatric Emergency Department. A Pilot Study on Critical Codes. J. Prev. Med. Hyg. 2008, 49, 120–123. [Google Scholar] [PubMed]
- Harrell, E.F., Jr. Rms: Regression Modeling Strategies; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Zeileis, A.; Kleiber, C.; Jackman, S. Regression Models for Count Data in R. J. Stat. Softw. 2008, 27, 1–25. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Dipasquale, V.; Romano, C.; Iannelli, M.; Tortora, A.; Melita, G.; Ventimiglia, M.; Pallio, S. Managing Pediatric Foreign Body Ingestions: A 10-Year Experience. Pediatr. Emerg. Care 2021. [Google Scholar] [CrossRef]
- Park, J.; Jung, J.; Kwak, Y.; Jung, J. Epidemiology of Pediatric Visits to the Emergency Department Due to Foreign Body Injuries in South Korea: Nationwide Cross-Sectional Study. Medicine (Baltimore) 2019, 98, e15838. [Google Scholar] [CrossRef]
- Sarafoleanu, C.; Ballali, S.; Gregori, D.; Bellussi, L.; Passali, D. Retrospective Study on Romanian Foreign Bodies Injuries in Children. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, S73–S75. [Google Scholar] [CrossRef]
- Chotigavanich, C.; Ballali, S.; Foltran, F.; Passali, D.; Bellussi, L.; Gregori, D. ESFBI Study Group Foreign Bodies Injuries in Children: Analysis of Thailand Data. Int. J. Pediatr. Otorhinolaryngol. 2012, 76 (Suppl. 1), S80–S83. [Google Scholar] [CrossRef]
- Gregori, D. The ESFBI Study Final Report; Franco Angeli: Milano, Italy, 2005; Volume 390, ISBN 88-464-6739-6. [Google Scholar]
- Shruti Jayachandra, G.D.E. A Systematic Review of Paediatric Foreign Body Ingestion: Presentation, Complications, and Management. Int. J. Pediatric Otorhinolaryngol. 2013, 77, 311–317. [Google Scholar] [CrossRef]
- European Union Directive 2009/48/EC of the European Parliament and of the Council of 18 June 2009 on the Safety of Toys 2019. Available online: https://data.europa.eu/eli/dir/2009/48/oj (accessed on 27 September 2021).
- Nichols, B.G.; Visotcky, A.; Aberger, M.; Braun, N.M.; Shah, R.; Tarima, S.; Brown, D.J. Pediatric Exposure to Choking Hazards Is Associated with Parental Knowledge of Choking Hazards. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 169–173. [Google Scholar] [CrossRef]
- Fano, C.; Lorenzoni, G.; Azzolina, D.; Giuliani, A.; French, M.; Campagna, S.; Berchialla, P.; Gregori, D. Perception of Choking Injury Risk Among Healthcare Students. J. Community Health 2019, 44, 974–981. [Google Scholar] [CrossRef]
- CHOP—Pacchetto Sicurezza Degli Alimenti Nelle Scuole. Available online: https://www.chop.school/ (accessed on 5 August 2019).
- Lorenzoni, G.; Azzolina, D.; Baldas, S.; Messi, G.; Lanera, C.; French, M.A.; Da Dalt, L.; Gregori, D. Increasing Awareness of Food-Choking and Nutrition in Children through Education of Caregivers: The CHOP Community Intervention Trial Study Protocol. BMC Public Health 2019, 19, 1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenzoni, G.; Lanera, C.; Azzolina, D.; Baldas, S.; Messi, G.; Gregori, D. Assessing School-Based Intervention Strategies to Foster the Prevention of Choking Injuries in Children: The Results of the CHOP (CHOking Prevention) Trial. Health Soc. Care Community 2021. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Level | N | Other ED Presentations | FB-Related Presentations | FB Presentations Odds Ratio | Overall | p Value |
|---|---|---|---|---|---|---|---|
| (N = 208,504) | (N = 3084) | (N = 211,588) | |||||
| Age (continuous) | 211,646 | 1/4/9 | 2/4/7 | 0.79 [0.74–0.85] | 1/4/9 | 0.003 | |
| Age categories | Infant-toddler (<2 y) | 211,646 | 38% (80,043) | 36% (1112) | * | 38% (81,155) | <0.001 |
| Preschooler (<6 y) | 23% (46,980) | 32% (980) | 1.5 [1.38–1.64] | 23% (47,960) | |||
| Schooler (>6 y) | 39% (81,481) | 32% (992) | 0.88 [0.8–0.96] | 39% (82,473) | |||
| Sex | Female | 211,646 | 44% (90,870) | 45% (1375) | * | 44% (92,245) | 0.265 |
| Male | 56% (117,634) | 55% (709) | 0.96 [0.89–1.03] | 56% (119,343) | |||
| Nationality | Not Italian | 211,646 | 22% (46,173) | 20% (617) | 22% (46,790) | 0.005 | |
| Italian | 78% (162,331) | 80% (2467) | 1.14 [1.04–1.24] | 78% (164,798) | |||
| Outcome | Other | 211,645 | 1% (1513) | 1% (37) | * | 1% (1550) | 0.023 |
| Death | 0% (9) | 0% (0) | Not estimable | 0% (9) | |||
| Discharged home | 94% (195,569) | 93% (2877) | 0.6 [0.43–0.84] | 94% (198,446) | |||
| Admitted | 5% (11,412) | 6% (170) | 0.61 [0.43–0.87] | 5% (11,582) | |||
| Triage color | White | 211,630 | 15% (31,201) | 13% (398) | * | 15% (31,599) | <0.001 |
| Green | 67% (140,244) | 66% (2046) | 1.14 [1.03–1.27] | 67% (142,290) | |||
| Yellow | 17% (35,368) | 20% (613) | 1.36 [1.2–1.54] | 17% (35,981) | |||
| Red | 1% (1691) | 1% (27) | 1.25 [0.85–1.85] | 1% (1718) | 0.263 |
| Variable | Level | N | Discharge | Admission to Hospital | Other | Overall | p Value |
|---|---|---|---|---|---|---|---|
| (N = 2877) | (N = 170) | (N = 37) | (N = 3084) | ||||
| Age (continuous) | 3084 | 2/4/7 | 1/2/5 | 2/4/7 | 02/04/2007 | <0.001 | |
| Age categories | Infant-toddler (<2 y) | 3084 | 35% (1007) | 55% (94) | 30% (11) | 36% (1112) | <0.001 |
| Preschooler(<6 y) | 32% (927) | 22% (38) | 41% (15) | 32% (980) | |||
| Schooler(>6 y) | 33% (943) | 22% (38) | 30% (11) | 32% (992) | |||
| Sex | Female | 3084 | 45% (1296) | 38% (65) | 38% (14) | 45% (1375) | 0.157 |
| Male | 55% (1581) | 62% (105) | 62% (23) | 55% (1709) | |||
| Nationality | Not Italian | 3084 | 20% (571) | 21% (35) | 30% (11) | 20% (617) | 0.322 |
| Italian | 80% (2306) | 79% (135) | 70% (26) | 80% (2467) | |||
| Foreign body type | No-food | 591 | 66% (365) | 71% (27) | 100% (2) | 67% (394) | 0.503 |
| Food | 34% (186) | 29% (11) | 0% (0) | 33% (197) | |||
| Foreign body site | Ears, nose, throat | 2566 | 44% (1061) | 65% (100) | 42% (8) | 46% (1169) | <0.001 |
| Gastrointestinal tract | 41% (974) | 35% (54) | 32% (6) | 40% (1034) | |||
| Eyes | 15% (357) | 1% (1) | 26% (5) | 14% (363) | |||
| Triage color | White | 3084 | 13% (382) | 6% (10) | 16% (6) | 13% (398) | <0.001 |
| Green | 68% (1958) | 38% (65) | 62% (23) | 66% (2046) | |||
| Yellow | 18% (524) | 48% (81) | 22% (8) | 20% (613) | |||
| Red | 0% (13) | 8% (14) | 0% (0) | 1% (27) |
| Year | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | |||||||||||||
| FB Events | 254 | 210 | 250 | 278 | 283 | 260 | 227 | 248 | 238 | 239 | 276 | 321 | |
| IR | 10.45 (9.24, 11.77) | 8.59( 7.51, 9.79) | 10.04 (8.87, 11.32) | 11.04 (9.82, 12.37) | 11.2 (9.97, 12.54) | 10.29 (9.11, 11.58) | 8.89 (7.81, 10.09) | 9.53 (8.42, 10.75) | 9.1 (8.02, 10.29) | 9.22 (8.13, 10.43) | 10.79 (9.59, 12.09) | 12.66 (11.35, 14.08) | 0.15 |
| % ED presentations | 1.5 (1.31, 1.67) | 1.2 (1.04, 1.36) | 1.4 (1.26, 1.61) | 1.6 (1.42, 1.79) | 1.6 (1.43, 1.8) | 1.5 (1.37, 1.74) | 1.4 (1.21, 1.57) | 1.4 (1.27, 1.63) | 1.4 (1.28, 1.64) | 1.4 (1.24, 1.6) | 1.4 (1.24, 1.57) | 1.6 (1.41, 1.75) | 0.472 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ocagli, H.; Azzolina, D.; Bressan, S.; Bottigliengo, D.; Settin, E.; Lorenzoni, G.; Gregori, D.; Da Dalt, L. Epidemiology and Trends over Time of Foreign Body Injuries in the Pediatric Emergency Department. Children 2021, 8, 938. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100938
Ocagli H, Azzolina D, Bressan S, Bottigliengo D, Settin E, Lorenzoni G, Gregori D, Da Dalt L. Epidemiology and Trends over Time of Foreign Body Injuries in the Pediatric Emergency Department. Children. 2021; 8(10):938. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100938
Chicago/Turabian StyleOcagli, Honoria, Danila Azzolina, Silvia Bressan, Daniele Bottigliengo, Elisabetta Settin, Giulia Lorenzoni, Dario Gregori, and Liviana Da Dalt. 2021. "Epidemiology and Trends over Time of Foreign Body Injuries in the Pediatric Emergency Department" Children 8, no. 10: 938. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100938