
Adaptation, Translation and Validation of the Food Allergy Quality of Life Questionnaire-Parent Form (FAQLQ-PF): The Malay Version

 , , ,
, , ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Tool
2.3. Conduct of the Study
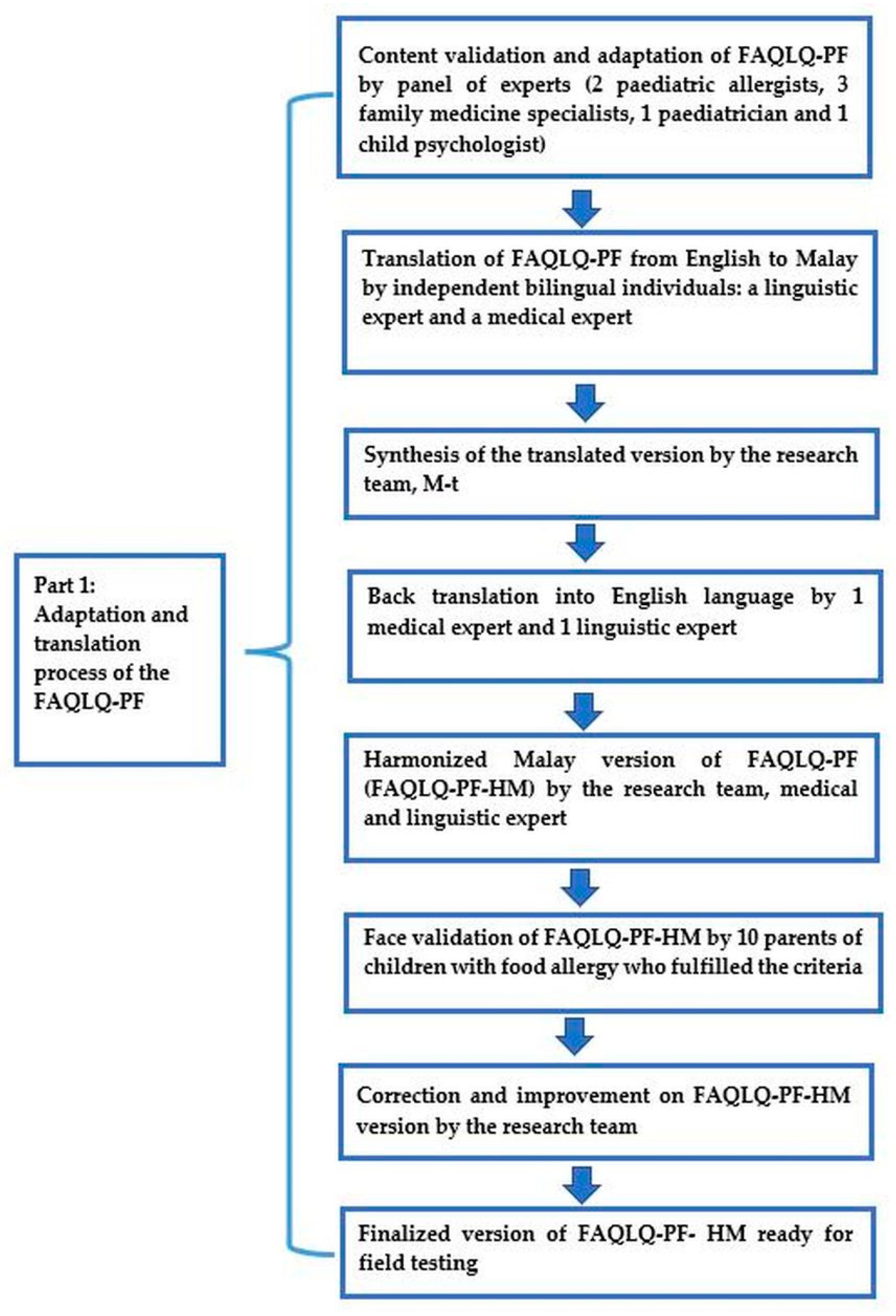
2.3.1. Part 1: Cross-Cultural Adaptation, Translation and Face Validation
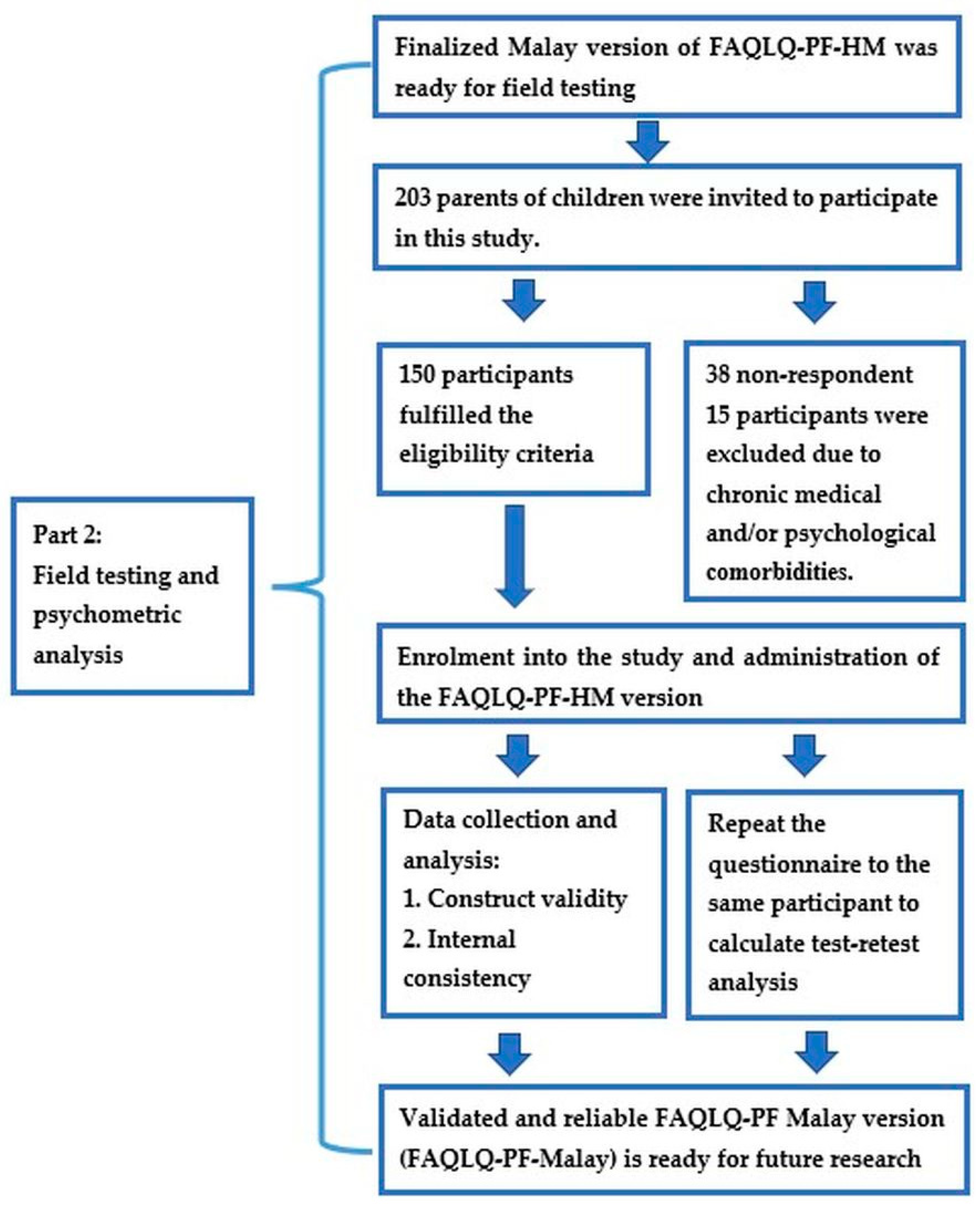
2.3.2. Part 2: Field Testing and Psychometric Analysis
2.4. Statistical Analysis
3. Results
3.1. Participant Demographics
3.2. Cross-Cultural Adaptation, Translation, and Face Validation
3.3. Psychometric Analysis
3.4. Reliability
4. Discussion
Strengths, Limitations and Implication for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Branum, A.M.; Lukacs, S.L. Food Allergy Among Children in the United States. Pediatrics 2009, 124, 1549–1555. [Google Scholar] [CrossRef] [Green Version]
- Nwaru, B.I.; Hickstein, L.; Panesar, S.S.; Roberts, G.; Muraro, A.; Sheikh, A. Prevalence of common food allergies in Europe: A systematic review and meta-analysis. Eur. J. Allergy Clin. Immunol. 2014, 69, 992–1007. [Google Scholar] [CrossRef]
- Prescott, S.; Allen, K.J. Food allergy: Riding the second wave of the allergy epidemic. Pediatric Allergy Immunol. 2011, 22, 155–160. [Google Scholar] [CrossRef]
- Savage, J.; Johns, C.B. Food Allergy Epidemiology and Natural History Food allergy Epidemiology Natural history Peanut Milk Egg. Immunol. Allergy Clin. NA 2015, 35, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Soller, L.; Ben-Shoshan, M.; Harrington, D.W.; Fragapane, J.; Joseph, L.; Pierre, Y.S.; Godefroy, S.B.; La Vieille, S.; Elliott, S.J.; Clarke, A.E. Overall prevalence of self-reported food allergy in Canada. J. Allergy Clin. Immunol. 2012, 130, 986–988. [Google Scholar] [CrossRef]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Lowe, A.J.; Matheson, M.C.; Ponsonby, A.L.; Wake, M.; Tang, M.L.K.; Dharmage, S.C.; et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J. Allergy Clin. Immunol. 2011, 127, 668–676.e662. [Google Scholar] [CrossRef]
- Kemp, A.; Chiang, W.C.; Gerez, I.; Goh, A.; Liew, W.K.; Shek, L.; van Bever, H.P.S.; Lee, B.W. Childhood food allergy: A singaporean perspective. Ann. Acad. Med. Singap. 2010, 39, 404–411. [Google Scholar]
- Kim, J.; Chang, E.; Han, Y.; Ahn, K.; Lee, S.I. The incidence and risk factors of immediate type food allergy during the first year of life in Korean infants: A birth cohort study. Pediatric Allergy Immunol. 2011, 22, 715–719. [Google Scholar] [CrossRef]
- Wu, T.C.; Tsai, T.C.; Huang, C.F.; Chang, F.Y.; Lin, C.C.; Huang, I.F.; Chu, C.H.; Lau, B.H.; Wu, L.; Peng, H.J.; et al. Prevalence of food allergy in Taiwan: A questionnaire-based survey. Intern. Med. J. 2012, 42, 1310–1315. [Google Scholar] [CrossRef]
- Yadav, A.; Naidu, R. Clinical manifestation and sensitization of allergic children from Malaysia. Asia Pac. Allergy 2015, 5, 78–83. [Google Scholar] [CrossRef] [Green Version]
- Sicherer, S.H.; Sampson, H.A. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J. Allergy Clin. Immunol. 2014, 133, 291–307.E5. [Google Scholar] [CrossRef]
- Muraro, A.; Agache, I.; Clark, A.; Sheikh, A.; Roberts, G.; Akdis, C.A.; Borrego, L.M.; Higgs, J.; Hourihane, J.O.; Jorgensen, P.; et al. EAACI Food Allergy and Anaphylaxis Guidelines: Managing patients with food allergy in the community. Allergy Eur. J. Allergy Clin. Immunol. 2014, 69, 1046–1057. [Google Scholar] [CrossRef]
- Graham, F.; Eigenmann, P.A. Clinical implications of food allergen thresholds. Clin. Exp. Allergy 2018, 48, 632–640. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Noone, S.A.; Muñoz-Furlong, A. The impact of childhood food allergy on quality of life. Ann. Allergy Asthma Immunol. 2001, 87, 461–464. [Google Scholar] [CrossRef]
- Bollinger, M.E.; Dahlquist, L.M.; Mudd, K.; Sonntag, C.; Dillinger, L.; McKenna, K. The impact of food allergy on the daily activities of children and their families. Ann. Allergy Asthma Immunol. 2006, 96, 415–421. [Google Scholar] [CrossRef]
- Roy, K.M.; Roberts, M.C. Peanut allergy in children: Relationships to health-related quality of life, anxiety, and parental stress. Clin. Pediatrics 2011, 50, 1045–1051. [Google Scholar] [CrossRef]
- Williams, N.A.; Parra, G.R.; Elkin, T.D. Subjective distress and emotional resources in parents of children with food allergy. Child. Health Care 2009, 38, 213–227. [Google Scholar] [CrossRef]
- Cohen, B.L.; Noone, S.; Muñoz-Furlong, A.; Sicherer, S.H. Development of a questionnaire to measure quality of life in families with a child with food allergy. J. Allergy Clin. Immunol. 2004, 114, 1159–1163. [Google Scholar] [CrossRef]
- Natalie, J.A.; Rosemary, M.K.; Susan, K.; Jonathan, O.B.H. Assessment of quality of life in children with peanut allergy. Pediatric Allergy Immunol. 2003, 14, 378–382. [Google Scholar]
- Knibb, R.C.; Ibrahim, N.F.; Petley, R.; Cummings, A.J.; King, R.M.; Roberts, G.; Erlewyn-Lajeunesse, M.; Lucas, J.S. Validation of the Paediatric Food Allergy Quality of Life Questionnaire (PFA-QL). Pediatric Allergy Immunol. 2013, 24, 288–292. [Google Scholar] [CrossRef]
- van der Velde, J.L.; Flokstra-de Blok, B.M.; Vlieg-Boerstra, B.J.; Oude Elberink, J.N.; DunnGalvin, A.; Hourihane, J.O.; Duiverman, E.J.; Dubois, A.E. Development, validity and reliability of the food allergy independent measure (FAIM). Allergy 2010, 65, 630–635. [Google Scholar] [CrossRef]
- DunnGalvin, A.; De BlokFlokstra, B.M.J.; Burks, A.W.; Dubois, A.E.J.; Hourihane, J.O.B. Food allergy QoL questionnaire for children aged 0-12 years: Content, construct, and cross-cultural validity. Clin. Exp. Allergy 2008, 38, 977–986. [Google Scholar] [CrossRef]
- Mizuno, Y.; Ohya, Y.; Nagao, M.; DunnGalvin, A.; Fujisawa, T. Validation and reliability of the Japanese version of the Food Allergy Quality of Life Questionnaire-Parent Form. Allergol. Int. 2017, 66, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Bartolla, E.M.N.; Selvaa, B.; Badillob, R.; Pereiraa, G.; Uixeraa, S.; Nietoa, A.Á.M. Validation of a Spanish version of the EuroPrevall Food Allergy Quality of Life Questionnaire-Parental Form. Allergol. Immunopathol. 2017, 46, 82–86. [Google Scholar] [CrossRef]
- Arik, Y.E.; Cavkaytar, O.; Buyuktiryaki, B.; Soyer, O.; Sahiner, U.M.; Sekerel, B.E.; DunnGalvin, A.; Karabulut, E.; Sackesen, C. Factors Affecting Food Allergy-Related Quality of Life From Parents’. Perception in Turkish Children. Allergy Asthma Immunol. Res. 2018, 10, 379–386. [Google Scholar] [CrossRef]
- Couto, M.; Silva, D.; Piedade, S.; Borrego, L.; Flokstra-de Blok, B.; Dunn Galvin, A.; Morais-Almeida, M. Translation to Portuguese and cultural adaptation of Food Allergy Quality of Life Questionnaire-Parent Form (FAQLQ-PF). Eur. Ann. Allergy Clin. Immunol. 2016, 48, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Wassenberg, J.; Cochard, M.M.; Dunngalvin, A.; Ballabeni, P.; Flokstra-de Blok, B.M.; Newman, C.J.; Hofer, M.; Eigenmann, P.A. Parent perceived quality of life is age-dependent in children with food allergy. Pediatric Allergy Immunol. 2012, 23, 412–419. [Google Scholar] [CrossRef]
- Protudjer, J.L.; Jansson, S.A.; Ostblom, E.; Arnlind, M.H.; Bengtsson, U.; Dahlen, S.E.; Kallstrom, -B.I.; Marklund, B.; Middelveld, R.J.; Rentzos, G.; et al. Health-related quality of life in children with objectively diagnosed staple food allergy assessed with a disease-specific questionnaire. Acta Paediatr. 2015, 104, 1047–1054. [Google Scholar] [CrossRef]
- van der Velde, J.L.; Flokstra-de Blok, B.M.; Dunngalvin, A.; Hourihane, J.O.; Duiverman, E.J.; Dubois, A.E. Parents report better health-related quality of life for their food-allergic children than children themselves. Clin. Exp. Allergy 2011, 41, 1431–1439. [Google Scholar] [CrossRef]
- Oksana, M.A.M.; Lesya, B.; Taras, G.; Oksana, K.; Olesya, B.; Olena, S.; Natalia, L.; Bertine, F.B. Translation, adaptation, and initial validation of the Food Allergy Quality of Life Questionnaire–Parent Form (0–12 years) in Ukrainian language. Pedaitria Polska 2021, 96, 47–52. [Google Scholar]
- Vale, S.; Smith, J.; Said, M.; Mullins, R.J.; Loh, R. ASCIA guidelines for prevention of anaphylaxis in schools, pre-schools and childcare: 2015 update. J. Paediatr. Child Health 2015, 51, 949–954. [Google Scholar] [CrossRef] [Green Version]
- Yusoff, M.S.B. ABC of Content Validation and Content Validity Index Calculation. Educ. Med. J. 2019, 11, 49–54. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila. PA 1976) 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Yusoff, M.S.B. ABC of response process validation and face validity index calculation. Educ. Med. J. 2019, 11, 55–61. [Google Scholar] [CrossRef]
- Pallant, J. Spss Survival Manual a Step by Step Guide to Data Analysis Ssing SPSS, 4th ed.; Allen & Unwin: New South Wales, Australia, 2011. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; SAGE: London, UK, 2009. [Google Scholar]
- Costello, A.B.; Osborne, J.W. Best Practices in Exploratory Factor Analysis: Four Recommendations for Getting the Most From Your Analysis. Pract. Assess. Res. Eval. 2005, 10, 1–9. [Google Scholar]
- Wood, N.D.; Akloubou, G.D.C.; Bowling, J. Combining Parallel and Exploratory Factor Analysis in Identifying Relationship Scales in Secondary Data. Marriage Fam. Rev. 2015, 51, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Finch, W.H. Using Fit Statistic Differences to Determine the Optimal Number of Factors to Retain in an Exploratory Factor Analysis. Educ. Psychol. Meas. 2020, 80, 217–241. [Google Scholar] [CrossRef]
- Holli, A.; DeVon, M.E.B.; Patricia, M.-W.; Diane, M.E.; Hayden, S.J.; Lazzara, D.J.; Suzanne, M.S.; Elizabeth, K.-P.; DeVon, H.A.; Block, M.E.; et al. psychometric Toolbox for testing Validity and Reliability. J. Nurs. Scholarship. 2007, 39, 155–164. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Chung, D. The Eight Stages of Psychosocial Protective Development. J. Behav. Brain Sci. 2018, 8, 369–398. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.; Santo, R.M.; Guillemin, F. A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensus. J. Clin. Epidemiol. 2015, 68, 435–441. [Google Scholar] [CrossRef]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.; Bouter, L.M.; de Vet, H.C. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Kyriazos, T.A. Applied Psychometrics: Sample Size and Sample Power Considerations in Factor Analysis (EFA, CFA) and SEM in General. Psychology 2018, 9, 2207–2230. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | n (%) | Median (IQR) |
|---|---|---|
| Age (years), median (IQR) | 5 (7) | |
| Age Group (years) | ||
| <4 years old 4–6 years old 7–12 years old | 57 (38%) 32 (21%) 61 (41%) | |
| Gender | ||
| Male Female | 29 (19%) 121 (81%) | |
| Ethnicity | ||
| Malay Chinese Indian | 141 (94%) 7 (4.7%) 2 (1.3%) | |
| Severity of food allergy | ||
| Mild to moderate Severe | 95 (63%) 55 (37%) | |
| Number of food Allergens | ||
| 1 2 3 4 ≥5 | 38 (25%) 41 (27%) 21 (14%) 21 (14%) 29 (20%) | |
| Type of food allergens | ||
| Cow’s Milk/Dairy Egg Soy Wheat Peanut Tree nut Fish Shellfish Others | 60 (40%) 68 (45%) 26 (17%) 24 (16%) 34 (23%) 16 (11%) 29 (19%) 70 (47%) 27 (43%) |
| Item | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|
| Item 14: “Because of food allergy, my child’s ability to take part has been limited in social activities in other people’s houses (sleepovers, parties, playtime)”/ “Disebabkan alahan makanan, keupayaan anak saya untuk mengambil bahagian telah terbatas dalam aktiviti sosial di rumah orang lain. (bermalam, majlis keraian, masa bermain” | 0.903 | ||
| Item 15: “Because of food allergy, my child’s ability to take part has been limited in preschool/school events involving food (class parties/treats/ lunchtime)”/“Disebabkan alahan makanan, keupayaan anak saya untuk mengambil bahagian telah terbatas dalam acara prasekolah/sekolah yang melibatkan makanan (majlis keraian kelas/makanan ringan/waktu makan tengah hari” | 0.737 | ||
| Item 13: “Because of food allergy, my child’s social environment is restricted because of limitations on holiday destinations we can safely go to as a family”/ “Disebabkan alahan makanan, persekitaran sosial anak saya terhad disebabkan batasan terhadap destinasi percutian yang kami sekeluarga boleh pergi dengan selamat” | 0.731 | ||
| Item 12: “Because of food allergy, my child’s social environment is restricted because of limitations on restaurants we can safely go to as family”/“Disebabkan alahan makanan, persekitaran sosial anak saya terhad disebabkan batasan terhadap restoran yang kami sekeluarga boleh pergi dengan selamat” | 0.688 | ||
| Item 22: “Because of food allergy, my child feels frustrated by social restrictions”/“Disebabkan alahan makanan, anak saya berasa kecewa dengan had sosial” | 0.660 | ||
| Item 19: “Because of food allergy, my child feels upset that family social outings have been restricted by the need to plan ahead”/“Disebabkan alahan makanan, anak saya berasa sedih kerana acara sosial keluarga telah terbatas oleh keperluan untuk merancang lebih awal” | 0.636 | 0.443 | |
| Item 9: “Because of food allergy, my child has been negatively affected by receiving more attention than other children of his/her age”/“Disebabkan alahan makanan, anak saya telah terkesan secara negatif dengan mendapat perhatian yang lebih berbanding kanak-kanak lain yang seusia dengannya” | 0.605 | ||
| Item 5: “Because of food allergy, my child feels concerned that I am worried that he/she will have a reaction to food”/“Disebabkan alahan makanan, anak saya berasa khuatir bahawa saya bimbang dia akan mengalami reaksi terhadap makanan” | 0.545 | ||
| Item 16: “Because of food allergy, my child feels worried when going to unfamiliar places”/“Disebabkan alahan makanan, anak saya berasa bimbang apabila pergi ke tempat yang dia tidak biasa” | 0.542 | ||
| Item 11: “Because of food allergy, my child has been negatively affected by his/her environment being more restricted than other children of his/her age”/ “Disebabkan alahan makanan, anak saya telah terkesan secara negatif dengan persekitarannya yang lebih terbatas daripada kanak-kanak lain yang seusia dengannya” | 0.520 | ||
| Item 18: “Because of food allergy, my child feels ‘left out’ in activities involving food”/“Disebabkan alahan makanan, anak saya berasa ‘terpinggir’ dalam aktiviti yang melibatkan makanan.” | 0.497 | 0.456 | |
| Item 17: “Because of food allergy, my child feels concerned that he/she must always be cautious about food”/“Disebabkan alahan makanan, anak saya berasa khuatir bahawa dia mesti sentiasa berwaspada tentang makanan” | 0.745 | ||
| Item 24: “Because of food allergy, my child is more cautious in general than other children of his/her age”/“Disebabkan alahan makanan, anak saya secara amnya lebih berhati-hati berbanding kanak-kanak lain yang seusia dengannya” | 0.706 | ||
| Item 28: “Because of food allergy, my child feels many people do not understand the serious nature of food allergy”/“Disebabkan alahan makanan, anak saya berasa ramai orang tidak memahami tahap keseriusan alahan makanan” | 0.703 | ||
| Item 1: “Because of food allergy, my child feels worried about food”/“Disebabkan alahan makanan, anak saya berasa bimbang tentang makanan” | 0.699 | ||
| Item 20: “Because of food allergy, my child feels concerned about accidentally eating an ingredient to which he/she is allergic”/“Disebabkan alahan makanan, anak saya berasa khuatir jika tidak sengaja termakan bahan makanan yang dia alah” | 0.584 | ||
| Item 29: “Because of food allergy, my child feels concerned by poor labelling on food products”/“Disebabkan alahan makanan, anak saya berasa khuatir dengan pelabelan yang tidak lengkap pada bahan makanan” | 0.514 | ||
| Item 4: “Because of food allergy, my child feels afraid to try unfamiliar foods”/ “Disebabkan alahan makanan, anak saya berasa takut mencuba makanan yang dia tidak biasa” | 0.509 | ||
| Item 26: “Because of food allergy, my child wishes his/her food allergy would go away”/“Disebabkan alahan makanan, anak saya berharap agar alahan makanannya akan hilang” | 0.454 | ||
| Item 7: “Because of food allergy, my child experiences emotional distress”/ “Disebabkan alahan makanan, anak saya mengalami tekanan emosi” | 0.811 | ||
| Item 6: “Because of food allergy, my child experiences physical distress”/ “Disebabkan alahan makanan, anak saya mengalami tekanan fizikal” | 0.802 | ||
| Item 3: “Because of food allergy, my child feels frustrated by dietary restriction”/“Disebabkan alahan makanan, anak saya berasa kecewa dengan pemakanan yang terbatas” | 0.771 | ||
| Item 2: “Because of food allergy, my child feels different from other children”/ “Disebabkan alahan makanan, anak saya berasa berbeza daripada kanak-kanak lain” | 0.745 | ||
| Item 8: “Because of food allergy, my child has a lack of variety in his /her diet”/ “Disebabkan alahan makanan, anak saya mempunyai kekurangan variasi dalam pemakanannya” | 0.711 | ||
| Item 25: “Because of food allergy, my child is not as confident as other children of his/her age in social situations”/“Disebabkan alahan makanan, anak saya kurang berkeyakinan dalam situasi sosial berbanding kanak-kanak lain yang seusia dengannya” | 0.639 | 0.457 | |
| Item 21: “Because of food allergy, my child feels worried when eating with unfamiliar adults/children”/“Disebabkan alahan makanan, anak saya berasa Bimbang ketika makan dengan orang dewasa/kanak-kanak yang dia tidak biasa” | 0.452 | 0.417 |
| Subscale | Number of Items | Cronbach’s Alpha | Corrected Item-Total Correlation | Cronbach’s Alpha If Item Deleted | Intraclass Correlation Coefficient, ICC (95%CI) |
|---|---|---|---|---|---|
| Social and dietary implication | 11 | 0.94 | |||
| Item 5 | 0.74 | 0.94 | 0.84 (0.53–0.94) | ||
| Item 9 | 0.63 | 0.94 | 0.86 (0.72–0.93) | ||
| Item 11 | 0.70 | 0.94 | 0.81 (0.64–0.90) | ||
| Item 12 | 0.81 | 0.93 | 0.85 (0.71–0.92) | ||
| Item 13 | 0.79 | 0.94 | 0.87 (0.74–0.93) | ||
| Item 14 | 0.80 | 0.93 | 0.93 (0.87–0.97) | ||
| Item 15 | 0.80 | 0.94 | 0.90 (0.71–0.96) | ||
| Item 16 | 0.70 | 0.94 | 0.85 (0.56–0.95) | ||
| Item 18 | 0.80 | 0.93 | 0.90 (0.74–0.97) | ||
| Item 19 | 0.80 | 0.94 | 0.90 (0.71–0.96) | ||
| Item 22 | 0.69 | 0.94 | 0.89 (0.54–0.97) | ||
| Food anxiety | 8 | 0.88 | |||
| Item 1 | 0.58 | 0.88 | 0.79 (0.60–0.89) | ||
| Item 4 | 0.60 | 0.87 | 0.77 (0.56–0.88) | ||
| Item 17 | 0.68 | 0.87 | 0.85 (0.55–0.95) | ||
| Item 20 | 0.70 | 0.86 | 0.81 (0.46–0.94) | ||
| Item 24 | 0.77 | 0.86 | 0.88 (0.64–0.96) | ||
| Item 26 | 0.55 | 0.88 | 0.97 (0.90–0.99) | ||
| Item 28 | 0.75 | 0.86 | 0.93 (0.72–0.98) | ||
| Item 29 | 0.63 | 0.87 | 0.89 (0.60–0.97) | ||
| Emotional and physical impact | 7 | 0.91 | |||
| Item 2 | 0.77 | 0.90 | 0.80 (0.60–0.90) | ||
| Item 3 | 0.71 | 0.89 | 0.54 (0.10–0.77) | ||
| Item 6 | 0.79 | 0.90 | 0.78 (0.58–0.90) | ||
| Item 7 | 0.84 | 0.88 | 0.79 (0.60–0.90) | ||
| Item 8 | 0.66 | 0.90 | 0.83 (0.68–0.91) | ||
| Item 21 | 0.69 | 0.90 | 0.59 (0.25–0.86) | ||
| Item 25 | 0.66 | 0.90 | 0.74 (0.28–0.91) | ||
| Overall | 26 | 0.95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, I.S.; Baharudin, N.; Isa, M.R.; Ismail, I.H.; Mohamed-Yassin, M.-S.; Kamarudin, I.K.; Abdul Latiff, A.H.; Zahedi, F.D.; Ali, A.; Arshad, A.I. Adaptation, Translation and Validation of the Food Allergy Quality of Life Questionnaire-Parent Form (FAQLQ-PF): The Malay Version. Children 2021, 8, 1050. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111050
Ibrahim IS, Baharudin N, Isa MR, Ismail IH, Mohamed-Yassin M-S, Kamarudin IK, Abdul Latiff AH, Zahedi FD, Ali A, Arshad AI. Adaptation, Translation and Validation of the Food Allergy Quality of Life Questionnaire-Parent Form (FAQLQ-PF): The Malay Version. Children. 2021; 8(11):1050. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111050
Chicago/Turabian StyleIbrahim, Izyana Syazlin, Noorhida Baharudin, Mohamad Rodi Isa, Intan Hakimah Ismail, Mohamed-Syarif Mohamed-Yassin, Intan Kartika Kamarudin, Amir Hamzah Abdul Latiff, Farah Dayana Zahedi, Adli Ali, and Azuin Izzati Arshad. 2021. "Adaptation, Translation and Validation of the Food Allergy Quality of Life Questionnaire-Parent Form (FAQLQ-PF): The Malay Version" Children 8, no. 11: 1050. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111050