
The Impact of Clinical Atropine Use in Taiwanese Schoolchildren: Changes in Physiological Characteristics and Visual Functions



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Procedures
2.3. Statistics
3. Results
3.1. Subjects
3.2. Effects of Atropine on Pupil Sizes, Intraocular Pressure, and Visual Acuity
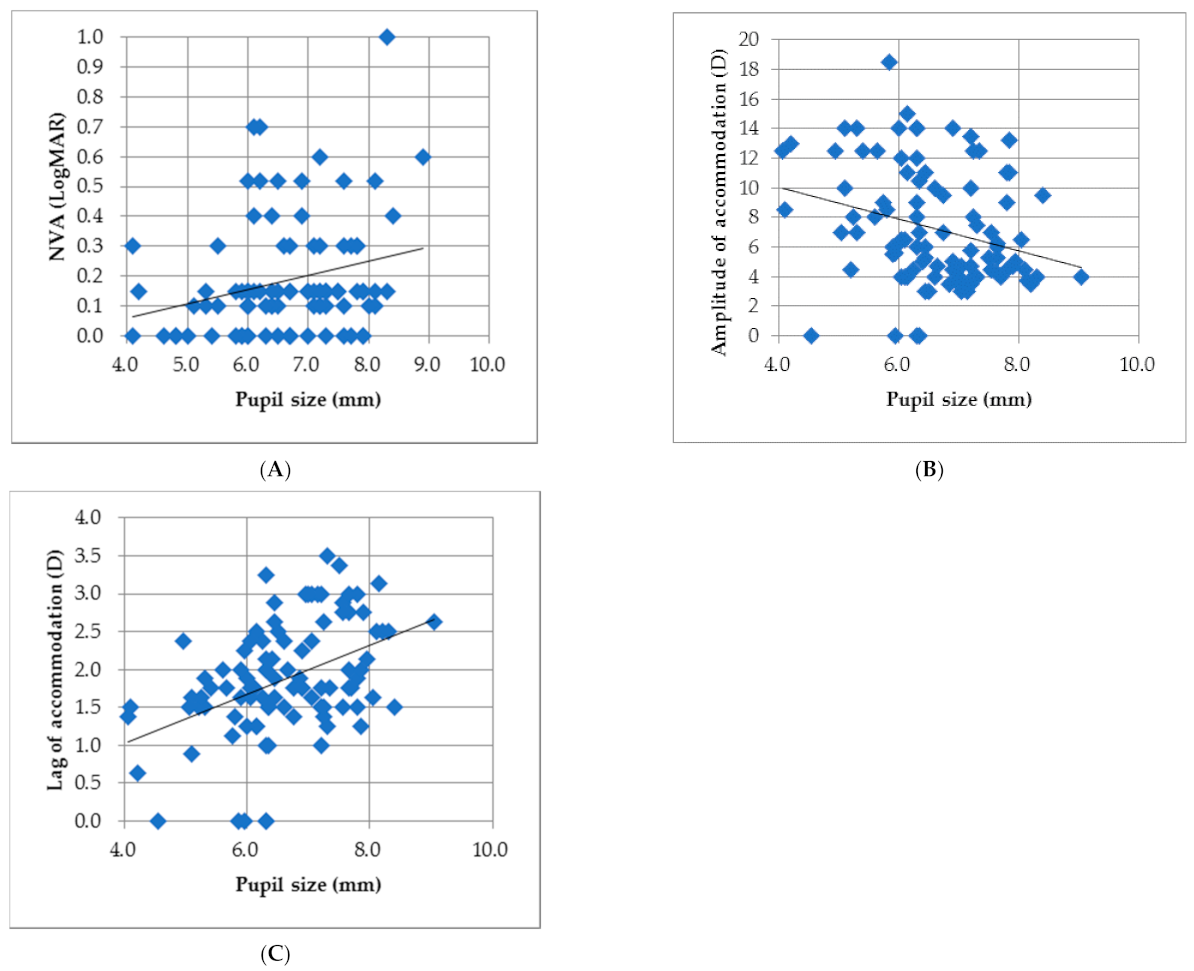
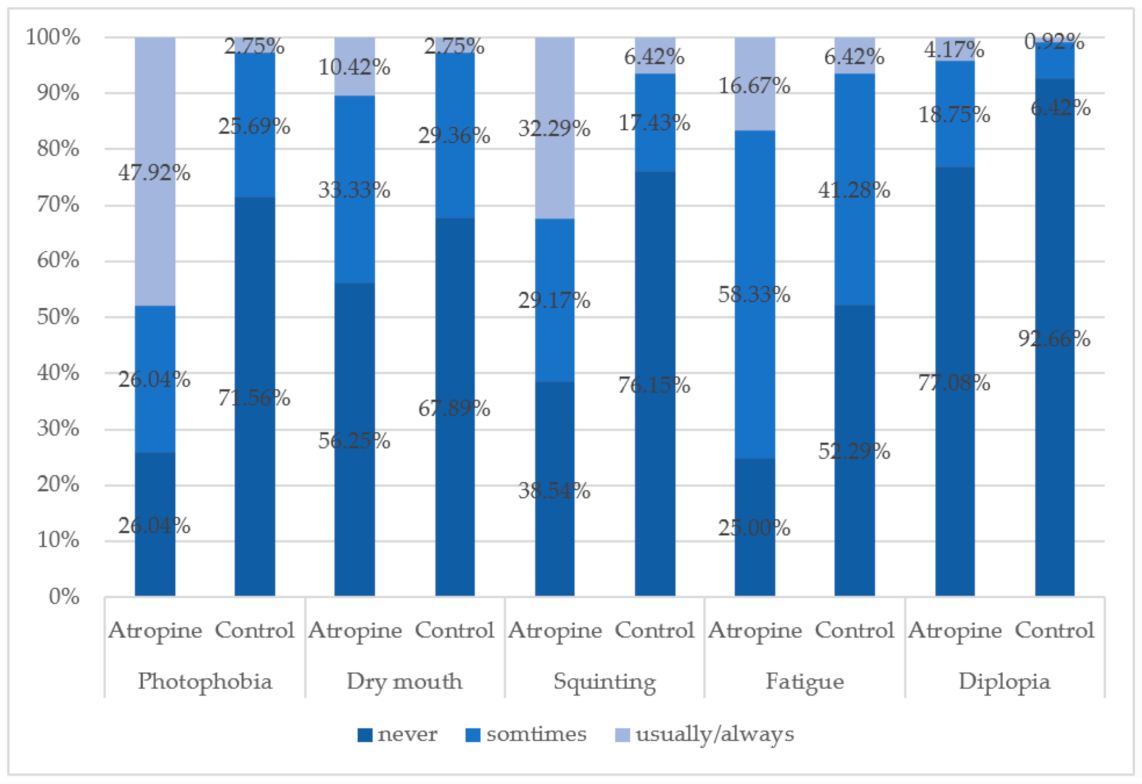
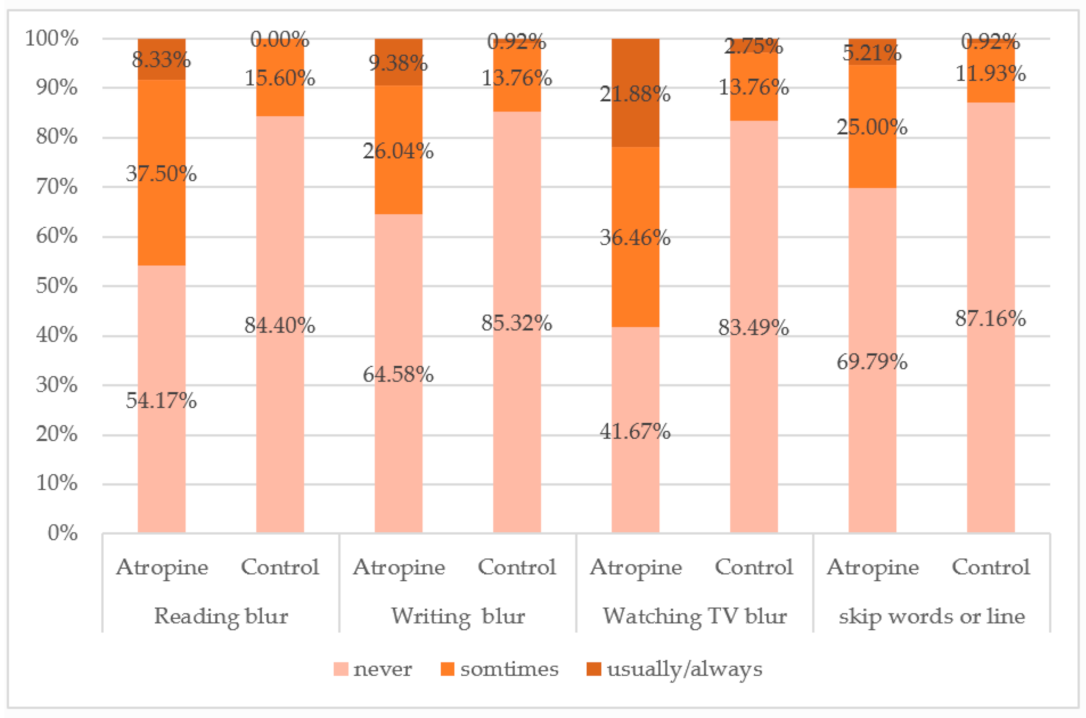
3.3. Effects of Atropine on Visual Function
4. Discussion
5. Study Limitations
- (i)
- Due to the issue of drug administration, the information of subject medication history can only be collected by using a questionnaire and which mainly relies on the parents’ memory. So, it would be optimal to collaborate with ophthalmologists in the future for both population allocation and medical database sharing.
- (ii)
- The concentrations of the atropine eyedrops were recorded based on the medications the children were using at the time point of data collection. However, there may be some who changed the doses in the past 6 months prior to the examination. Again, it would be beneficial to work with ophthalmologists to solve this problem and keep the doses fixed.
- (iii)
- To examine the effect of atropine dose on visual function and ocular physical changes, it is required to recruit more participants using different doses of atropine eyedrops.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourne, R.R.; Stevens, G.A.; White, R.A.; Smith, J.L.; Flaxman, S.R.; Price, H.; Jonas, J.B.; Keeffe, J.; Leasher, J.; Naidoo, K.; et al. Causes of vision loss worldwide, 1990–2010: A systematic analysis. Lancet Glob. Health 2013, 1, e339–e349. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.L.K.; Shih, Y.F.; Hsiao, C.K.; Chen, C.J. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann. Acad. Med. Singap. 2004, 33, 27–33. [Google Scholar]
- Grzybowski, A.; Kanclerz, P.; Tsubota, K.; Lanca, C.; Saw, S.-M. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020, 20, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.-K.; Lee, J.H.; Kakizaki, H.; Jee, D. Prevalence of myopia and its association with body stature and educational level in 19-year-old male conscripts in Seoul, South Korea. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5579–5583. [Google Scholar] [CrossRef] [Green Version]
- Vitale, S.; Sperduto, R.D.; Ferris, F.L. Increased prevalence of myopia in the United States between 1971–1972 and 1999–2004. Arch. Ophthalmol. 2009, 127, 1632–1639. [Google Scholar] [CrossRef] [Green Version]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.; Resnikoff, S. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Wu, A.; Zhang, L.; Wang, W.; Chen, X.; Yu, X.; Wang, K. The increasing prevalence of myopia and high myopia among high school students in Fenghua city, eastern China: A 15-year population-based survey. BMC Ophthalmol. 2018, 18, 159. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.H.; Liu, Y.L.; Ma, I.H.; Su, C.C.; Lin, C.W.; Lin, L.L.; Hsiao, C.K.; Wang, I.J. Evolution of the Prevalence of Myopia among Taiwanese Schoolchildren: A Review of Survey Data from 1983 through 2017. Ophthalmology 2021, 128, 290–301. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Richdale, K. Myopia Control 2020: Where are we and where are we heading? Ophthalmic Physiol. Opt. 2020, 40, 254–270. [Google Scholar] [CrossRef] [PubMed]
- Kang, P. Optical and pharmacological strategies of myopia control. Clin. Exp. Optom. 2018, 101, 321–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBrien, N.A.; Moghaddam, H.O.; Reeder, A.P. Atropine reduces experimental myopia and eye enlargement via a nonaccommodative mechanism. Investig. Ophthalmol. Vis. Sci. 1993, 34, 205–215. [Google Scholar]
- Barathi, V.A.; Beuerman, R.W. Molecular mechanisms of muscarinic receptors in mouse scleral fibroblasts: Prior to and after induction of experimental myopia with atropine treatment. Mol. Vis. 2011, 17, 680. [Google Scholar]
- Stone, R.A.; Pardue, M.T.; Iuvone, P.M.; Khurana, T.S. Pharmacology of myopia and potential role for intrinsic retinal circadian rhythms. Exp. Eye Res. 2013, 114, 35–47. [Google Scholar] [CrossRef] [Green Version]
- McBrien, N.A.; Cornell, L.M.; Gentle, A. Structural and ultrastructural changes to the sclera in a mammalian model of high myopia. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2179–2187. [Google Scholar]
- Prepas, S.B. Light, literacy and the absence of ultraviolet radiation in the development of myopia. Med. Hypotheses 2008, 70, 635–637. [Google Scholar] [CrossRef]
- Nickla, D.L.; Zhu, X.; Wallman, J. Effects of muscarinic agents on chick choroids in intact eyes and eyecups: Evidence for a muscarinic mechanism in choroidal thinning. Ophthalmic Physiol. Opt. 2013, 33, 245–256. [Google Scholar] [CrossRef] [Green Version]
- Gimbel, H.V. The control of myopia with atropine. Can. J. Ophthalmol. 1973, 8, 527–532. [Google Scholar] [PubMed]
- Sampson, W.G. Role of cycloplegia in the management of functional myopia. Ophthalmology 1979, 86, 695–697. [Google Scholar] [CrossRef]
- Shih, Y.-F.; Chen, C.-H.; Chou, A.-C.; Ho, T.-C.; Lin, L.L.-K.; Hung, P.-T. Comparison of the effect of atropine and cyclopentolate on myopia. Ann. Ophthalmol. 1989, 21, 180–182. [Google Scholar]
- Shih, Y.F.; Chen, C.H.; Chou, A.C.; Ho, T.C.; Lin, L.L.; Hung, P.T. Effects of different concentrations of atropine on controlling myopia in myopic children. J. Ocul. Pharmacol. Ther. 1999, 15, 85–90. [Google Scholar] [CrossRef]
- Pineles, S.L.; Kraker, R.T.; VanderVeen, D.K.; Hutchinson, A.K.; Galvin, J.A.; Wilson, L.B.; Lambert, S.R. Atropine for the prevention of myopia progression in children: A report by the American Academy of Ophthalmology. Ophthalmology 2017, 124, 1857–1866. [Google Scholar] [CrossRef] [PubMed]
- Walline, J.J.; Lindsley, K.B.; Vedula, S.S.; Cotter, S.A.; Mutti, D.O.; Ng, S.M.; Twelker, J.D.; Walline, J.J.; Lindsley, K.B.; Vedula, S.S.; et al. Interventions to slow progression of myopia in children. Cochrane Database Syst. Rev. 2020, 1, CD004916. [Google Scholar]
- Chua, W.H.; Balakrishnan, V.; Chan, Y.H. Atropine for the treatment of childhood myopia. Ophthalmology 2006, 113, 2285–2291. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.; Chua, W.-H.; Cheung, Y.-B.; Wong, W.-L.; Lingham, A.; Fong, A.; Tan, D. Atropine for the treatment of childhood myopia: Safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012, 119, 347–354. [Google Scholar] [CrossRef]
- Luu, C.; Lau, A.M.I.; Koh, A.H.C.; Tan, D. Multifocal electroretinogram in children on atropine treatment for myopia. Br. J. Ophthalmol. 2005, 89, 151–153. [Google Scholar] [CrossRef]
- Chia, A.; Li, W.; Tan, D.; Luu, C.D. Full-field electroretinogram findings in children in the atropine treatment for myopia (ATOM2) study. Doc. Ophthalmol. 2013, 126, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, H.; Fricke, A.; Mauritz, Y.; Löwinger, A.; Klabe, K.; Breyer, D.; Lagenbucher, A.; Seitz, B.; Schaeffel, F. Short-term effects of low-concentration atropine eye drops on pupil size and accommodation in young adult subjects. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 2211–2217. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.-Y.; Wang, H.; Wang, B.-S.; Qi, H.; Rong, Z.-X.; Chen, H.-Z. Atropine in ameliorating the progression of myopia in children with mild to moderate myopia: A meta-analysis of controlled clinical trials. J. Ocul. Pharmacol. Ther. 2011, 27, 361–368. [Google Scholar] [CrossRef]
- Chiang, M.F.; Kouzis, A.; Pointer, R.W.; Repka, M.X. Treatment of childhood myopia with atropine eyedrops and bifocal spectacles. Binocul. Vis. Strabismus Q. 2001, 16, 209–215. [Google Scholar]
- Wang, Y.; Zhao, K.; Jin, Y.; Niu, Y.; Zuo, T. Changes of higher order aberration with various pupil sizes in the myopic eye. J. Refract. Surg. 2003, 19, 270–274. [Google Scholar] [CrossRef]
- Hiraoka, T.; Miyata, K.; Nakamura, Y.; Miyai, T.; Ogata, M.; Okamoto, F.; Oshika, T. Influences of cycloplegia with topical atropine on ocular higher-order aberrations. Ophthalmology 2013, 120, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Joachimsen, L.; Farassat, N.; Bleul, T.; Böhringer, D.; Lagrèze, W.A.; Reich, M. Side effects of topical atropine 0.05% compared to 0.01% for myopia control in German school children: A pilot study. Int. Ophthalmol. 2021, 41, 2001–2008. [Google Scholar] [CrossRef]
- Cooper, J.; Eisenberg, N.; Schulman, E.; Wang, F.M. Maximum atropine dose without clinical signs or symptoms. Optom. Vis. Sci. 2013, 90, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Syniuta, L.A.; Isenberg, S.J. Atropine and bifocals can slow the progression of myopia in children. Binocul. Vis. Strabismus Q. 2001, 16, 203–208. [Google Scholar] [PubMed]
- Brodstein, R.S.; Brodstein, D.E.; Olson, R.J.; Hunt, S.C.; Williams, R.R. The treatment of myopia with atropine and bifocals: A long-term prospective study. Ophthalmology 1984, 91, 1373–1378. [Google Scholar] [CrossRef]
- Tan, Q.; Ng, A.L.; Cheng, G.P.; Woo, V.C.; Cho, P. Combined atropine with orthokeratology for myopia control: Study design and preliminary results. Curr. Eye Res. 2019, 44, 671–678. [Google Scholar] [CrossRef]
- Huang, J.; Mutti, D.O.; Jones-Jordan, L.A.; Walline, J.J. Bifocal & Atropine in Myopia (B.A.M.) Study: Baseline Data and Methods. Optom. Vis. Sci. 2019, 96, 335. [Google Scholar]
- Yam, J.C.; Li, F.F.; Zhang, X.; Tang, S.M.; Yip, B.H.K.; Kam, K.W.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Two-year clinical trial of the low-concentration atropine for myopia progression (LAMP) study: Phase 2 report. Ophthalmology 2020, 127, 910–919. [Google Scholar] [CrossRef]
- Arnold, R.W.; Gionet, E.; Hickel, J.; Owen, M.; Armitage, M.D. Duration and effect of single-dose atropine: Paralysis of accommodation in penalization treatment of functional amblyopia. Binocul. Vis. Strabismus Q. 2004, 19, 81–86. [Google Scholar]
- Lee, C.E.; Lee, Y.C.; Lee, S.Y. Factors influencing the prevalence of amblyopia in children with anisometropia. Korean J. Ophthalmol. 2010, 24, 225. [Google Scholar] [CrossRef] [Green Version]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-concentration atropine for myopia progression (LAMP) study: A randomized, double-blinded, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops in myopia control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control Group | Atropine Group | p-Value | ||
|---|---|---|---|---|
| Number | 113 | 99 | ||
| Age (yr) | 10.19 ± 1.21 | 10.38 ± 1.16 | 0.246 | |
| Hight (cm) | 139.77 ± 9.25 | 139.26 ± 9.48 | 0.699 | |
| IOP (mmHg) | OD | 15.84 ± 3.61 | 15.99 ± 3.47 | 0.765 |
| OS | 15.63 ± 3.21 | 15.87 ± 3.06 | 0.598 | |
| Spherical equivalent (D) | OD | −0.59 ± 1.41 | −1.96 ± 1.46 | <0.001 ** |
| OS | −0.52 ± 1.36 | −2.04 ± 1.51 | 0.001 ** | |
| Pupil size (mm) | OD | 5.40 ± 0.90 | 6.60 ± 1.01 | <0.001 ** |
| OS | 5.42 ± 0.87 | 6.64 ± 1.00 | <0.001 ** | |
| Light entrance area (mm2) | OD | 20.63 ± 7.74 | 28.95 ± 11.11 | <0.001 ** |
| OS | 20.67 ± 7.41 | 29.20 ± 10.92 | <0.001 ** | |
| Distance visual acuity (logMAR) | OD | 0.12 ± 0.28 | 0.45 ± 0.35 | <0.01 * |
| OS | 0.11 ± 0.28 | 0.50 ± 0.34 | <0.01 * | |
| OU | 0.05 ± 0.25 | 0.36 ± 0.32 | <0.01 * | |
| Near visualacuity (logMAR) | OD | 0.06 ± 0.08 | 0.19 ± 0.19 | <0.001 ** |
| OS | 0.06 ± 0.08 | 0.167 ± 0.17 | <0.001 ** | |
| OU | 0.04 ± 0.07 | 0.12 ± 0.16 | <0.001 ** | |
| Control Group | Atropine Group | p-Value | |
|---|---|---|---|
| AA_OD (D) | 15.27 ± 5.24 | 7.41 ± 4.01 | <0.001 ** |
| AA_OS (D) | 15.82 ± 5.70 | 7.24 ± 3.83 | <0.001 ** |
| NPC_break point (cm) | 4.23 ± 3.63 | 12.82 ± 8.19 | <0.001 ** |
| NPC_recovery point (cm) | 6.37 ± 4.29 | 15.27 ± 8.60 | <0.001 ** |
| MEM_OD (D) | 0.86 ± 0.52 | 1.89 ± 0.73 | <0.001 ** |
| MEM_OS (D) | 0.95 ± 0.48 | 1.94 ± 0.71 | <0.001 ** |
| Control Group | Atropine Group | |||
|---|---|---|---|---|
| n | % | n | % | |
| 92 | 85 | |||
| Good (≤40) | 55 | 59.8 | 30 | 35.3 |
| Average (41–63) | 14 | 16.2 | 23 | 27.1 |
| Poor (64–100) | 15 | 16.3 | 20 | 21.5 |
| Very poor (>100) | 8 | 8.7 | 12 | 14.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, H.-Y.; Ke, C.-H.; Chen, S.-T.; Sun, H.-Y. The Impact of Clinical Atropine Use in Taiwanese Schoolchildren: Changes in Physiological Characteristics and Visual Functions. Children 2021, 8, 1054. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111054
Kuo H-Y, Ke C-H, Chen S-T, Sun H-Y. The Impact of Clinical Atropine Use in Taiwanese Schoolchildren: Changes in Physiological Characteristics and Visual Functions. Children. 2021; 8(11):1054. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111054
Chicago/Turabian StyleKuo, Hui-Ying, Ching-Hsiu Ke, Shyan-Tarng Chen, and Han-Yin Sun. 2021. "The Impact of Clinical Atropine Use in Taiwanese Schoolchildren: Changes in Physiological Characteristics and Visual Functions" Children 8, no. 11: 1054. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111054