
Botulinum Toxin a Injection Combined with Radial Extracorporeal Shock Wave Therapy in Children with Spastic Cerebral Palsy: Shear Wave Sonoelastographic Findings in the Medial Gastrocnemius Muscle, Preliminary Study


Abstract
:1. Introduction
2. Materials and Methods
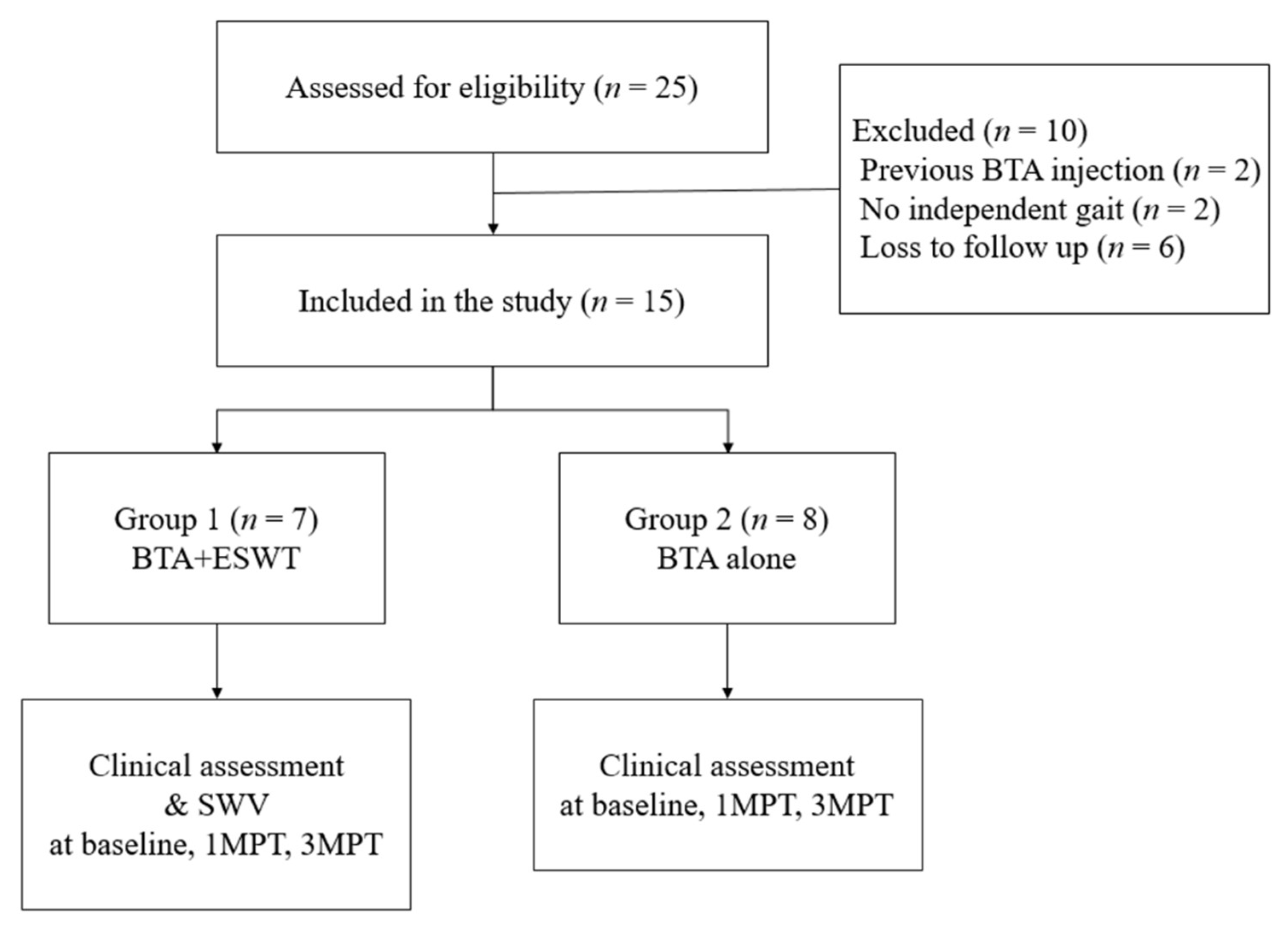
2.1. Participants
2.2. Intervention
2.3. Clinical Assessment
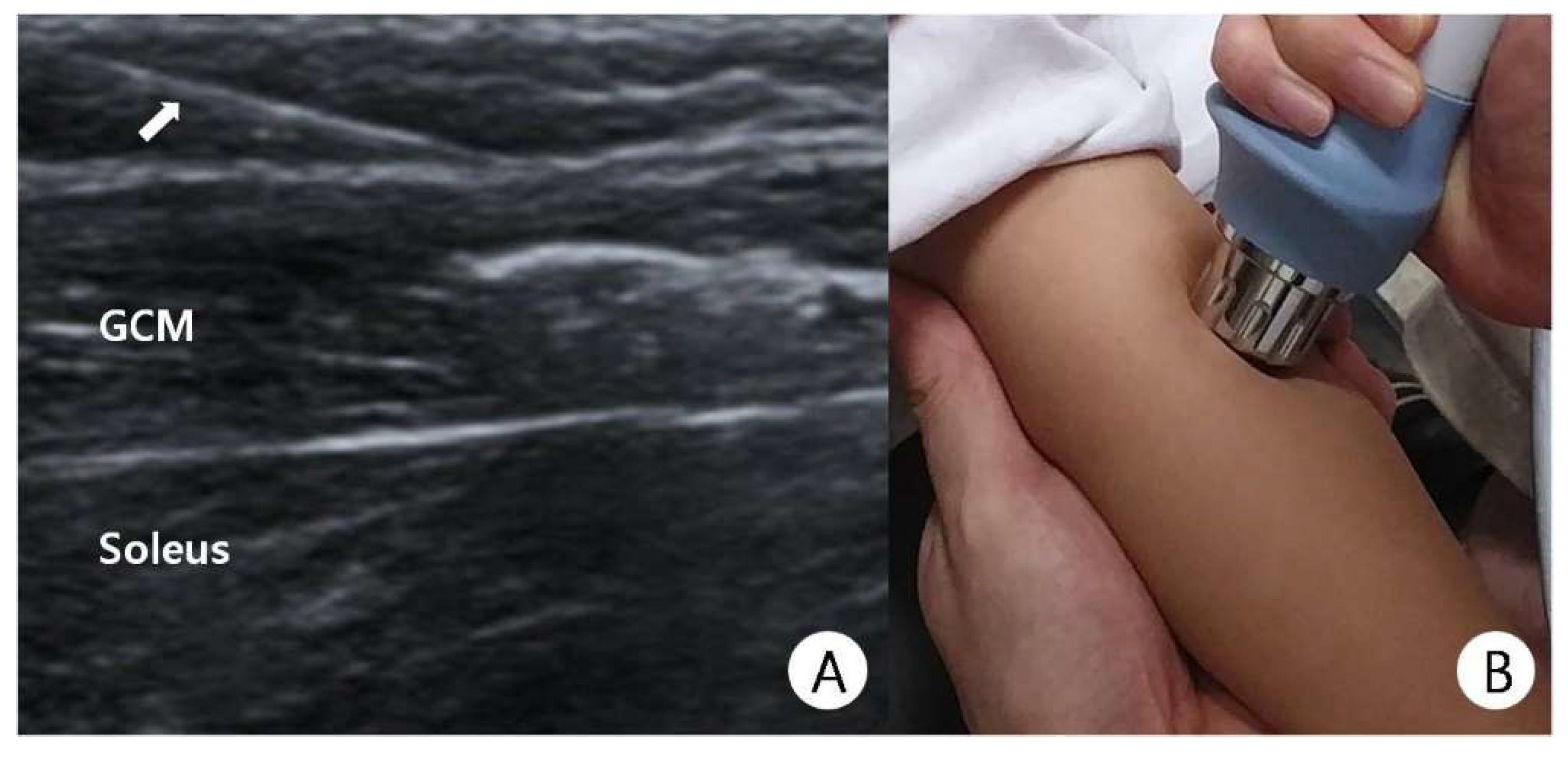
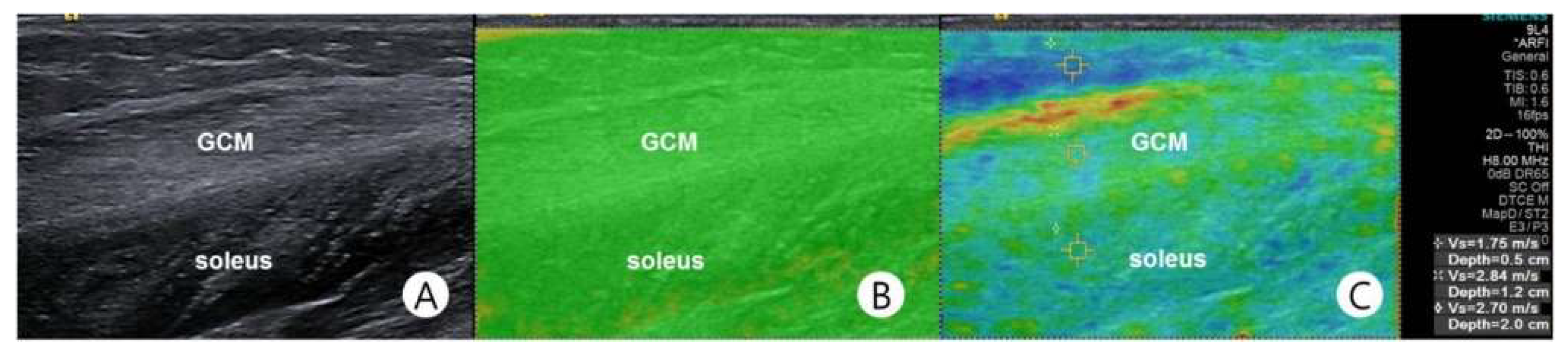
2.4. Shear-Wave Sonoelastography
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borodic, G.E.; Ferrante, R.; Pearce, L.B.; Smith, K. Histologic assessment of dose-related diffusion and muscle fiber response after therapeutic botulinum a toxin injections. Mov. Disord. 1994, 9, 31–39. [Google Scholar] [CrossRef]
- Delgado, M.R.; Hirtz, D.G.; Aisen, M.L.; Ashwal, S.; Fehlings, D.L.; McLaughlin, J.F.; Morrison, L.; Shrader, M.W.; Tilton, A.; Vargusadams, J. Practice Parameter: Pharmacologic treatment of spasticity in children and adolescents with cerebral palsy (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2010, 74, 336–343. [Google Scholar] [CrossRef] [Green Version]
- Kwon, D.R.; Park, G.Y.; Kwon, J.G. The Change of Intrinsic Stiffness in Gastrocnemius after Intensive Rehabilitation with Botulinum Toxin a Injection in Spastic Diplegic Cerebral Palsy. Ann. Rehabil. Med. 2012, 36, 400–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, G.-Y.; Kwon, D.R. Sonoelastographic Evaluation of Medial Gastrocnemius Muscles Intrinsic Stiffness After Rehabilitation Therapy with Botulinum Toxin A Injection in Spastic Cerebral Palsy. Arch. Phys. Med. Rehabil. 2012, 93, 2085–2089. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-Y.; Park, G.-Y.; Kwon, D.R. Comparison of Treatment Effects Between Children with Spastic Cerebral Palsy Under and Over Five Years After Botulinum Toxin Type A Injection. Ann. Rehabil. Med. 2014, 38, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, A.P.; Corry, I.S.; Graham, H.K. Botulinum toxin in the management of the lower LIMB in cerebral palsy. Dev. Med. Child. Neurol. 1994, 36, 386–396. [Google Scholar] [CrossRef]
- Cosgrove, A.P.; Graham, H.K. Botunum toxin a prevents the development of contractures in the hereditary spastc mouse. Dev. Med. Child. Neurol. 2008, 36, 379–385. [Google Scholar] [CrossRef]
- Kim, K.; Shin, H.-I.; Kwon, B.S.; Kim, S.J.; Jung, I.-Y.; Bang, M.S. Neuronox versus BOTOX for spastic equinus gait in children with cerebral palsy: A randomized, double-blinded, controlled multicentre clinical trial. Dev. Med. Child. Neurol. 2010, 53, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Amelio, E.; Manganotti, P. Effect of shock wave stimulation on hypertonic plantar flexor muscles in patients with cerebral palsy: A placebo-controlled study. J. Rehabil. Med. 2010, 42, 339–343. [Google Scholar] [CrossRef] [Green Version]
- Vidal, X.; Morral, A.; Costa, L.; Tur, M. Radial extracorporeal shock wave therapy (rESWT) in the treatment of spasticity in cerebral palsy: A randomized, placebo-controlled clinical trial. NeuroRehabilitation 2011, 29, 413–419. [Google Scholar] [CrossRef]
- Park, D.-S.; Kwon, D.R.; Park, G.-Y.; Lee, M.Y. Therapeutic Effect of Extracorporeal Shock Wave Therapy According to Treatment Session on Gastrocnemius Muscle Spasticity in Children with Spastic Cerebral Palsy: A Pilot Study. Ann. Rehabil. Med. 2015, 39, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Park, J.-W.; Nam, K. Effect of extracorporeal shockwave therapy on muscle spasticity in patients with cerebral palsy: Meta-analysis and systematic review. Eur. J. Phys. Rehabil. Med. 2020, 55, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Kudva, A.; Abraham, M.E.; Gold, J.; Patel, N.A.; Gendreau, J.L.; Herschman, Y.; Mammis, A. Intrathecal baclofen, selective dorsal rhizotomy, and extracorporeal shockwave therapy for the treatment of spasticity in cerebral palsy: A systematic review. Neurosurg. Rev. 2021, 44, 3209–3228. [Google Scholar] [CrossRef] [PubMed]
- Dymarek, R.; Ptaszkowski, K.; Ptaszkowska, L.; Kowal, M.; Sopel, M.; Taradaj, J.; Rosińczuk, J. Shock Waves as a Treatment Modality for Spasticity Reduction and Recovery Improvement in Post-Stroke Adults—Current Evidence and Qualitative Systematic Review. Clin. Interv. Aging 2020, 15, 9–28. [Google Scholar] [CrossRef] [Green Version]
- Guo, P.; Gao, F.; Zhao, T.; Sun, W.; Wang, B.; Li, Z. Positive Effects of Extracorporeal Shock Wave Therapy on Spasticity in Poststroke Patients: A Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 2470–2476. [Google Scholar] [CrossRef]
- Manganotti, P.; Amelio, E. Long-Term Effect of Shock Wave Therapy on Upper Limb Hypertonia in Patients Affected by Stroke. Stroke 2005, 36, 1967–1971. [Google Scholar] [CrossRef] [Green Version]
- Kisch, T.; Wuerfel, W.; Forstmeier, V.; Liodaki, E.; Stang, F.H.; Knobloch, K.; Mailaender, P.; Kraemer, R. Repetitive shock wave therapy improves muscular microcirculation. J. Surg. Res. 2016, 201, 440–445. [Google Scholar] [CrossRef]
- López-Marín, L.M.; Rivera, A.L.; Fernández, F.; Loske, A.M. Shock wave-induced permeabilization of mammalian cells. Phys. Life Rev. 2018, 26, 1–38. [Google Scholar] [CrossRef]
- Luh, J.-J.; Huang, W.-T.; Lin, K.-H.; Huang, Y.-Y.; Kuo, P.-L.; Chen, W.-S. Effects of Extracorporeal Shock Wave-Mediated Transdermal Local Anesthetic Drug Delivery on Rat Caudal Nerves. Ultrasound Med. Biol. 2018, 44, 214–222. [Google Scholar] [CrossRef]
- Picelli, A.; La Marchina, E.; Gajofatto, F.; Pontillo, A.; Vangelista, A.; Filippini, R.; Baricich, A.; Cisari, C.; Smania, N. Sonographic and clinical effects of botulinum toxin Type A combined with extracorporeal shock wave therapy on spastic muscles of children with cerebral palsy. Dev. Neurorehabilit. 2016, 20, 160–164. [Google Scholar] [CrossRef]
- Park, G.Y.; Kwon, D.R.; Gil Kwon, D. Shear wave sonoelastography in infants with congenital muscular torticollis. Medicine 2018, 97, e9818. [Google Scholar] [CrossRef]
- Brandenburg, J.E.; Eby, S.; Song, P.; Bamlet, W.R.; Sieck, G.C.; An, K.-N. Quantifying Effect of Onabotulinum Toxin A on Passive Muscle Stiffness in Children with Cerebral Palsy Using Ultrasound Shear Wave Elastography. Am. J. Phys. Med. Rehabil. 2018, 97, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Vola, E.A.; Albano, M.; Di Luise, C.; Servodidio, V.; Sansone, M.; Russo, S.; Corrado, B.; Iammarrone, C.S.; Caprio, M.G.; Vallone, G. Use of ultrasound shear wave to measure muscle stiffness in children with cerebral palsy. J. Ultrasound 2018, 21, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Mathevon, L.; Michel, F.; Aubry, S.; Testa, R.; Lapole, T.; Arnaudeau, L.F.; Fernandez, B.; Parratte, B.; Calmels, P. Two-dimensional and shear wave elastography ultrasound: A reliable method to analyse spastic muscles? Muscle Nerve 2018, 57, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Brandenburg, J.E.; Eby, S.; Song, P.; Kingsley-Berg, S.; Bamlet, W.; Sieck, G.; An, K.-N. Quantifying passive muscle stiffness in children with and without cerebral palsy using ultrasound shear wave elastography. Dev. Med. Child. Neurol. 2016, 58, 1288–1294. [Google Scholar] [CrossRef] [Green Version]
- Lehoux, M.-C.; Sobczak, S.; Cloutier, F.; Charest, S.; Bertrand-Grenier, A. Shear wave elastography potential to characterize spastic muscles in stroke survivors: Literature review. Clin. Biomech. 2020, 72, 84–93. [Google Scholar] [CrossRef]
- Banky, M.; Ryan, H.K.; Clark, R.; Olver, J.; Williams, G. Do clinical tests of spasticity accurately reflect muscle function during walking: A systematic review. Brain Inj. 2017, 31, 440–455. [Google Scholar] [CrossRef]
- Ansari, N.N.; Naghdi, S.; Moammeri, H.; Jalaie, S. Ashworth Scales are unreliable for the assessment of muscle spasticity. Physiother. Theory Pr. 2006, 22, 119–125. [Google Scholar] [CrossRef]
- Barr, R.G.; Zhang, Z. Shear-Wave Elastography of the Breast: Value of a Quality Measure and Comparison with Strain Elastography. Radiology 2015, 275, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.L.; Chen, C.Y.; Chen, H.C.; Wu, C.Y.; Lin, K.C.; Hsieh, Y.W.; Shen, I.H. Responsiveness and minimal clinically important difference of Modified Ashworth Scale in patients with stroke. Eur. J. Phys. Rehabil. Med. 2019, 55, 754–760. [Google Scholar] [CrossRef]
- Booth, C.M.; Cortina-Borja, M.J.F.; Theologis, T. Collagen accumulation in muscles of children with cerebral palsy and correlation with severity of spasticity. Dev. Med. Child. Neurol. 2001, 43, 314–320. [Google Scholar] [CrossRef]
- Mariotto, S.; Cavalieri, E.; Amelio, E.; Ciampa, A.R.; de Prati, A.C.; Marlinghaus, E.; Russo, S.; Suzuki, H. Extracorporeal shock waves: From lithotripsy to anti-inflammatory action by NO production. Nitric Oxide 2005, 12, 89–96. [Google Scholar] [CrossRef]
- Trompetto, C.; Avanzino, L.; Bove, M.; Marinelli, L.; Molfetta, L.; Trentini, R.; Abbruzzese, G. External shock waves therapy in dystonia: Preliminary results. Eur. J. Neurol. 2009, 16, 517–521. [Google Scholar] [CrossRef]
- Picelli, A.; Bonetti, P.; Fontana, C.; Barausse, M.; Dambruoso, F.; Gajofatto, F.; Girardi, P.; Manca, M.; Gimigliano, R.; Smania, N. Is Spastic Muscle Echo Intensity Related to the Response to Botulinum Toxin Type A in Patients with Stroke? A Cohort Study. Arch. Phys. Med. Rehabil. 2012, 93, 1253–1258. [Google Scholar] [CrossRef]
- Picelli, A.; Tamburin, S.; Cavazza, S.; Scampoli, C.; Manca, M.; Cosma, M.; Berto, G.; Vallies, G.; Roncari, L.; Melotti, C.; et al. Relationship Between Ultrasonographic, Electromyographic, and Clinical Parameters in Adult Stroke Patients with Spastic Equinus: An Observational Study. Arch. Phys. Med. Rehabil. 2014, 95, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Pitcher, C.; Elliott, C.; Panizzolo, F.A.; Valentine, J.P.; Stannage, K.; Reid, S. Ultrasound characterization of medial gastrocnemius tissue composition in children with spastic cerebral palsy. Muscle Nerve 2015, 52, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Lohse-Busch, H.; Kraemer, M.; Reime, U. A pilot investigation into the effects of extracorporeal shock waves on muscular dysfunction in children with spastic movement disorders. Schmerz 1997, 11, 108–112. [Google Scholar] [CrossRef]
- Kamelger, F.; Oehlbauer, M.; Piza-Katzer, H.; Meirer, R. Extracorporeal Shock Wave Treatment in Ischemic Tissues: What is the Appropriate Number of Shock Wave Impulses? J. Reconstr. Microsurg. 2010, 26, 117–121. [Google Scholar] [CrossRef]
- Santamato, A.; Notarnicola, A.; Panza, F.; Ranieri, M.; Micello, M.F.; Manganotti, P.; Moretti, B.; Fortunato, F.; Filoni, S.; Fiore, P. SBOTE Study: Extracorporeal Shock Wave Therapy Versus Electrical Stimulation After Botulinum Toxin Type A Injection for Post-Stroke Spasticity—A Prospective Randomized Trial. Ultrasound Med. Biol. 2013, 39, 283–291. [Google Scholar] [CrossRef]
- Patrick, E.; Ada, L. The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it. Clin. Rehabil. 2006, 20, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Benini, R.; Shevell, M.I. Updates in the Treatment of Spasticity Associated with Cerebral Palsy. Curr. Treat. Opt. Neurol. 2012, 14, 650–659. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PROM | MAS | |||
|---|---|---|---|---|
| Group 1 | Group 2 | Group 1 | Group 2 | |
| Baseline | −14.1 ± 20.4 | 5.7 ± 1.5 | 3.2 ± 0.4 | 3.2 ± 0.8 |
| 1MPT | 6.2 ± 7.2 (a) | 15.3 ± 4.4 (a) | 1.4 ± 0.6 (c) | 2.0 ± 0.7 (c) |
| ∆ | 20.2 ± 17.0 (b) | 9.6 ± 4.6 (b) | −1.8 ± 0.3 | −1.2 ± 0.6 |
| 3MPT | 0.2 ± 10.5 (a) | 12.0 ± 4.1 (a) | 1.8 ± 0.5 (c) | 2.5 ± 0.6 (c) |
| ∆ | 14.1 ± 20.4 (b) | 6.2 ± 3.6 (b) | −1.4 ± 0.7 | −0.8 ± 0.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, D.R.; Kwon, D.G. Botulinum Toxin a Injection Combined with Radial Extracorporeal Shock Wave Therapy in Children with Spastic Cerebral Palsy: Shear Wave Sonoelastographic Findings in the Medial Gastrocnemius Muscle, Preliminary Study. Children 2021, 8, 1059. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111059
Kwon DR, Kwon DG. Botulinum Toxin a Injection Combined with Radial Extracorporeal Shock Wave Therapy in Children with Spastic Cerebral Palsy: Shear Wave Sonoelastographic Findings in the Medial Gastrocnemius Muscle, Preliminary Study. Children. 2021; 8(11):1059. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111059
Chicago/Turabian StyleKwon, Dong Rak, and Dae Gil Kwon. 2021. "Botulinum Toxin a Injection Combined with Radial Extracorporeal Shock Wave Therapy in Children with Spastic Cerebral Palsy: Shear Wave Sonoelastographic Findings in the Medial Gastrocnemius Muscle, Preliminary Study" Children 8, no. 11: 1059. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111059