
Effects of Live Music Therapy on Autonomic Stability in Preterm Infants: A Cluster-Randomized Controlled Trial

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting and Procedures
2.3. Participants
2.4. Clusters Randomization and Recruitment
2.5. Interventions
2.6. Outcomes
2.7. Power Calculation
2.8. Data Analysis
3. Results
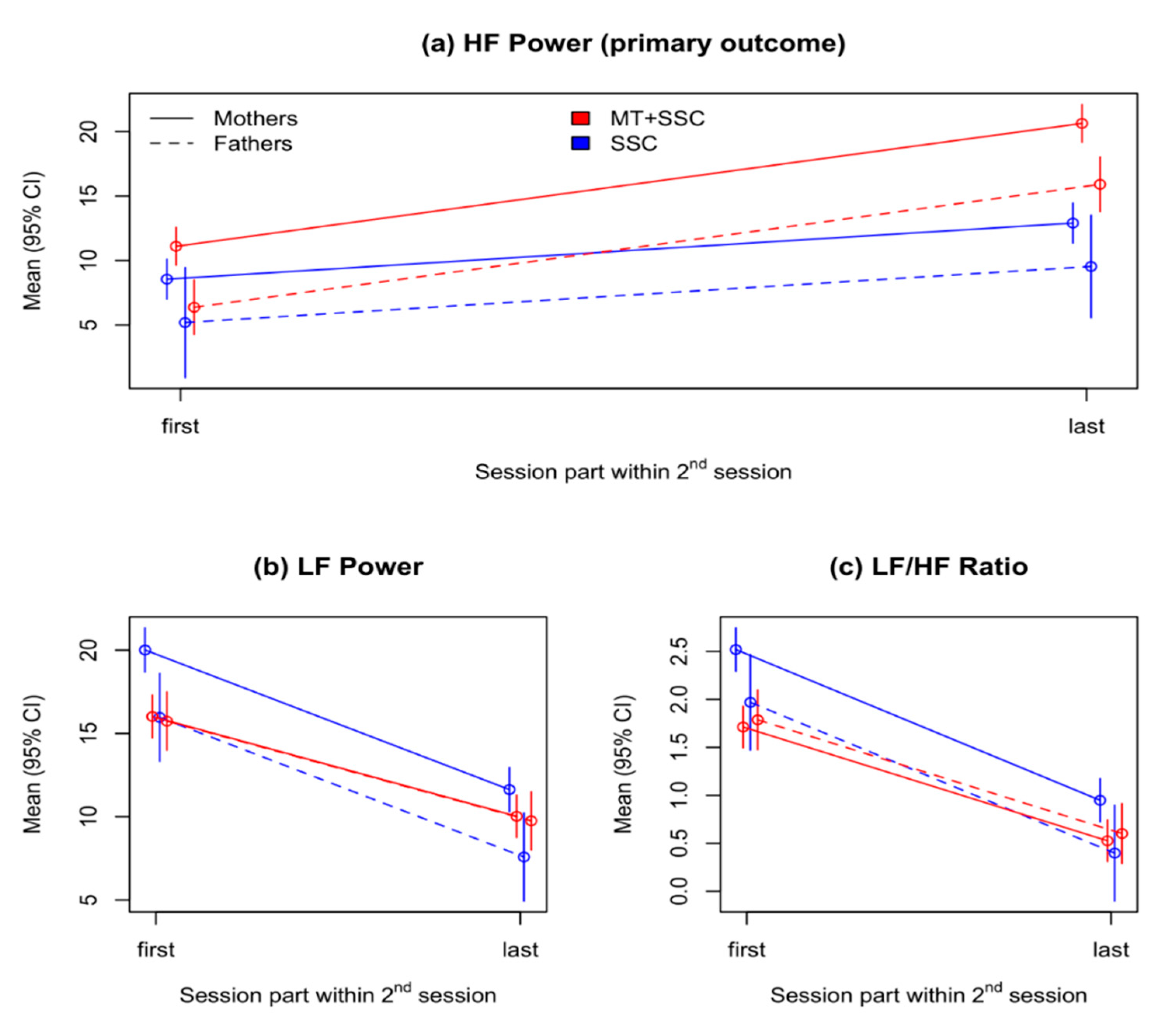
3.1. Primary Outcome: Change in Infants’ HF Power during the Second Session
3.2. Secondary Outcomes
3.2.1. LF Power and LF/HF Ratio in the Second Session
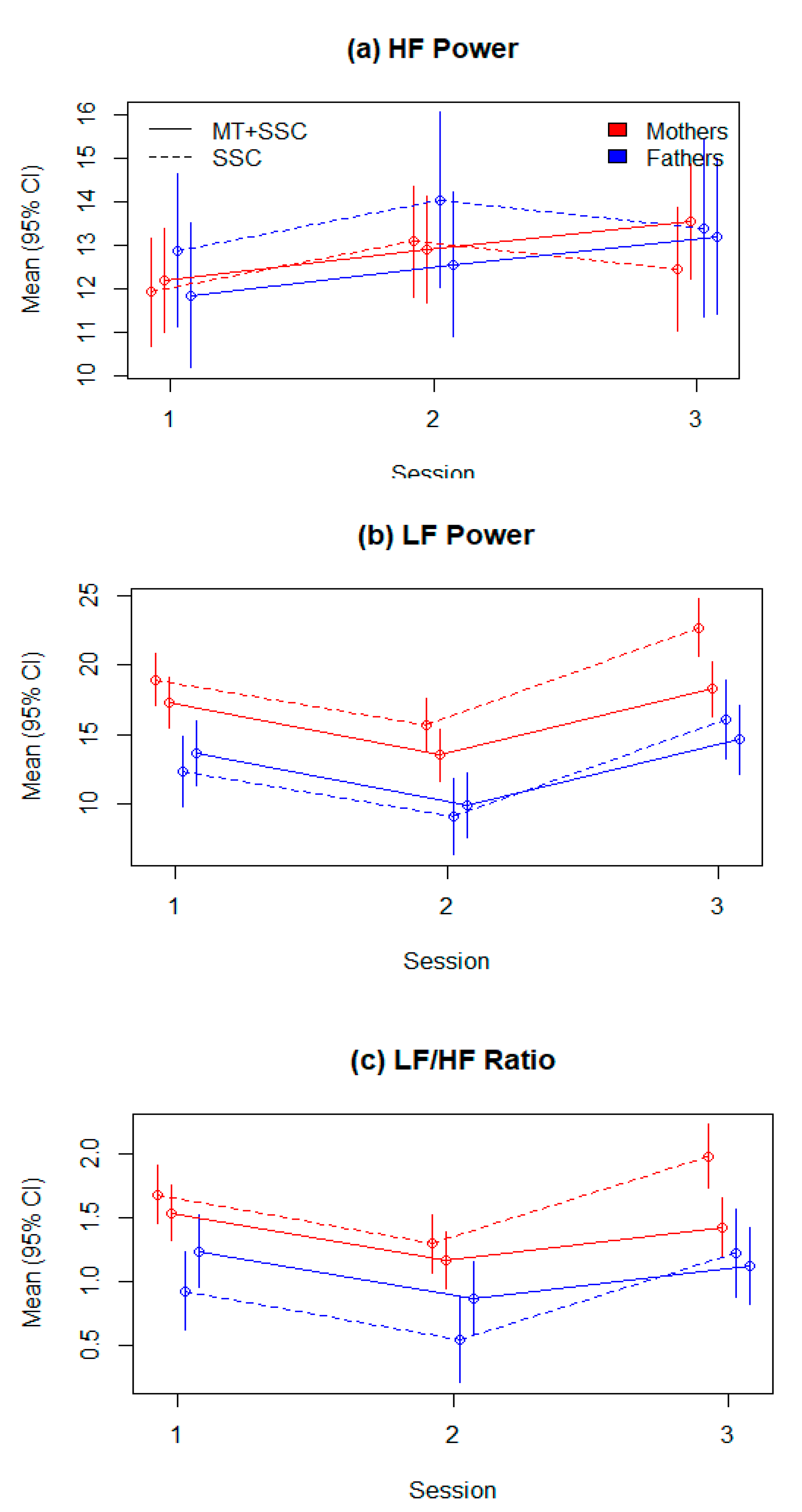
3.2.2. HRV Parameters across All Three Sessions
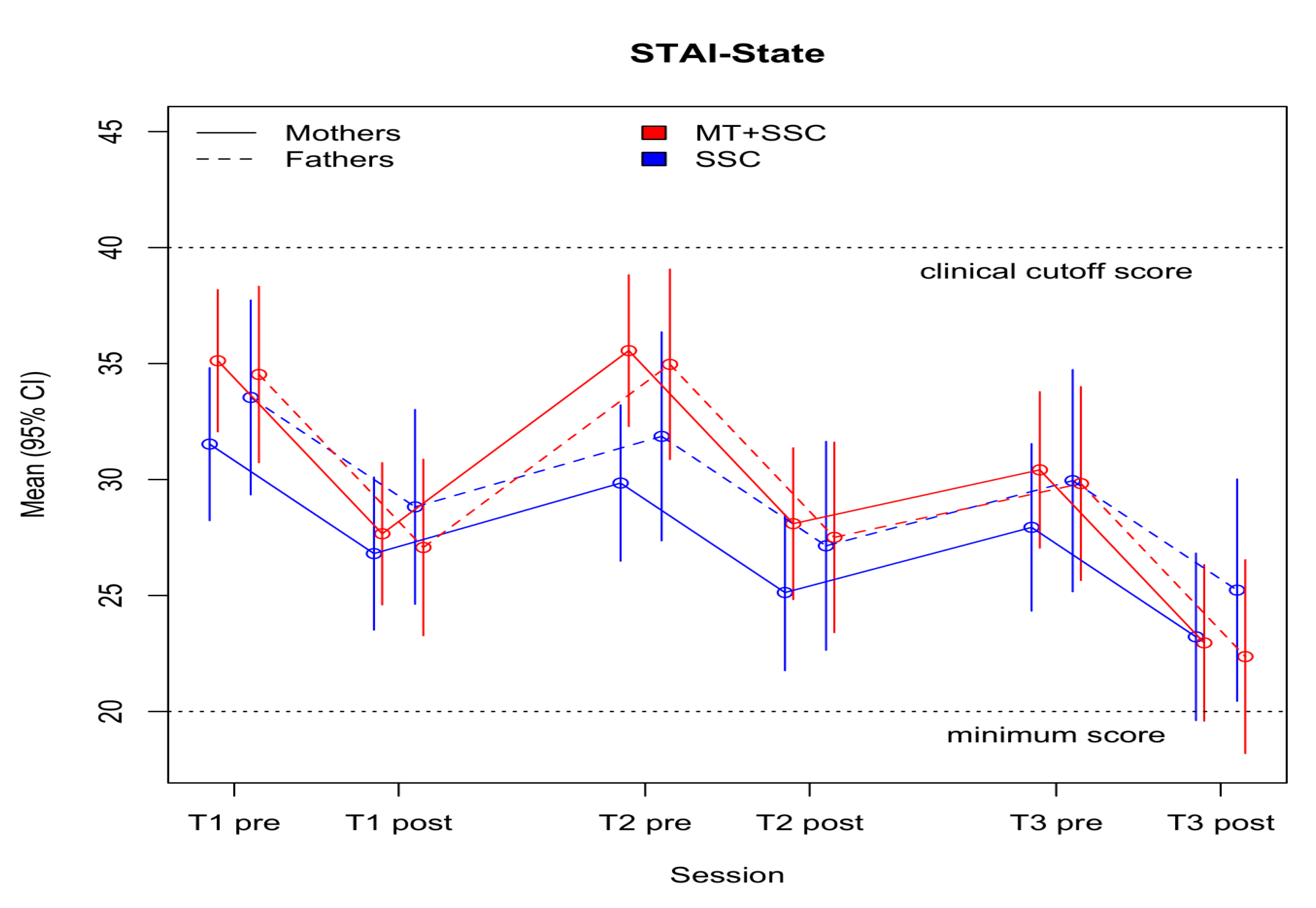
3.3. Parental Outcomes
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Browne, J.V. Infant mental health in intensive care: Laying a foundation for social, emotional and mental health outcomes through regulation, relationships and reflection. J. Neonatal. Nurs. 2021, 27, 33–39. [Google Scholar] [CrossRef]
- Als, H.; Duffy, F.H.; McAnulty, G.B.; Rivkin, M.J.; Vajapeyam, S.; Mulkern, R.V.; Warfield, S.K.; Huppi, P.S.; Butler, S.C.; Conneman, N.; et al. Early experience alters brain function and structure. Pediatrics 2004, 113, 846–857. [Google Scholar] [CrossRef] [Green Version]
- Gui, L.; Loukas, S.; Lazeyras, F.; Hüppi, P.S.; Meskaldji, D.E.; Borradori Tolsa, C. Longitudinal study of neonatal brain tissue volumes in preterm infants and their ability to predict neurodevelopmental outcome. Neuroimage 2019, 185, 728–741. [Google Scholar] [CrossRef] [PubMed]
- Moore, T.A.; Berger, A.M.; Wilson, M.E. A New Way of Thinking About Complications of Prematurity. Biol. Res. Nurs. 2014, 16, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Nist, M.D.; Harrison, T.M.; Steward, D.K. The biological embedding of neonatal stress exposure: A conceptual model describing the mechanisms of stress-induced neurodevelopmental impairment in preterm infants. Res. Nurs. Health 2019, 42, 61–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graven, S.N.; Browne, J.V. Sensory Development in the Fetus, Neonate, and Infant: Introduction and Overview. Newborn Infant Nurs. Rev. 2008, 8, 169–172. [Google Scholar] [CrossRef] [Green Version]
- Barthel, D.; Göbel, A.; Barkmann, C.; Helle, N.; Bindt, C. Does Birth-Related Trauma Last? Prevalence and Risk Factors for Posttraumatic Stress in Mothers and Fathers of VLBW Preterm and Term Born Children 5 Years After Birth. Front. Psychiatry 2020, 11, 1466. [Google Scholar] [CrossRef]
- Feldman, R.; Eidelman, A.I. Skin-to-skin contact (Kangaroo Care) accelerates autonomic and neurobehavioural maturation in preterm infants. Dev. Med. Child Neurol. 2003, 45, 274–281. [Google Scholar] [CrossRef]
- Bieleninik, Ł.; Ghetti, C.; Gold, C. Music therapy for preterm infants and their parents: A meta-analysis. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [Green Version]
- Bergman, N.; Carney, G.; Ludington-Hoe, S.M. Kangaroo Care for the Preterm Infant. ICAN Infant Child Adolesc. Nutr. 2010, 2, 165–169. [Google Scholar] [CrossRef]
- Haslbeck, F.; Hugoson, P. Sounding Together: Family-Centered Music Therapy as Facilitator for Parental Singing During Skin-to-Skin Contact. In Early Vocal Contact and Preterm Infant Brain Development: Bridging the Gaps Between Research and Practice; Springer: Cham, Switzerland; Zurich, Switzerland, 2017; pp. 217–238. ISBN 978-3-319-65075-3. [Google Scholar]
- Pineda, R.; Guth, R.; Herring, A.; Reynolds, L.; Oberle, S.; Smith, J. Enhancing sensory experiences for very preterm infants in the NICU: An integrative review. J. Perinatol. 2017, 37, 323–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettenberger, M.; Rojas Cárdenas, C.; Parker, M.; Odell-Miller, H. Family-centred music therapy with preterm infants and their parents in the Neonatal Intensive Care Unit (NICU) in Colombia–A mixed-methods study. Nord. J. Music Ther. 2017, 26, 207–234. [Google Scholar] [CrossRef] [Green Version]
- Teckenberg-Jansson, P.; Huotilainen, M.; Pölkki, T.; Lipsanend, J.; Järvenpääe, A.L. Rapid effects of neonatal music therapy combined with kangaroo care on prematurely-born infants. Nord. J. Music Ther. 2011, 20, 22–42. [Google Scholar] [CrossRef]
- Epstein, S.; Bauer, S.; Levkovitz Stern, O.; Litmanovitz, I.; Elefant, C.; Yakobson, D.; Arnon, S. Preterm infants with severe brain injury demonstrate unstable physiological responses during maternal singing with music therapy: A randomized controlled study. Eur. J. Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kostilainen, K.; Mikkola, K.; Erkkilä, J.; Huotilainen, M. Effects of maternal singing during kangaroo care on maternal anxiety, wellbeing, and mother-infant relationship after preterm birth: A mixed methods study. Nord. J. Music Ther. 2020, 1–20. [Google Scholar] [CrossRef]
- Arnon, S.; Diamant, C.; Bauer, S.; Regev, R.; Sirota, G.; Litmanovitz, I. Maternal singing during kangaroo care led to autonomic stability in preterm infants and reduced maternal anxiety. Acta Paediatr. Int. J. Paediatr. 2014, 103, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Flacking, R.; Thomson, G.; Axelin, A. Pathways to emotional closeness in neonatal units-a cross-national qualitative study. BMC Pregnancy Childbirth 2016, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flacking, R.; Lehtonen, L.; Thomson, G.; Axelin, A.; Ahlqvist, S.; Moran, V.H.; Ewald, U.; Dykes, F. Closeness and separation in neonatal intensive care. Acta Paediatr. 2012, 101, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Loewy, J.; Jaschke, A.C. Mechanisms of Timing, Timbre, Repertoire, and Entrainment in Neuroplasticity: Mutual Interplay in Neonatal Development. Front. Integr. Neurosci. 2020, 14, 8. [Google Scholar] [CrossRef]
- Foroushani, S.M.; Herman, C.A.; Wiseman, C.A.; Anthony, C.M.; Drury, S.S.; Howell, M.P. Evaluating physiologic outcomes of music interventions in the neonatal intensive care unit: A systematic review. J. Perinatol. 2020, 40, 1770–1779. [Google Scholar] [CrossRef]
- Longin, E.; Gerstner, T.; Schaible, T.; Lenz, T.; König, S. Maturation of the autonomic nervous system: Differences in heart rate variability in premature vs. term infants. J. Perinat. Med. 2006, 34, 303–308. [Google Scholar] [CrossRef]
- Yue, W.; Han, X.; Luo, J.; Zeng, Z.; Yang, M. Effect of music therapy on preterm infants in neonatal intensive care unit: Systematic review and meta-analysis of randomized controlled trials. J. Adv. Nurs. 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Graven, S.N. Sound and the Developing Infant in the NICU: Conclusions and Recommendations for Care. J. Perinatol. 2000, 20, S88–S93. [Google Scholar] [CrossRef] [PubMed]
- Yakobson, D.; Arnon, S.; Gold, C.; Elefant, C.; Litmanovitz, I.; Beck, B.D. Music Therapy for Preterm Infants and Their Parents: A Cluster-Randomized Controlled Trial Protocol. J. Music Ther. 2020, 57, 219–242. [Google Scholar] [CrossRef] [PubMed]
- Korner, A.F.; Stevenson, D.K.; Forrest, T.; Constantinou, J.C.; Dimiceli, S.; Brown, B.W.M. Preterm medical complications differentially affect neurobehavioral functions: Results from a new neonatal medical index. Infant Behav. Dev. 1994, 17, 37–43. [Google Scholar] [CrossRef]
- Loewy, J.; Stewart, K.; Dassler, A.M.; Telsey, A.; Homel, P. The effects of music therapy on vital signs, feeding, and sleep in premature infants. Pediatrics 2013, 131, 902–918. [Google Scholar] [CrossRef] [Green Version]
- Lullaby Ocean Disc. Available online: https://remo.com/products/product/ocean-disk/ (accessed on 17 June 2021).
- Loewy, J. NICU music therapy: Song of kin as critical lullaby in research and practice. Ann. N. Y. Acad. Sci. 2015, 1337, 178–185. [Google Scholar] [CrossRef]
- Jefferies, A.L.; Canadian Paediatric Society, F. and N.C. and N.C. Kangaroo care for the preterm infant and family. Paediatr. Child Health 2012, 17, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Cowan, M.J. Measurement of Heart Rate Variability. West. J. Nurs. Res. 1995, 17, 32–48. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [CrossRef] [Green Version]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [Green Version]
- Philips Patient Monitoring in Irvine California-USOC Medical. Available online: https://usocmedical.com/product-category/patient-monitoring/philips-patient-monitoring/ (accessed on 17 June 2021).
- Condon, J.T.; Corkindale, C.J. The assessment of parent-to-infant attachment: Development of a self-report questionnaire instrument. J. Reprod. Infant Psychol. 1998, 16, 57–76. [Google Scholar] [CrossRef]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.R.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1–Y2); Consulting Psychologists Press: Santa Clara, CA, USA, 1983; Volume 4. [Google Scholar]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 17 June 2021).
- Butruille, L.; Blouin, A.; De Jonckheere, J.; Mur, S.; Margez, T.; Rakza, T.; Storme, L. Impact of skin-to-skin contact on the autonomic nervous system in the preterm infant and his mother. Infant Behav. Dev. 2017, 49, 83–86. [Google Scholar] [CrossRef]
- McCain, G.C.; Ludington-Hoe, S.M.; Swinth, J.Y.; Hadeed, A.J. Heart rate variability responses of a preterm infant to kangaroo care. J. Obstet. Gynecol. Neonatal. Nurs. JOGNN 2005, 34, 689–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haraldsdottir, K.; Watson, A.M.; Goss, K.N.; Beshish, A.G.; Pegelow, D.F.; Palta, M.; Tetri, L.H.; Barton, G.P.; Brix, M.D.; Centanni, R.M.; et al. Impaired autonomic function in adolescents born preterm. Physiol. Rep. 2018, 6, e13620. [Google Scholar] [CrossRef] [PubMed]
- Patural, H.; Barthelemy, J.C.; Pichot, V.; Mazzocchi, C.; Teyssier, G.; Damon, G.; Roche, F. Birth prematurity determines prolonged autonomic nervous system immaturity. Clin. Auton. Res. 2004, 14, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Porges, S.W.; Furman, S.A. The early development of the autonomic nervous system provides a neural platform for social behaviour: A polyvagal perspective. Infant Child Dev. 2011, 20, 106–118. [Google Scholar] [CrossRef] [Green Version]
- Mulkey, S.B.; du Plessis, A.J. Autonomic nervous system development and its impact on neuropsychiatric outcome. Pediatr. Res. 2019, 85, 120–126. [Google Scholar] [CrossRef]
- Feldman, R.; Rosenthal, Z.; Eidelman, A.I. Maternal-preterm skin-to-skin contact enhances child physiologic organization and cognitive control across the first 10 years of life. Biol. Psychiatry 2014, 75, 56–64. [Google Scholar] [CrossRef]
- Billman, G. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rogalski Landrot, I.; Roche, F.; Pichot, V.; Teyssier, G.; Gaspoz, J.-M.; Barthelemy, J.-C.; Patural, H. Autonomic nervous system activity in premature and full-term infants from theoretical term to 7 years. Auton. Neurosci. 2007, 136, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Julian, L.J. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011, 63, S467–S472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson-Abromeit, D.; Shoemark, H.; Loewy, J. Music therapy with pediatric units: Newborn intensive care unit (NICU). In Medical Music Therapy for Pediatrics in Hospital Settings. Using Music to Support Medical Interventions; Hanson-Abromeit, D., Ed.; American Music Therapy Association: Silver Spring, MD, USA, 2008; pp. 15–69. [Google Scholar]
- Roué, J.-M.; Kuhn, P.; Lopez Maestro, M.; Maastrup, R.A.; Mitanchez, D.; Westrup, B.; Sizun, J. Eight principles for patient-centred and family-centred care for newborns in the neonatal intensive care unit. Arch. Dis. Child. -Fetal Neonatal Ed. 2017, 102, F364–F368. [Google Scholar] [CrossRef] [PubMed]
- Cong, X.; Ludington-Hoe, S.M.; McCain, G.; Fu, P. Kangaroo Care modifies preterm infant heart rate variability in response to heel stick pain: Pilot study. Early Hum. Dev. 2009, 85, 561–567. [Google Scholar] [CrossRef] [Green Version]
- Gardner, F.C.; Adkins, C.S.; Hart, S.E.; Travagli, R.A.; Doheny, K.K. Preterm Stress Behaviors, Autonomic Indices, and Maternal Perceptions of Infant Colic. Adv. Neonatal. Care 2018, 18, 49–57. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. Claude Bernard and the heart–brain connection: Further elaboration of a model of neurovisceral integration. Neurosci. Biobehav. Rev. 2009, 33, 81–88. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | MT + SSC | SSC | p-Value a |
|---|---|---|---|
| Neonatal | N = 37 | N = 31 | |
| Gestational age, wk b | 30.56 ± 2.66 | 31.06 ± 2.92 | 0.47 |
| Birth weight, g b | 1474.86 ± 494.00 | 1492.84 ± 460.10 | 0.88 |
| Age at study entry, d b | 29.08 ± 24.44 | 24.19 ± 16.93 | 0.34 |
| Age at study entry, wk b | 34.74 ± 1.92 | 34.45 ± 1.70 | 0.54 |
| Male sex c | 15 (40%) | 18 (58%) | 0.15 |
| Neonatal medical index grade 1/2/3 c | 11(30%)/20 (54%)/ 4 (12%) | 12 (39%)/13 (42%)/ 6 (19%) | 0.33 |
| AGA/SGA c Ethnic Origin c | 31 (84%)/ 5 (13%) | 24 (77%)/ 7 (23%) | 0.43 |
| Jewish/Arab | 35(95%)/2(5%) | 28(90%)/3(10%) | 0.50 |
| Parental | N = 42 | N = 37 | |
| Female sex c | 30 (71%) | 27 (73%) | |
| Participation of one parent/ Both parents c | 28 (76%)/9 (24%) | 26 (84%)/5 (16%) | 0.40 |
| HF Power Change in Second Session | B (SE) | p-Value |
|---|---|---|
| No. of observations: 124 | ms2/Hz SD | |
| Intercept a | 8.55 (0.69) | <0.001 |
| Session part: last | 4.35 (0.96) | <0.001 |
| Parent: father | −3.36 (1.83) | 0.068 |
| Treatment: MT + SSC | 2.55 (0.94) | 0.027 |
| Session part: last X treatment: MT + SSC | 5.19 (1.27) | <0.001 |
| Parent: father X treatment: MT + SSC | −1.36 (2.06) | 0.510 |
| HRV Variable | MT + SSC | SSC | p-Value a | Effect Size (95% CI) |
|---|---|---|---|---|
| ms2/Hz (SD) | ms2/Hz (SD) | |||
| Mean HF, first part | 9.86 (2.44) | 8.45 (2.02) | 0.020 | 0.623 (0.084, 1.156) |
| Mean HF, last part | 19.66 (6.26) | 12.69 (1.23) | <0.001 | 1.461 (0.866, 2.046) |
| Mean LF, first part | 15.88 (2.52) | 19.88 (2.82) | <0.001 | −1.501 (−2.089, −0.903) |
| Mean LF, last part | 9.97 (2.10) | 11.41 (2.45) | 0.023 | −0.635 (−1.165, −0.100) |
| Mean LF/HF ratio, first part | 1.71 (0.57) | 2.52 (0.66) | <0.001 | −1.320 (−1.893, −0.736) |
| Mean LF/HF ratio, last part | 0.53 (0.29) | 0.90 (0.27) | <0.001 | −1.368 (−1.945, −0.781) |
| LF Change in Second Session | B (SE) | p-Value |
|---|---|---|
| No. of observations: 127 | ||
| Intercept a | 20.01 (0.59) | <0.001 |
| Session part: last | −8.38 (0.70) | <0.001 |
| Parent: father | −4.05 (1.13) | <0.001 |
| Treatment: MT + SSC | −4.00 (0.81) | 0.001 |
| Session part: last X treatment: MT + SSC | 2.40 (0.93) | 0.011 |
| Parent: father X treatment: MT + SSC | 3.78 (1.34) | 0.006 |
| LF/HF Ratio Change in Second Session | ||
| No. of observations: 126 | ||
| Intercept | 2.52 (0.10) | <0.001 |
| Session part: last | −1.57 (0.14) | <0.001 |
| Parent: father | −0.55 (0.22) | 0.015 |
| Treatment: MT + SSC | −0.81 (0.14) | <0.001 |
| Session part: last X treatment: MT + SSC | 0.38 (0.18) | 0.039 |
| Parent: father X treatment: MT + SSC | 0.62 (0.26) | 0.019 |
| HF Power across Sessions | B (SE) | p-Value |
|---|---|---|
| No. of observations: 199 | ||
| Intercept a | 11.93 (0.55) | <0.001 |
| Second session | 1.16 (0.66) | 0.078 |
| Third session | 0.52 (0.71) | 0.462 |
| Parent: fathers | 0.95 (0.76) | 0.212 |
| Treatment: MT + SSC | 0.27 (0.75) | 0.725 |
| Second session X treatment: MT + SSC | −0.45 (0.89) | 0.608 |
| Third session X treatment: MT + SSC | 0.83 (0.95) | 0.385 |
| Parent: fathers X treatment: MT + SSC | −1.30 (0.99) | 0.194 |
| LF Power across Sessions | ||
| No. of observations: 199 | ||
| Intercept | 18.92 (0.82) | <0.001 |
| Second session | −3.24 (0.82) | <0.001 |
| Third session | 3.73 (0.89) | <0.001 |
| Parent: fathers | −6.62 (0.98) | <0.001 |
| Treatment: MT + SSC | −1.68 (1.13) | 0.177 |
| Second session X treatment: MT + SSC | −0.51 (1.11) | 0.646 |
| Third session X treatment: MT + SSC | −2.74 (1.20) | 0.023 |
| Parent: fathers X treatment: MT + SSC | 3.00 (1.27) | 0.020 |
| LF/HF Power across Sessions | ||
| No. of observations: 198 | ||
| Intercept | 1.68 (0.10) | <0.001 |
| Second session | −0.38 (0.10) | <0.001 |
| Third session | 0.30 (0.11) | 0.008 |
| Parent: fathers | −0.76 (0.12) | <0.001 |
| Treatment: MT + SSC | −0.14 (0.14) | 0.325 |
| Second session X treatment: MT + SSC | 0.02 (0.14) | 0.897 |
| Third session X treatment: MT + SSC | −0.42 (0.15) | 0.006 |
| Parent: fathers X treatment: MT + SSC | 0.46 (0.16) | 0.004 |
| Maternal Postnatal Attachment Scale | B (SE) | p-Value |
|---|---|---|
| No. of observations: 166 | ||
| Intercept a | 81.69 (1.31) | <0.001 |
| One month assessment | 0.14 (2.00) | 0.942 |
| Three-month follow-up | −1.88 (1.82) | 0.303 |
| Parent: fathers | −1.37 (2.10) | 0.517 |
| Treatment: MT + SSC | −3.26 (1.75) | 0.100 |
| One month assessment X Treatment: MT + SSC | −1.11(2.97) | 0.709 |
| Three months X treatment: MT + SSC | 2.98 (2.41) | 0.219 |
| Parent: father X treatment: MT + SSC | −1.40 (2.71) | 0.606 |
| State–Trait Anxiety Inventory | ||
| No. of observations: 400 | ||
| Intercept | 31.53 (1.46) | <0.001 |
| Second session | −1.68 (1.46) | 0.252 |
| Third session | −3.59 (1.59) | 0.024 |
| Session part: post | −4.72 (1.25) | <0.001 |
| Parent: fathers | 2.01 (1.61) | 0.213 |
| Treatment: MT + SSC | 3.59 (1.97) | 0.106 |
| Second session X treatment: MT + SSC | 2.11 (1.98) | 0.286 |
| Third session X treatment: MT + SSC | −1.12 (2.10) | 0.596 |
| Session part: post X treatment: MT + SSC | −2.74 (1.67) | 0.102 |
| Parent: father X treatment: MT + SSC | −2.60 (2.11) | 0.218 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yakobson, D.; Gold, C.; Beck, B.D.; Elefant, C.; Bauer-Rusek, S.; Arnon, S. Effects of Live Music Therapy on Autonomic Stability in Preterm Infants: A Cluster-Randomized Controlled Trial. Children 2021, 8, 1077. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111077
Yakobson D, Gold C, Beck BD, Elefant C, Bauer-Rusek S, Arnon S. Effects of Live Music Therapy on Autonomic Stability in Preterm Infants: A Cluster-Randomized Controlled Trial. Children. 2021; 8(11):1077. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111077
Chicago/Turabian StyleYakobson, Dana, Christian Gold, Bolette Daniels Beck, Cochavit Elefant, Sofia Bauer-Rusek, and Shmuel Arnon. 2021. "Effects of Live Music Therapy on Autonomic Stability in Preterm Infants: A Cluster-Randomized Controlled Trial" Children 8, no. 11: 1077. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111077