
What Are the Cleaning and Disinfection Methods for Acrylic Orthodontic Removable Appliance? A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Focused Question and Eligibility Criteria
- −
- P (Population/Problem): Removable acrylic orthodontic appliances worn by orthodontic patients;
- −
- I (Intervention): Cleaning and disinfection methods;
- −
- C (Comparison): Placebo or negative control;
- −
- O (Outcome): Global biofilm amount, S. mutans colony count or, Candida colony count on removable acrylic orthodontic appliances.
2.3. Search Strategy and Information Sources
2.4. Study Selection
2.5. Data Collection Procedure
2.6. Risk of Bias Evaluation
3. Results
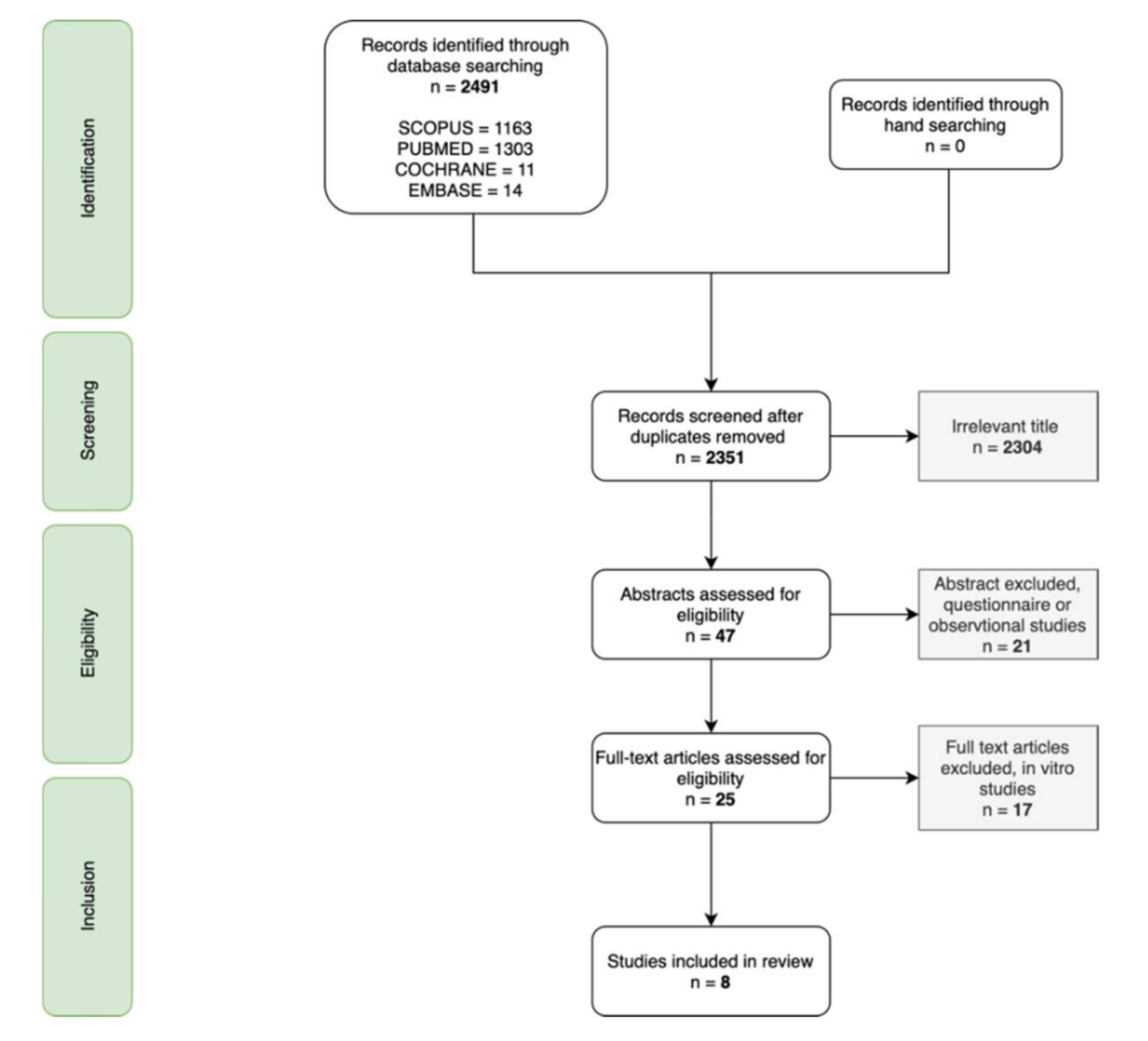
3.1. Study Selection
3.2. Study Characteristics
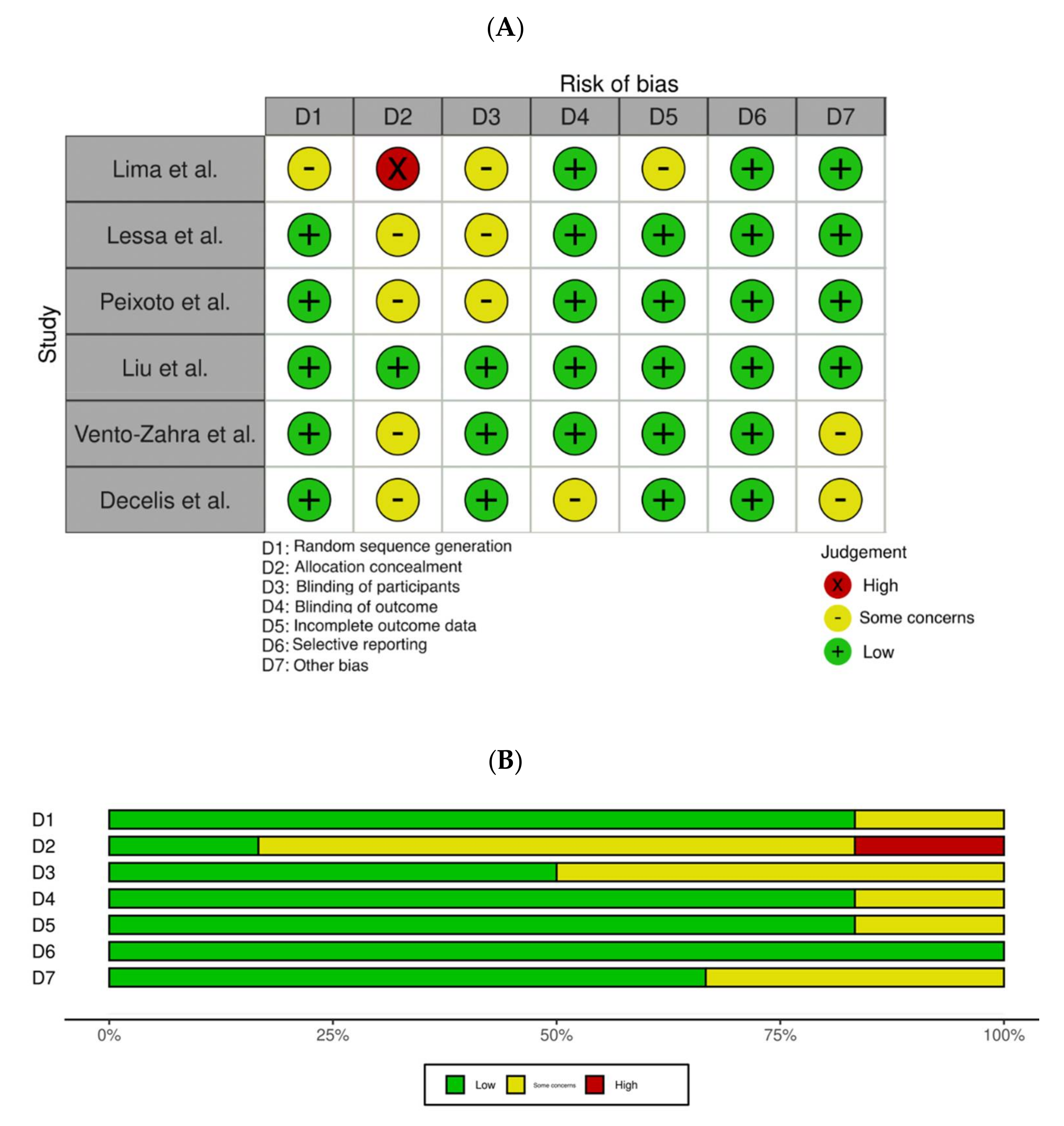
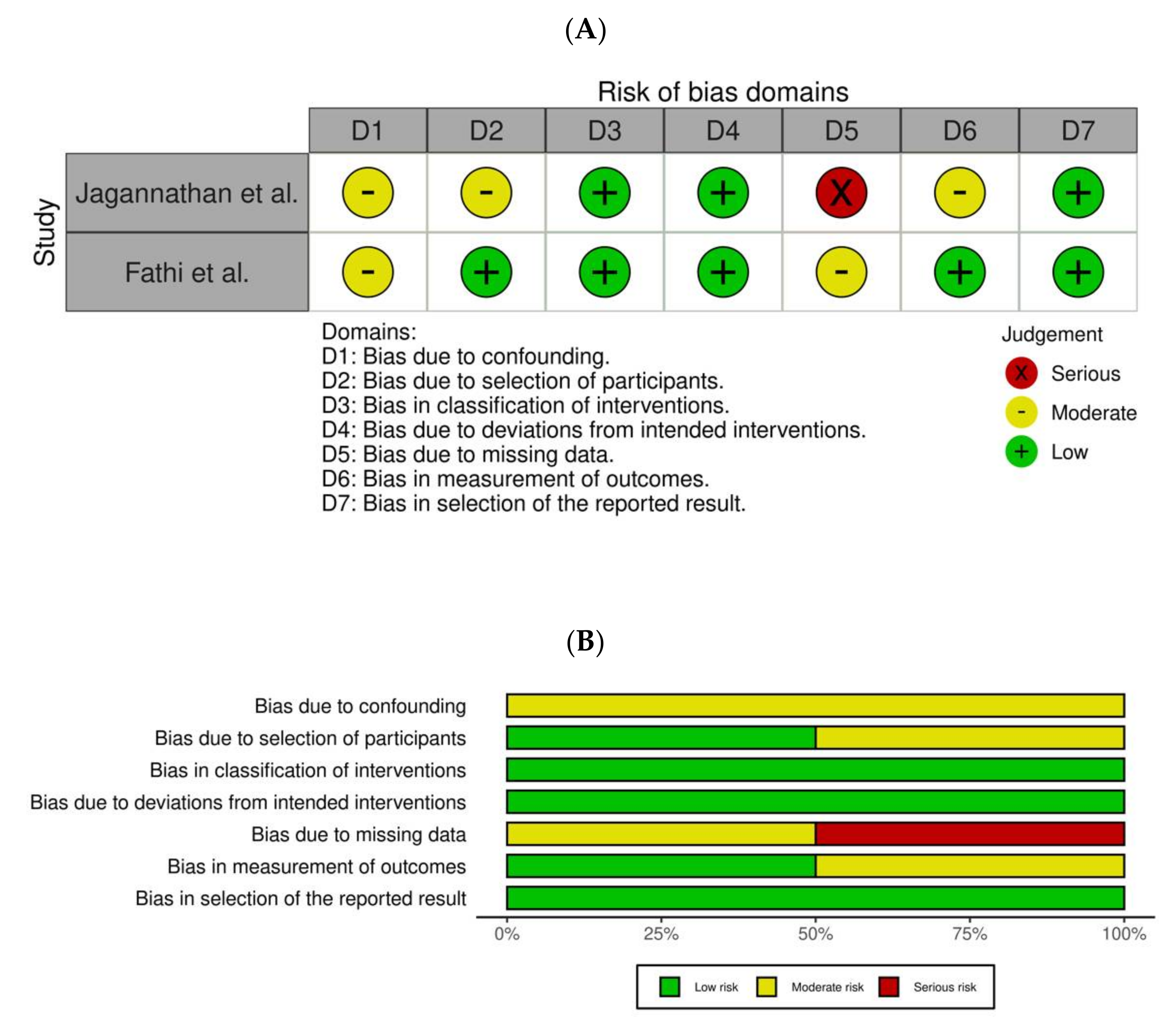
3.3. Results of Bias
3.4. Results of Individual Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alfuriji, S.; Alhazmi, N.; Alhamlan, N.; Al-Ehaideb, A.; Alruwaithi, M.; Alkatheeri, N.; Geevarghese, A. The Effect of Orthodontic Therapy on Periodontal Health: A Review of the Literature. Int. J. Dent. 2014, 2014, 585048. [Google Scholar] [CrossRef]
- Okada, E.M.P.; Ribeiro, L.N.S.; Borsatto, M.C.; De Paula-Silva, F.W.G.; Stuani, M.B.S.; Fidalgo, T.K.D.S.; Küchler, E.C. Effects of chlorhexidine varnish on caries during orthodontic treatment: A systematic review and meta-analysis. Braz. Oral Res. 2016, 30, e115. [Google Scholar] [CrossRef] [PubMed]
- Arab, S.; Malekshah, S.N.; Mehrizi, E.A.; Khanghah, A.E.; Naseh, R.; Imani, M.M. Effect of Fixed Orthodontic Treatment on Salivary Flow, pH and Microbial Count. J. Dent. Tehran Iran 2016, 13, 18–22. [Google Scholar]
- Topaloglu, A.; Ertugrul, F.; Eden, E.; Ates, M.; Bulut, H. Effect of Orthodontic Appliances on Oral Microbiota—6 Month Follow-up. J. Clin. Pediatr. Dent. 2011, 35, 433–436. [Google Scholar] [CrossRef]
- Jordan, C.; LeBlanc, D.J. Influences of orthodontic appliances on oral populations of mutans streptococci. Oral Microbiol. Immunol. 2002, 17, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Anhoury, P.; Nathanson, D.; Hughes, C.V.; Socransky, S.; Feres, M.; Chou, L.L. Microbial profile on metallic and ceramic bracket materials. Angle Orthod. 2002, 72, 338–343. [Google Scholar]
- Batoni, G.; Pardini, M.; Giannotti, A.; Ota, F.; Giuca, M.R.; Gabriele, M.; Campa, M.; Senesi, S. Effect of removable orthodontic appliances on oral colonisation by mutans streptococci in children. Eur. J. Oral Sci. 2001, 109, 388–392. [Google Scholar] [CrossRef]
- Nammi, K.; Starke, E.M.; Ou, S.-S.; Ward, M.; Jenkins, W.; Milleman, J.L.; Milleman, K.R. The Effects of Use of a Powered and a Manual Home Oral Hygiene Regimen on Plaque and Gum Health in an Orthodontic Population. J. Clin. Dent. 2019, 30, A1–A8. [Google Scholar] [PubMed]
- Deleuse, M.; Meiffren, C.; Bruwier, A.; Maes, N.; Le Gall, M.; Charavet, C. Smartphone application-assisted oral hygiene of orthodontic patients: A multicentre randomized controlled trial in adolescents. Eur. J. Orthod. 2020, 42, 605–611. [Google Scholar] [CrossRef]
- Jurišić, S.; Verzak, Ž.; Jurišić, G.; Jurić, H. Assessment of efficacy of two chlorhexidine mouthrinses on oral hygiene and gingival health in adolescents wearing two types of orthodontic brackets. Int. J. Dent. Hyg. 2018, 16, e52–e57. [Google Scholar] [CrossRef]
- Al-Musallam, T.A.; Evans, C.; Drummond, J.L.; Matasa, C.; Wu, C.D. Antimicrobial properties of an orthodontic adhesive combined with cetylpyridinium chloride. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Li, N.; Liu, B.; Zhang, Y. Preparation of an orthodontic bracket coated with an nitrogen-doped TiO(2-x)N(y) thin film and examination of its antimicrobial performance. Dent. Mater. J. 2013, 32, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Hibino, K.; Wong, R.W.K.; HÄgg, U.; Samaranayake, L.P. The effects of orthodontic appliances on Candida in the human mouth. Int. J. Paediatr. Dent. 2009, 19, 301–308. [Google Scholar] [CrossRef]
- Pathak, A.K.; Sharma, D.S. Biofilm Associated Microorganisms on Removable Oral Orthodontic Appliances in Children in the Mixed Dentition. J. Clin. Pediatr. Dent. 2013, 37, 335–340. [Google Scholar] [CrossRef]
- Rodríguez-Rentería, M.; Márquez-Preciado, R.; Ortiz-Magdaleno, M.; Bermeo-Escalona, J.; Sánchez-Vargas, L.O. Frequency of Pathogenic Microorganisms in Removable Orthodontic Appliances and Oral Mucosa in Children. J. Clin. Pediatr. Dent. 2021, 45, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Charman, K.M.; Fernandez, P.; Loewy, Z.; Middleton, A.M. Attachment of Streptococcus oralis on acrylic substrates of varying roughness. Lett. Appl. Microbiol. 2009, 48, 472–477. [Google Scholar] [CrossRef]
- Morgan, T.; Wilson, M. The effects of surface roughness and type of denture acrylic on biofilm formation by Streptococcus oralis in a constant depth film fermentor. J. Appl. Microbiol. 2001, 91, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Radford, D.; Sweet, S.; Challacombe, S.; Walter, J. Adherence of Candida albicans to denture-base materials with different surface finishes. J. Dent. 1998, 26, 577–583. [Google Scholar] [CrossRef]
- Eichenauer, J.; Serbesis, C.; Ruf, S. Cleaning removable orthodontic appliances—A survey. J. Orofac. Orthop. Fortschr. Kieferorthopädie 2011, 72, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Muscat, Y.; Farrugia, C.; Camilleri, L.; Arias-Moliz, M.T.; Valdramidis, V.; Camilleri, J. Investigation of Acrylic Resin Disinfection Using Chemicals and Ultrasound. J. Prosthodont. 2016, 27, 461–468. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.; Hernán, M.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuinness, L.A.; Higgins, J. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Vento-Zahra, E.; De Wever, B.; Decelis, S.; Mallia, K.; Camilleri, S. Randomized, double-blind, placebo-controlled trial to test the efficacy of nitradine tablets in maxillary removable orthodontic appliance patients. Quintessence Int. 2011, 42, 37–43. [Google Scholar]
- Decelis, S.; Camilleri, S.; Zahra, E.V.; Scerri, E.; De Wever, B. The effect of NitrAdine on the Candida levels of maxillary removable appliances. Quintessence Int. 2012, 43, 239–245. [Google Scholar] [PubMed]
- Peixoto, I.T.A.; Enoki, C.; Ito, I.Y.; Matsumoto, M.A.N.; Nelson-Filho, P. Evaluation of home disinfection protocols for acrylic baseplates of removable orthodontic appliances: A randomized clinical investigation. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.Y.; Tonggu, L.; Niu, L.N.; Gong, S.Q.; Fan, B.; Wang, L.; Zhao, J.H.; Huang, C.; Pashley, D.H.; Tay, F.R. Antimicrobial activity of a quaternary ammonium methacryloxy silicate-containing acrylic resin: A randomised clinical trial. Sci. Rep. 2016, 6, 21882. [Google Scholar] [CrossRef] [Green Version]
- Lima, E.M.C.X.; Moura, J.S.; Cury, A.A.D.B.; Garcia, R.C.M.R.; Cury, J.A. Effect of enzymatic and NaOCl treatments on acrylic roughness and on biofilm accumulation. J. Oral Rehabil. 2006, 33, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Lessa, F.; Enoki, C.; Ito, I.Y.; Faria, G.; Matsumoto, M.A.N.; Nelson-Filho, P. In-vivo evaluation of the bacterial contamination and disinfection of acrylic baseplates of removable orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 705.e11–705.e17. [Google Scholar] [CrossRef]
- Fathi, H.; Fathi, H.; Martiny, H.; Jost-Brinkmann, P.-G. Efficacy of cleaning tablets for removable orthodontic appliances: An in vivo pilot study. J. Orofac. Orthop. Fortschr. Kieferorthopädie 2015, 76, 143–151. [Google Scholar] [CrossRef]
- Jagannathan, J.; Kaniappan, A.S.; Raveendran, A.; Shekhar, S. Comparison of Antimicrobial Efficacy of Natural Extracts as a Disinfectant for Removable Orthodontic Appliances: An Ex Vivo Study. Int. J. Clin. Pediatr. Dent. 2021, 13, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Maruniak, J.; Clark, W.B.; Walker, C.B.; Magnusson, I.; Marks, R.G.; Taylor, M.; Clouser, B. The effect of 3 mouthrinses on plaque and gingivitis development. J. Clin. Periodontol. 1992, 19, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Catic, T.; Mehic, M.; Binakaj, Z.; Sahman, B.; Cordalija, V.; Kerla, A.; Martinovic, I.; Eskic, H. Efficacy and Safety of Oral Spray Containing Lysozyme and Cetylpyridinium: Subjective Determination of Patients with Tonsillopharyngitis. Mater. Socio Med. 2016, 28, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Guvenir, M.; Suer, K.; Ozkan, L. Antimicrobial effects of sodium hypochlorite and Er,Cr:YSGG laser against Enterococcus faecalis biofilm. Niger. J. Clin. Pract. 2020, 23, 1188–1193. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, D.; Narayanan, R.K.; Vadakkepurayil, K. A Comparative Evaluation on Antimicrobial Effect of Honey, Neem Leaf Extract and Sodium Hypochlorite as Intracanal Irrigant: An Ex-Vivo Study. J. Clin. Diagn. Res. 2016, 10, ZC88–ZC91. [Google Scholar] [CrossRef] [PubMed]
- Gong, S.-Q.; Epasinghe, J.; Rueggeberg, F.A.; Niu, L.-N.; Mettenberg, D.; Yiu, C.K.Y.; Blizzard, J.D.; Wu, C.D.; Mao, J.; Drisko, C.L.; et al. An ORMOSIL-Containing Orthodontic Acrylic Resin with Concomitant Improvements in Antimicrobial and Fracture Toughness Properties. PLoS ONE 2012, 7, e42355. [Google Scholar] [CrossRef] [Green Version]
- Gong, S.-Q.; Epasinghe, D.J.; Zhou, B.; Niu, L.-N.; Kimmerling, K.A.; Rueggeberg, F.; Yiu, C.K.; Mao, J.; Pashley, D.H.; Tay, F.R. Effect of water-aging on the antimicrobial activities of an ORMOSIL-containing orthodontic acrylic resin. Acta Biomater. 2013, 9, 6964–6973. [Google Scholar] [CrossRef] [Green Version]
- Kuroiwa, A.; Nomura, Y.; Ochiai, T.; Sudo, T.; Nomoto, R.; Hayakawa, T.; Kanzaki, H.; Nakamura, Y.; Hanada, N. Antibacterial, Hydrophilic Effect and Mechanical Properties of Orthodontic Resin Coated with UV-Responsive Photocatalyst. Materials 2018, 11, 889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-H.; Jo, J.-K.; Kim, D.-A.; Patel, K.D.; Kim, H.-W.; Lee, H.-H. Nano-graphene oxide incorporated into PMMA resin to prevent microbial adhesion. Dent. Mater. 2018, 34, e63–e72. [Google Scholar] [CrossRef]
- Lee, J.H.; El-Fiqi, A.; Jo, J.K.; Kim, D.A.; Kim, S.C.; Jun, S.K.; Kim, H.W.; Lee, H.H. Development of long-term antimicrobial poly(methyl methacrylate) by incorporating mesoporous silica nanocarriers. Dent. Mater. 2016, 32, 1564–1574. [Google Scholar] [CrossRef] [PubMed]
- Sodagar, A.; Khalil, S.; Kassaee, M.Z.; Shahroudi, A.S.; Pourakbari, B.; Bahador, A. Antimicrobial properties of poly (methyl methacrylate) acrylic resins incorporated with silicon dioxide and titanium dioxide nanoparticles on cariogenic bacteria. J. Orthod. Sci. 2016, 5, 7–13. [Google Scholar]
- Mangal, U.; Kim, J.-Y.; Seo, J.-Y.; Kwon, J.-S.; Choi, S.-H. Novel Poly(Methyl Methacrylate) Containing Nanodiamond to Improve the Mechanical Properties and Fungal Resistance. Materials 2019, 12, 3438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajami, S.; Habibagahi, R.; Khashei, R.; Soroorian, M. Evaluation of flexural strength and antibacterial effect of orthodontic acrylic resins containing Galla chinensis extract. Dent. Press J. Orthod. 2020, 25, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Pourhajibagher, M.; Salehi-Vaziri, A.; Noroozian, M.; Akbar, H.; Bazarjani, F.; Ghaffari, H.; Bahador, A. An orthodontic acrylic resin containing seaweed Ulva lactuca as a photoactive phytocompound in antimicrobial photodynamic therapy: Assessment of anti-biofilm activities and mechanical properties. Photodiagn. Photodyn Ther. 2021, 35, 102295. [Google Scholar] [CrossRef]
- Tsolakis, A.; Kakali, L.; Prevezanos, P.; Bitsanis, I.; Polyzois, G. Use of different cleaning methods for removable orthodontic appliances: A questionnaire study. Oral Health Prev. Dent. 2019, 17, 299–302. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Database | Keywords |
|---|---|
| Pubmed | ((“removable orthodontic appliance”) OR “Orthodontic Appliances, Removable”[MAJR] OR ((preventive OR functional) AND appliance AND orthod*) OR (orthod* resin) OR (orthod* acrylic)) AND (((removal OR reducing OR controlling) AND (biofilm OR bacteria OR “dental plaque”)) OR disinfection OR decontamination OR “Disinfection/methods”[MeSH] OR “Biofilms/drug effects”[MeSH] OR “Equipment Contamination/prevention and control”[Mesh] OR “Anti-Infective Agents, Local”[Mesh] OR “Oral Hygiene”[MeSH] OR antimicrobial OR antibacterial OR clean*) |
| Scopus | ((“removable orthodontic appliance”) OR ((preventive OR functional) AND appliance AND orthod*) OR (orthod* resin) OR (orthod* acrylic)) AND (((removal OR reducing OR controlling) AND (biofilm OR bacteria OR dental plaque)) OR decontamination OR disinfection OR antimicrobial OR antibacterial OR clean*) AND (LIMIT-TO (SUBJAREA,”DENT”)) AND NOT (fixed OR bracket) |
| Embase, Cochrane | (“removable appliance” AND “orthodontic”) AND (“biofilm removal” OR “biofilm adhesion” OR “decontamination” OR “disinfection” OR “dental plaque” OR “antimicrobial” OR “antibacterial” OR “clean*”) |
| Authors | Journal and Year Published | Study | Population | Inclusion and Exclusion Criteria | Intervention | Comparison | Support |
|---|---|---|---|---|---|---|---|
| Lima et al. [29] | Journal of Oral Rehabilitation, 2006 | RCT | 13 participants | N/A | 0.5% NaOCl solution or enzymatic solution (Ortoform®) | Sterile tap water | None |
| Lessa et al. [30] | AJODO, 2007 | RCT | 20 participants | No use of antimicrobial mouthwash, no systemic disease and no use of antibAliotics in the previous 3 months | Antimicrobial sprays: Periogard or Cepacol | Sterile tap water | None |
| Peixoto et al. [27] | AJODO, 2011 | RCT | 21 participants | Good general health, favorable dental alignment and salivary counts of S. mutans. No use of antimicrobial mouthwash, no systemic disease and no use of antibiotics in the previous 3 months | Periogard once or twice a week and manual brushing of appliance | Sterile tap water and manual brushing of appliance | None |
| Liu et al. [28] | Scientific Reports, 2016 | RCT | 32 participants | Good general health, no active caries or periodontal disease. No use of antimicrobial mouthwash, no use of antibiotics in the previous 6 months, no cleft palate or gag reflex. | QAMS-containing PMMA orthodontic resin | Conventional PMMA orthodontic resin | None |
| Fathi et al. [31] | Journal of Orofacial Orthopedics, 2015 | CCT | 20 participants | No dentures or orthodontic appliances, no missing teeth, no active caries or periodontal disease | Fittydent ®, NitrAdine ® or Kukis ® | Water | None |
| Jagganathan et al. [32] | Int Journal of Clinical Pediatric Dentistry, 2020 | CCT | 50 participants | Children in the mixed dentition using maxillary orthodontic appliances. Children not regularly visiting appointments or in the primary/permanent dentition were excluded. | Neem extract, katha extract and cinnamon extract | Chlorhexidine (positive control) and normal saline (negative control) | None |
| Vento-Zahra et al. [25] | Quintessence International, 2011 | RCT | 70 participants | Ongoing maxillary removable appliance therapy for more than 1-month, full time maxillary appliance wear, aged 11 to 14. | Nitradine® tablets | Placebo | Yes |
| Decelis et al. [26] | Quintessence International, 2012 | RCT | 92 participants | Orthodontic treatment for at least a month, aged 11 to 14. No conditions or undergoing treatment predisposing to oral candidosis. | Nitradine ® tablets | Placebo | Yes |
| Authors | Protocol | Variable (Main) | Results |
|---|---|---|---|
| Lima et al. [29] | Three phases of 4 days each, one for each treatment, with 3 different appliances of the same type. | Surface roughness and biofilm accumulation (light absorption at 280 nm) | No significant difference in surface roughness after treatment between Orthoform®, NaOCl and water (Control 0.497 mm; Orthoform® 0.535 mm; NaOCl 0.496 mm; p > 0.05). |
| Immersion eight times a day (5 min) in 20% sucrose solution to enhance biofilm formation. | In terms of biofilm accumulation, NaOCl was more efficient than control (Control: 0.547; NaOCl: 0.473; p < 0.05), but no difference was found between control and enzymatic solution (Control: 0.547; Orthoform®: 0.521; p > 0.05). | ||
| Daily immersion in 3 solutions: sterile tap water (negative control); enzymatic commercial solution (Ortoform®) (30 min) or 0.5% sodium hypochlorite (NaOCL) (10 min). | |||
| Lessa et al. [30] | A 3-stage changeover system with a 1-week interval between each stage (each stage being associated with a different solution). | S. mutans colony count (SEM examination) | Comparing S. mutans colony counts on appliances, both treatments were found significantly more efficient than control (p < 0.001). Periogard was found to be significantly more efficient than Cepacol (p < 0.001). |
| Acrylic baseplate worn full time for 7 days except during meals, brushed once a day with toothbrush and toothpaste used by the patient. The baseplate was retrieved after one week and sprayed on both sides following a randomized protocol with either 0.05% cetylpyridinium chloride solution (Cepacol), 0.12% chlorhexidine gluconate solution (Periogard), or sterile tap water. Baseplates were then placed in an individual sterile receptacle containing a selective enrichment broth for S. mutans and were incubated for 3 to 4 days at 37 °C. | |||
| Peixoto et al. [27] | Three-stage changeover system with a 1-week interval, each stage being associated with a different protocol. Acrylic baseplates were worn full time for 7 days except during meals, brushed thrice a day using a toothbrush and toothpaste. At bedtime, subjects were told to spray their appliances either: every day with sterile tap water (protocol I), on the 7th day with Periogard (protocol II), or on the 4th and 7th day with Periogard (protocol III). Baseplates were then placed in an individual sterile receptacle containing a selective enrichment broth for S. mutans and were incubated for 3 to 4 days at 37 °C. | S. mutans colony count (SEM examination) | Both protocols were significantly more efficient than control (percentage of S. mutans contaminated baseplates: water (protocol I) 100%; protocol II 80%; protocol III 60%; p < 0.05), but no significant difference was found between the two treatment protocols (p > 0.05). |
| Liu et al. [28] | Subjects were randomized into two groups: one whose appliance would have the QAMS-modified resin on the right side, and one who would have it on the right side (the other side being the control unmodified acrylic resin). The appliance was worn for 48 h continuously by subjects, then were retrieved for analysis of the resin disks. Biovolume was analyzed to determine the percentage of kill within the mass. | Percentage biofilm kill (CLSM examination) | QAMS had a significantly higher percentage kill than control disks (percentage kill in biovolume: control: 3.73 ± 2.11%; QAMS: 33.94 ± 22.88%; p ≤ 0.001). |
| Fathi et al. [31] | Splint was worn continuously for 96 h, taken off only for toothbrushing. They were then collected and randomized for cleaning protocol, which was either: immersion in fittydent super® for 30 min, in Kukis® for 10 min, in NitrAdine® for 15 min, or in water (control) for 10 min. The protein amount on the resin surface was calculated before and after cleaning. | Amount of biofilm (relative protein rate removal) | Comparing relative median protein rate removal, Fittydent was found significantly more efficient than Kukis (Fittydent: 86.8%; Kukis: 79.8%; p = 0.001), but no other significant difference was found between tablets (fittydent® vs. Nitradine®: 86.8% vs. 81.8%; p = 0.057; Nitradine® vs. Kukis®: 81.8% vs. 79.8%; p = 0.411). Tablets were all significantly more efficient than water (median protein removal rate for water: 56.6%; p < 0.003). |
| Jagganathan et al. [32] | Salivary swabs were collected from palatal side of the appliance. Neem, katha, and cinnamon extracts were prepared. Samples were inoculated on agar plates, and antimicrobial agents were introduced with a micropipette | Zone of inhibition of extracts in saliva cultures | According to the mean zone of inhibition in saliva cultures, all extracts were more significantly efficient than negative control and less than positive control (p < 0.001). Neem and katha extract were significantly more efficient than cinnamon extract (p < 0.001). |
| Vento-Zahra et al. [25] | Patients were randomized into two groups: experimental (NitrAdine® OrthoJunior) and control (placebo tablet). The appliance was treated by daily soaking in a solution containing the dissolved tablet and brushed with only water, for 6 weeks. Appliances were inspected visually before and after treatment, and saliva samples were collected and analyzed before and after treatment. | Salivary Candida levels | NitrAdine tablets significantly decreased significantly plaque index (p = 0.0253) and odor (p = 0.0007) of the appliance compared to the control group. However, no significant difference was found in salivary Candida levels between the two groups. |
| Plaque index on the appliance | |||
| Appliance odor | |||
| Decelis et al. [26] | Patients were randomized into two groups: experimental (NitrAdine® OrthoJunior) and control (placebo tablet). The appliance was treated by daily soaking for 20 min in a solution containing the dissolved tablet and brushed with only water, for 6 weeks. Samples were taken on the palatal side of the appliance before and after treatment. | Candida colony count | Significant increase in Candida levels for control group during treatment (p = 0.008). A decrease, but not significant, of Candida levels during treatment for experimental group was found (p = 0.353). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charavet, C.; Graveline, L.; Gourdain, Z.; Lupi, L. What Are the Cleaning and Disinfection Methods for Acrylic Orthodontic Removable Appliance? A Systematic Review. Children 2021, 8, 967. https://0-doi-org.brum.beds.ac.uk/10.3390/children8110967
Charavet C, Graveline L, Gourdain Z, Lupi L. What Are the Cleaning and Disinfection Methods for Acrylic Orthodontic Removable Appliance? A Systematic Review. Children. 2021; 8(11):967. https://0-doi-org.brum.beds.ac.uk/10.3390/children8110967
Chicago/Turabian StyleCharavet, Carole, Léa Graveline, Zoé Gourdain, and Laurence Lupi. 2021. "What Are the Cleaning and Disinfection Methods for Acrylic Orthodontic Removable Appliance? A Systematic Review" Children 8, no. 11: 967. https://0-doi-org.brum.beds.ac.uk/10.3390/children8110967