
Analysis of the Impact of Oral Health on Adolescent Quality of Life Using Standard Statistical Methods and Artificial Intelligence Algorithms


 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Respondents and Research Protocol
2.2. The Impact of Oral Health on Adolescent Quality of Life
2.3. Artificial Intelligence Algorithms
3. Results
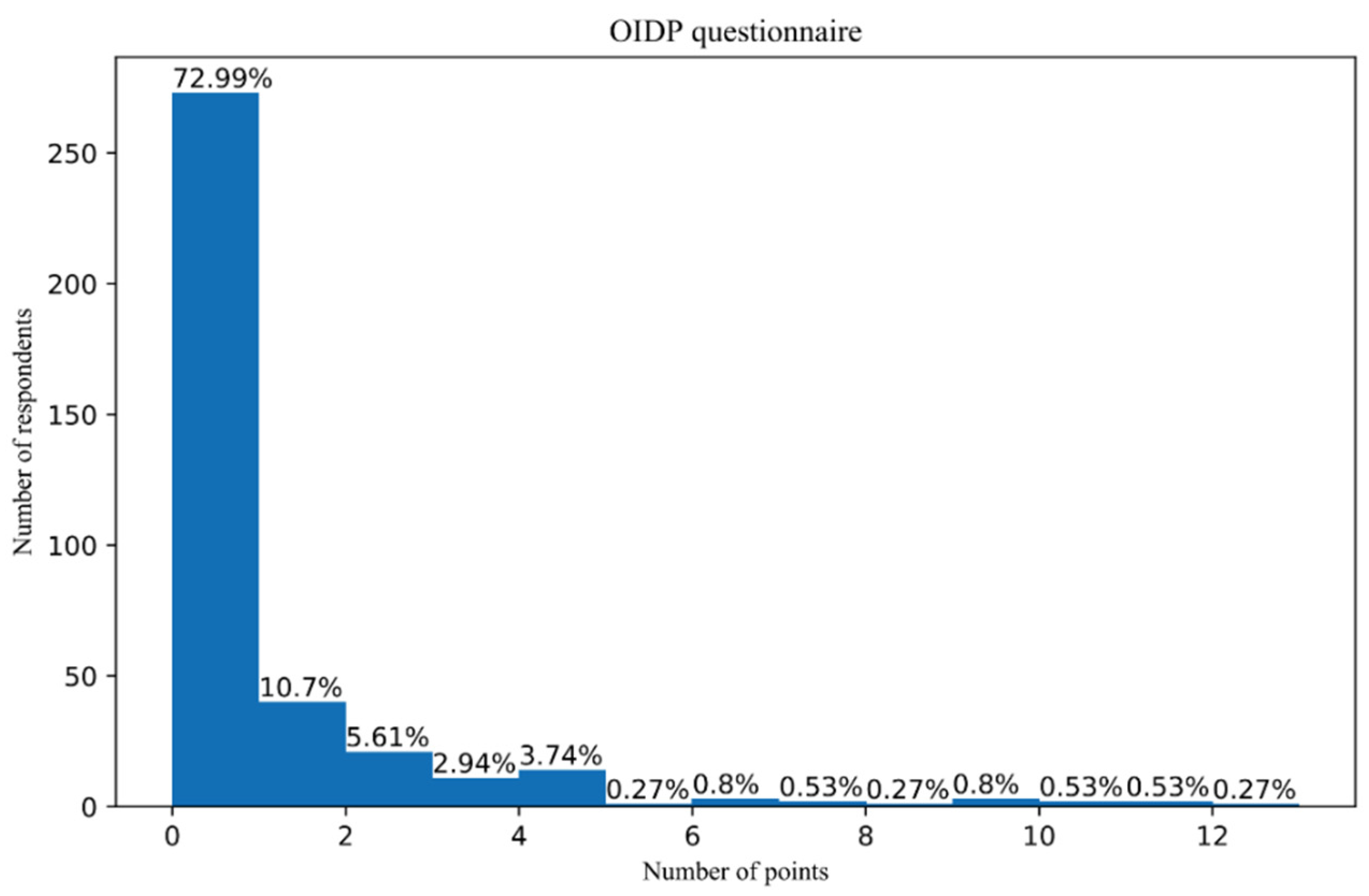
- (1)
- Absence of oral impact on daily activities (OIDP score = 0);
- (2)
- Presence of oral impact on daily activities (OIDP score > 0) (Table 2).
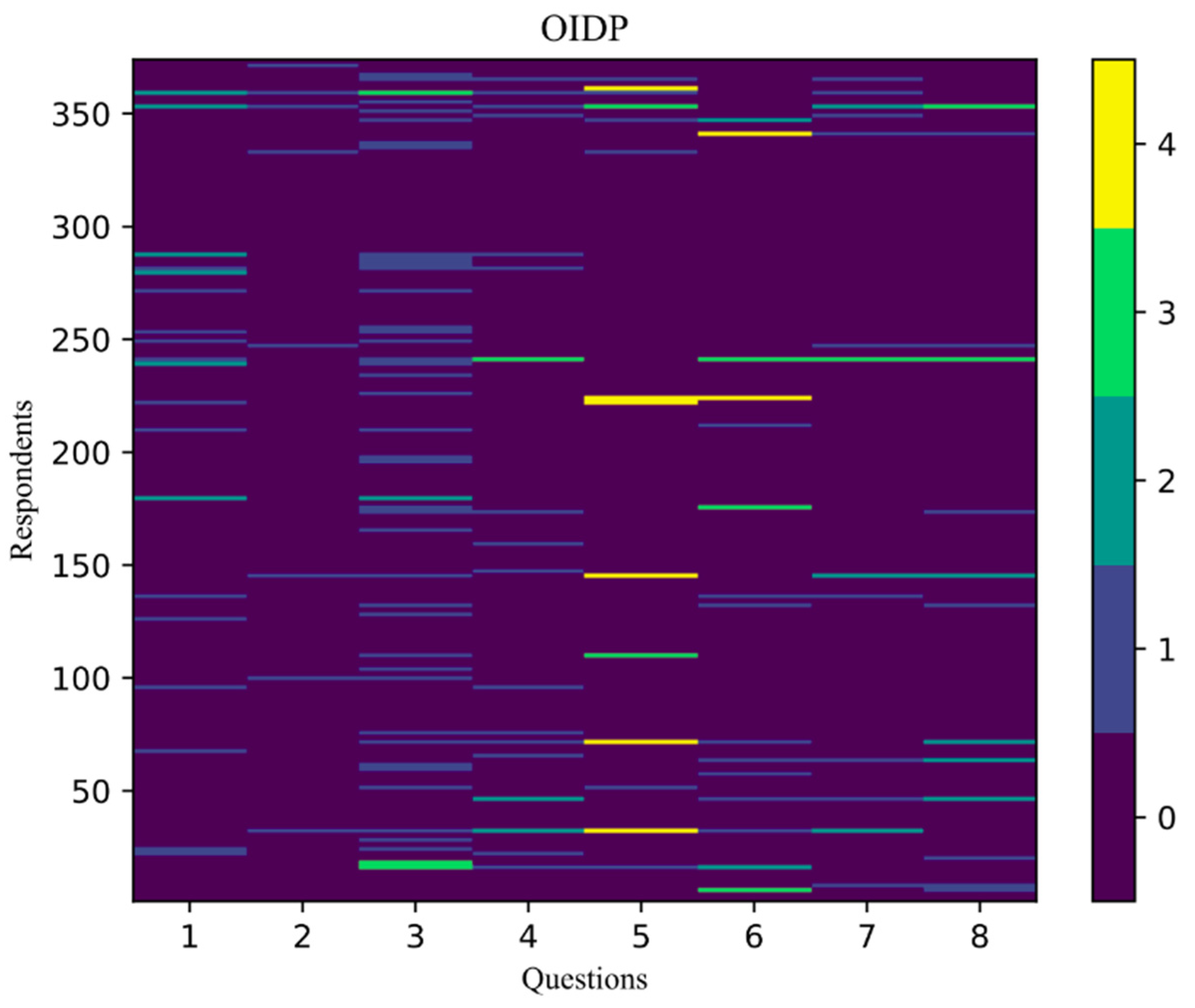
- Never or less than once a month—0 points—purple;
- Once to twice a month—1 point—blue;
- Once to twice a week—2 points—turquoise;
- Three to four times a week—3 points—green;
- Almost every day—4 points—yellow.
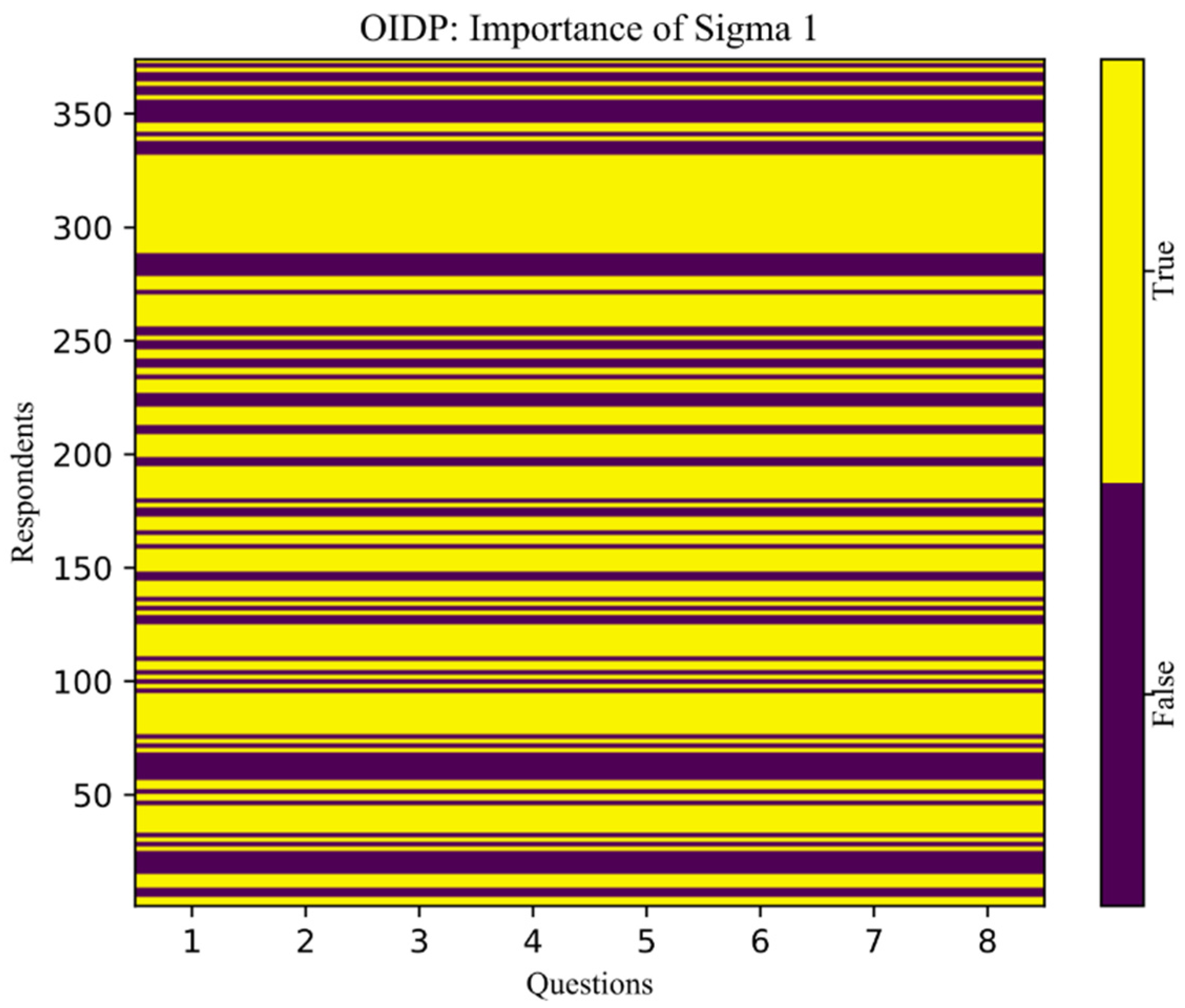
- “True”—yellow color;
- “False”—purple color.
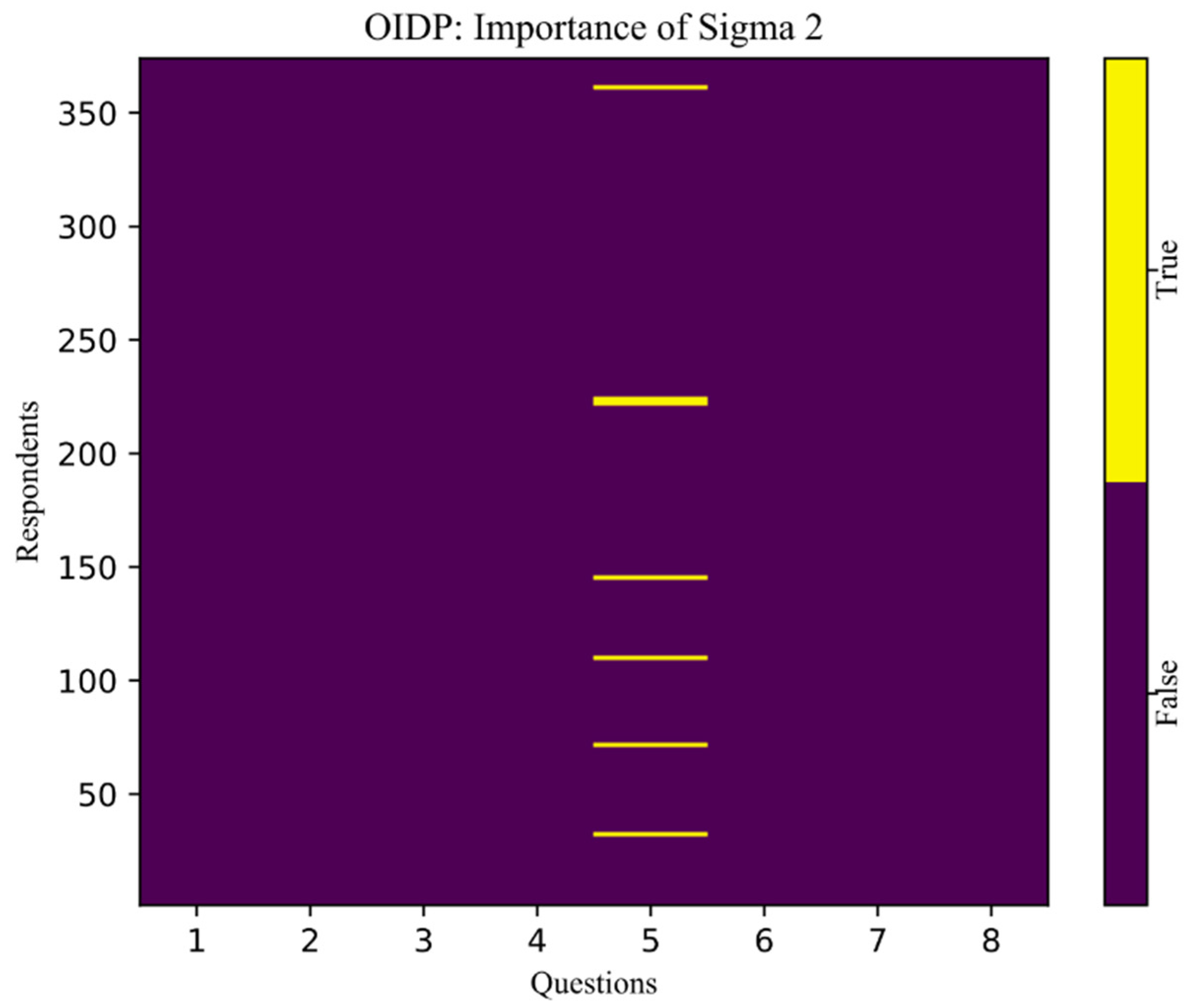
- “False”—purple;
- “True”—yellow.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gajic, M. Exploring the Impact of Oral Health on Adolescents’ Health Related Quality of Life by Means of Artificial Intelligence Algorithms. Ph.D. Thesis, Faculty of Stomatology Pancevo, University Business Academy in Novi Sad, Pancevo, Serbia, 2018. [Google Scholar]
- Gilbert, G.H.; Litaker, M.S. Validity of Self-Reported Periodontal Status in the Florida Dental Care Study. J. Periodontol. 2007, 78, 1429–1438. [Google Scholar] [CrossRef]
- Adulyanon, S.; Vourapukjaru, J.; Sheiham, A. Oral impacts affecting daily performance in a low dental disease Thai population. Community Dent. Oral Epidemiol. 1996, 24, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Stancic, I.; Kulic, J.; Sojic, L.T.; Stojanovic, Z. Applicability of a Serbian version of the “Oral Impacts on Daily Performance (OIDP)” index—assessment of oral health-related quality of life. Vojn. Pregl. 2012, 69, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Gajic, M.; Lalic, M.; Kalevski, K.; Marjanovic, M. Oral health-related quality of life among Belgrade adolescents. Vojn. Pregl. 2018, 75, 8–15. [Google Scholar] [CrossRef]
- Alsumait, A.; El Salhy, M.; Raine, K.; Cor, K.; Gokiert, R.; Al-Mutawa, S.; Amin, M. Impact of dental health on children's oral health-related quality of life: A cross-sectional study. Heal. Qual. Life Outcomes 2015, 13, 98. [Google Scholar] [CrossRef] [Green Version]
- Ko, C.C.; Shen, D.; Wang, L. Machine Learning in Dentistry; Springer: Berlin/Heidelberg, Germany, 2021; ISBN 978-3-030-71880-0. [Google Scholar] [CrossRef]
- Marjanovic, V.; Gracia, J.; Glass, C.W. HPC benchmarking: Problem size matters. In Proceedings of the PMBS 2016: 7th International Workshop on Performance Modeling, Benchmarking and Simulation of High Performance Computing Systems—Held in conjunction with SC 2016. The International Conference for High Performance Computing, Networking, Salt Lake City, UT, USA, 14 November 2016; pp. 1–10. [Google Scholar]
- Bryt, O.; Elad, M. Compression of facial images using the K-SVD algorithm. J. Vis. Commun. Image Represent. 2008, 19, 270–282. [Google Scholar] [CrossRef]
- Rykaczewski, R. Comments on “An SVD-Based Watermarking Scheme for Protecting Rightful Ownership”. IEEE Trans. Multimedia 2007, 9, 421–423. [Google Scholar] [CrossRef]
- Lei, B.; Soon, I.Y.; Tan, E.-L. Robust SVD-Based Audio Watermarking Scheme with Differential Evolution Optimization. IEEE Trans. Audio Speech, Lang. Process. 2013, 21, 2368–2378. [Google Scholar] [CrossRef]
- De Lathauwer, L.; De Moor, B.; Vandewalle, J. A Multilinear Singular Value Decomposition. SIAM J. Matrix Anal. Appl. 2000, 21, 1253–1278. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.; Sun, H.; Yao, T. A SVD- and quantization based semi-fragile watermarking technique for image authentication. In Proceedings of the 6th International Conference on Signal Processing, Beijing, China, 26–30 August 2002. [Google Scholar] [CrossRef]
- Strang, G. Linear Algebra and Its Applications; Thomson Brooks/Cole: Belmont, CA, USA, 2012. [Google Scholar]
- Golub, G.H.; Van Loan, C.F. Matrix Computations; Johns Hopkins University Press: Baltimore, MD, USA, 1996. [Google Scholar]
- Gajic, M.; Lalic, M.; Kalevski, K.; Lazic, E.; Pavlovic, M.; Ivanovic, M.; Milic, J.; Matijevic, D.; Vojinovic, J. The application of artificial intelligence algorithms for testing the correlation between the state of oral health and adolescent behavior concerning oral health. Vojn. Pregl. 2021, 78, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Klein, F. Elementary Mathematics from an Advanced Standpoint, Geometry; Dover Publications, INC: Mineola, NY, USA, 1908; 1939(1):80. [Google Scholar]
- Tada, A.; Hanada, N. Sexual differences in oral health behaviour and factors associated with oral health behaviour in Japanese young adults. Public Health 2004, 118, 104–109. [Google Scholar] [CrossRef]
- Vazquez, F.D.L.; Cortellazzi, K.L.; Kaieda, A.K.; Guerra, L.M.; Ambrosano, G.M.B.; Tagliaferro, E.P.D.S.; Mialhe, F.L.; Meneghim, M.D.C.; Pereira, A.C. Quality of life and socio-dental impact among underprivileged Brazilian adolescents. Qual. Life Res. 2014, 24, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Fortunato, L.; Nobile, C.G.A.; Pavia, M. Prevalence and determinants of oral impacts on daily performance: Results from a survey among school children in Italy. Eur. J. Public Health 2009, 20, 595–600. [Google Scholar] [CrossRef] [Green Version]
- Pentapati, K.C.; Acharya, S.; Bhat, M.; Rao, S.V.K.; Singh, S. Oral health impact, dental caries, and oral health behaviors among the National Cadets Corps in South India. J. Investig. Clin. Dent. 2012, 4, 39–43. [Google Scholar] [CrossRef]
- Caglayan, F.; Altun, O.; Mil Oglu, O.; Kaya, M.D.; Yilmaz, A.B. Correlation between oral health-related quality of life (HRQoL) and oral disorders in a Turkish patient population. Med. Oral Patol. Oral Y Cirugía Bucal. 2009, 14, 573–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagarajappa, R.; Batra, M.; Sanadhya, S.; Daryani, H.; Ramesh, G. Relationship between oral clinical conditions and daily performances among young adults in India—A cross sectional study. J. Epidemiol. Glob. Health 2015, 5, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Peres, K.; Cascaes, A.; Leão, A.; Côrtes, M.; Vettore, M. Aspectos sociodemográficos e clínicos da qualidade de vida relacionada à saúde bucal em adolescentes. Rev. Saúde Pública 2013, 47 (Suppl. 3), 19–28. [Google Scholar] [CrossRef] [Green Version]
- Pavlović, M. Oral Status and Need for Prosthodontic Treatment in Urban Adolescents. Ph.D. Thesis, Faculty of Stomatology Pancevo, University Business Academy in Novi Sad, Pancevo, Serbia, 2016. [Google Scholar]
- Tsakos, G.; Bernabé, E.; O'Brien, K.; Sheiham, A.; de Oliveira, C. Comparison of the self-administered and interviewer-administered modes of the child-OIDP. Heal. Qual. Life Outcomes 2008, 6, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.J.; Cheng, M.L.; Zhang, C.Z.; Xu, M.R.; Gao, X.L.; Du, S.; Ding, M.; Wang, X.; Feng, X.P.; Tai, B.J.; et al. Associated Factors of Oral Health-related Quality of Life in Chinese Adolescents Aged 12–15 Years. Chin. J. Dent. Res. Off. J. Sci. Sect. Chin. Stomatol. Assoc. (CSA) 2021, 24, 105–112. [Google Scholar] [CrossRef]
- Chukwumah, N.M.; Folayan, M.O.; Oziegbe, E.O.; Umweni, A.A. Impact of dental caries and its treatment on the quality of life of 12- to 15-year-old adolescents in Benin, Nigeria. Int. J. Paediatr. Dent. 2015, 26, 66–76. [Google Scholar] [CrossRef]
- Shekhawat, K.S.; Samuel, S.R.; Chauhan, A. Frequency of Oral Impacts on Daily Performances and Dental Pain Among Indigenous Adolescents of Himalayas (Leh, Ladakh): A Cross-Sectional Study. Oral Health Prev. Dent. 2021, 19, 115–120. [Google Scholar] [CrossRef]
- Mota-Veloso, I.; Soares, M.E.C.; Alencar, B.M.; Marques, L.S.; Ramos-Jorge, M.L.; Ramos-Jorge, J. Impact of untreated dental caries and its clinical consequences on the oral health-related quality of life of schoolchildren aged 8–10 years. Qual. Life Res. 2015, 25, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Habbu, S.G.; Krishnappa, P. Effectiveness of oral health education in children—A systematic review of current evidence (2005–2011). Int. Dent. J. 2015, 65, 57–64. [Google Scholar] [CrossRef]
- de Aquino Goulart, M.; Vendrame, É.; de Aquino Goulart, J.T.; Celeste, R.K. Parenting practices and oral impact on daily performance in southern Brazil. J. Public Heath. Dent. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Knorst, J.K.; Brondani, B.; Tomazoni, F.; Vargas, A.W.; Cósta, M.D.; Godois, L.D.S.; Mendes, F.M.; Ardenghi, D.M.; Ardenghi, T.M. COVID-19 pandemic reduces the negative perception of oral health-related quality of life in adolescents. Qual. Life Res. 2021, 30, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Kolawole, K.A.; Ayodele-Oja, M.M. Oral health–related quality of life of adolescents assessed with the Malocclusion Impact and Child Perceptions questionnaires. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e149–e156. [Google Scholar] [CrossRef]
- Veras, S.; Kozmhinsky, V.; Goes, P.; Heimer, M. Behavioral and Psychosocial Factors as Mediators of the Oral Health Impact on Adolescents Quality of Life. Quality of Life—Biopsychosocial Perspectives; IntechOpen: London, UK, 2020. [Google Scholar] [CrossRef] [Green Version]
- Keles, S.; Abacigil, F.; Adana, F. Oral Health Status and Oral Health Related Quality of Life in Adolescent Workers. Med. Pharm. Rep. 2018, 91, 462–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crocombe, L.A.; Broadbent, J.; Thomson, W.M.; Brennan, D.S.; Poulton, R. Impact of dental visiting trajectory patterns on clinical oral health and oral health-related quality of life. J. Public Health Dent. 2011, 72, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Miladinovic, M.; Mihailovic, B.; Mladenovic, D.; Duka, M.; Zivkovic, D.; Mladenovic, S.; Subaric, L. Artificial intelligence in clinical medicine and dentistry. Vojn. Pregl. 2017, 74, 267–272. [Google Scholar] [CrossRef] [Green Version]
- Schwendicke, F.; Samek, W.; Krois, J. Artificial Intelligence in Dentistry: Chances and Challenges. J. Dent. Res. 2020, 99, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Shan, T.; Tay, F.; Gu, L. Application of Artificial Intelligence in Dentistry. J. Dent. Res. 2020, 100, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Machoy, M.E.; Szyszka-Sommerfeld, L.; Vegh, A.; Gedrange, T.; Woźniak, K. The ways of using machine learning in dentistry. Adv. Clin. Exp. Med. 2020, 29, 375–384. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OIDP Questionnaire t-test for Males and Females | |||
|---|---|---|---|
| Statistical Parameters | Males | Females | Total |
| n | 128 | 246 | 374 |
| Minimum value | 0 | 0 | 0 |
| Maximum value | 14 | 14 | 14 |
| Average value | 1.28 | 1.14 | 1.19 |
| SE | 0.33 | 0.22 | 0.18 |
| SD | 2.64 | 2.40 | 2.48 |
| CV (%) | 205.79 | 210.88 | 209.29 |
| 95% CI | |||
| Lower limit | 0.62 | 0.70 | 0.82 |
| Upper limit | 1.95 | 1.57 | 1.55 |
| Significance of differences in average values | |||
| t = 0.372 | |||
| p = 0.711 | |||
| Dichotomized OIDP Score for Both Sexes | |||
|---|---|---|---|
| Impact of Mouth and Teeth on | OIDP > 0 | OIDP = 0 | |
| Males | Females | ||
| Eating and enjoying food | 4% | 6% | 90% |
| Speaking and pronouncing clearly | 0% | 4% | 96% |
| Cleaning teeth | 8% | 15% | 77% |
| Sleeping and relaxing | 4% | 6% | 90% |
| Smiling, laughing and showing teeth without embarrassment | 3% | 4% | 93% |
| Maintaing usual emotional state without being irritable | 3% | 5% | 92% |
| Enjoying contact with people or social role | 3% | 4% | 93% |
| Carrying out major work | 3% | 4% | 93% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajic, M.; Vojinovic, J.; Kalevski, K.; Pavlovic, M.; Kolak, V.; Vukovic, B.; Mladenovic, R.; Aleksic, E. Analysis of the Impact of Oral Health on Adolescent Quality of Life Using Standard Statistical Methods and Artificial Intelligence Algorithms. Children 2021, 8, 1156. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121156
Gajic M, Vojinovic J, Kalevski K, Pavlovic M, Kolak V, Vukovic B, Mladenovic R, Aleksic E. Analysis of the Impact of Oral Health on Adolescent Quality of Life Using Standard Statistical Methods and Artificial Intelligence Algorithms. Children. 2021; 8(12):1156. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121156
Chicago/Turabian StyleGajic, Milica, Jovan Vojinovic, Katarina Kalevski, Maja Pavlovic, Veljko Kolak, Branislava Vukovic, Rasa Mladenovic, and Ema Aleksic. 2021. "Analysis of the Impact of Oral Health on Adolescent Quality of Life Using Standard Statistical Methods and Artificial Intelligence Algorithms" Children 8, no. 12: 1156. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121156