
Standards of Nutritional Care for Patients with Cystic Fibrosis: A Methodological Primer and AGREE II Analysis of Guidelines

 ,
,  , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. PICAR, Search Strategy, Inclusion, and Exclusion Criteria
2.2. Inclusion and Exclusion Criteria
2.3. Appraisal of CPGs
2.4. CPGs Review and MNT Information
3. Results
3.1. Retrieved CPGs and Their Characteristics
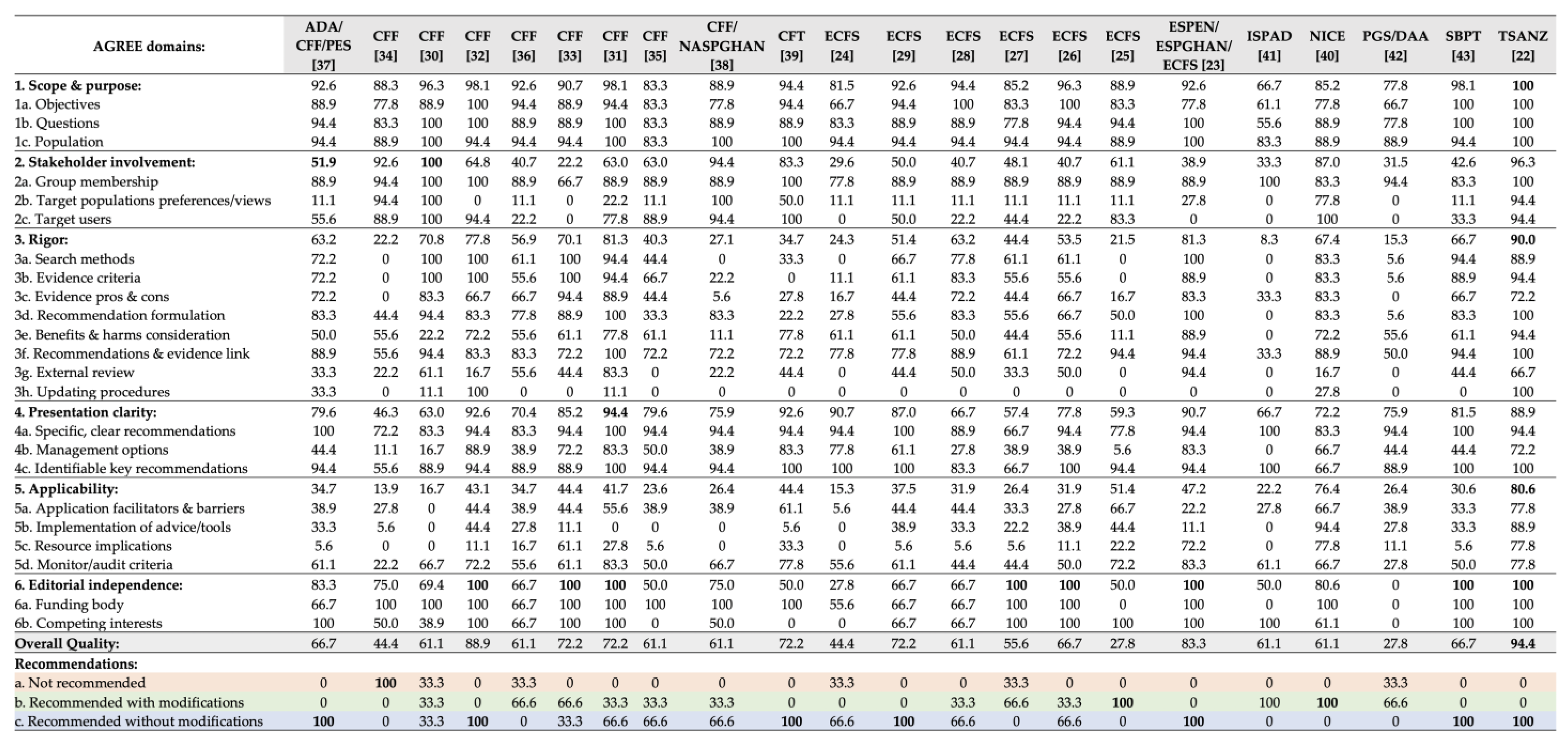
3.2. AGREE Scoring of Included Guidelines
3.3. Nutrition Recommendations in the Included Guidelines
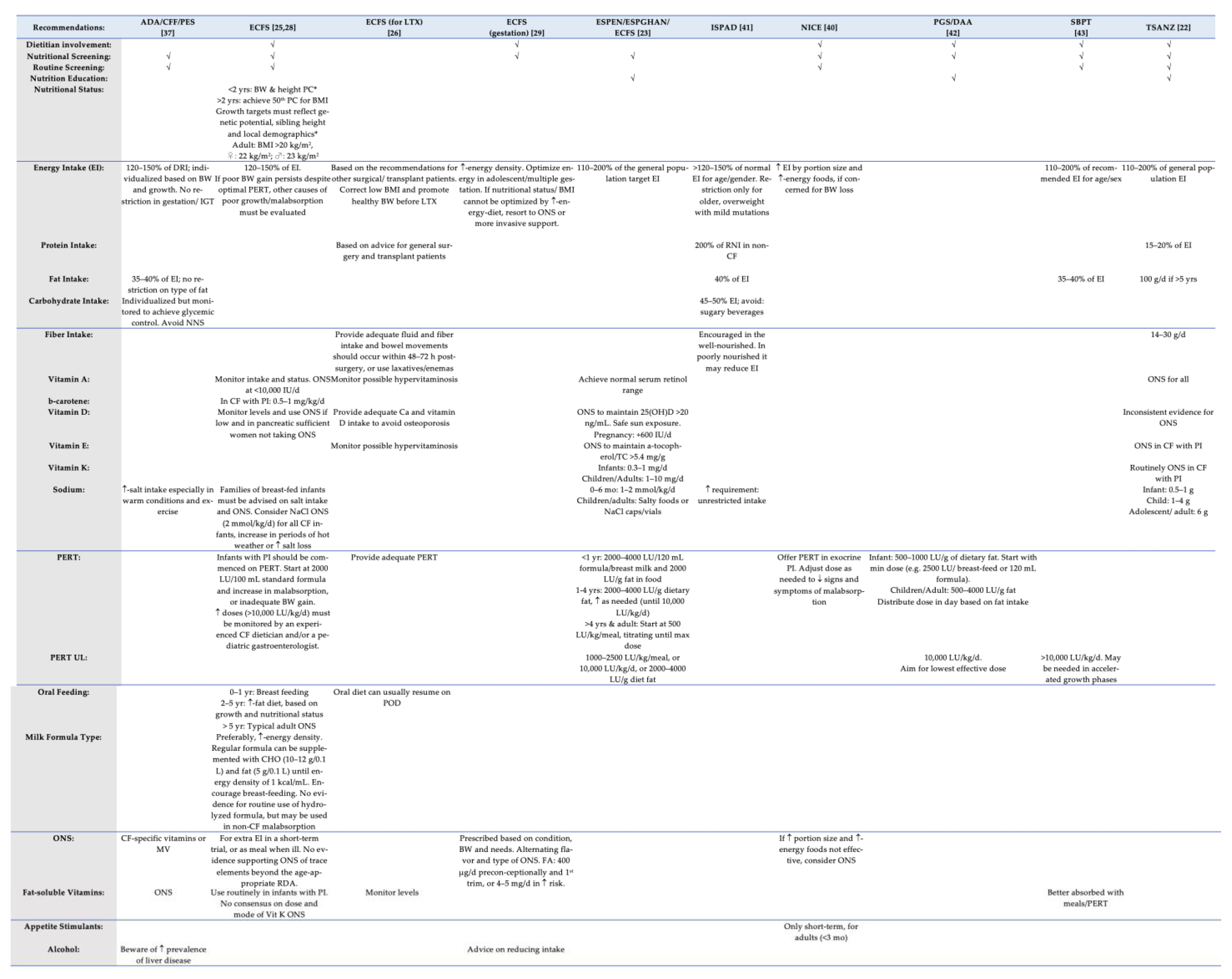
3.3.1. General Features of the Delivery MNT in Patients with CF
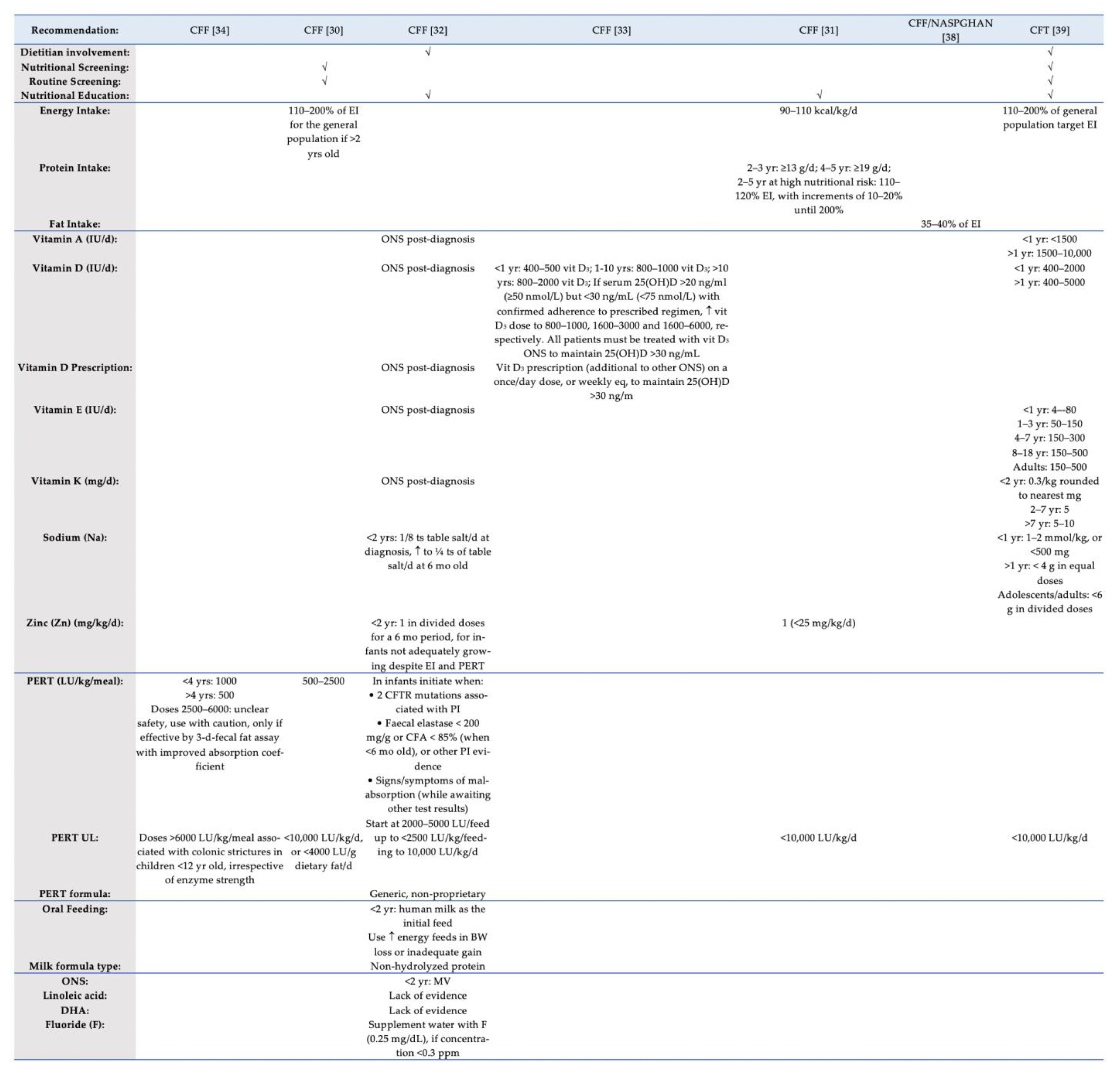
3.3.2. Energy and Nutrient Intake
3.3.3. Pancreatic Enzyme Replacement Therapy (PERT)
3.3.4. Oral Feeding and Formula Type
3.3.5. Other Issues of Nutritional Concern
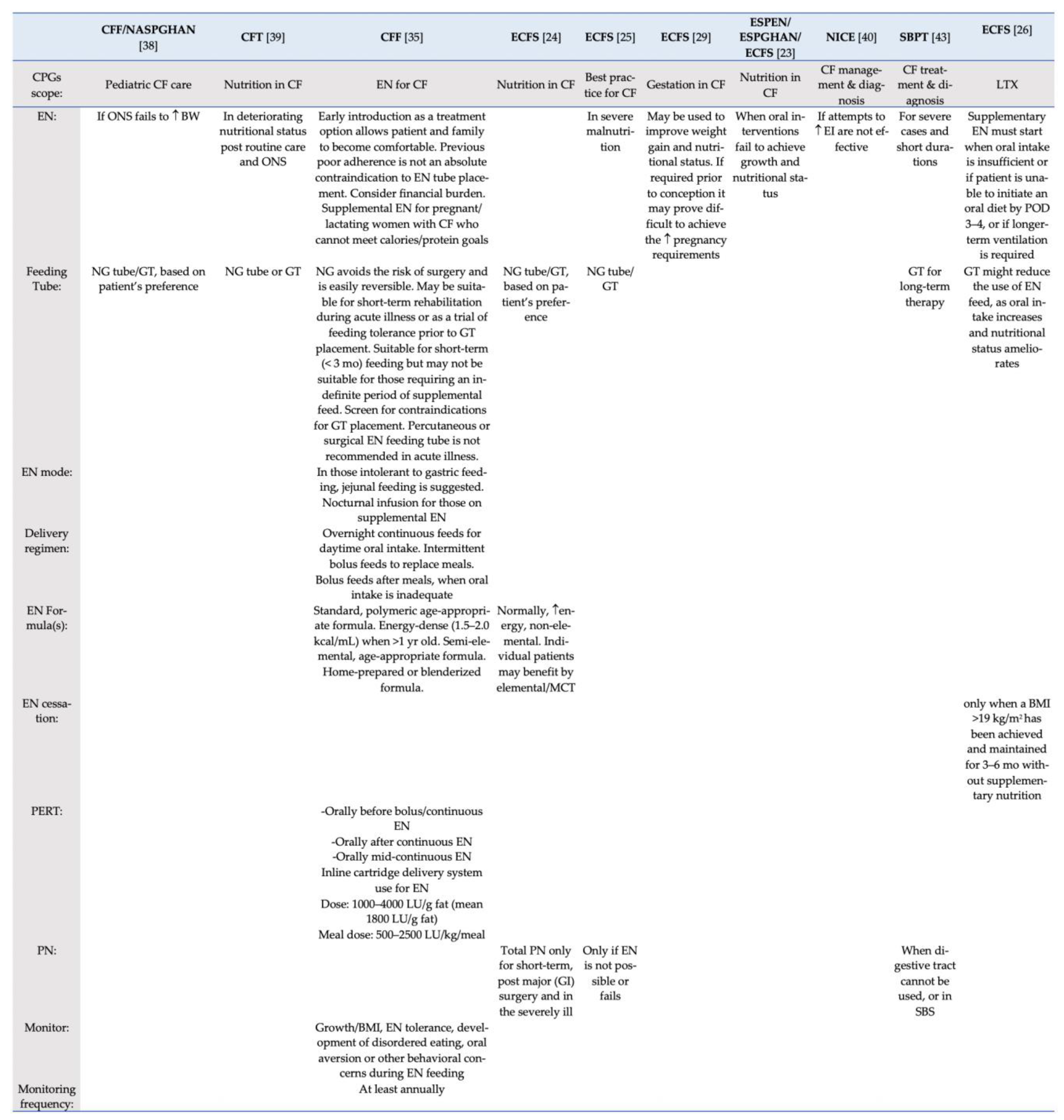
3.3.6. Provision of EN and PN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farrell, P.M.; White, T.B.; Ren, C.L.; Hempstead, S.E.; Accurso, F.; Derichs, N.; Howenstine, M.; McColley, S.A.; Rock, M.; Rosenfeld, M.; et al. Diagnosis of Cystic Fibrosis: Consensus Guidelines from the Cystic Fibrosis Foundation. J. Pediatr. 2017, 181, S4–S15.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drumm, M.L.; Collins, F.S. Molecular biology of cystic fibrosis. Mol. Genet. Med. 1993, 3, 33–68. [Google Scholar]
- Kerem, B.; Rommens, J.M.; Buchanan, J.A.; Markiewicz, D.; Cox, T.K.; Chakravarti, A.; Buchwald, M.; Tsui, L.C. Identification of the cystic fibrosis gene: Genetic analysis. Science 1989, 245, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Calella, P.; Valerio, G.; Brodlie, M.; Donini, L.M.; Siervo, M. Cystic fibrosis, body composition, and health outcomes: A systematic review. Nutrition 2018, 55–56, 131–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, J.J.; Edwards, C.A.; Weaver, L.T. Malnutrition in children with cystic fibrosis: The energy-balance equation. J. Pediatr. Gastroenterol. Nutr. 1997, 25, 127–136. [Google Scholar] [CrossRef]
- Zemel, B.S.; Jawad, A.F.; FitzSimmons, S.; Stallings, V.A. Longitudinal relationship among growth, nutritional status, and pulmonary function in children with cystic fibrosis: Analysis of the Cystic Fibrosis Foundation National CF Patient Registry. J. Pediatr. 2000, 137, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Bradley, G.M.; Blackman, S.M.; Watson, C.P.; Doshi, V.K.; Cutting, G.R. Genetic modifiers of nutritional status in cystic fibrosis. Am. J. Clin. Nutr. 2012, 96, 1299–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauschild, D.B.; Rosa, A.F.; Ventura, J.C.; Barbosa, E.; Moreira, E.A.M.; Ludwig Neto, N.; Moreno, Y.M.F.; Moreno, Y.M.F. Association of nutritional status with lung function and morbidity in children and adolescents with cystic fibrosis: A 36-month cohort study. Rev. Paul. Pediatr. 2018, 36, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smyth, R.L.; Rayner, O. Oral calorie supplements for cystic fibrosis. Cochrane Database Syst. Rev. 2017, 5, CD000406. [Google Scholar] [CrossRef] [Green Version]
- Poulimeneas, D.; Petrocheilou, A.; Grammatikopoulou, M.G.; Kaditis, A.G.; Loukou, I.; Doudounakis, S.E.; Laggas, D.; Vassilakou, T. High attainment of optimal nutritional and growth status observed among Greek pediatric cystic fibrosis patients: Results from the GreeCF study. J. Pediatr. Endocrinol. Metab. 2017, 30, 1169–1176. [Google Scholar] [CrossRef]
- McNamara, J.J.; McColley, S.A.; Marigowda, G.; Liu, F.; Tian, S.; Owen, C.A.; Stiles, D.; Li, C.; Waltz, D.; Wang, L.T.; et al. Safety, pharmacokinetics, and pharmacodynamics of lumacaftor and ivacaftor combination therapy in children aged 2–5 years with cystic fibrosis homozygous for F508del-CFTR: An open-label phase 3 study. Lancet Respir. Med. 2019, 7, 325–335. [Google Scholar] [CrossRef]
- McPhail, G.L.; Acton, J.D.; Fenchel, M.C.; Amin, R.S.; Seid, M. Improvements in Lung Function Outcomes in Children with Cystic Fibrosis are Associated with Better Nutrition, Fewer Chronic Pseudomonas aeruginosa Infections, and Dornase Alfa Use. J. Pediatr. 2008, 153, 752–757. [Google Scholar] [CrossRef]
- Stephenson, A.L.; Mannik, L.A.; Walsh, S.; Brotherwood, M.; Robert, R.; Darling, P.B.; Nisenbaum, R.; Moerman, J.; Stanojevic, S. Longitudinal trends in nutritional status and the relation between lung function and BMI in cystic fibrosis: A population-based cohort study. Am. J. Clin. Nutr. 2013, 97, 872–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayanan, S.; Mainz, J.G.; Gala, S.; Tabori, H.; Grossoehme, D. Adherence to therapies in cystic fibrosis: A targeted literature review. Expert Rev. Respir. Med. 2017, 11, 129–145. [Google Scholar] [CrossRef] [PubMed]
- Madge, S.; Bell, S.C.; Burgel, P.-R.; De Rijcke, K.; Blasi, F.; Elborn, J.S. ERS/ECFS task force: The provision of care for adults with cystic fibrosis in Europe Limitations to providing adult cystic fibrosis care in Europe: Results of a care centre survey. J. Cyst. Fibros. 2017, 16, 85–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skolnik, K.; Quon, B.S. Recent advances in the understanding and management of cystic fibrosis pulmonary exacerbations. F1000Research 2018, 7, Faculty Rev-575. [Google Scholar] [CrossRef] [Green Version]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Johnston, A.; Kelly, S.E.; Hsieh, S.-C.; Skidmore, B.; Wells, G.A. Systematic reviews of clinical practice guidelines: A methodological guide. J. Clin. Epidemiol. 2019, 108, 64–76. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. J. Clin. Epidemiol. 2010, 63, 1308–1311. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kerkvliet, K.; Spithoff, K.; AGREE Next Steps Consortium. The AGREE Reporting Checklist: A tool to improve reporting of clinical practice guidelines. BMJ 2016, 352, i1152. [Google Scholar] [CrossRef] [Green Version]
- Grammatikopoulou, M.G.; Theodoridis, X.; Gkiouras, K.; Stamouli, E.-M.; Mavrantoni, M.-E.; Dardavessis, T.; Bogdanos, D.P. AGREEing on Guidelines for Nutrition Management of Adult Severe Burn Patients. JPEN. J. Parenter. Enteral Nutr. 2019, 43, 490–496. [Google Scholar] [CrossRef]
- Saxby, N.; Painter, C.; Kench, A.; King, S.; Crowder, T.; van der Haak, N.; Australian and New Zealand Cystic Fibrosis Nutrition Guideline Authorship Group. Nutrition Guidelines for Cystic Fibrosis in Australia and New Zealand; CFA: Sydney, Australia; CFNZ: Sydney, Australia; TSANZ: Sydney, Australia, 2017. [Google Scholar]
- Turck, D.; Braegger, C.P.; Colombo, C.; Declercq, D.; Morton, A.; Pancheva, R.; Robberecht, E.; Stern, M.; Strandvik, B.; Wolfe, S.; et al. ESPEN-ESPGHAN-ECFS guidelines on nutrition care for infants, children, and adults with cystic fibrosis. Clin. Nutr. 2016, 35, 557–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinaasappel, M.; Stern, M.; Littlewood, J.; Wolfe, S.; Steinkamp, G.; Heijerman, H.G.M.; Robberecht, E.; Döring, G. Nutrition in patients with cystic fibrosis: A European Consensus. J. Cyst. Fibros. 2002, 1, 51–75. [Google Scholar] [CrossRef] [Green Version]
- Castellani, C.; Duff, A.J.A.; Bell, S.C.; Heijerman, H.G.M.; Munck, A.; Ratjen, F.; Sermet-Gaudelus, I.; Southern, K.W.; Barben, J.; Flume, P.A.; et al. ECFS best practice guidelines: The 2018 revision. J. Cyst. Fibros. 2018, 17, 153–178. [Google Scholar] [CrossRef] [Green Version]
- Hirche, T.O.; Knoop, C.; Hebestreit, H.; Shimmin, D.; Solé, A.; Elborn, J.S.; Ellemunter, H.; Aurora, P.; Hogardt, M.; Wagner, T.O.F.; et al. Practical guidelines: Lung transplantation in patients with cystic fibrosis. Pulm. Med. 2014, 2014, 621342. [Google Scholar] [CrossRef] [Green Version]
- Colombo, C.; Ellemunter, H.; Houwen, R.; Munck, A.; Taylor, C.; Wilschanski, M. Guidelines for the Diagnosis and Management of Distal Intestinal Obstruction Syndrome in Cystic Fibrosis Patients. J. Cyst. Fibros. 2011, 10, S24–S28. [Google Scholar] [CrossRef] [Green Version]
- Sermet-Gaudelus, I.; Mayell, S.J.; Southern, K.W. Guidelines on the early management of infants diagnosed with cystic fibrosis following newborn screening. J. Cyst. Fibros. 2010, 9, 323–329. [Google Scholar] [CrossRef] [Green Version]
- Edenborough, F.P.; Borgo, G.; Knoop, C.; Lannefors, L.; Mackenzie, W.E.; Madge, S.; Morton, A.M.; Oxley, H.C.; Touw, D.J.; Benham, M.; et al. Guidelines for the management of pregnancy in women with cystic fibrosis. J. Cyst. Fibros. 2008, 7, S2–S32. [Google Scholar] [CrossRef] [PubMed]
- Stallings, V.A.; Stark, L.J.; Robinson, K.A.; Feranchak, A.P.; Quinton, H. Clinical Practice Guidelines on Growth and Nutrition Subcommittee; Ad Hoc Working Group Evidence-Based Practice Recommendations for Nutrition-Related Management of Children and Adults with Cystic Fibrosis and Pancreatic Insufficiency: Results of a Systematic Review. J. Am. Diet. Assoc. 2008, 108, 832–839. [Google Scholar] [CrossRef]
- Lahiri, T.; Hempstead, S.E.; Brady, C.; Cannon, C.L.; Clark, K.; Condren, M.E.; Guill, M.F.; Guillerman, R.P.; Leone, C.G.; Maguiness, K.; et al. Clinical Practice Guidelines From the Cystic Fibrosis Foundation for Preschoolers With Cystic Fibrosis. Pediatrics 2016, 137, e20151784. [Google Scholar] [CrossRef] [Green Version]
- Borowitz, D.; Robinson, K.A.; Rosenfeld, M.; Davis, S.D.; Sabadosa, K.A.; Spear, S.L.; Michel, S.H.; Parad, R.B.; White, T.B.; Farrell, P.M.; et al. Cystic Fibrosis Foundation Evidence-Based Guidelines for Management of Infants with Cystic Fibrosis. J. Pediatr. 2009, 155, S73–S93. [Google Scholar] [CrossRef]
- Tangpricha, V.; Kelly, A.; Stephenson, A.; Maguiness, K.; Enders, J.; Robinson, K.A.; Marshall, B.C.; Borowitz, D. Cystic Fibrosis Foundation Vitamin D Evidence-Based Review Committee An update on the screening, diagnosis, management, and treatment of vitamin D deficiency in individuals with cystic fibrosis: Evidence-based recommendations from the Cystic Fibrosis Foundation. J. Clin. Endocrinol. Metab. 2012, 97, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Borowitz, D.S.; Grand, R.J.; Durie, P.R. Use of pancreatic enzyme supplements for patients with cystic fibrosis in the context of fibrosing colonopathy. Consensus Committee. J. Pediatr. 1995, 127, 681–684. [Google Scholar] [CrossRef]
- Schwarzenberg, S.J.; Hempstead, S.E.; McDonald, C.M.; Powers, S.W.; Wooldridge, J.; Blair, S.; Freedman, S.; Harrington, E.; Murphy, P.J.; Palmer, L.; et al. Enteral tube feeding for individuals with cystic fibrosis: Cystic Fibrosis Foundation evidence-informed guidelines. J. Cyst. Fibros. 2016, 15, 724–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cystic Fibrosis Foundation, D.; Borowitz, D.; Parad, R.B.; Sharp, J.K.; Sabadosa, K.A.; Robinson, K.A.; Rock, M.J.; Farrell, P.M.; Sontag, M.K.; Rosenfeld, M.; et al. Cystic Fibrosis Foundation practice guidelines for the management of infants with cystic fibrosis transmembrane conductance regulator-related metabolic syndrome during the first two years of life and beyond. J. Pediatr. 2009, 155, S106–S116. [Google Scholar] [CrossRef]
- Moran, A.; Brunzell, C.; Cohen, R.C.; Katz, M.; Marshall, B.C.; Onady, G.; Robinson, K.A.; Sabadosa, K.A.; Stecenko, A.; Slovis, B.; et al. Clinical care guidelines for cystic fibrosis-related diabetes: A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care 2010, 33, 2697–2708. [Google Scholar] [CrossRef] [Green Version]
- Borowitz, D.; Baker, R.D.; Stallings, V. Consensus report on nutrition for pediatric patients with cystic fibrosis. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 246–259. [Google Scholar] [CrossRef] [Green Version]
- Cystic Fibrosis Trust. Nutritional Management of Cystic Fibrosis; Cystic Fibrosis Trust: London, UK, 2016. [Google Scholar]
- National Institute for Health and Care Excellence (NICE). Cystic Fibrosis: Diagnosis and Management; National Institute for Health and Care Excellence: London, UK, 2017. [Google Scholar]
- Moran, A.; Pillay, K.; Becker, D.J.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2014 Compendium Management of cystic fibrosis-related diabetes in children and adolescents. Pediatr. Diabetes 2014, 65–76. [Google Scholar] [CrossRef]
- Anthony, H.; Collins, C.E.; Davidson, G.; Mews, C.; Robinson, P.; Shepherd, R.; Stapleton, D. Pancreatic enzyme replacement therapy in cystic fibrosis: Australian guidelines. Pediatric Gastroenterological Society and the Dietitians Association of Australia. J. Paediatr. Child Health 1999, 35, 125–129. [Google Scholar] [CrossRef]
- Athanazio, R.A.; da Silva Filho, L.V.R.F.; Vergara, A.A.; Ribeiro, A.F.; Riedi, C.A.; Procianoy, E.; Adde, F.V.; Reis, F.J.C.; Ribeiro, J.D.; Torres, L.A.; et al. Brazilian guidelines for the diagnosis and treatment of cystic fibrosis. J. Bras. Pneumol. 2017, 43, 219–245. [Google Scholar] [CrossRef] [Green Version]
- Declercq, D.; Van Meerhaeghe, S.; Marchand, S.; Van Braeckel, E.; van Daele, S.; De Baets, F.; Van Biervliet, S. The nutritional status in CF: Being certain about the uncertainties. Clin. Nutr. ESPEN 2018, 29, 15–21. [Google Scholar] [CrossRef]
- Simsek, H.; Meseri, R.; Sahin, S.; Ucku, R. Prevalence of food insecurity and malnutrition, factors related to malnutrition in the elderly: A community-based, cross-sectional study from Turkey. Eur. Geriatr. Med. 2013, 4, 226–230. [Google Scholar] [CrossRef]
- Scheuing, N.; Berger, G.; Bergis, D.; Gohlke, B.; Konrad, K.; Laubner, K.; Lilienthal, E.; Moser, C.; Schütz-Fuhrmann, I.; Thon, A.; et al. Adherence to clinical care guidelines for cystic fibrosis-related diabetes in 659 German/Austrian patients. J. Cyst. Fibros. 2014, 13, 730–736. [Google Scholar] [CrossRef] [Green Version]
- Rozga, M.; Handu, D. Nutrition Care for Patients with Cystic Fibrosis: An Evidence Analysis Center Scoping Review. J. Acad. Nutr. Diet. 2019, 119, 137–151.e1. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Eßer, W.; Siering, U.; Neugebauer, E.A.M.; Brockhaus, A.C.; Lampert, U.; Eikermann, M. Guideline appraisal with AGREE II: Systematic review of the current evidence on how users handle the 2 overall assessments. PLoS ONE 2017, 12, e0174831. [Google Scholar] [CrossRef]
- Bero, L. Developing reliable dietary guidelines. BMJ 2017, 359, j4845. [Google Scholar] [CrossRef]
- Gené-Badia, J.; Gallo, P.; Caïs, J.; Sánchez, E.; Carrion, C.; Arroyo, L.; Aymerich, M. The use of clinical practice guidelines in primary care: Professional mindlines and control mechanisms. Gac. Sanit. 2016, 30, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, J.-L.; Chen, R.-F. Critical factors influencing physicians’ intention to use computerized clinical practice guidelines: An integrative model of activity theory and the technology acceptance model. BMC Med. Inform. Decis. Mak. 2016, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, E. Status of practice guidelines in the United States: CDC guidelines as an example. Prev. Med. 2003, 36, 519–524. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Forouhi, N.G. Dietary guidelines and health—is nutrition science up to the task? BMJ 2018, 360, k822. [Google Scholar] [CrossRef] [Green Version]
- Hollander, F.M.; de Roos, N.M.; Heijerman, H.G.M. The optimal approach to nutrition and cystic fibrosis. Curr. Opin. Pulm. Med. 2017, 23, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Poulimeneas, D.; Grammatikopoulou, M.G.; Petrocheilou, A.; Kaditis, A.G.; Vassilakou, T. Triage for Malnutrition Risk among Pediatric and Adolescent Outpatients with Cystic Fibrosis, Using a Disease-Specific Tool. Children 2020, 7, 269. [Google Scholar] [CrossRef] [PubMed]
- Poulimeneas, D.; Grammatikopoulou, M.G.; Devetzi, P.; Petrocheilou, A.; Kaditis, A.G.; Papamitsou, T.; Doudounakis, S.E.; Vassilakou, T. Adherence to dietary recommendations, nutrient intake adequacy and diet quality among pediatric cystic fibrosis patients: Results from the Greecf study. Nutrients 2020, 12, 3126. [Google Scholar] [CrossRef] [PubMed]
- Sainath, N.N.; Schall, J.; Bertolaso, C.; McAnlis, C.; Stallings, V.A. Italian and North American dietary intake after ivacaftor treatment for Cystic Fibrosis Gating Mutations. J. Cyst. Fibros. 2019, 18, 135–143. [Google Scholar] [CrossRef]
- Sutherland, R.; Katz, T.; Liu, V.; Quintano, J.; Brunner, R.; Tong, C.W.; Collins, C.E.; Ooi, C.Y. Dietary intake of energy-dense, nutrient-poor and nutrient-dense food sources in children with cystic fibrosis. J. Cyst. Fibros. 2018, 17, 804–810. [Google Scholar] [CrossRef]
- Lonabaugh, K.P.; O’Neal, K.S.; McIntosh, H.; Condren, M. Cystic fibrosis-related education: Are we meeting patient and caregiver expectations? Patient Educ. Couns. 2018, 101, 1865–1870. [Google Scholar] [CrossRef]
- Watson, H.; Bilton, D.; Truby, H. A Randomized Controlled Trial of a New Behavioral Home-Based Nutrition Education Program, “Eat Well with CF,” in Adults with Cystic Fibrosis. J. Am. Diet. Assoc. 2008, 108, 847–852. [Google Scholar] [CrossRef]
- Janicke, D.M.; Mitchell, M.J.; Quittner, A.L.; Piazza-Waggoner, C.; Stark, L.J. The Impact of Behavioral Intervention on Family Interactions at Mealtime in Pediatric Cystic Fibrosis. Child. Health Care 2008, 37, 49–66. [Google Scholar] [CrossRef]
- Singh, S.B.; Shelton, A.U.; Greenberg, B.; Starner, T.D. Implementation of cystic fibrosis clinical pathways improved physician adherence to care guidelines. Pediatr. Pulmonol. 2017, 52, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Ruseckaite, R.; Pekin, N.; King, S.; Carr, E.; Ahern, S.; Oldroyd, J.; Earnest, A.; Wainwright, C.; Armstrong, D. Evaluating the impact of 2006 Australasian Clinical Practice Guidelines for nutrition in children with cystic fibrosis in Australia. Respir. Med. 2018, 142, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Savant, A.P.; Britton, L.J.; Petren, K.; McColley, S.A.; Gutierrez, H.H. Sustained improvement in nutritional outcomes at two paediatric cystic fibrosis centres after quality improvement collaboratives. BMJ Qual. Saf. 2014, 23, i81–i89. [Google Scholar] [CrossRef] [PubMed]
- Garber, E.; Desai, M.; Zhou, J.; Alba, L.; Angst, D.; Cabana, M.; Saiman, L. CF Infection Control Study Consortium Barriers to adherence to cystic fibrosis infection control guidelines. Pediatr. Pulmonol. 2008, 43, 900–907. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICAR Acronym Criteria | PICAR Items Relevant to Screening CPGs for Inclusion |
|---|---|
| (P) Population | Patients with Cystic fibrosis, throughout the lifespan. |
| (I) Intervention | Any dietary intervention or MNT for patients with cystic fibrosis (i.e., micronutrient supplementation, provision of energy or macronutrient intake, management of lung transplantation, management of CFRD, etc.). |
| (C) Comparators, Comparison, and ‘key’ content | Any comparator or comparison. No ‘key’ CPG content is of interest. |
| (A) Attributes of the CPGs | Eligible CPGs were: (1) CPGs, Practice, or Consensus Papers, (2) published in the English language, (3) in full-text format, (4) until August 2018, (5) from professional or governmental organizations, with (6) nutrition-related recommendations, (7) intended for health professionals, (8) without any limitation in their quality based on the AGREE II. |
| (R) Recommendation characteristics and other considerations | Not applicable. |
| Advising Body | Year | Origin | Aim | Age Group | Organization | Total Pages | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CF Care with Nutritional Advice | CF MNT | Management of CF Issues, Including Nutritional Care | Infants | Children/Adolescents | Adults | Professional | State | ||||
| ADA/CFF/PES [37] | 2010 | US | CFRD | √ | √ | √ | 12 | ||||
| CFF [34] | 1995 | US | √ | PERT | √ | √ | √ | √ | 4 | ||
| CFF [30] | 2008 | US | √ | √ | √ | √ | 8 | ||||
| CFF [32] | 2009 | US | √ | √ | √ | 21 | |||||
| CFF [36] | 2009 | US | CFTR-Related MS | √ | √ | √ | √ | 22 | |||
| CFF [33] | 2012 | US | Vitamin D deficiency | √ | √ | √ | √ | 12 | |||
| CFF [31] | 2016 | US | √ | √ | √ | 28 | |||||
| CFF [35] | 2016 | US | √ | EN feeding | √ | √ | √ | 12 | |||
| CFF/NASPGHAN [38] | 2002 | US | √ | √ | √ | 14 | |||||
| CFT [39] | 2016 | UK | √ | √ | √ | √ | √ | 60 | |||
| ECFS [24] | 2002 | EU | √ | √ | √ | √ | √ | 25 | |||
| ECFS [29] | 2008 | EU | √ | Pregnancy | √ | √ | 31 | ||||
| ECFS [28] | 2010 | EU | √ | √ | √ | 7 | |||||
| ECFS [27] | 2011 | EU | DIOS | √ | √ | √ | 5 | ||||
| ECFS [26] | 2014 | EU | √ | LTX | √ | √ | √ | 22 | |||
| ECFS [25] | 2018 | EU | √ | √ | √ | √ | √ | 26 | |||
| ESPEN/ESPGHAN/ECFS [23] | 2016 | EU | √ | √ | √ | √ | √ | 21 | |||
| ISPAD [41] | 2018 | International | √ | CFRD | √ | √ | 11 | ||||
| NICE [40] | 2017 | UK | √ | √ | √ | √ | √ | 768 | |||
| PGS/DAA [42] | 1999 | AU | √ | √ | √ | √ | √ | 5 | |||
| SBPT [43] | 2017 | BR | √ | √ | √ | √ | √ | 27 | |||
| TSANZ [22] | 2017 | AU & NZ | √ | √ | √ | √ | √ | 284 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grammatikopoulou, M.G.; Vassilakou, T.; Goulis, D.G.; Theodoridis, X.; Nigdelis, M.P.; Petalidou, A.; Gkiouras, K.; Poulimeneas, D.; Alexatou, O.; Tsiroukidou, K.; et al. Standards of Nutritional Care for Patients with Cystic Fibrosis: A Methodological Primer and AGREE II Analysis of Guidelines. Children 2021, 8, 1180. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121180
Grammatikopoulou MG, Vassilakou T, Goulis DG, Theodoridis X, Nigdelis MP, Petalidou A, Gkiouras K, Poulimeneas D, Alexatou O, Tsiroukidou K, et al. Standards of Nutritional Care for Patients with Cystic Fibrosis: A Methodological Primer and AGREE II Analysis of Guidelines. Children. 2021; 8(12):1180. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121180
Chicago/Turabian StyleGrammatikopoulou, Maria G., Tonia Vassilakou, Dimitrios G. Goulis, Xenophon Theodoridis, Meletios P. Nigdelis, Arianna Petalidou, Konstantinos Gkiouras, Dimitrios Poulimeneas, Olga Alexatou, Kyriaki Tsiroukidou, and et al. 2021. "Standards of Nutritional Care for Patients with Cystic Fibrosis: A Methodological Primer and AGREE II Analysis of Guidelines" Children 8, no. 12: 1180. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121180