
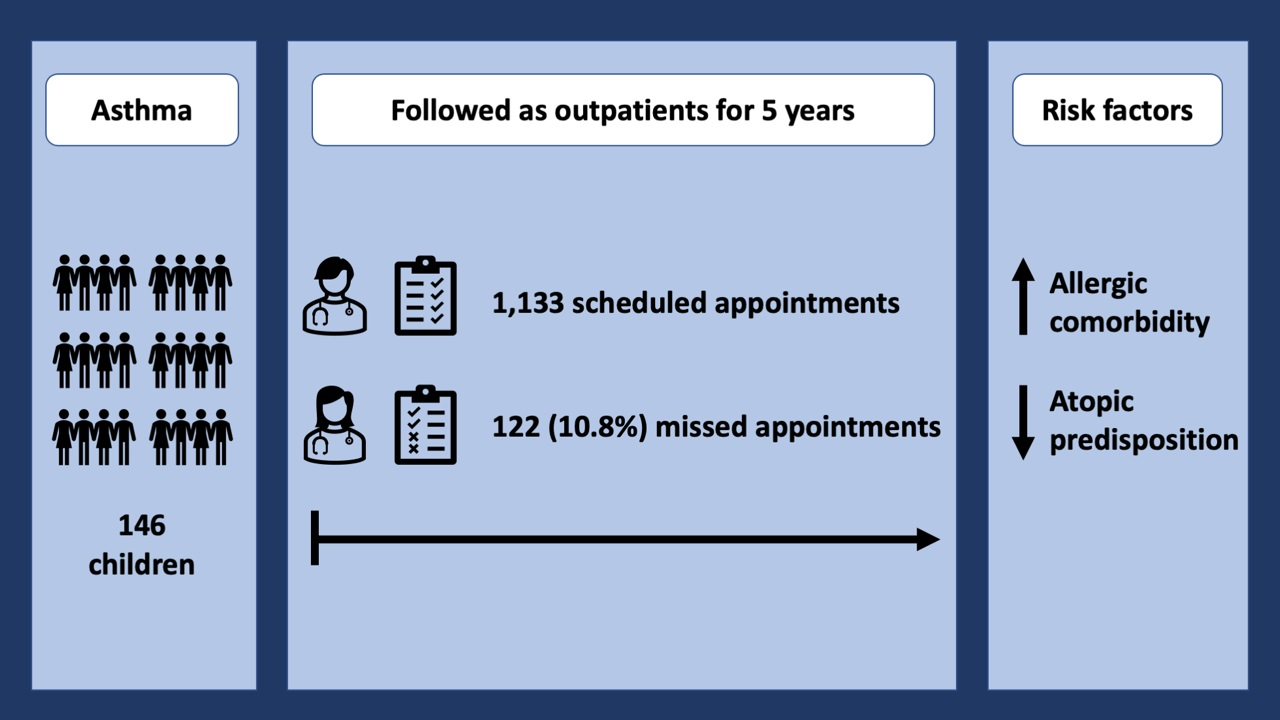
Allergic Comorbidity Is a Risk Factor for Not Attending Scheduled Outpatient Visits in Children with Asthma


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Assessment of Non-Attendance of Scheduled Outpatient Visits
2.3. Risk Factors of Non-Attendance
2.4. Loss of Asthma Control Measures
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Risk Factors for Non-Attendance of Scheduled Appointments
3.3. Non-Attendance, Treatment Adherence and Loss of Asthma Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Baseline Characteristic | Included (n = 146) | Excluded (n = 9) | p |
|---|---|---|---|
| Sex, n (%) | p = 1 | ||
| Male | 85 (0.58) | 5 (0.56) | |
| Female | 61 (0.42) | 4 (0.44) | |
| Ethnicity, n (%) | p = 0.25 | ||
| Caucasian | 109 (0.75) | 5 (0.55) | |
| Non-Caucasian | 37 (0.25) | 4 (0.44) | |
| Age, years, mean (SD) | 12.25 (2.51) | 12.70 (2.60) | p = 0.63 |
| BMI, WHO z-score, mean (SD) | 0.056 (1.05) | −0.63 (1.11) | p = 0.10 |
| Comorbidity, n (%) | |||
| Any allergic sensitization, no | 42 (0.27) | 7 (0.78) | p = 0.005 |
| Any allergic sensitization, yes | 104 (0.67) | 2 (0.22) | |
| Allergic rhinitis, no | 52 (0.36) | 7 (0.78) | p = 0.027 |
| Allergic rhinitis, yes | 94 (0.64) | 2 (0.22) | |
| House dust mite allergic sensitization, no | 85 (0.58) | 8 (0.89) | p = 0.086 |
| House dust mite allergic sensitization, yes | 61 (0.42) | 1 (0.11) | |
| Cat/dog/horse allergic sensitization, no | 80 (0.55) | 8 (0.89) | p = 0.079 |
| Cat/dog/horse allergic sensitization, yes | 66 (0.45) | 1 (0.11) | |
| Pollen allergic sensitization, no | 62 (0.43) | 7 (0.77) | p = 0.079 |
| Pollen allergic sensitization, yes | 84 (0.57) | 2 (0.22) | |
| Eczema, no | 91 (0.64) | 8 (0.89) | p = 0.17 |
| Eczema, yes | 51 (0.36) | 1 (0.11) | |
| Food allergy, no | 127 (0.88) | 9 (1.0) | p = 0.60 |
| Food allergy, yes | 17 (0.12) | 0 (0) | |
| Lung function, mean (SD) | |||
| FEV1% predicted | 90.19 (11.22) | 93.21 (11.18) | p = 0.45 |
| FEV1/FVC-ratio | 82.27 (0.96) | 80.76 (1.09) | p = 0.67 |
| FeNO, ppb | 22.34 (20.77) | 17.89 (18.59) | p = 0.51 |
| GINA step at baseline, median (IQR) | 2 (2) | 2 (1.25) | p = 0.43 |
| Exercise challenge test result, n (%) | p = 1 | ||
| Negative | 74 (0.63) | 3 (0.60) | |
| Positive | 43 (0.37) | 2 (0.40) | |
| Regular physical activity, n (%) | p = 1 | ||
| No | 19 (0.15) | 1 (0.14) | |
| Yes | 110 (0.85) | 6 (0.86) | |
| Asthma in 1st degree relative, n (%) | p = 0.73 | ||
| No | 70 (0.56) | 6 (0.67) | |
| Yes | 56 (0.44) | 3 (0.33) | |
| Allergy in 1st degree relative, n (%) | p = 0.73 | ||
| No | 54 (0.44) | 5 (0.56) | |
| Yes | 70 (0.56) | 4 (0.44) | |
| Eczema in 1st degree relative, n (%) | p = 1 | ||
| No | 96 (0.78) | 7 (0.78) | |
| Yes | 27 (0.22) | 2 (0.22) | |
| Adherence, PDC > 80%, n (%) | p = 0.50 | ||
| No | 48 (0.53) | 2 (1.0) | |
| Yes | 42 (0.47) | 0 (0) |
References
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef] [PubMed]
- McGovern, C.M.; Redmond, M.; Arcoleo, K.; Stukus, D.R. A missed primary care appointment correlates with a subsequent emergency department visit among children with asthma. J. Asthma 2017, 54, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.E.; Tang, M.; Zhao, C.; Hurst, J.; Wu, A.; Goldstein, B.A. Well-Child Care Attendance and Risk of Asthma Exacerbations. Pediatrics 2020, 146, e20201023. [Google Scholar] [CrossRef]
- Anderson, H.; Gupta, R.; Kapetanakis, V.; Asher, M.; Clayton, T.; Robertson, C.; Strachan, D. International correlations between indicators of prevalence, hospital admissions and mortality for asthma in children. Int. J. Epidemiol. 2008, 37, 573–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furtado, P.R.; Maciel, Á.C.C.; Barbosa, R.R.T.; Silva, A.A.M.d.; Freitas, D.A.d.; Mendonça, K.M.P.P.d. Association between quality of life, severity of asthma, sleep disorders and exercise capacity in children with asthma: A cross-sectional study. Brazil. J. Phys. Ther. 2019, 23, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.R.; Wakefield, D.B.; Cloutier, M.M. Relationship between pediatric primary provider visits and acute asthma ED visits. Pediatr. Pulmonol. 2007, 42, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Hauerslev, M.; Garpvall, K.; Marckmann, M.; Hermansen, M.N.; Hansen, K.S.; Chawes, B.L. Long-term predictors of loss of asthma control in school-aged well-controlled children with mild to moderate asthma: A 5-year follow-up. Pediatr. Pulmonol. 2021, 57, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Marckmann, M.; Hermansen, M.N.; Hansen, K.S.; Chawes, B.L. Assessment of adherence to asthma controllers in children and adolescents. Pediatr. Allerg. Immunol. 2020, 31, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.; Levy, M. A Pocket Guide for Health Professionals. Available online: https://www.ginasthma.org (accessed on 2 November 2021).
- Wolf, E.R.; Hochheimer, C.J.; Sabo, R.T.; DeVoe, J.; Wasserman, R.; Geissal, E.; Opel, D.J.; Warren, N.; Puro, J.; O’Neil, J.; et al. Gaps in Well-Child Care Attendance Among Primary Care Clinics Serving Low-Income Families. Pediatrics 2018, 142, e20174019. [Google Scholar] [CrossRef] [Green Version]
- Selden, T.M. Compliance with well-child visit recommendations: Evidence from the Medical Expenditure Panel Survey, 2000–2002. Pediatrics 2006, 118, e1766–e1778. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Int. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Kluthe, C.; Tsui, J.; Spady, D.; Carroll, M.; Wine, E.; Huynh, H.Q. The Frequency of Clinic Visits Was Not Associated with Medication Adherence or Outcome in Children with Inflammatory Bowel Diseases. Can. J. Gastroenterol. Hepatol. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, J.T.; Volkening, L.K.; Laffel, L.M.B. Care Utilization in a Pediatric Diabetes Clinic: Cancellations, Parental Attendance, and Mental Health Appointments. J. Pediatr. 2014, 164, 1384–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Just, J.; Saint-Pierre, P.; Gouvis-Echraghi, R.; Laoudi, Y.; Roufai, L.; Momas, I.; Annesi Maesano, I. Childhood allergic asthma is not a single phenotype. J. Pediatr. 2014, 164, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Just, J.; Saint Pierre, P.; Amat, F.; Gouvis-Echraghi, R.; Lambert-Guillemot, N.; Guiddir, T.; Annesi Maesano, I. What lessons can be learned about asthma phenotypes in children from cohort studies? Pediatr. Allerg. Immunol. Off. Publ. Eur. Soc. Pediatr. Allerg. Immunol. 2015, 26, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, C.C.; Rubin, D.M.; Zorc, J.J.; Mohamad, Z.; Faerber, J.A.; Feudtner, C. Childhood Asthma Hospital Discharge Medication Fills and Risk of Subsequent Readmission. J. Pediatr. 2015, 166, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Utidjian, L.H.; Fiks, A.G.; Localio, A.R. Pediatric asthma hospitalizations among urban minority children and the continuity of primary care. J. Asthma Off. J. Assoc. Care Asthma 2017, 54, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Brandão, H.V.; Cruz, C.S.; Guimarães, A.; Camargos, A.; Cruz, Á.A. Predictors of hospital admission due to asthma in children and adolescents enrolled in an asthma control program. J. Brasil. Pneumol. 2010, 36, 700–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardura-Garcia, C.; Arias, E.; Hurtado, P.; Bonnett, L.J.; Sandoval, C.; Maldonado, A.; Workman, L.J.; Platts-Mills, T.A.E.; Cooper, P.J.; Blakey, J.D. Predictors of severe asthma attack re-attendance in Ecuadorian children: A cohort study. Eur. Respir. J. 2019, 54, 1802419. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.M.; Grunwell, J.R.; Bruce, A.C.; Smith, R.C.; Fitzpatrick, A.M. Predictors of emergency department use in children with persistent asthma in metropolitan Atlanta, Georgia. Ann. Allerg. Asthma Immunol. 2017, 119, 129–136. [Google Scholar] [CrossRef] [PubMed]
| Baseline Characteristic | Missing Data | All Children (n = 146) | Children Attending All Scheduled Visits (n = 79) | Children not Attending ≥1 Scheduled Visits (n = 67) |
|---|---|---|---|---|
| Gender, male, n (%) | 0 | 85 (58%) | 44 (56%) | 41 (61%) |
| Caucasian, n (%) | 0 | 109 (75%) | 59 (75%) | 50 (75%) |
| Age, years, mean (SD) | 0 | 12.3 (2.5) | 12.1 (2.5) | 12.5 (2.5) |
| BMI, WHO z-score, mean (SD) | 1 | 0.06 (1.05) | 0.02 (1.02) | 0.1 (1.09) |
| Physically active, n (%) | 17 | 110 (85%) | 58 (85%) | 52 (85%) |
| GINA treatment step, baseline, median (IQR) | 4 | 2 (1–3) | 2 (1–3) | 2 (1–3) |
| Adherence, PDC > 80%, n (%) | 56 | 42 (47%) | 22 (51%) | 20 (42%) |
| Rhinitis, n (%) | 0 | 94 (64%) | 44 (56%) | 50 (75%) |
| Eczema, n (%) | 4 | 51 (36%) | 28 (37%) | 23 (35%) |
| Sensitization, any, n (%) | 0 | 104 (71%) | 47 (59%) | 57 (85%) |
| Sensitization, house dust mites, n (%) | 0 | 61 (42%) | 25 (32%) | 36 (54%) |
| Sensitization, furred animals, n (%) | 0 | 66 (45%) | 30 (38%) | 36 (54%) |
| Sensitization, pollen, n (%) | 0 | 84 (56%) | 38 (48%) | 46 (69%) |
| Food allergy, n (%) | 2 | 17 (12%) | 11 (14%) | 6 (9%) |
| Asthma predisposition, n (%) | 19 | 58 (46%) | 33 (49%) | 25 (42%) |
| Allergy predisposition, n (%) | 22 | 70 (56%) | 35 (52%) | 35 (61%) |
| Eczema predisposition, n (%) | 23 | 26 (21%) | 18 (27%) | 8 (14%) |
| FEV1%-predicted, baseline, mean (SD) | 0 | 88.6 (11.4) | 89.2 (10.4) | 87.8 (12,5) |
| FEV1/FVC-ratio, mean (SD) | 0 | 82.1 (7.3) | 82.4 (7.2) | 81.7 (7.5) |
| FeNO, ppb, median (IQR) | 6 | 15.5 (10–27) | 14 (9–27) | 18 (12–28) |
| Positive exercise challenge test, n (%) | 0 | 42 (28%) | 27 (34%) | 15 (22%) |
| Risk Factor | Not Attending ≥1 vs. Attending All Scheduled Apointments | |||||
|---|---|---|---|---|---|---|
| Unadjusted Analysis | Adjusted for No. of Scheduled Visits | |||||
| OR | 95% CI | p | aOR | 95% CI | p | |
| Sex (male vs. female) | 0.80 | 0.41–1.54 | 0.50 | 0.82 | 0.42–1.61 | 0.57 |
| Caucasian (yes vs. no) | 1.00 | 0.47–2.12 | 0.99 | 1.11 | 0.51–2.38 | 0.79 |
| Physically active (yes vs. no) | 0.99 | 0.37–2.69 | 0.99 | 1.06 | 0.39–2.92 | 0.90 |
| Rhinitis (yes vs. no) | 2.34 | 1.17–4.82 | 0.02 | 2.21 | 1.09–4.60 | 0.03 |
| Eczema (yes vs. no) | 0.92 | 0.46–1.82 | 0.80 | 0.93 | 0.46–1.87 | 0.84 |
| Sensitization, any (yes vs. no) | 3.88 | 1.78–9.07 | 0.0005 | 3.65 | 1.66–8.61 | 0.002 |
| Sensitization, house dust mites (yes/no) | 2.51 | 1.29–4.98 | 0.007 | 2.38 | 1.21–4.77 | 0.01 |
| Sensitization, furred animals (yes vs. no) | 1.90 | 0.98–3.70 | 0.06 | 1.83 | 0.94–3.62 | 0.08 |
| Sensitization, pollen (yes vs. no) | 2.36 | 1.21–4.72 | 0.01 | 2.19 | 1.11–4.41 | 0.03 |
| Food allergy (yes vs. no) | 0.61 | 0.20–1.70 | 0.36 | 0.64 | 0.21–1.80 | 0.41 |
| Asthma predisposition (yes vs. no) | 0.80 | 39–1.62 | 0.54 | 0.81 | 0.40–1.67 | 0.58 |
| Allergy predisposition (yes vs. no) | 1.45 | 0.71–3.00 | 0.31 | 1.43 | 0.69–3.00 | 0.33 |
| Eczema predisposition (yes vs. no) | 0.44 | 0.16–1.07 | 0.08 | 0.39 | 0.14–0.99 | 0.06 |
| Positive exercise challenge (yes vs. no) | 0.56 | 0.25–1.20 | 0.14 | 0.54 | 0.24–1.19 | 0.13 |
| Age (years) | 1.07 | 0.94–1.22 | 0.34 | 1.07 | 0.94–1.23 | 0.31 |
| BMI (WHO z-score) | 1.10 | 0.81–1.50 | 0.55 | 1.10 | 0.80–1.50 | 0.56 |
| GINA baseline step (1, 2, 3, 4–5) | 1.12 | 0.80–1.57 | 0.51 | 1.12 | 0.80–1.59 | 0.52 |
| FEV1 baseline (%-predicted) | 0.34 | 0.02–6.11 | 0.46 | 0.34 | 0.02–6.46 | 0.47 |
| FEV1/FVC baseline ratio | 0.30 | 0.003–27.25 | 0.60 | 0.30 | 0.0029–29.35 | 0.94 |
| Reversibility (%-change in FEV1) | 0.99 | 0.95–1.02 | 0.44 | 0.99 | 0.95–1.02 | 0.45 |
| FeNO baseline (ppb) | 1.01 | 0.99–1.03 | 0.31 | 1.01 | 0.99–1.03 | 0.30 |
| Log 2(FeNO baseline (ppb)) | 1.22 | 0.90–1.68 | 0.20 | 1.23 | 0.90–1.70 | 0.19 |
| Risk Factor | Not Attending Scheduled Outpatient Apointments | |||||
|---|---|---|---|---|---|---|
| Unadjusted Analysis | Adjusted for No. of Scheduled Visits | |||||
| OR | 95% CI | p | aOR | 95% CI | p | |
| Rhinitis (yes vs. no) | 0.52 | 0.12–1.84 | 0.33 | 0.51 | 0.12–1.82 | 0.32 |
| Sensitization, any (yes vs. no) | 6.60 | 1.30–39.42 | 0.03 | 6.61 | 1.30–39.65 | 0.03 |
| Sensitization, house dust mites (yes vs. no) | 1.11 | 0.42–2.96 | 0.83 | 1.12 | 0.42–2.99 | 0.82 |
| Sensitization, furred animals (yes vs. no) | 1.29 | 0,49–3.44 | 0.60 | 1.29 | 0.49–3.44 | 0.60 |
| Sensitization, pollen (yes vs. no) | 0.89 | 0.23–2.94 | 0.84 | 0.90 | 0.25–3.00 | 0.86 |
| Eczema predisposition (yes vs. no) | 0.35 | 0.13–0.92 | 0.04 | 0.36 | 0.13–0.92 | 0.04 |
| Endpoint | Not Attending ≥1 vs. Attending All Scheduled Apointments | |||||
|---|---|---|---|---|---|---|
| Unadjusted Analysis | Adjusted for No. of Scheduled Visits | |||||
| OR | 95% CI | p | aOR | 95% CI | p | |
| Adherence, PDC > 80% (yes vs. no) | 0.70 | 0.30–1.60 | 0.40 | 0.61 | 0.25–1.43 | 0.26 |
| ß-coefficient | 95% CI | p | aß-coefficient | 95% CI | p | |
| GINA treatment step-up (No. of steps) | 0.92 | 0.75–1.11 | 0.46 | 0.85 | 0.68–1.03 | 0.14 |
| IRR | 95% CI | p | aIRR | 95% CI | p | |
| Admissions (total No.) | 1.04 | 0.51–1.60 | 0.89 | 0.92 | 0.45–1.45 | 0.78 |
| Exacerbations (total No.) | 0.97 | 0.63–1.32 | 0.86 | 0.86 | 0.55–1.19 | 0.43 |
| OCS courses (total No.) | 1.17 | 0.68–1.69 | 0.48 | 1.09 | 0.63–1.59 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garpvall, K.; Hauerslev, M.; Marckmann, M.; Hermansen, M.N.; Hansen, K.S.; Chawes, B.L. Allergic Comorbidity Is a Risk Factor for Not Attending Scheduled Outpatient Visits in Children with Asthma. Children 2021, 8, 1193. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121193
Garpvall K, Hauerslev M, Marckmann M, Hermansen MN, Hansen KS, Chawes BL. Allergic Comorbidity Is a Risk Factor for Not Attending Scheduled Outpatient Visits in Children with Asthma. Children. 2021; 8(12):1193. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121193
Chicago/Turabian StyleGarpvall, Kalle, Marie Hauerslev, Mads Marckmann, Mette N. Hermansen, Kirsten S. Hansen, and Bo L. Chawes. 2021. "Allergic Comorbidity Is a Risk Factor for Not Attending Scheduled Outpatient Visits in Children with Asthma" Children 8, no. 12: 1193. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121193