
Association between CCC-2 and Structural Language, Pragmatics, Social Cognition, and Executive Functions in Children with Developmental Language Disorder




Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.1.1. DLD Group
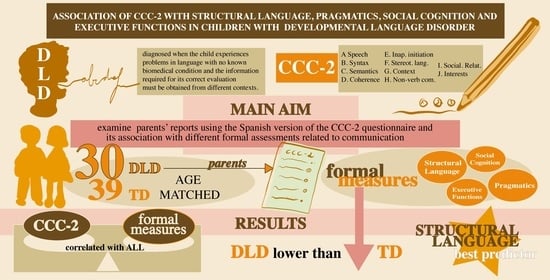
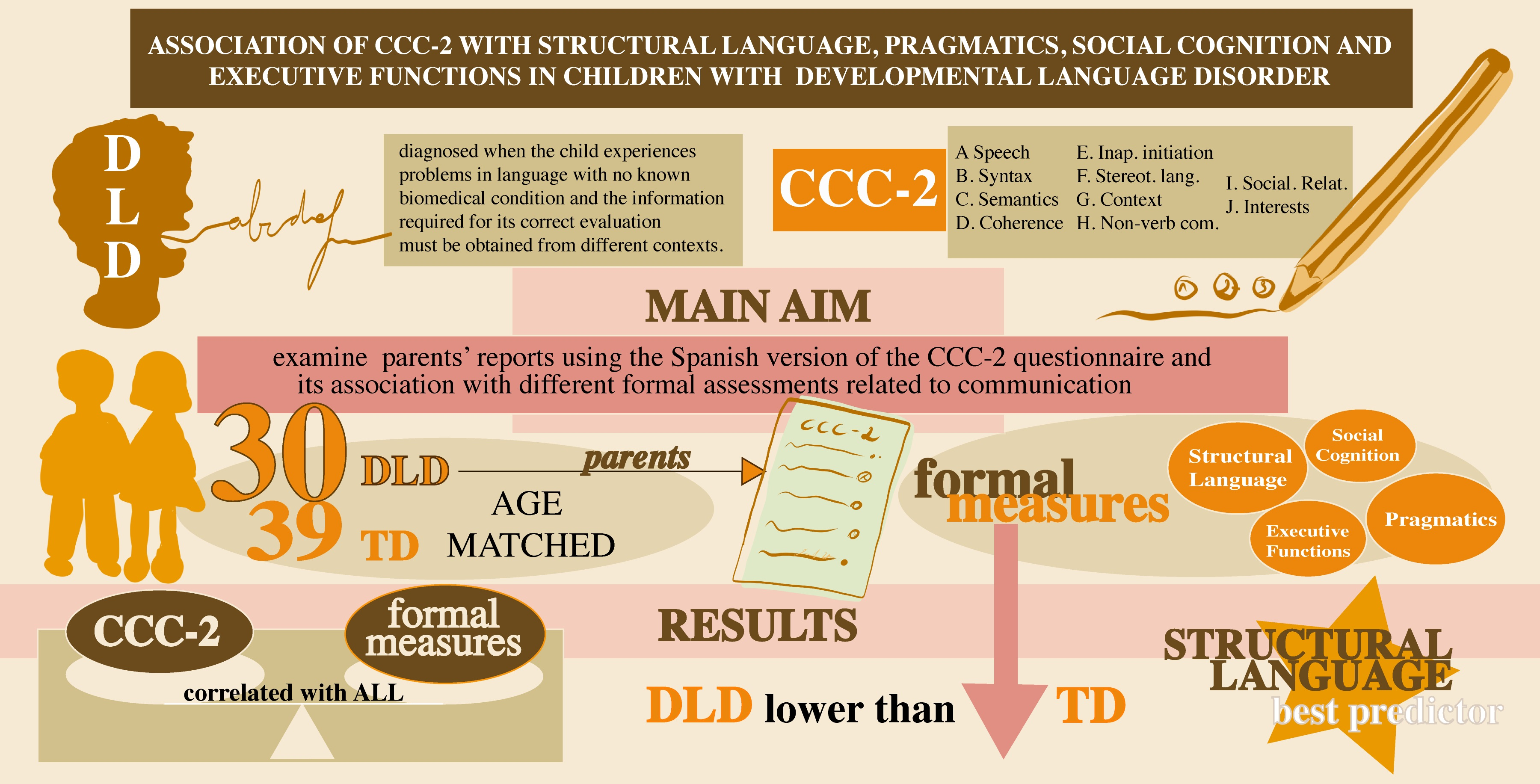
- Diagnosis of DLD: Children with DLD had an updated diagnosis by a qualified educational psychologist from the ordinary schools where the sample was recruited. All these psychologists from the different schools belonged to the same local health services, and so they followed the same diagnostic protocols, thereby ensuring that the criteria used for all these diagnoses were homogeneous. In this regard, their records confirmed that the children had substantial language disability as the main cause for receiving speech and language therapy, while presenting a typical nonverbal intelligence based on standardized language and cognitive tests. Moreover, participants were recruited for the DLD group if they were native speakers of Spanish receiving speech and language therapy in the school at the time of the study; had language difficulties (discarding possible auditory disorders, neuro-sensory and intellectual disability); and finally, their clinical record had to be free of any medical condition that was likely to affect language, such as a diagnosis of ASD. Additionally, DLD condition was confirmed by the research group. The research team assessed each selected participant using two standardized grammar measures: on the one hand, Comprensión de Estructuras Gramaticales [62], and on the other hand, a Memory subtest on the Evaluación del Lenguaje Infantil, which is a sentence repetition task that measures expressive language ability and short-term auditory memory (ELI; [63]), both of which have been reported as a valid formal measure in the diagnosis of DLD (e.g., [64]). Participants were recruited only if they scored one standard deviation below the mean in at least one of these two tests. This threshold has been used in similar papers to conduct in-depth studies in children with DLD [52]. Moreover, Raven’s Progressive Matrices revised version [65] was used to ensure that the children’s IQ was within the normal range (above the 15th percentile). In this sense, the DLD group obtained a mean of 28.57 (SD = 72.04, range = 25–99).
2.1.2. Chronological Age-Matched (AM) Group
2.2. Measures
2.2.1. Parent Reports
Children’s Communication Checklist (CCC-2)
2.2.2. Formal measures
- Non-verbal reasoning
- Structural language
- Pragmatics
- Social cognition
- Executive Functions
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics and between-Group Comparisons on Formal Measures
3.2. Descriptive Statistics on CCC-2
3.3. Correlations between CCC-2 Scores and Age, Structural Language, Linguistic Pragmatics, Social Pragmatics and Executive Functions
3.4. Predictive Analysis of the CCC-2 Scores of Structural Language, Pragmatics and Autistic Indexes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bishop, D.V.M.; Snowling, M.J.; Thompson, P.A.; Greenhalgh, T. Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J. Child Psychol. Psychiatry 2017, 58, 1068–1080. [Google Scholar] [CrossRef]
- Davies, C.; Andrés-Roqueta, C.; Norbury, C.F. Referring expressions and structural language abilities in children with specific language impairment: A pragmatic tolerance account. J. Exp. Child Psychol. 2016, 144, 98–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norbury, C.F.; Nash, M.; Baird, G.; Bishop, D.V. Using a parental checklist to identify diagnostic groups in children with communication impairment: A validation of the Children’s Communication Checklist–2. Int. J. Lang. Commun. Disord. 2004, 39, 345–364. [Google Scholar] [CrossRef] [PubMed]
- Dockrell, J.E.; Lindsay, G.; Palikara, O. Explaining the academic achievement at school leaving for pupils with a history of language impairment: Previous academic achievement and literacy skills. Child Lang. Teach. Ther. 2011, 27. [Google Scholar] [CrossRef]
- Durkin, K.; Toseeb, U.; Botting, N.; Pickles, A.; Conti-Ramsden, G. Social confidence in early adulthood among young people with and without a history of language impairment. J. Speech Lang. Hear. Res. 2017, 60, 1635–1647. [Google Scholar] [CrossRef]
- Snowling, M.J.; Duff, F.J.; Nash, H.M.; Hulme, C. Language profiles and literacy outcomes of children with resolving, emerging, or persisting language impairments. J. Child Psychol. Psychiatry 2016, 57, 1360–1369. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Norbury, C.F. Exploring the borderlands of autistic disorder and specific language impairment: A study using standardised diagnostic instruments. J. Child Psychol. Psychiatry 2002, 43, 917–929. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Botting, N. Emotional health in adolescents with and without a history of specific language impairment (SLI). J. Child Psychol. Psychiatry 2008, 49, 516–525. [Google Scholar] [CrossRef]
- Kilpatrick, T.; Leitão, S.; Boyes, M. Mental health in adolescents with a history of developmental language disorder: The moderating effect of bullying victimisation. Autism Dev. Lang. Impair. 2019, 4. [Google Scholar] [CrossRef]
- Lindsay, G.; Dockrell, J.E. Longitudinal patterns of behavioral, emotional, and social difficulties and self-concepts in adolescents with a history of specific language impairment. Lang. Speech Hear. Serv. Sch. 2012, 43, 445–460. [Google Scholar] [CrossRef]
- Snowling, M.J.; Bishop, D.V.; Stothard, S.E.; Chipchase, B.; Kaplan, C. Psychosocial outcomes at 15 years of children with a preschool history of speech-language impairment. J. Child Psychol. Psychiatry 2006, 47, 759–765. [Google Scholar] [CrossRef] [PubMed]
- van den Bedem, N.P.; Dockrell, J.E.; van Alphen, P.M.; Kalicharan, S.V.; Rieffe, C. Victimization, Bullying, and Emotional Competence: Longitudinal Associations in (Pre)Adolescents With and Without Developmental Language Disorder. J. Speech Lang. Hear. Res. 2018, 61, 2028–2044. [Google Scholar] [CrossRef]
- Amador, J.A.; Forns, M.; Guàrdia, J.; Peró, M. Estructura factorial y datos descriptivos del perfil de atención y del cuestionario TDAH para niños en edad escolar [Factor structure and descriptive data from the Attention Profile and the ADHD Questionnaire for school-age children]. Psicothema 2006, 18, 696–703. [Google Scholar]
- Zhang, Y.; Xu, X.; Jiang, Y.; Sun, W.; Wang, Y.; Song, Y.; Dong, S.; Zhu, Q.; Jiang, F.; Sheng, L. Early language and communication development in Chinese children: Adaptation and validation of a parent report instrument. Int. J. Speech Lang. Pathol. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Thudge, J.; Hogan, D. An ecological approach to observations of children’s everyday lives. In Researching Children’s Experience: Approaches and Methods; Greene, S., Hogan, D., Eds.; SAGE Publications: London, UK, 2004. [Google Scholar]
- Rosetti, L. The Rossetti Infant-Toddler Language Scale; LinguiSystems: East Moline, IL, USA, 2006. [Google Scholar]
- Rutter, M.; Bailey, A.; Lord, C. SCQ: The Social Communication Questionnaire; Western Psychological Services: Torrance, CA, USA, 2003. [Google Scholar]
- Bishop, D.V.M. The Children’s Communication Checklist–2; Psychological Corp.: London, UK, 2003. [Google Scholar]
- Bishop, D.V.; Norbury, C.F. Executive functions in children with communication impairments, in relation to autistic symptomatology. 1: Generativity. Autism 2005, 9, 7–27. [Google Scholar] [CrossRef]
- Bishop, D.V.M. Development of the Children’s Communication Checklist (CCC): A method for assessing qualitative aspects of communicative impairment in children. J. Child Psychol. Psychiatry 1998, 39, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.V.M. What Causes Specific Language Impairment in Children? Curr. Dir. Psychol. Sci. 2006, 15, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Geurts, H.M. CCC-2-NL: Children’s Communication Checklist-2; Harcourt Assessment B.V.: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Helland, W.A.; Biringer, E.; Helland, T.; Heimann, M. The usability of a Norwegian adaptation of the Children’s Communication Checklist Second Edition (CCC-2) in differentiating between language impaired and non-language impaired 6- to 12-year-olds. Scand. J. Psychol. 2009, 50, 287–292. [Google Scholar] [CrossRef]
- Glumbić, N.; Brojčin, B.; Đorđević, M. Pouzdanost Komunikacione čekliste za decu [Reliability of the Communication Checkpoint for Children]. Beogradska Defektološka Škola 2010, 16, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Glumbić, N.; Brojčin, B. Factor structure of the Serbian version of the Children’s Communication Checklist-2. Res. Dev. Disabil. 2012, 33, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Vézina, M.; Samson-Morasse, C.; Gauthier-Desgagné, J.; Fossard, M.; Sylvestre, A. Développement de la version québécoise francophone du Children’s Communication Checklist—2 (CCC-2): Traduction, adaptation et équivalence conceptuelle. Revue Canadienne d’orthophonie et d’audiologie 2011, 35, 244–253. [Google Scholar]
- Costa, V.B.; Harsányi, E.; Martins-Reis, V.O.; Kummer, A. Translation and cross-cultural adaptation into Brazilian Portuguese of the Children’s Communication Checklist-2. Codas 2013, 25, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Eguílaz, N.; Magallón, S.; Sánchez-Carpintero, R.; Narbona, J. La adaptación al castellano de la Children’s Communication Checklist permite detectar las dificultades en el uso del lenguaje pragmático y diferenciar subtipos clínicos. [The Spanish adapted version of the Children’s Communication Checklist identifies disorders of pragmatic use of language and differentiates between clinical subtypes]. Rev. Neurol. 2016, 62, S49–S57. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, E.; Garzón, M. Puede el CCC-2 diferenciar perfiles pragmáticos? [Can CCC-2 differentiate pragmatic profiles?]. Rev. Chil. Fonoaudiol. 2012, 11, 37–56. [Google Scholar] [CrossRef]
- Andrés-Roqueta, C.; Adrian, J.E.; Clemente, R.A.; Villanueva, L. Social cognition makes an independent contribution to peer relations in children with Specific Language Impairment. Res. Dev. Disabil. 2016, 49, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Bignell, S.; Cain, K. Pragmatic aspects of communication and language comprehension in groups of children differentiated by teacher ratings of inattention and hyperactivity. Br. J. Dev. Psychol. 2007, 25, 499–512. [Google Scholar] [CrossRef] [Green Version]
- Bishop, D.V.M.; McDonald, D. Identifying language impairment in children: Combining language test scores with parental report. Int. J. Lang. Commun. Disord. 2009, 44, 600–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geurts, H.; Embrechts, M. Pragmatics in pre-schoolers with language impairments. Int. J. Lang. Commun. Disord. 2010, 45, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Grzadzinski, R.; Di Martino, A.; Brady, E.; Mairena, M.A.; O’Neale, M.; Petkova, E.; Castellanos, F.X. Examining autistic traits in children with ADHD: Does the autism spectrum extend to ADHD? J. Autism Dev. Disord. 2011, 41, 1178–1191. [Google Scholar] [CrossRef] [Green Version]
- Volden, J.; Phillips, L. Measuring pragmatic language in speakers with autism spectrum disorders: Comparing the children’s communication checklist—2 and the test of pragmatic language. Am. J. Speech Lang. Pathol. 2010, 19, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Volden, J.; Coolican, J.; Garon, N.; White, J.; Bryson, S. Brief report: Pragmatic language in autism spectrum disorder: Relationships to measures of ability and disability. J. Autism Dev. Disord. 2009, 39, 388–393. [Google Scholar] [CrossRef]
- Whitehouse, A.; Barry, J.G.; Bishop, D.V. Further defining the language impairment of autism: Is there a specific language impairment subtype? J. Commun. Disord. 2008, 41, 319–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, D.V.M.; Hardiman, M.J.; Barry, J.G. Is auditory discrimination mature by middle childhood? A study using time-frequency analysis of mismatch responses from 7 years to adulthood. Dev. Sci. 2011, 14, 402–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawes, P.; Bishop, D. Auditory processing disorder in relation to developmental disorders of language, communication and attention: A review and critique. Int. J. Lang. Commun. Disord. 2009, 44, 440–465. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, M.A.; Hall, R.L.; Riley, A. Communication, listening, cognitive and speech perception skills in children with auditory processing disorder (APD) or Specific Language Impairment (SLI). J. Speech Lang. Hear. Res. 2011, 54, 211–227. [Google Scholar] [CrossRef]
- Solomon, M.; Olsen, E.; Niendam, T.; Ragland, J.D.; Yoon, J.; Minzenberg, M.; Carter, C.S. From lumping to splitting and back again: Atypical social and language development in individuals with clinical-high-risk for psychosis, first episode schizophrenia, and autism spectrum disorders. Schizophr. Res. 2011, 131, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Quach, J.; Hiscock, H.; Canterford, L.; Wake, M. Australian population longitudinal study: Outcomes of child sleep problems over the school-transition period. Pediatrics 2009, 123, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, A.; Martens, M.A.; Fox, R.; Rabidoux, P.; Andridge, R. Pragmatic language assessment in Williams syndrome: A comparison of the Test of Pragmatic Language-2 and the Children’s Communication Checklist-2. Am. J. Speech Lang. Pathol. 2013, 22, 198–204. [Google Scholar] [CrossRef]
- Ramirez-Inscoe, J.; Moore, D.R. Processes that influence communicative impairments in deaf children using cochlear implants. Ear Hear. 2011, 32, 690–698. [Google Scholar] [CrossRef]
- Andrés-Roqueta, C.; Katsos, N. The contribution of grammar, vocabulary and theory of mind in pragmatic language competence in children with autistic spectrum disorders. Front. Psychol. 2017, 8, 996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, C. Intervention for children with pragmatic language impairments: Frameworks, evidence and diversity. In Understanding Developmental Language Disorders: From Theory to Practice; Norbury, C.F., Tomblin, J.B., Bishop, D.V.M., Eds.; Psychology Press: London, UK, 2008; pp. 189–204. [Google Scholar]
- Andrés-Roqueta, C.; Clemente, R.A. Idiom understanding competence of Spanish children with Specific Language Impairment. In Atypical Language Development in Romance Languages; Aguilar-Mediavilla, E., Buil-Legaz, L., López-Penadés, R., Sanchez-Azanza, V.A., Adrover-Roig, D., Eds.; John Benjamins Publishing Company: Amsterdam, The Netherlands, 2019; pp. 114–126. [Google Scholar] [CrossRef]
- Norbury, C.F. Factors supporting idiom comprehension in children with communication disorders. J. Speech Lang. Hear. Res. 2004, 47, 1179–1193. [Google Scholar] [CrossRef]
- Norbury, C.F. The relationship between theory of mind and metaphor: Evidence from children with language impairment and autistic spectrum disorders. Br. J. Dev. Psychol. 2005, 23, 383–399. [Google Scholar] [CrossRef] [Green Version]
- Andrés-Roqueta, C.; Katsos, N. A distinction between linguistic and social pragmatics helps the precise characterization of pragmatic challenges in children with Autism Spectrum Disorders and Developmental Language Disorder. J. Speech Lang. Hear. Res. 2020, 63, 1494–1508. [Google Scholar] [CrossRef]
- Katsos, N.; Andrés-Roqueta, C.; Clemente, R.A.; Cummins, C. Are children with Specific Language Impairment challenged by linguistic-pragmatics? Cognition 2011, 119, 43–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surian, L.; Baron-Cohen, S.; Van der Lely, H. Are children with autism deaf to Gricean Maxims? Cogn. Neuropsychiatr. 1996, 1, 55–71. [Google Scholar] [CrossRef]
- Brock, J.; Norbury, C.; Einav, S.; Nation, K. Do individuals with autism process words in context? Evidence from language-mediated eye-movements. Cognition 2008, 108, 896–904. [Google Scholar] [CrossRef]
- Norbury, C.F.; Gemmell, T.; Paul, R. Pragmatics abilities in narrative production: A cross-disorder comparison. J. Child. Lang. 2014, 41, 485–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrés-Roqueta, C.; Ballester-Manuel, L. Comprensión del Humor Gráfico en niños y niñas con Trastorno Específico del Lenguaje y con Trastorno del Espectro Autista [Graphic Humour understanding in children with Specific Language Impairment and children with Autistic Spectrum Disorder]. In Psicología y educación: Presente y futuro; Castejón, J., Ed.; ACIPE—Asociación Científica de Psicología y Educación: Alicante, Spain, 2016; pp. 1803–1811. [Google Scholar]
- Andrés-Roqueta, C.; Clemente, R.A. Dificultades pragmáticas en el Trastorno Específico del Lenguaje. El papel de las tareas mentalistas [Pragmatic difficulties in children with specific language impairment. The role of mentalistic tasks]. Psicothema 2010, 22, 677–683. [Google Scholar]
- Happé, F. An advanced test of theory of mind: Understanding of story characters thoughts and feelings by able autistic, mentally handicapped, and normal children and adults. Autism Dev. Disord. 1994, 2, 129–154. [Google Scholar] [CrossRef]
- Botting, N.; Conti-Ramsden, G. The role of language, social cognition, and social skill in the functional social outcomes of young adolescents with and without a history of SLI. Br. J. Dev. Psychol. 2008, 26, 281–300. [Google Scholar] [CrossRef]
- Martin, I.; McDonald, S. Weak coherence, no theory of mind, or executive dysfunction? Solving the puzzle of pragmatic language disorders. Brain Lang. 2003, 85, 451–466. [Google Scholar] [CrossRef]
- Green, B.C.; Johnson, K.A.; Bretherton, L. Pragmatic language difficulties in children with hyperactivity and attention problems: An integrated review. Int. J. Lang. Commun. Disord. 2014, 49, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, E.; Carballo, G.; Muñoz, J.; Fresneda, M.D. CEG: Test de Comprensión de Estructuras Gramaticales [Grammatical Structures Comprehension Test]; TEA Ediciones: Madrid, Spain, 2005. [Google Scholar]
- Saborit, C.; Julián, J.P. L’avaluacio del Llenguatge Infantil, ELI [Assessment of Children’s Language]; Universitat Jaume I. Col·leccio Educació: Castellón, España, 2005. [Google Scholar]
- Conti-Ramsden, G.; Botting, N.; Faragher, B. Psycholinguistic markers for specific language impairment (SLI). J. Child Psychol. Psychiatry 2001, 42, 741–748. [Google Scholar] [CrossRef]
- Raven, J.C. Manual for the Coloured Progressive Matrices (Revised); NFERNelson: Windsor, UK, 1984. [Google Scholar]
- Norbury, C.; Bishop, D. Children’s Communication Checklist—2: A validation study. Rev. Tranel (Travaux Neuchâtelois de Linguistique) 2005, 42, 83-63. [Google Scholar]
- Bishop, D.V.M.; Laws, G.; Adams, C.; Norbury, C.F. High heritability of speech and language impairments in 6-year-old twins demonstrated using parent and teacher report. Behav. Genet. 2006, 36, 173–184. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Maybery, M.; Wong, D.; Maley, A.; Hallmayer, J. Characteristics of the broader phenotype in autism: A study of siblings using the Children’s Communication Checklist-2. Am. J. Med. Genet. 2006, 141, 117–122. [Google Scholar] [CrossRef]
- Raven, J.C.; Court, J.H.; Raven, J. Section 2: Coloured Progressive Matrices (1990 Edition, with US Norms). Manual for the Raven’s Progressive Matrices and Vocabulary Scales; Oxford Psychologist Press: Oxford, UK, 1990. [Google Scholar]
- Bishop, D.V.M. Test for Reception of Grammar. Medical Research Council; Chapel Press; University of Manchester: Manchester, UK, 1983. [Google Scholar]
- Kaufman, A.S.; Kaufman, N.L. K-BIT. Test Breve de Inteligencia de Kaufman (K-BIT), 2nd ed.; TEA Ediciones: Madrid, Spain, 2000. [Google Scholar]
- Wechsler, D. Manual for the Wechsler Intelligence Scale for Children, 3rd ed.; The Psychological Corporation: San Antonio, TX, USA, 1991. [Google Scholar]
- Dunn, L.M.; Dunn, L.M.; Arribas, D. PPVT-III Peabody, Test de Vocabulario en Imágenes; TEA Ediciones: Madrid, Spain, 2006. [Google Scholar]
- Kirk, S.; McCarthy, J.; Kirk, W. Illinois Test of Psycholinguistic Abilities. Examiner’s Manual; University of Illinois Press: Champaign, IL, USA, 1968; pp. 3–14. [Google Scholar]
- Muñoz, J.; Fresneda, M.D.; Mendoza, E.; Carballo, G. Propiedades psicométricas de una prueba de comprensión gramatical [Psychometric properties of a grammatical comprehension test]. Rev. Neurol. 2008, 47, 21–23. [Google Scholar]
- White, S.; Hill, E.; Happé, F.; Frith, U. Revisiting the Strange Stories: Revealing mentalising impairments in autism. Child Dev. 2009, 80, 1097–1117. [Google Scholar] [CrossRef] [PubMed]
- Cairns, E.; Cammock, T. Development of a more reliable version of the Matching Familiar Figures Test. Dev. Psychol. 1978, 14, 555–560. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Aspects of Communication | Sample Items |
|---|---|
| A. Speech | He/she speaks fluently and clearly, producing all speech sounds accurately and without hesitating. |
| B. Syntax | He/she produces long and complicated phrases like: “When we were in the park I went to see the ducks” or “I saw that man standing on the corner”. |
| C. Semantics | He/she uses words that refer to classes of objects, rather than specific things; e.g., talks about the table, chair and drawers as “furniture”, or calls bananas, apples and pears “fruit”. |
| D. Coherence | It is difficult to know whether he/she is talking about something real or something invented. |
| E. Inappropriate initiation | He/she talks repeatedly about things that no-one is interested in. |
| F. Stereotyped language | When he/she answers a question, he/she provides sufficient and relevant information, without being overly precise if it is not necessary. |
| G. Context | His/her ability to communicate is different according to the situation. He/she may not have any trouble talking one-on-one with a familiar adult, but may find it difficult to express him/herself with a group of children of his/her own age. |
| H. Non-verbal communication | He/she doesn’t look at people when he/she talks to them. |
| I. Social Relations | He/she hurts or disturbs other children without realizing it, unintentionally. |
| J. Interests | He/she leads the conversation towards his/her favorite topics, even when others are not interested. |
| DLD (n = 30) | AM (n = 39) | U | p | r | |||
|---|---|---|---|---|---|---|---|
| M (SD) | Range | M (SD) | Range | ||||
| Age and Gender | |||||||
| Months | 70.50 (17.86) | 46–108 | 68.62 (14.26) | 43–109 | 560.5 | 0.767 | |
| Gender (M:F) | 22:08 | 28:11:00 | - | - | |||
| Structural language measures | |||||||
| Phonetics (range: 0–3) | 1.07 (0.91) | 0–3 | 0 (0) | 0–0 | 156 | 0 | 0.761 |
| Receptive grammar (range: 0–80) | 50.43 (10.62) | 17–68 | 64.69 (7.56) | 48–77 | 146 | 0 | 0.682 |
| Expressive grammar (range: 0–10) | 5.13 (1.83) | 2–8 | 7.97 (1.31) | 4–9 | 126 | 0 | 0.64 |
| Receptive vocabulary (range: 0–30) | 21.03 (6.22) | 5–30 | 23.92 (4.91) | 10–29 | 390 | 0.018 | 0.285 |
| Expressive vocabulary (range: 0–30) | 18.47 (6.31) | 7–27 | 22.64 (6.20) | 10–30 | 351 | 0.005 | 0.341 |
| Structural language | 53.71 (16.62) | 14.54–75.53 | 75.62 (6.24) | 60.62–83.7 | 89 | 0 | 0.722 |
| Pragmatics | |||||||
| Receptive pragmatics (range: 0–6) | 4.8 (1.32) | 1–6 | 5.59 (0.91) | 2–6 | 332.5 | 0.001 | 0.414 |
| Expressive Pragmatics (range: 0–8) | 2.8 (1.91) | 0–8 | 5.10 (1.77) | 1–8 | 213.5 | 0 | 0.547 |
| Pragmatics (range: 0–14) | 7.6 (2.66) | 3–14 | 10.69 (2.33) | 5–14 | 221.5 | 0 | 0.533 |
| Social cognition measure | |||||||
| Speaker’s intention (range: 0–18) | 4.8 (3.68) | 0–12 | 10.87 (3.87) | 1–16 | 152.5 | 0 | 0.632 |
| Executive function measures | |||||||
| Sustained attention | 22.14 (12.58) | 7–53 | 15.74 (7.14) | 4–32 | 405 | 0.046 | 0.24 |
| Response latency | 7.3 (5.71) | 1.71–20.30 | 15.40 (12.57) | 2.82–75.15 | 260 | 0 | 0.456 |
| Executive function | 33.53 (14.64) | 2.28–56.75 | 44.67 (12.56) | 20.3–82.46 | 323 | 0.003 | 0.362 |
| DLD (n = 30) | ||
|---|---|---|
| M (SD) | Range | |
| GCC score | 67.53 (16.71) | 30–100 |
| SIDI index | 10.07 (9.28) | −7–39 |
| Structural Language (A + B + C + D) scaled score | 28.57 (8.07) | 14–49 |
| Pragmatics (D + E + F + G + H) scaled score | 47.93 (12.45) | 28–73 |
| Autistic index (I + J) scaled score | 18.53–5.91 | 11–35 |
| A. Speech | 6.47 (3.39) | 0–13 |
| B. Syntax | 5.6 (3.05) | 0–12 |
| C. Semantics | 7.53(2.36) | 4–15 |
| D. Coherence | 8.97 (3.2) | 5–16 |
| E. Inappropriate initiation | 11.37 (4.06) | 4–21 |
| F. Stereotyped language | 10.37 (3.38) | 5–16 |
| G. Context | 8.50 (3.19) | 4–20 |
| H. Non-verbal communication | 8.73 (3.99) | 3–21 |
| I. Social relations | 7.37 (4.09) | 2–21 |
| J. Interests | 11.17 (4.55) | 1–22 |
| Structural Language (A + B + C + D) raw score (range: 0–28) | 21.37 (12.54) | 2–52 |
| Pragmatics (D + E + F + G + H) raw score (range: 0–35) | 21 (12.14) | 5–45 |
| Autistic index (I + J) raw score (range: 0–14) | 8.20 (3.75) | 3–18 |
| Age | St. Lang | Prag | SC | EF | St. Lang CCC-2 | Prag CCC-2 | |
|---|---|---|---|---|---|---|---|
| Age | |||||||
| St. lang | 0.624 ** | ||||||
| Prag | 0.382 * | 0.557 ** | |||||
| SC | 0.292 | 0.434 * | 0.384 * | ||||
| EF | 0.563 ** | 0.593 ** | 0.552 ** | 0.250 | |||
| St. lang CCC-2 | −0.705 ** | −0.703 ** | −0.445 * | −0.354 | −0.685 ** | ||
| Prag CCC-2 | −0.231 | −0.442 * | −0.401 * | −0.457 * | −0.510 ** | 0.663 ** | |
| Aut CCC-2 | −0.276 | −0.444 * | −0.219 | −0.280 | −0.472 ** | 0.568 ** | 0.527 ** |
| Structural Language CCC-2 (A + B + C + D) | ||||||
|---|---|---|---|---|---|---|
| Predictor | R2 Adjusted | B | B 95% CI (LL, UL) | SE B | t | p |
| Step 1 | 0.369 | |||||
| Constant | 51.672 | [36.841, 67.801] | 6.592 | 0.001 | ||
| Age | −0.427 | [−0.635, −0.248] | −0.607 | −3.972 | 0.003 | |
| Step 2 | 0.226 | |||||
| Constant | 56.748 | [42.854, 70.537] | 8.680 | 0.000 | ||
| Age | −0.141 | [−0.305, 0.149] | −0.200 | −1.216 | 0.167 | |
| St. Language | −0.472 | [−0.848, −0.208] | −0.626 | −3.807 | 0.013 | |
| Step 3 | 0.026 | |||||
| Constant | 59.296 | [44.281, 72.738] | 8.804 | 0.000 | ||
| Age | −0.137 | [−0.292, 0.202] | −0.196 | −1.206 | 0.192 | |
| St. Lang | −0.395 | [−0.832, −0.162] | −0.524 | −2.917 | 0.031 | |
| Prag | −0.907 | [−2.346, 0.570] | −0.192 | −1.312 | 0.214 | |
| Step 4 | 0.003 | |||||
| Constant | 59.018 | [43.206, 73.028] | 8.581 | 0.000 | ||
| Age | −0.136 | [−0.291, 0.202] | −0.194 | −1.176 | 0.203 | |
| St. Language | −0.381 | [−0.833, −0.133] | −0.505 | −2.685 | 0.042 | |
| Prag | −0.852 | [−2.580, 0.661] | −0.181 | −1.193 | 0.300 | |
| SC | −0.207 | [−1.200, 0.825] | −0.061 | −0.430 | 0.653 | |
| Step 5 | 0.018 | |||||
| Constant | 57.804 | [42.260, 72.465] | 8.311 | 0.000 | ||
| Age | −0.092 | [−0.254, 0.323] | −0.131 | −0.752 | 0.453 | |
| St. Language | −0.356 | [−0.839, −0.109] | −0.472 | −2.480 | 0.060 | |
| Prag | −0.568 | [−2.315, 1.163] | −0.121 | −0.747 | 0.518 | |
| SC | −0.219 | [−1.043, 0.838] | −0.064 | −0.455 | 0.648 | |
| EF | −0.159 | [−0.599, 0.104] | −0.183 | −1.061 | 0.356 | |
| Pragmatic CCC-2 (D + E + F + G + H) | ||||||
|---|---|---|---|---|---|---|
| Predictor | R2 Adjusted | B | B 95% CI (LL, UL) | SE B | t | p |
| Step 1 | 0.071 | |||||
| Constant | 34.013 | [16.291, 52.549] | 3.725 | 0.003 | ||
| Age | −0.180 | [−0.432, 0.055] | −0.266 | −1.435 | 0.155 | |
| Step 2 | 0.155 | |||||
| Constant | 38.048 | [21.054, 55.890] | 4.385 | 0.001 | ||
| Age | 0.048 | [−0.282, 0.361] | 0.071 | 0.313 | 0.755 | |
| St. Language | −0.375 | [−0.746, −0.003] | −0.518 | −2.280 | 0.037 | |
| Step 3 | 0.060 | |||||
| Constant | 41.751 | [21.742, 58.248] | 4.703 | 0.001 | ||
| Age | 0.052 | [−0.242, 0.379] | 0.078 | 0.349 | 0.707 | |
| St. Lang | −0.264 | [−0.711, 0.053] | −0.364 | −1.477 | 0.138 | |
| Prag | −1.318 | [−3.045, 0.789] | −0.291 | −1.447 | 0.158 | |
| Step 4 | 0.054 | |||||
| Constant | 40.602 | [21.339, 58.148] | 4.639 | 0.001 | ||
| Age | 0.057 | [−0.255, 0.357] | 0.085 | 0.387 | 0.676 | |
| St. Language | −0.204 | [−0.664, 0.208] | −0.282 | −1.130 | 0.295 | |
| Prag | −1.092 | [−2.960, 1.203] | −0.241 | −1.202 | 0.295 | |
| SC | −0.855 | [−2.391, 0.538] | −0.262 | −1.395 | 0.272 | |
| Step 5 | 0.030 | |||||
| Constant | 39.076 | [18.758, 56.919] | 4.412 | 0.003 | ||
| Age | 0.112 | [−0.191, 0.444] | 0.166 | 0.718 | 0.433 | |
| St. Language | −0.172 | [−0.648, 0.191] | −0.238 | −0.944 | 0.377 | |
| Prag | −0.735 | [−2.722, 1.758] | −0.162 | −0.759 | 0.515 | |
| SC | −0.870 | [−2.401, 0.461] | −0.266 | −1.421 | 0.252 | |
| EF | −0.200 | [−0.864, 0.167] | −0.240 | −1.047 | 0.346 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrés-Roqueta, C.; Garcia-Molina, I.; Flores-Buils, R. Association between CCC-2 and Structural Language, Pragmatics, Social Cognition, and Executive Functions in Children with Developmental Language Disorder. Children 2021, 8, 123. https://0-doi-org.brum.beds.ac.uk/10.3390/children8020123
Andrés-Roqueta C, Garcia-Molina I, Flores-Buils R. Association between CCC-2 and Structural Language, Pragmatics, Social Cognition, and Executive Functions in Children with Developmental Language Disorder. Children. 2021; 8(2):123. https://0-doi-org.brum.beds.ac.uk/10.3390/children8020123
Chicago/Turabian StyleAndrés-Roqueta, Clara, Irene Garcia-Molina, and Raquel Flores-Buils. 2021. "Association between CCC-2 and Structural Language, Pragmatics, Social Cognition, and Executive Functions in Children with Developmental Language Disorder" Children 8, no. 2: 123. https://0-doi-org.brum.beds.ac.uk/10.3390/children8020123