
Can Event-Related Potentials Evoked by Heel Lance Assess Pain Processing in Neonates? A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statement on Review
2.2. Search Strategy
2.3. Selection Criteria
2.4. Study Selection Process
2.4.1. Primary Screening
2.4.2. Secondary Screening
2.5. Assessment of the Methodological Quality of the Studies
2.6. Data Extraction
3. Results
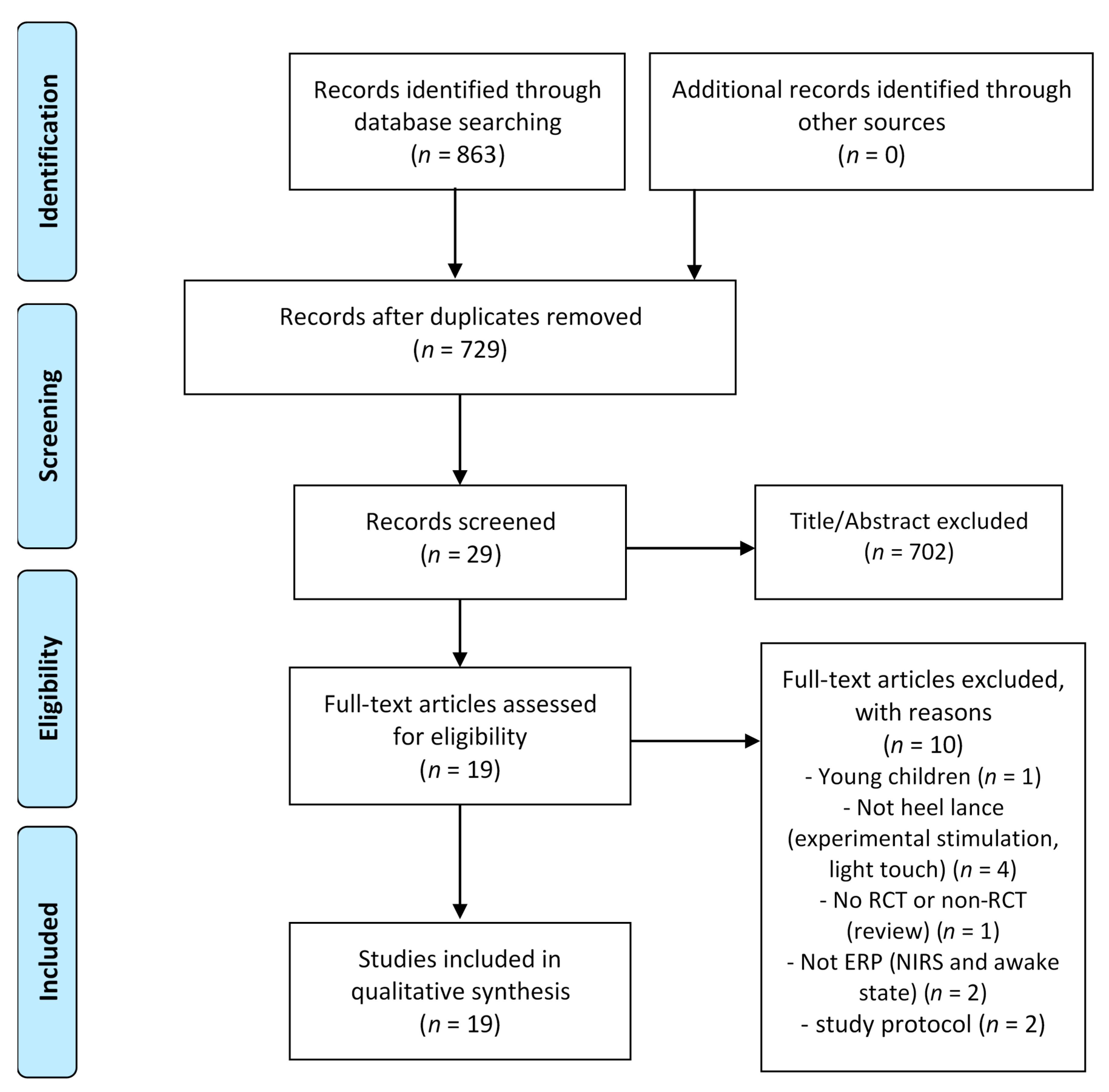
3.1. Study Selection
3.2. Study Characteristics
3.3. ERP Evoked by Heel Lance
3.4. Comparison of ERP Evoked by Heel Lance and Tactile Stimulation
3.5. Association between GA and ERP Evoked by Heel Lance
3.6. ERP as an Indicator of the Effect of Pain Relief Strategies against Heel Lance in Neonates
4. Discussion
4.1. Results of ERP Evoked by Heel Lance in Term Infants
4.1.1. Characteristics of ERP Evoked by Heel Lance
4.1.2. Question about Latency of ERP Evoked by Heel Lance in Neonates
4.2. Comparison between ERP and PIPP
4.3. ERP-Based Evaluation of Intervention Effect
4.4. ERP Evoked by Heel Lance in Preterm Infants
4.5. Problems of ERP Study Methods in Neonates
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz, M.D.; Fernandes, A.M.; Oliveira, C.R. Epidemiology of painful procedures performed in neonates: A systematic review of observational studies. Eur. J. Pain 2016, 20, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Ranger, M.; Grunau, R.E. Early repetitive pain in preterm infants in relation to the developing brain. Pain Manag. 2014, 4, 57–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brummelte, S.; Grunau, R.E.; Chau, V.; Poskitt, K.J.; Brant, R.; Vinall, J.; Gover, A.; Synnes, A.R.; Miller, S.P. Procedural pain and brain development in premature newborns. Ann. Neurol. 2012, 71, 385–396. [Google Scholar] [CrossRef]
- Lax, I.D.; Duerden, E.G.; Lin, S.Y.; Mallar Chakravarty, M.; Donner, E.J.; Lerch, J.P.; Taylor, M.J. Neuroanatomical consequences of very preterm birth in middle childhood. Brain Struct. Funct. 2013, 218, 575–585. [Google Scholar] [CrossRef]
- Nosarti, C.; Giouroukou, E.; Healy, E.; Rifkin, L.; Walshe, M.; Reichenberg, A.; Chitnis, X.; Williams, S.C.R.; Murray, R.M. Grey and white matter distribution in very preterm adolescents mediates neurodevelopmental outcome. Brain 2008, 131, 205–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nosarti, C.; Al-Asady, M.H.S.; Frangou, S.; Stewart, A.L.; Rifkin, L.; Murray, R.M. Adolescents who were born very preterm have decreased brain volumes. Brain 2002, 125, 1616–1623. [Google Scholar] [CrossRef] [Green Version]
- Grunau, R.E.; Whitfield, M.F.; Petrie-Thomas, J.; Synnes, A.R.; Cepeda, I.L.; Keidar, A.; Rogers, M.; MacKay, M.; Hubber-Richard, P.; Johannesen, D. Neonatal pain, parenting stress and interaction, in relation to cognitive and motor development at 8 and 18 months in preterm infants. Pain 2009, 143, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Vinall, J.; Miller, S.P.; Bjornson, B.H.; Fitzpatrick, K.P.V.; Poskitt, K.J.; Brant, R.; Synnes, A.R.; Cepeda, I.L.; Grunau, R.E. Invasive procedures in preterm children: Brain and cognitive development at school age. Pediatrics 2014, 133, 412–421. [Google Scholar] [CrossRef] [Green Version]
- Vinall, J.; Miller, S.P.; Synnes, A.R.; Grunau, R.E. Parent behaviors moderate the relationship between neonatal pain and internalizing behaviors at 18 months corrected age in children born very prematurely. Pain 2013, 154, 1831–1839. [Google Scholar] [CrossRef] [Green Version]
- Walker, S.M.; Melbourne, A.; O’Reilly, H.; Beckmann, J.; Eaton-Rosen, Z.; Ourselin, S.; Marlow, N. Somatosensory function and pain in extremely preterm young adults from the UK EPICure cohort: Sex-dependent differences and impact of neonatal surgery. Br. J. Anaesth. 2018, 121, 623–635. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.; Doyle, L.W. Neurobehavioral Outcomes of School-age Children Born Extremely Low Birth Weight or Very Preterm in the 1990s. J. Am. Med. Assoc. 2003, 289, 3264–3272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loe, I.M.; Lee, E.S.; Luna, B.; Feldman, H.M. Behavior problems of 9-16year old preterm children: Biological, sociodemographic, and intellectual contributions. Early Hum. Dev. 2011, 87, 247–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grunau, R.E.; Whitfield, M.F.; Fay, T.B. Psychosocial and academic characteristics of extremely low birth weight (≤800 g) adolescents who are free of major impairment compared with term-born control subjects. Pediatrics 2004, 114, e725–e732. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, L.A.; Miskovic, V.; Boyle, M.; Saigal, S. Frontal electroencephalogram asymmetry, salivary cortisol, and internalizing behavior problems in young adults who were born at extremely low birth weight. Child Dev. 2010, 81, 183–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dührsen, L.; Simons, S.H.P.; Dzietko, M.; Genz, K.; Bendix, I.; Boos, V.; Sifringer, M.; Tibboel, D.; Felderhoff-Mueser, U. Effects of repetitive exposure to pain and morphine treatment on the neonatal rat brain. Neonatology 2012, 103, 35–43. [Google Scholar] [CrossRef]
- Harrison, D.; Loughnan, P.; Manias, E.; Johnston, L. Analgesics administered during minor painful procedures in a cohort of hospitalized infants: A prospective clinical audit. J. Pain 2009, 10, 715–722. [Google Scholar] [CrossRef]
- Bellieni, C.V.; Tei, M.; Cornacchione, S.; Di Lucia, S.; Nardi, V.; Verrotti, A.; Buonocore, G. Pain perception in NICU: A pilot questionnaire. J. Matern. Fetal Neonatal Med. 2018, 31, 1921–1923. [Google Scholar] [CrossRef]
- Pillai Riddell, R.; Racine, N.; Gennis, H.; Turcotte, K.; Uman, L.; Horton, R.; Ahola Kohut, S.; Hillgrove Stuart, J.; Stevens, B.; Lisi, D. Non-pharmacological management of infant and young child procedural pain (Review) summary of findings for the main comparison. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Stevens, B.; Yamada, J.; Ohlsson, A.; Haliburton, S.; Shorkey, A. Sucrose for analgesia in newborn infants undergoing painful procedures (Review) SUMMARY OF FINDINGS FOR THE MAIN COMPARISON. Cochrane Libr. 2017. [Google Scholar] [CrossRef]
- Campbell-Yeo, M. Combining facilitated tucking and non-nutritive sucking appears to promote greater regulation for preterm neonates following heel lance, but does not provide effective pain relief. Evid. Based Nurs. 2019, 22, 19. [Google Scholar] [CrossRef]
- Gao, H.; Li, M.; Gao, H.; Xu, G.; Li, F.; Zhou, J.; Zou, Y.; Jiang, H. Effect of non-nutritive sucking and sucrose alone and in combination for repeated procedural pain in preterm infants: A randomized controlled trial. Int. J. Nurs. Stud. 2018, 83, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.F.; Yin, T.; Yang, L.; Wang, C.; Chang, Y.C.; Jeng, M.J.; Liaw, J.J. Non-nutritive sucking, oral breast milk, and facilitated tucking relieve preterm infant pain during heel-stick procedures: A prospective, randomized controlled trial. Int. J. Nurs. Stud. 2018, 77, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Perroteau, A.; Nanquette, M.C.; Rousseau, A.; Renolleau, S.; Bérard, L.; Mitanchez, D.; Leblanc, J. Efficacy of facilitated tucking combined with non-nutritive sucking on very preterm infants’ pain during the heel-stick procedure: A randomized controlled trial. Int. J. Nurs. Stud. 2018, 86, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Davari, S.; Borimnejad, L.; Khosravi, S.; Haghani, H. The effect of the facilitated tucking position on pain intensity during heel stick blood sampling in premature infants: A surprising result. J. Matern. Neonatal Med. 2019, 32, 3427–3430. [Google Scholar] [CrossRef]
- Uematsu, H.; Sobue, I. Effect of music (brahms lullaby) and non-nutritive sucking on heel lance in preterm infants: A randomized controlled crossover trial. Paediatr. Child Health 2019, 24, E33–E39. [Google Scholar] [CrossRef] [Green Version]
- Ballantyne, M.; Stevens, B.; McAllister, M.; Dionne, K.; Jack, A. Validation of the premature infant pain profile in the clinical setting. Clin. J. Pain 1999, 15, 297–303. [Google Scholar] [CrossRef]
- Stevens, B.; Johnston, C.; Petryshen, P.; Taddio, A. Premature Infant Pain Profile: Development and initial validation. Clin. J. Pain 1996, 12, 13–22. [Google Scholar] [CrossRef]
- Gibbins, S.; Stevens, B.J.; Yamada, J.; Dionne, K.; Campbell-Yeo, M.; Lee, G.; Caddell, K.; Johnston, C.; Taddio, A. Validation of the Premature Infant Pain Profile-Revised (PIPP-R). Early Hum. Dev. 2014, 90, 189–193. [Google Scholar] [CrossRef]
- Stevens, B.J.; Gibbins, S.; Yamada, J.; Dionne, K.; Lee, G.; Johnston, C.; Taddio, A. The premature infant pain profile-revised (PIPP-R): Initial validation and feasibility. Clin. J. Pain 2014, 30, 238–243. [Google Scholar] [CrossRef]
- Stevens, B.; Johnston, C.; Taddio, A.; Gibbins, S.; Yamada, J. The premature infant pain profile: Evaluation 13 years after development. Clin. J. Pain 2010, 26, 813–830. [Google Scholar] [CrossRef] [Green Version]
- Hartley, C.; Goksan, S.; Poorun, R.; Brotherhood, K.; Mellado, G.S.; Moultrie, F.; Rogers, R.; Adams, E.; Slater, R. The relationship between nociceptive brain activity, spinal reflex withdrawal and behaviour in newborn infants. Sci. Rep. 2015, 5, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moultrie, F.; Slater, R.; Hartley, C. Improving the treatment of infant pain. Curr. Opin. Support. Palliat. Care 2017, 11, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiroshita, Y.; Kirimoto, H.; Nakagawa, K.; Uematsu, H.; Sobue, I. Evoked Potential as a Pain Evaluation Index for Neonatal Procedural Pain. Int. J. Nurs. Clin. Pract. 2020, 7. [Google Scholar] [CrossRef]
- Gursul, D.; Hartley, C.; Slater, R. Nociception and the neonatal brain. Semin. Fetal Neonatal Med. 2019, 24, 101016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Relland, L.M.; Gehred, A.; Maitre, N.L. Behavioral and Physiological Signs for Pain Assessment in Preterm and Term Neonates during a Nociception-Specific Response: A Systematic Review. Pediatr. Neurol. 2019, 90, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Hartley, C.; Slater, R. Neurophysiological measures of nociceptive brain activity in the newborn infant-the next steps. Acta Paediatr. Int. J. Paediatr. 2014, 103, 238–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzabazis, A.Z.; Klukinov, M.; Crottaz-Herbette, S.; Nemenov, M.I.; Angst, M.S.; Yeomans, D.C. Selective nociceptor activation in volunteers by infrared diode laser. Mol. Pain 2011, 7, 1744–8069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zotterman, Y. Touch, pain and tickling: An electro-physiological investigation on cutaneous sensory nerves. J. Physiol. 1939, 95, 1–28. [Google Scholar] [CrossRef]
- Burgess, P.R.; Perl, E.R. Myelinated afferent fibres responding specifically to noxious stimulation of the skin. J. Physiol. 1967, 190, 541–562. [Google Scholar] [CrossRef]
- Torebjörk, H.E.; Hallin, R.G. Perceptual changes accompanying controlled preferential blocking of A and C fibre responses in intact human skin nerves. Exp. Brain Res. 1973, 16, 321–332. [Google Scholar] [CrossRef]
- Hallin, R.G.; Torebjörk, H.E. Electrically induced A and C fibre responses in intact human skin nerves. Exp. Brain Res. 1973, 16, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; Barrell, J.J.; Gracely, R.H. A psychophysical analysis of experiential factors that selectively influence the affective dimension of pain. Pain 1980, 8, 137–149. [Google Scholar] [CrossRef]
- Adriaensen, H.; Gybels, J.; Handwerker, H.O.; Van Hees, J. Response properties of thin myelinated (A-delta) fibers in human skin nerves. J. Neurophysiol. 1983, 49, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, L. Neonatal pain: What’s age got to do with it? Surg. Neurol. Int. 2014, 5, 479. [Google Scholar] [CrossRef]
- Basbaum, A.I.; Fields, H.L. Endogenous pain control systems: Brainstem spinal pathways and endorphin circuitry. Annu. Rev. Neurosci. 1984, 7, 309–338. [Google Scholar] [CrossRef]
- Inui, K.; Kakigi, R. Pain perception in humans: Use of intraepidermal electrical stimulation. J. Neurol. Neurosurg. Psychiatry 2012, 83, 551–556. [Google Scholar] [CrossRef]
- Truini, A.; Panuccio, G.; Galeotti, F.; Maluccio, M.R.; Sartucci, F.; Avoli, M.; Cruccu, G. Laser-evoked potentials as a tool for assessing the efficacy of antinociceptive drugs. Eur. J. Pain 2010, 14, 222–225. [Google Scholar] [CrossRef] [Green Version]
- Malver, L.P.; Brokjær, A.; Staahl, C.; Graversen, C.; Andresen, T.; Drewes, A.M. Electroencephalography and analgesics. Br. J. Clin. Pharmacol. 2014, 77, 72–95. [Google Scholar] [CrossRef] [Green Version]
- Slater, R.; Worley, A.; Fabrizi, L.; Roberts, S.; Meek, J.; Boyd, S.; Fitzgerald, M. Evoked potentials generated by noxious stimulation in the human infant brain. Eur. J. Pain 2010, 14, 321–326. [Google Scholar] [CrossRef]
- Benoit, B.; Martin-Misener, R.; Newman, A.; Latimer, M.; Campbell-Yeo, M. Neurophysiological assessment of acute pain in infants: A scoping review of research methods. Acta Paediatr. Int. J. Paediatr. 2017, 106, 1053–1066. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maimon, N.; Grunau, R.E.; Cepeda, I.L.; Friger, M.; Selnovik, L.; Gilat, S.; Shany, E. Electroencephalographic activity in response to procedural pain in preterm infants born at 28 and 33 weeks gestational age. Clin. J. Pain 2013, 29, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Maitre, N.L.; Stark, A.R.; McCoy Menser, C.C.; Chorna, O.D.; France, D.J.; Key, A.F.; Wilkens, K.; Moore-Clingenpeel, M.; Wilkes, D.M.; Bruehl, S. Cry presence and amplitude do not reflect cortical processing of painful stimuli in newborns with distinct responses to touch or cold. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F428–F433. [Google Scholar] [CrossRef] [PubMed]
- Hartley, C.; Duff, E.P.; Green, G.; Mellado, G.S.; Worley, A.; Rogers, R.; Slater, R. Nociceptive brain activity as a measure of analgesic efficacy in infants. Sci. Transl. Med. 2017, 9, eaah6122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.; Laudiano-Dray, M.P.; Whitehead, K.; Verriotis, M.; Meek, J.; Fitzgerald, M.; Fabrizi, L. EEG, behavioural and physiological recordings following a painful procedure in human neonates. Sci. Data 2018, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (Minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T. Assessing the methodological quality of published papers. BMJ 1997, 315, 305–308. [Google Scholar] [CrossRef]
- Oremus, M.; Wolfson, C.; Perrault, A.; Demers, L.; Momoli, F.; Moride, Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement. Geriatr. Cogn. Disord. 2001, 12, 232–236. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Wu, P.L.; Lee, M.; Huang, T.T. Effectiveness of physical activity on patients with depression and Parkinson’s disease: A systematic review. PLoS ONE 2017, 12, e0181515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crellin, D.J.; Harrison, D.; Santamaria, N.; Babl, F.E. Systematic review of the Face, Legs, Activity, Cry and Consolability scale for assessing pain in infants and children. Pain 2015, 156, 2132–2151. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Laudiano-Dray, M.P.; Whitehead, K.; Meek, J.; Fitzgerald, M.; Fabrizi, L.; Pillai Riddell, R. The impact of parental contact upon cortical noxious-related activity in human neonates. Eur. J. Pain 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gursul, D.; Goksan, S.; Hartley, C.; Mellado, G.S.; Moultrie, F.; Hoskin, A.; Adams, E.; Hathway, G.; Walker, S.; McGlone, F.; et al. Stroking modulates noxious-evoked brain activity in human infants. Curr. Biol. 2018, 28, R1380–R1381. [Google Scholar] [CrossRef] [Green Version]
- Slater, R.; Cornelissen, L.; Fabrizi, L.; Patten, D.; Yoxen, J.; Worley, A.; Boyd, S.; Meek, J.; Fitzgerald, M. Oral sucrose as an analgesic drug for procedural pain in newborn infants: A randomised controlled trial. Lancet 2010, 376, 1225–1232. [Google Scholar] [CrossRef] [Green Version]
- Norman, E.; Rosén, I.; Vanhatalo, S.; Stjernqvist, K.; Ökland, O.; Fellman, V.; Hellström-Westas, L. Electroencephalographic response to procedural pain in healthy term newborn infants. Pediatr. Res. 2008, 64, 429–434. [Google Scholar] [CrossRef] [Green Version]
- Hartley, C.; Moultrie, F.; Hoskin, A.; Green, G.; Monk, V.; Bell, J.L.; King, A.R.; Buckle, M.; van der Vaart, M.; Gursul, D.; et al. Analgesic efficacy and safety of morphine in the Procedural Pain in Premature Infants (Poppi) study: Randomised placebo-controlled trial. Lancet 2018, 392, 2595–2605. [Google Scholar] [CrossRef] [Green Version]
- Slater, R.; Fabrizi, L.; Worley, A.; Meek, J.; Boyd, S.; Fitzgerald, M. Premature infants display increased noxious-evoked neuronal activity in the brain compared to healthy age-matched term-born infants. Neuroimage 2010, 52, 583–589. [Google Scholar] [CrossRef]
- Verriotis, M.; Jones, L.; Whitehead, K.; Laudiano-Dray, M.; Panayotidis, I.; Patel, H.; Meek, J.; Fabrizi, L.; Fitzgerald, M. The distribution of pain activity across the human neonatal brain is sex dependent. Neuroimage 2018, 178, 69–77. [Google Scholar] [CrossRef]
- Fabrizi, L.; Verriotis, M.; Williams, G.; Lee, A.; Meek, J.; Olhede, S.; Fitzgerald, M. Encoding of mechanical nociception differs in the adult and infant brain. Sci. Rep. 2016, 6, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabrizi, L.; Slater, R.; Worley, A.; Meek, J.; Boyd, S.; Olhede, S.; Fitzgerald, M. A shift in sensory processing that enables the developing human brain to discriminate touch from pain. Curr. Biol. 2011, 21, 1552–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worley, A.; Fabrizi, L.; Boyd, S.; Slater, R. Multi-modal pain measurements in infants. J. Neurosci. Methods 2012, 205, 252–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verriotis, M.; Fabrizi, L.; Lee, A.; Cooper, R.J.; Fitzgerald, M.; Meek, J. Mapping cortical responses to somatosensory stimuli in human infants with simultaneous near-infrared spectroscopy and event-related potential recording. ENeuro 2016, 3, 663–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.; Fabrizi, L.; Laudiano-Dray, M.; Whitehead, K.; Meek, J.; Verriotis, M.; Fitzgerald, M. Nociceptive Cortical Activity Is Dissociated from Nociceptive Behavior in Newborn Human Infants under Stress. Curr. Biol. 2017, 27, 3846–3851.e3. [Google Scholar] [CrossRef] [Green Version]
- Green, G.; Hartley, C.; Hoskin, A.; Duff, E.; Shriver, A.; Wilkinson, D.; Adams, E.; Rogers, R.; Moultrie, F.; Slater, R. Behavioural discrimination of noxious stimuli in infants is dependent on brain maturation. Pain 2019, 160, 493–500. [Google Scholar] [CrossRef]
- Fabrizi, L.; Williams, G.; Lee, A.; Meek, J.; Slater, R.; Olhede, S.; Fitzgerald, M. Cortical activity evoked by an acute painful tissue-damaging stimulus in healthy adult volunteers. J. Neurophysiol. 2013, 109, 2393–2403. [Google Scholar] [CrossRef] [Green Version]
- Inui, K.; Tran, T.D.; Hoshiyama, M.; Kakigi, R. Preferential stimulation of Aδ fibers by intra-epidermal needle electrode in humans. Pain 2002, 96, 247–252. [Google Scholar] [CrossRef]
- Otsuru, N.; Inui, K.; Yamashiro, K.; Miyazaki, T.; Takeshima, Y.; Kakigi, R. Assessing Aδ fiber function with lidocaine using intraepidermal electrical stimulation. J. Pain 2010, 11, 621–627. [Google Scholar] [CrossRef]
- Mouraux, A.; Iannetti, G.D.; Plaghki, L. Low intensity intra-epidermal electrical stimulation can activate Aδ-nociceptors selectively. Pain 2010, 150, 199–207. [Google Scholar] [CrossRef]
- Mouraux, A.; Marot, E.; Legrain, V. Short trains of intra-epidermal electrical stimulation to elicit reliable behavioral and electrophysiological responses to the selective activation of nociceptors in humans. Neurosci. Lett. 2014, 561, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodaira, M.; Inui, K.; Kakigi, R. Evaluation of nociceptive Aδ- and C-fiber dysfunction with lidocaine using intraepidermal electrical stimulation. Clin. Neurophysiol. 2014, 125, 1870–1877. [Google Scholar] [CrossRef] [PubMed]
- Omori, S.; Isose, S.; Misawa, S.; Watanabe, K.; Sekiguchi, Y.; Shibuya, K.; Beppu, M.; Amino, H.; Kuwabara, S. Pain-related evoked potentials after intraepidermal electrical stimulation to Aδ and C fibers in patients with neuropathic pain. Neurosci. Res. 2017, 121, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Kirimoto, H.; Tamaki, H.; Otsuru, N.; Yamashiro, K.; Onishi, H.; Nojima, I.; Oliviero, A. Transcranial static magnetic field stimulation over the primary motor cortex induces plastic changes in cortical nociceptive processing. Front. Hum. Neurosci. 2018, 12, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otsuru, N.; Inui, K.; Yamashiro, K.; Miyazaki, T.; Ohsawa, I.; Takeshima, Y.; Kakigi, R. Selective Stimulation of C Fibers by an Intra-Epidermal Needle Electrode in Humans. Open Pain J. 2009, 2, 53–56. [Google Scholar] [CrossRef] [Green Version]
- Novotny, G.E.; Gommert-Novotny, E. Intraepidermal nerves in human digital skin. Cell Tissue Res. 1988, 254, 111–117. [Google Scholar] [CrossRef]
- Levitt, P. Structural and functional maturation of the developing primate brain. J. Pediatr. 2003, 143, 35–45. [Google Scholar] [CrossRef]
- Takahashi, T. Postsynaptic receptor mechanisms underlying developmental speeding of synaptic transmission. Neurosci. Res. 2005, 53, 229–240. [Google Scholar] [CrossRef]
- Khazipov, R.; Luhmann, H.J. Early patterns of electrical activity in the developing cerebral cortex of humans and rodents. Trends Neurosci. 2006, 29, 414–418. [Google Scholar] [CrossRef]
- Kucyi, A.; Davis, K.D. The dynamic pain connectome. Trends Neurosci. 2015, 38, 86–95. [Google Scholar] [CrossRef]
- Apkarian, A.V.; Bushnell, M.C.; Treede, R.D.; Zubieta, J.K. Human brain mechanisms of pain perception and regulation in health and disease. Eur. J. Pain 2005, 9, 463. [Google Scholar] [CrossRef]
- Maitre, N.L.; Key, A.P.; Chorna, O.D.; Slaughter, J.C.; Matusz, P.J.; Wallace, M.T.; Murray, M.M. The Dual Nature of Early-Life Experience on Somatosensory Processing in the Human Infant Brain. Curr. Biol. 2017, 27, 1048–1054. [Google Scholar] [CrossRef] [Green Version]
- Iannetti, G.D.; Zambreanu, L.; Cruccu, G.; Tracey, I. Operculoinsular cortex encodes pain intensity at the earliest stages of cortical processing as indicated by amplitude of laser-evoked potentials in humans. Neuroscience 2005, 131, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Ohara, S.; Crone, N.E.; Weiss, N.; Treede, R.D.; Lenz, F.A. Amplitudes of laser evoked potential recorded from primary somatosensory, parasylvian and medial frontal cortex are graded with stimulus intensity. Pain 2004, 110, 318–328. [Google Scholar] [CrossRef] [PubMed]
- García-larrea, L.; Peyron, R.; Laurent, B.; Mauguière, F.; Bernard, U.C.; Neurologie, D.; Bellevue, H.; Etienne, S. garcia_Larrea97. Neuroreport 1997, 8, 1–5. [Google Scholar]
- Beydoun, A.; Morrow, T.J.; Shen, J.F.; Casey, K.L. Variability of laser-evoked potentials: Attention, arousal and lateralized differences. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials 1993, 88, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Legrain, V.; Mancini, F.; Sambo, C.F.; Torta, D.M.; Ronga, I.; Valentini, E. Cognitive aspects of nociception and pain. Bridging neurophysiology with cognitive psychology. Neurophysiol. Clin. 2012, 42, 325–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iannetti, G.D.; Hughes, N.P.; Lee, M.C.; Mouraux, A. Determinants of laser-evoked EEG responses: Pain perception or stimulus saliency? J. Neurophysiol. 2008, 100, 815–828. [Google Scholar] [CrossRef] [Green Version]
- Baumgärtner, U.; Greffrath, W.; Treede, R.D. Contact heat and cold, mechanical, electrical and chemical stimuli to elicit small fiber-evoked potentials: Merits and limitations for basic science and clinical use. Neurophysiol. Clin. 2012, 42, 267–280. [Google Scholar] [CrossRef]
- Goksan, S.; Hartley, C.; Emery, F.; Cockrill, N.; Poorun, R.; Moultrie, F.; Rogers, R.; Campbell, J.; Sanders, M.; Adams, E.; et al. fMRI reveals neural activity overlap between adult and infant pain. Elife 2015, 4, e06356. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Study Design | A Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-up Period Appropriate to the Aim of the Study | Loss to Follow Up Less than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Group | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Slater, 2010 [69] | Comparative | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 15 |
| Maimon, 2013 [53] | Comparative | 2 | 2 | 2 | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 1 | 2 | 15 |
| Fabrizi, 2016 [71] | Comparative | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 2 | 12 |
| Hartley, 2017 [55] | Comparative | 2 | 1 | 2 | 1 | 0 | 0 | 1 | 2 | 1 | 0 | 1 | 2 | 13 |
| Verriotis, 2018 [70] | Comparative | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 2 | 14 |
| Slater, 2010 [49] | Non-comparative | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 0 | – | – | – | – | 6 |
| Fabrizi, 2011 [72] | Non-comparative | 2 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | – | – | – | – | 7 |
| Worley, 2012 [73] | Non-comparative | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | – | – | – | – | 3 |
| Hartley, 2015 [31] | Non-comparative | 2 | 2 | 2 | 1 | 1 | 0 | 0 | 0 | – | – | – | – | 8 |
| Verriotis, 2016 [74] | Non-comparative | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | – | – | – | – | 8 |
| Maitre, 2017 [54] | Non-comparative | 2 | 2 | 2 | 1 | 0 | 0 | 0 | 2 | – | – | – | – | 9 |
| Jones, 2017 [75] | Non-comparative | 1 | 1 | 2 | 1 | 1 | 0 | 0 | 0 | – | – | – | – | 6 |
| Jones, 2018 [56] | Non-comparative | 1 | 1 | 2 | 1 | 0 | 0 | 0 | 0 | – | – | – | – | 5 |
| Green, 2019 [76] | Non-comparative | 2 | 2 | 2 | 1 | 1 | 0 | 1 | 0 | – | – | – | – | 9 |
| Author, Year | Randomization | Blinding | Withdrawals and Dropouts | Inclusion/ Exclusion Criteria | Adverse Effects | Statistical Analysis | Total |
|---|---|---|---|---|---|---|---|
| Norman, 2008 [67] | 1 | 1 | 0 | 1 | 0 | 1 | 4 |
| Slater, 2010 [66] | 2 | 2 | 1 | 1 | 1 | 1 | 8 |
| Gursul, 2018 [65] | 1 | 0 | 0 | 0 | 0 | 1 | 2 |
| Hartley, 2018 [68] | 2 | 1 | 1 | 1 | 1 | 1 | 7 |
| Jones, 2020 [64] | 0 | 0 | 0 | 1 | 0 | 1 | 2 |
| Author, Year | Study Design | Participants | Stimulation | Outcomes Measured | Results | * Quality Score | ||
|---|---|---|---|---|---|---|---|---|
| Age at Birth | Age at Time of the Study | Number | ||||||
| Slater, 2010 [49] | Non- comparative | 35–39 weeks PMA | 2–13 days | 10 | Heel lance Non-noxious control (contact of a heel lance device against the skin without the skin being touched by the blade) | ERP | ERP evoked by heel lance was different from that by non-noxious control stimulation. | 6/16 |
| Slater, 2010 [69] | Comparative | Term infants: 37–40 weeks PMA, Preterm infants: 24–32 weeks PMA | Term infants: 37–41 weeks PMA, Preterm infants: 37–41 weeks PMA | 15 (term infants: n = 8, preterm infants: n = 7) | Heel lance Lightly tapping a rubber bung | ERP | ERP evoked by heel lance was significantly larger in preterm infants than term infants. | 15/24 |
| Fabrizi, 2011 [72] | Non- comparative | 24–42 weeks GA | 28–46 weeks GA | 46 | Heel lance Lightly tapping a tendon hammer | ERP | In full-term infants, ERP evoked by heel lance (300–700 ms) was different from that by tactile stimulation (50–300 ms). The percentage of occurrence of ERP by both heel lance and tactile stimulation was significantly smaller in the preterm infants than the full-term infants. | 7/16 |
| Worley, 2012 [73] | Non- comparative | Infants | No data | 6 | Heel lance Lightly tapping a tendon hammer | ERP EMG NIRS ECG Behavioral responses Autonomic responses (heart rate, oxygen saturation, respiratory rate, and cardiovascular activity) | ERP evoked by heel lance consisted of an early component followed by a late component. Tapping stimuli evoked only the early component. ERP evoked by heel lance was coupled with NIRS response. Only heel lance elicited a larger flexion withdrawal reflex and behavioral responses, increased heart rate, and decreased oxygen saturation. | 3/16 |
| Maimon, 2013 [53] | Comparative | Group 1: 27–29 weeks GA, Group 2: 27–29 weeks GA, Group 3: 32–33 weeks GA | Group 1: 30 weeks GA; <10 days PNA, Group 2: 33 weeks GA, Group 3: 34.1 weeks GA | Group 1: n = 24, Group 2: n = 22, Group 3: n = 25 | Heel lance | ERP (evoked power) Behavioral indicators of infant pain | No significant difference in brain activity was found between pre- and post-heel lance. | 15/24 |
| Hartley, 2015 [31] | Non- comparative | Term infants | 37–42 weeks GA; <10 days PNA | 30 | Heel lance Noxious stimulation (pinprick: 32 mN, 64 mN, 128 mN) | ERP PIPP EMG | ERP evoked by heel lance (400–700 ms) was greater than that by non-noxious control stimulation. The magnitude of ERP was significantly correlated with the magnitude of EMG. The ERP and EMG magnitudes increased with stimulus intensity of pinprick. | 8/16 |
| Verriotis, 2016 [74] | Non- comparative | 36.3–42.0 weeks GA | 36.6–43.3 weeks GA; 0–16 days PNA | 30 | Heel lanceControl stimulation (contact of a heel lance device against the skin without the skin being touched by the blade) Tactile stimulation (lightly tapping a tendon hammer) | ERP NIRS | ERP evoked by heel lance consisted of N2P2 waves (139 and 202 ms) followed by N3P3 waves (385 and 554 ms). Tactile stimulation induced only N2P2 waves (147 and 248 ms). Electrophysiological (ERP) and hemodynamic responses (NIRS) by heel lance coincided and were positively correlated. | 8/16 |
| Fabrizi, 2016 [71] | Comparative | Infants: 37–42 weeks GA, Adults: – | Infants: 0–19 days PNA (5.8 ± 4.3), Adults: 23–48 years (29.7 ± 6.0 | Infants: 18, Adults: 21 | Infants: Heel lance, Control stimulation (contact of a heel lance device against the skin without the skin being touched by the blade) Adults: Noxious stimulation (a sterile lancet to prick the fifth finger), Control stimulation (contact of a heel lance device against the skin) | ERP | Heel lance (or noxious stimulation) and control stimulation evoked N2P2 waves in infants (140 and 225.5 ms for heel lance and 151.5 and 227 ms for control stimulation) and in adults (102 and 249.5 ms for noxious stimulation and 93.5 and 180.5 ms for control stimulation). Heel lance also evoked a N3P3 waves (403 and 538 ms) in infants but not in adults. | 14/24 |
| Maitre, 2017 [54] | Non- comparative | 37–42 weeks GA | 2–3 days PNA | 54 | Heel lance Light touch (air puff) Cold puff | ERP Crying | ERP evoked by heel lance consisted of a late component. ERP evoked by heel lance was not associated with either the presence or amplitude of cries. | 9/16 |
| Jones, 2017 [75] | Non- comparative | 36–42 weeks GA | No data | 56 | Heel lance | ERP Salivary cortisol Heart rate variability PIPP | ERP evoked by heel lance consisted of N3P3 waves. ERP amplitude was significantly correlated with PIPP. | 6/16 |
| Hartley, 2017 [55] | Non- comparative | 31.9–41.4 weeks GA | 35.1–43.6 weeks GA | 72 | Heel lance Experimental noxious stimulation (128 mN, pinprick; MRC systems) Experimental tactile stimulation (modified tendon hammer) Visual stimulation Auditory stimulation | ERP Heart rate PIPP (facial expression) | ERP evoked by heel lance (400–700 ms) was different from that evoked by non-noxious tactile stimulation. | 13/24 |
| Verriotis, 2018 [70] | Non- comparative | 29–42 weeks GA | 29–43 weeks GA; no older than 2 weeks PNA | 81 | Heel lance | ERP | ERP evoked by heel lance consisted of N2P2 waves followed by N3P3 waves (400–700 ms). Females were more likely to exhibit a widespread ERP than males. | 14/24 |
| Jones, 2018 [56] | Non- comparative | 23–42 weeks GA | 29–47 weeks GA (0–96 days) | 112 | Heel lance Non-noxious sham (contact of a heel lance device against the skin without the skin being touched by the blade Auditory controls | ERP Facial expression Heart rate Oxygenation PIPP | ERP evoked by heel lance consisted of N2P2 waves followed by N3P3 waves. ERP evoked by non-noxious sham and auditory control consisted of N2P2 waves only. | 5/16 |
| Green, 2019 [76] | Non- comparative | 23–42 weeks GA | 28–42 weeks GA | 49 | Heel lance Control lance (contact of a heel lance device against the skin without the skin being touched by the blade) | PIPP-R (facial expression) ERP | ERP evoked by heel lance was different from that by non-noxious control stimulation. The occurrence of ERP evoked by heel lance increased with GA. | 9/16 |
| Author, Year | Participants | Stimulation | Intervention | Outcomes Measured | Results | * Quality Score | ||
|---|---|---|---|---|---|---|---|---|
| Age at Birth | Age at Time of the Study | Number | ||||||
| Norman 2008 [67] | 37–42 weeks GA | 37–143 h PNA | 72 | Heel lance Heel prick (non-skin-breaking pin-prick) Venous blood sampling from the dorsum of the hand | (Only heel prick) Glucose Water | ERP (evoked power)PIPP | All noxious stimuli induced a significant increase in higher frequency components (10–30 Hz). (Only heel prick) There was no difference in brain activity between infants who received either glucose or water. The PIPP score was significantly lower in infants who received glucose than those who received water. | 4 |
| Slater 2010 [66] | 37–43 weeks PMA | >8 days PNA | 44 | Heel lance Non-noxious control (contact of a heel lance device against the skin) | Sucrose Sterile water | ERP PIPP EMG | ERP evoked by heel lance was significantly greater than that evoked by non-noxious control. ERP and EMG response did not differ significantly between infants who received either sucrose or sterile water. The PIPP score was significantly lower in infants who received sucrose than those who received sterile water. | 8 |
| Gursul 2018 [65] | 37–42 weeks GA | 1–5 days PNA | 30 | Heel lance Experimental noxious stimulus (128 mN, pinprick; MRC systems) | C-tactile (CT) optimal touch (brush velocity 30 cm/s) CT non-optimal touch (brush velocity 30 cm/s) No-touch control | ERP EMG | CT optimal touch significantly reduced ERP evoked by heel lance, as compared to no-touch control. CT non-optimal touch did not reduce ERP evoked by heel lance. | 2 |
| Hartley 2018 [68] | 34–42 weeks GA | 34.3–36.3 weeks GA 1–20 PNA | 31 | Heel lance Non-noxious control (contact of a heel lance device against the skin) Retinopathy of prematurity screening examination | Morphine Placebo | ERP PIPP-R | ERP evoked by heel lance was significantly greater than that by non-noxious control. ERP and PIPP-R did not differ between infants who received either morphine or placebo. | 7 |
| Jones 2020 [64] | 23–41 weeks GA | 0–96 PNA | 27 | Heel lance | While held by a parent in skin-to-skin While held by a parent with clothing Not held at all | ERP Facial response HR | Heel lance evoked noxious ERP components (497 to 755 ms). ERP was significantly lower in infants held skin-to-skin compared to those held with clothes. Facial response score and HR were higher in infants held with clothing than those not held or those held skin-to-skin. | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiroshita, Y.; Kirimoto, H.; Ozawa, M.; Watanabe, T.; Uematsu, H.; Yunoki, K.; Sobue, I. Can Event-Related Potentials Evoked by Heel Lance Assess Pain Processing in Neonates? A Systematic Review. Children 2021, 8, 58. https://0-doi-org.brum.beds.ac.uk/10.3390/children8020058
Shiroshita Y, Kirimoto H, Ozawa M, Watanabe T, Uematsu H, Yunoki K, Sobue I. Can Event-Related Potentials Evoked by Heel Lance Assess Pain Processing in Neonates? A Systematic Review. Children. 2021; 8(2):58. https://0-doi-org.brum.beds.ac.uk/10.3390/children8020058
Chicago/Turabian StyleShiroshita, Yui, Hikari Kirimoto, Mio Ozawa, Tatsunori Watanabe, Hiroko Uematsu, Keisuke Yunoki, and Ikuko Sobue. 2021. "Can Event-Related Potentials Evoked by Heel Lance Assess Pain Processing in Neonates? A Systematic Review" Children 8, no. 2: 58. https://0-doi-org.brum.beds.ac.uk/10.3390/children8020058