
Preschool Wheezing and Gastro-Esophageal Reflux: --Causal or Casual Coincidence? Update from Literature

 , and
, and
Abstract
:
{kind=link}
{kind=link}
1. Introduction
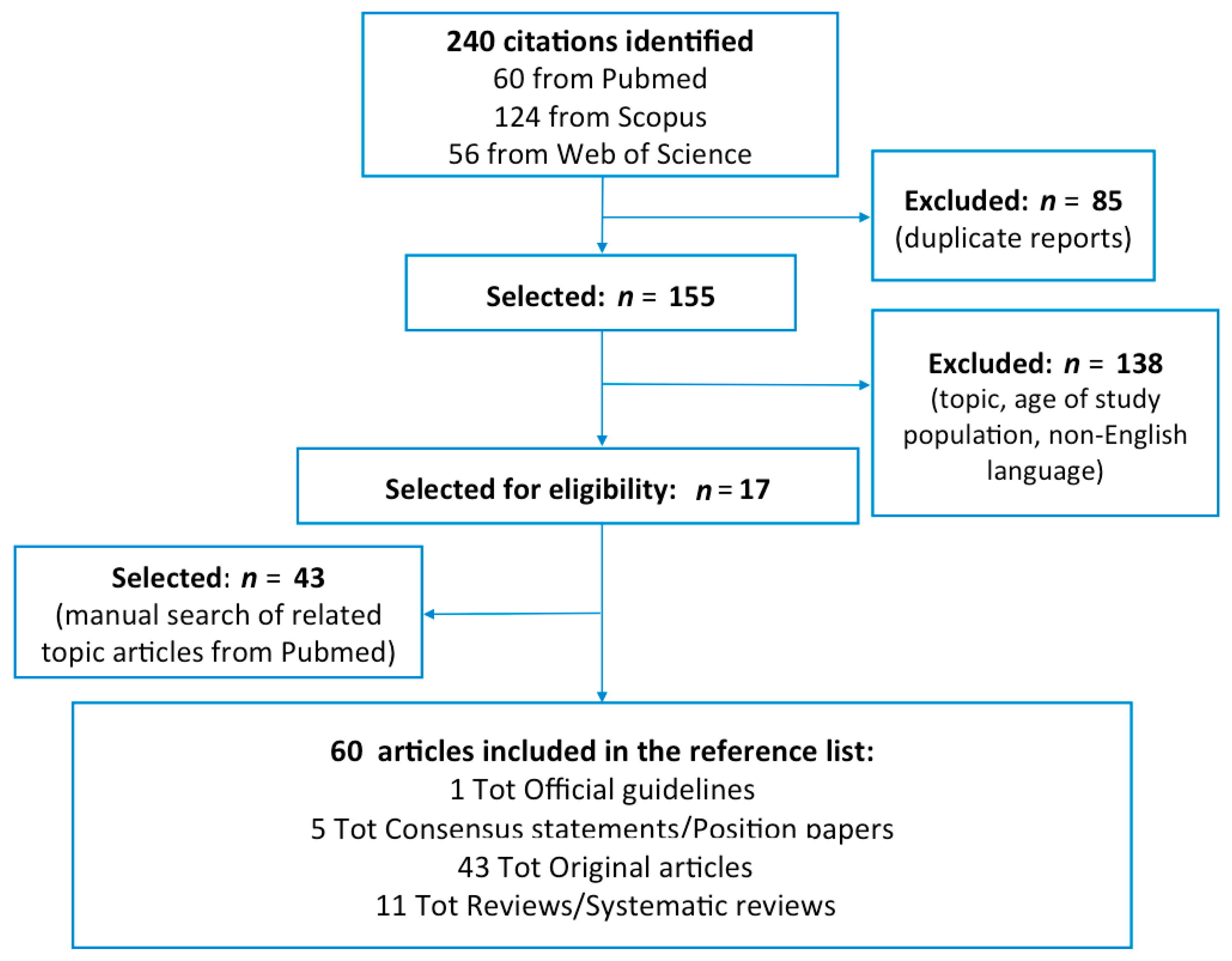
2. Methods
2.1. Definition of GER
2.2. Definition of Preschool Wheeze
3. Results
3.1. Prevalence of GER
3.2. Prevalence of Wheeze
3.3. Mechanisms of the Association between GER and Wheeze
3.4. What Has the Literature Added in the Last Two Decades
3.5. Pulmonologist’s Point of View
3.6. Gastroenterologist’s Point of View
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vandenplas, Y.; Rudolph, C.D. Pediatric gastroesophageal reflux clinical practice guidelines: Joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J. Pediatr. Gastroenterol. Nutr. 2009, 49, 498–547. [Google Scholar]
- Rosen, R.; Vandenplas, Y. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 516–554. [Google Scholar] [CrossRef] [PubMed]
- Sherman, P.M.; Hassall, E. A global, evidence-based consensus on the definition of gastroesophageal reflux disease in the pediatric population. Am. J. Gastroenterol. 2009, 104, 1278–1295. [Google Scholar] [CrossRef]
- Elphick, H.E.; Sherlock, P. Survey of respiratory sounds in infants. Arch. Dis. Child 2001, 84, 35–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacharier, L.B.; Guilbert, T.W. New Directions in Pediatric Asthma. Immunol. Allergy Clin. N. Am. 2019, 39, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Brand, P.L.; Baraldi, E. Definition, assessment and treatment of wheezing disorders in preschool children: An evidence-based approach. Eur. Respir. J. 2008, 32, 1096–1110. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.P.; Chen, E.H. Prevalence of symptoms of gastroesophageal reflux during infancy. A pediatric practice-based survey. Pediatric Practice Research Group. Arch. Pediatr. Adolesc. Med. 1997, 151, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.J.; Pratt, N. Natural history and familial relationships of infant spilling to 9 years of age. Pediatrics 2002, 109, 1061–1067. [Google Scholar] [CrossRef]
- Rasquin-Weber, A.; Hyman, P.E. Childhood functional gastrointestinal disorders. Gut 1999, 45 (Suppl. 2), 1160–1168. [Google Scholar] [CrossRef] [Green Version]
- Campanozzi, A.; Boccia, G. Prevalence and natural history of gastroesophageal reflux: Pediatric prospective survey. Pediatrics 2009, 123, 779–783. [Google Scholar] [CrossRef]
- Nelson, S.P.; Chen, E.H. Prevalence of symptoms of gastroesophageal reflux during childhood: A pediatric practice-based survey. Pediatric Practice Research Group. Arch. Pediatr. Adolesc. Med. 2000, 154, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Martigne, L.; Delaage, P.H. Prevalence and management of gastroesophageal reflux disease in children and adolescents: A nationwide cross-sectional observational study. Eur. J. Pediatr. 2012, 171, 1767–1773. [Google Scholar] [CrossRef] [PubMed]
- Gilger, M.A.; El-Serag, H.B. Prevalence of Endoscopic Findings of Erosive Esophagitis in Children: A Population-based Study. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 141–146. [Google Scholar] [CrossRef]
- Cane, R.S.; Ranganathan, S.C. What do parents of wheezy children understand by ‘‘wheeze’’? Arch. Dis. Child. 2000, 82, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Cane, R.S.; McKenzie, S.A. Parents’ interpretations of children’s respiratory symptoms on video. Arch. Dis. Child. 2001, 84, 31–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitburn, S.; Costelloe, C. The frequency distribution of presenting symptoms in children aged six months to six years to primary care. Prim. Health Care Res. Dev. 2011, 12, 123–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, C.A.; Turner, D. The economic impact of preschool asthma and wheeze. Eur. Respir. J. 2003, 21, 1000–1006. [Google Scholar] [CrossRef] [Green Version]
- Martinez, F.D.; Wright, A.L. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N. Engl. J. Med. 1995, 332, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Visser, C.A.; Garcia-Marcos, L. Prevalence and risk factors of wheeze in Dutch infants in their first year of life. Pediatr. Pulmonol. 2010, 45, 149–156. [Google Scholar] [CrossRef]
- Montella, S.; Baraldi, E. What drives prescribing of asthma medication to preschool wheezing children? A primary care study. Pediatr. Pulmonol. 2013, 48, 1160–1170. [Google Scholar] [CrossRef]
- Bisgaard, H.; Szefler, S. Prevalence of Asthma-Like Symptoms in Young Children. Pediatric. Pulmonol. 2007, 42, 723–728. [Google Scholar] [CrossRef]
- Mendelson, C.L. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am. J. Obstet. Gynecol. 1946, 52, 191–205. [Google Scholar] [CrossRef]
- Marik, P.E. Aspiration syndromes: Aspiration pneumonia and pneumonitis. Hosp. Pract. 2010, 38, 35–42. [Google Scholar] [CrossRef]
- Lopes, F.D.; Alvarenga, G.S. Pulmonary responses to tracheal or esophageal acidification in guinea pigs with airway inflammation. J. Appl. Physiol. 2002, 93, 842–847. [Google Scholar] [CrossRef] [Green Version]
- Allen, G.B.; Leclair, T.R. Acid aspiration-induced airways hyperresponsiveness in mice. J. Appl. Physiol. 2009, 107, 1763–1770. [Google Scholar] [CrossRef] [Green Version]
- Harding, S.M. Gastroesophagel reflux: A potential asthma trigger. Immunol. Allergy Clin. N. Am. 2005, 25, 131–148. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.I.; Schmidt, A. Pulmonary function and acid application in the esophagus. Chest 1986, 90, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.N.; Tanifuji, Y. Effects of esophageal acid perfusion on airway hyperresponsiveness in patients with bronchial asthma. Chest 2000, 118, 1553–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, W.G. Gastroesophageal reflux disease and asthma. Arch. Intern. Med. 1995, 155, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.M.; Charette, L. Gastro-oesophageal reflux and childhood asthma: The acid test. Thorax 1985, 40, 592–597. [Google Scholar] [CrossRef] [Green Version]
- Harding, S.M. Gastroesophageal reflux, asthma, and mechanisms of interaction. Am. J. Med. 2001, 111, 8–12. [Google Scholar] [CrossRef]
- Field, S.K. Gastroesophageal Reflux and Asthma: Can the Paradox Be Explained? Can. Respir. J. 2000, 7, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Mitsuhashi, M.; Tomomasa, T. The evaluation of gastroesophageal reflux symptoms in patients with bronchial asthma. Ann. Allergy 1985, 54, 317–320. [Google Scholar] [PubMed]
- Lazenby, J.P.; Guzzo, M.R. Oral Corticosteroids Increase Esophageal Acid Contact Times in Patients with Stable Asthma. Chest 2002, 121, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Saglani, S.; Nicholson, A.G. Investigation of young children with severe recurrent wheeze: Any clinical benefit? Eur. Respir. J. 2006, 27, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Siti Mazliah, K.; Norzila, M.Z. Prevalence, clinical predictors and diagnosis of gastro-oesophageal reflux in children with persistent respiratory symptoms. Med. J. Malays. 2000, 55, 180–187. [Google Scholar]
- Rosen, R.; Amirault, J. The utility of endoscopy and multichannel intraluminal impedance testing in children with cough and wheezing. Pediatr. Pulmonol. 2014, 49, 1090–1096. [Google Scholar] [CrossRef]
- Yuksel, H.; Yilmaz, O. Frequency of gastroesophageal reflux disease in nonatopic children with asthma-like airway disease. Respir Med. 2006, 100, 393–398. [Google Scholar] [CrossRef] [Green Version]
- Celedón, J.C.; Litonjua, A.A. Bottle Feeding in the Bed or Crib Before Sleep Time and Wheezing in Early Childhood. Pediatrics 2002, 110, e77. [Google Scholar] [CrossRef] [Green Version]
- Colombo, J.L.; Hallberg, T.K. Airway reactivity following repeated milk aspiration in rabbits. Pediatr. Pulmonol. 2000, 29, 113–119. [Google Scholar] [CrossRef]
- Ozdogan, S.; Tabakci, B. The evaluation of risk factors for recurrent hospitalizations resulting from wheezing attacks in preschool children. Ital. J. Pediatr. 2015, 41, 91. [Google Scholar] [CrossRef] [Green Version]
- Noronha, A.C.; de Bruin, V.M. Gastroesophageal reflux and obstructive sleep apnea in childhood. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 383–389. [Google Scholar] [CrossRef]
- Ing, A.J.; Ngu, M.C. Obstructive sleep apnea and gastroesophageal reflux. Am. J. Med. 2000, 108 (Suppl. 4a), 120S–125S. [Google Scholar] [CrossRef]
- Wasilewska, J.; Semeniuk, J. Respiratory response to proton pump inhibitor treatment in children with obstructive sleep apnea syndrome and gastroesophageal reflux disease. Sleep Med. 2012, 13, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Sacco, O.; Fregonese, B. Bronchoalveolar lavage and esophageal pH monitoring data in children with “difficult to treat” respiratory symptoms. Pediatr. Pulmonol. 2000, 30, 313–319. [Google Scholar] [CrossRef]
- Sacco, O.; Silvestri, M. IL-8 and airway neutrophilia in children with gastroesophageal reflux and asthma-like symptoms. Respir. Med. 2006, 100, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Baets, F.; Aarts, C. Milk protein and Oil-Red-O staining of alveolar macrophages in chronic respiratory disease of infancy. Pediatr. Pulmonol. 2010, 45, 1213–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullmann, N.; Sacco, O. Usefulness and safety of double endoscopy in children with gastroesophageal reflux and respiratory symptoms. Respir. Med. 2010, 104, 593–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattioli, G.; Pini-Prato, A. Esophageal impedance/pH monitoring in pediatric patients: Preliminary experience with 50 cases. Dig. Dis. Sci. 2006, 51, 2341–2347. [Google Scholar] [CrossRef]
- Ghezzi, M.; Guida, E. Weakly Acidic Gastroesophageal Refluxes Are Frequently Triggers in Young Children with Chronic Cough. Pediatr. Pulmonol. 2013, 48, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Guiddir, T.; Saint-Pierre, P. Neutrophilic Steroid-Refractory Recurrent Wheeze and Eosinophilic Steroid-Refractory Asthma in Children. J. Allergy Clin. Immunol. Pract. 2017, 5, 1351–1361. [Google Scholar] [CrossRef] [Green Version]
- Farrell, S.; McMaster, C. Pepsin in bronchoalveolar lavage fluid: A specific and sensitive method of diagnosing gastro-oesophageal reflux related pulmonary aspiration. J. Pediatr. Surg. 2006, 41, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, A.F.; El-Desoky, T. Clinical Utility of Bronchoalveolar Lavage Pepsin in Diagnosis of Gastroesophageal Reflux among Wheezy Infants. Can. Respir. J. 2016, 2016, 9480843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, M.; Heltshe, S.L. Exhaled nitric oxide predicts persistence of wheezing, exacerbations, and decline in lung function in wheezy infants and toddlers. Clin. Exp. Allergy 2013, 43, 1351–1361. [Google Scholar] [CrossRef] [Green Version]
- White, M.P.; Kolstad, T.K. Exhaled nitric oxide in wheezy infants predicts persistent atopic asthma and exacerbations at school age. J. Asthma Allergy 2020, 13, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, M.; Mattioli, G. Correlations between exhaled nitric oxide levels and pH-metry data in asthmatics with gastro-oesophageal reflux. Respiration 2004, 71, 329–335. [Google Scholar] [CrossRef]
- Wasowska-Królikowska, K.; Toporowska-Kowalska, E. Asthma and gastroesophageal reflux in children. Med. Sci. Monit. 2002, 8, 64–71. [Google Scholar]
- Jain, A.; Patwari, A.K. Association of gastroesophageal reflux disease in young children with persistent respiratory symptoms. J. Trop. Pediatr. 2002, 48, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Safe, M.; Chan, W.H. Widespread use of gastric acid inhibitors in infants: Are they needed? Are they safe? World J. Gastrointest. Pharmacol. Ther. 2016, 7, 531–539. [Google Scholar] [CrossRef]
- Berni Canani, R.; Cirillo, P. Therapy with gastric acidity inhibitors increases the risk of acute gastroenteritis and community-acquired pneumonia in children. Pediatrics 2006, 117, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, J.T.; Wise, R.A. Lansoprazole for children with poorly controlled asthma: A randomized controlled trial. JAMA 2012, 307, 373–381. [Google Scholar] [PubMed] [Green Version]
- British Guideline on the Management of Asthma. Available online: https://www.sign.ac.uk/media/1773/sign158-updated.pdf (accessed on 18 January 2021).
- Global Initiative for Asthma. Available online: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf (accessed on 18 January 2021).
- Mueller, G.A.; Wolf, S. Contemporary Topics in Pediatric Pulmonology for the Primary Care Clinician. Curr. Probl. Pediatr. Adolesc. Health Care 2013, 43, 130–156. [Google Scholar] [CrossRef] [PubMed]
- Bacharier, L.B.; Guilbert, W.T. Diagnosis and management of early asthma in preschool-aged children. J. Allergy Clin. Immunol. 2012, 130, 287–298. [Google Scholar] [CrossRef]
- Goussard, P. The role of bronchoscopy in wheezing preschool children. Curr. All Clin. Immunol. 2018, 31, 75–79. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borrelli, M.; Ponte, G.; Miele, E.; Maglione, M.; Caffarelli, C.; Santamaria, F. Preschool Wheezing and Gastro-Esophageal Reflux: --Causal or Casual Coincidence? Update from Literature. Children 2021, 8, 180. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030180
Borrelli M, Ponte G, Miele E, Maglione M, Caffarelli C, Santamaria F. Preschool Wheezing and Gastro-Esophageal Reflux: --Causal or Casual Coincidence? Update from Literature. Children. 2021; 8(3):180. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030180
Chicago/Turabian StyleBorrelli, Melissa, Giuliana Ponte, Erasmo Miele, Marco Maglione, Carlo Caffarelli, and Francesca Santamaria. 2021. "Preschool Wheezing and Gastro-Esophageal Reflux: --Causal or Casual Coincidence? Update from Literature" Children 8, no. 3: 180. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030180